
Quality and Presence of Behaviour Change Techniques in Mobile Apps for the Mediterranean Diet: A Content Analysis of Android Google Play and Apple App Store Apps




Abstract
:1. Introduction
2. Materials and Methods
2.1. App Identification and Selection
2.2. Data Extraction and Assessment of App Quality and BCTs
2.2.1. Assessment of App Quality
2.2.2. Assessment of Presence of BCTs
2.3. Data Analysis
3. Results
3.1. Identification of Apps
3.2. App Characteristics and Features
3.3. App Quality
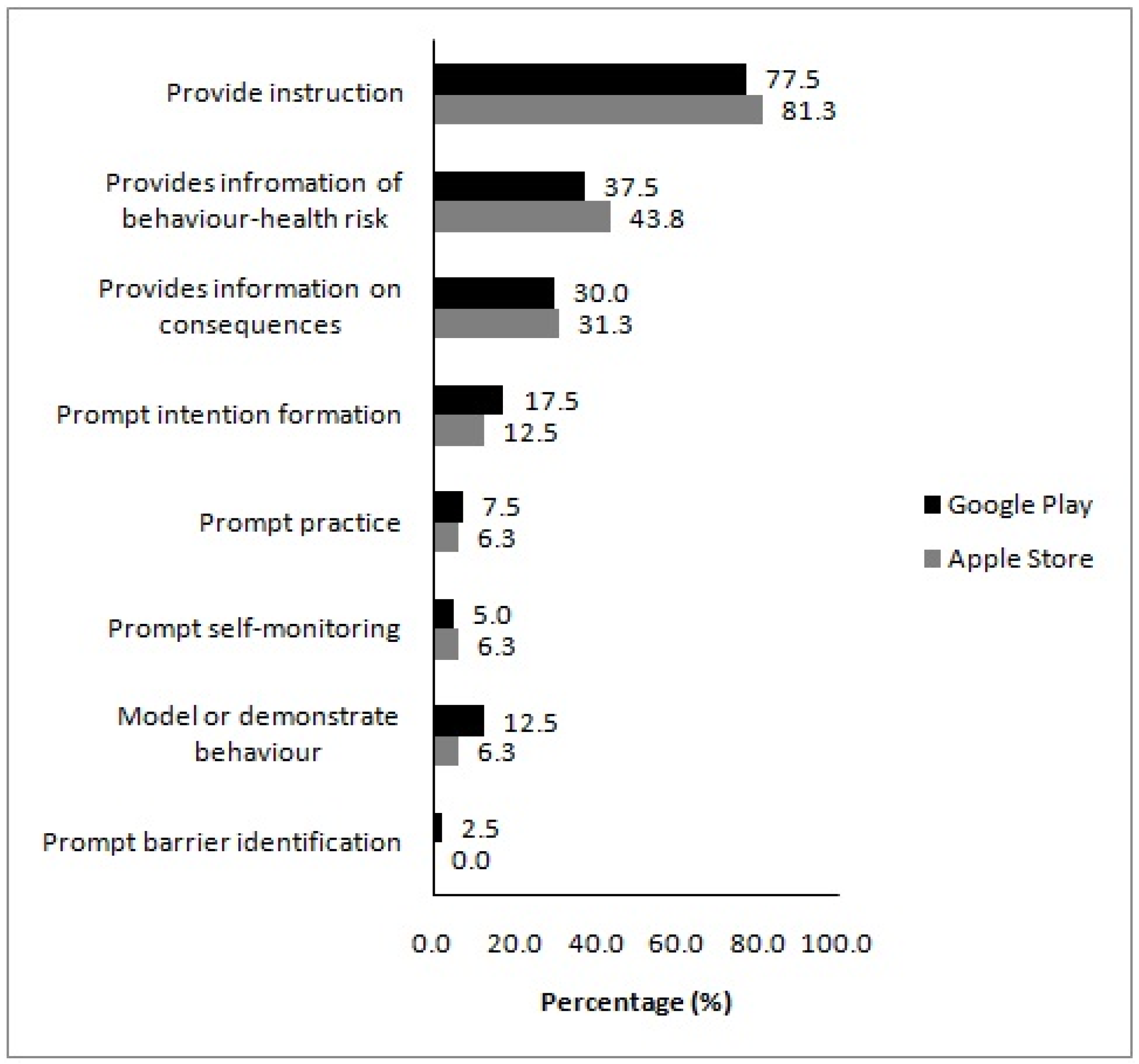
3.4. Presence of BCTs
3.5. Relationship between App Quality and the Presence of BCTs
4. Discussion
4.1. Main Findings
4.2. App Features
4.3. App Quality
4.4. Presence of BCTs
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trichopoulou, A.; Martínez-González, M.A.; Tong, T.Y.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and potential health benefits of the Mediterranean diet: Views from experts around the world. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, J.; Jones, D.P.; Goldberg, J.; Ziegler, T.R.; Bostick, R.M.; Wilson, P.W.; Manatunga, A.K.; Shallenberger, L.; Jones, L.; Vaccarino, V. Association between adherence to the Mediterranean diet and oxidative stress. Am. J. Clin. Nutr. 2008, 88, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R. Anti-inflammatory effects of the Mediterranean diet: The experience of the PREDIMED study. Proc. Nutr. Soc. 2010, 69, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, A.; Nolen-Doerr, E.; Mantzoros, C.S. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients 2020, 12, 3342. [Google Scholar] [CrossRef]
- Esposito, K.; Kastorini, C.M.; Panagiotakos, D.B.; Giugliano, D. Mediterranean diet and weight loss: Meta-analysis of randomized controlled trials. Metab. Syndr. Relat. Disord. 2011, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.; Bihuniak, J.D.; Shook, J.; Kenny, A.; Kerstetter, J.; Huedo-Medina, T.B. The effect of the traditional Mediterranean-style diet on metabolic risk factors: A meta-analysis. Nutrients 2016, 8, 168. [Google Scholar] [CrossRef] [Green Version]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [Green Version]
- Vilarnau, C.; Stracker, D.M.; Funtikov, A.; da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2019, 72, 83–91. [Google Scholar] [CrossRef]
- Council of the European Union. Council Conclusions on Nutrition and Physical Activity. Available online: http://www.consilium.europa.eu/uedocs/cms_data/docs/pressdata/en/lsa/143285.pdf (accessed on 22 November 2014).
- National Institute for Health and Care Excellence. Maintaining a Healthy Weight and Preventing Excess Weight Gain among Children and Adults: Draft Guideline. Available online: http://www.nice.org.uk/guidance/gid-phg78/resources/maintaining-a-healthy-weight-and-preventing-excess-weight-gain-among-children-and-adults-draft-guideline2 (accessed on 20 May 2017).
- Fiordelli, M.; Diviani, N.; Schulz, P.J. Mapping mHealth research: A decade of evolution. J. Med. Internet Res. 2013, 15, e95. [Google Scholar] [CrossRef] [PubMed]
- Handel, M.J. mHealth (mobile health)-using Apps for health and wellness. Explore 2011, 7, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, S.S.; Whitehead, M.; Sheats, J.Q.; Mastromonico, J.; Hardy, D.; Smith, S.A. Smartphone Applications for Promoting Healthy Diet and Nutrition: A Literature Review. Jacobs J. Food Nutr. 2015, 2, 21. [Google Scholar]
- Villinger, K.; Wahl, D.R.; Boeing, H.; Schupp, H.T.; Renner, B. The effectiveness of app-based mobile interventions on nutrition behaviours and nutrition-related health outcomes: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 1465–1484. [Google Scholar] [CrossRef] [Green Version]
- Statista. Number of Smartphone Users from 2016 to 2021 (In Billions). Available online: https://www.statista.com/statistics/330695/number-of-smartphone-users-worldwide/ (accessed on 4 December 2021).
- AppBrain. Google Play Stats: Most Popular Google Play Categories. Available online: https://www.appbrain.com/stats/android-market-app-categories (accessed on 4 December 2021).
- PocketGamer. App Store Metrics: Application Category Distribution. Available online: https://www.pocketgamer.biz/metrics/app-store/categories/ (accessed on 4 December 2021).
- Bardus, M.; van Beurden, S.B.; Smith, J.R.; Abraham, C. A review and content analysis of engagement, functionality, aesthetics, information quality, and change techniques in the most popular commercial apps for weight management. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simões, P.; Silva, A.G.; Amaral, J.; Queirós, A.; Rocha, N.P.; Rodrigues, M. Features, Behavioral Change Techniques, and Quality of the Most Popular Mobile Apps to Measure Physical Activity: Systematic Search in App Stores. JMIR Mhealth Uhealth 2018, 6, e11281. [Google Scholar] [CrossRef] [Green Version]
- Direito, A.; Dale, L.P.; Shields, E.; Dobson, R.; Whittaker, R.; Maddison, R. Do physical activity and dietary smartphone applications incorporate evidence-based behaviour change techniques? BMC Public Health 2014, 14, 646. [Google Scholar] [CrossRef] [Green Version]
- BinDhim, N.F.; Hawkey, A.; Trevena, L. A systematic review of quality assessment methods for smartphone health apps. Telemed. E Health 2015, 21, 97–104. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Tjondronegoro, D.; Mani, M. Mobile app rating scale: A new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth 2015, 3, e27. [Google Scholar] [CrossRef] [Green Version]
- McKay, F.H.; Cheng, C.; Wright, A.; Shill, J.; Stephens, H.; Uccellini, M. Evaluating mobile phone applications for health behaviour change: A systematic review. J. Telemed. Telecare 2018, 24, 22–30. [Google Scholar] [CrossRef]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Johnston, M.; Francis, J.; Hardeman, W.; Eccles, M. From Theory to Intervention: Mapping Theoretically Derived Behavioural Determinants to Behaviour Change Techniques. Appl. Psychol. 2008, 57, 660–680. [Google Scholar] [CrossRef]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, D.E.; Yang, C.H.; Maher, J.P. Behavior change techniques in top-ranked mobile apps for physical activity. Am. J. Prev. Med. 2014, 46, 649–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagoto, S.; Schneider, K.; Jojic, M.; DeBiasse, M.; Mann, D. Evidence-based strategies in weight-loss mobile apps. Am. J. Prev. Med. 2013, 45, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef] [Green Version]
- Middelweerd, A.; Mollee, J.S.; van der Wal, C.N.; Brug, J.; Te Velde, S.J. Apps to promote physical activity among adults: A review and content analysis. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 97. [Google Scholar] [CrossRef] [Green Version]
- Schoeppe, S.; Alley, S.; Rebar, A.L.; Hayman, M.; Bray, N.A.; Van Lippevelde, W.; Gnam, J.P.; Bachert, P.; Direito, A.; Vandelanotte, C. Apps to improve diet, physical activity and sedentary behaviour in children and adolescents: A review of quality, features and behaviour change techniques. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 83. [Google Scholar] [CrossRef]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Papadaki, A.; Scott, J.A. Process evaluation of an innovative healthy eating website promoting the Mediterranean diet. Health Educ. Res. 2006, 21, 206–218. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, A.; Thanasoulias, A.; Pound, R.; Sebire, S.J.; Jago, R. Employees’ expectations of internet-based, workplace interventions promoting the Mediterranean diet: A qualitative study. J. Nutr. Educ. Behav. 2016, 48, 706–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcus, B.H.; Nigg, C.R.; Riebe, D.; Forsyth, L.H. Interactive communication strategies: Implications for population-based physical-activity promotion. Am. J. Prev. Med. 2000, 19, 121–126. [Google Scholar] [CrossRef]
- Noell, J.; Glasgow, R.E. Interactive technology applications for behavioral counseling: Issues and opportunities for health care settings. Am. J. Prev. Med. 1999, 17, 269–274. [Google Scholar] [CrossRef]
- Womble, L.G.; Wadden, T.A.; McGuckin, B.G.; Sargent, S.L.; Rothman, R.A.; Krauthamer-Ewing, E.S. A randomized controlled trial of a commercial internet weight loss program. Obes. Res. 2004, 12, 1011–1018. [Google Scholar] [CrossRef]
- Winett, R.A.; Roodman, A.A.; Winett, S.G.; Bajzek, W.; Rovniak, L.S.; Whiteley, J.A. The effects of the Eat4Life Internet-based health behavior program on the nutrition and activity practices of high school girls. J. Gend. Cult. Health 1999, 4, 239–254. [Google Scholar] [CrossRef]
- Armstrong, S. Which app should I use? BMJ 2015, 351, h4597. [Google Scholar] [CrossRef]
- Dennison, L.; Morrison, L.; Conway, G.; Yardley, L. Opportunities and challenges for smartphone applications in supporting health behavior change: Qualitative study. J. Med. Internet Res. 2013, 15, e86. [Google Scholar] [CrossRef]
- Yardley, L.; Spring, B.J.; Riper, H.; Morrison, L.G.; Crane, D.H.; Curtis, K.; Merchant, G.C.; Naughton, F.; Blandford, A. Understanding and Promoting Effective Engagement With Digital Behavior Change Interventions. Am. J. Prev. Med. 2016, 51, 833–842. [Google Scholar] [CrossRef] [Green Version]
- West, J.H.; Belvedere, L.M.; Andreasen, R.; Frandsen, C.; Hall, P.C.; Crookston, B.T. Controlling Your “App”etite: How Diet and Nutrition-Related Mobile Apps Lead to Behavior Change. JMIR Mhealth Uhealth 2017, 5, e95. [Google Scholar] [CrossRef]
- Quintana, Y.; Feightner, J.W.; Wathen, C.N.; Sangster, L.M.; Marshall, J.N. Preventive health information on the Internet. Qualitative study of consumers’ perspectives. Can. Fam. Physician 2001, 47, 1759–1765. [Google Scholar] [PubMed]
- West, J.H.; Cougar Hall, P.; Arredondo, V.; Berrett, B.; Guerra, B.; Farrell, J. Health Behavior Theories in Diet Apps. J. Consum. Health Internet 2013, 17, 10–24. [Google Scholar] [CrossRef]
- Lieffers, J.R.L.; Arocha, J.F.; Grindrod, K.; Hanning, R.M. Experiences and Perceptions of Adults Accessing Publicly Available Nutrition Behavior-Change Mobile Apps for Weight Management. J. Acad. Nutr. Diet. 2018, 118, 229–239.e223. [Google Scholar] [CrossRef]
- DiFilippo, K.N.; Huang, W.D.; Chapman-Novakofski, K.M. Mobile Apps for the Dietary Approaches to Stop Hypertension (DASH): App Quality Evaluation. J. Nutr. Educ. Behav. 2018, 50, 620–625. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Mean | SD | Median | Min | Max | Cronbach’s α | |
|---|---|---|---|---|---|---|
| Engagement (5 items) | 2.29 | 0.61 | 2.00 | 1.60 | 3.60 | 0.850 |
| Functionality (4 items) | 3.58 | 0.44 | 3.75 | 1.75 | 4.25 | 0.761 |
| Aesthetics (3 items) | 2.83 | 0.59 | 3.00 | 1.33 | 4.00 | 0.831 |
| Information (7 items) | 2.67 | 0.54 | 2.67 | 1.00 | 3.80 | 0.710 |
| App Quality (overall mean) | 2.84 | 0.42 | 2.81 | 1.98 | 3.78 | 0.864 |
| App subjective quality (4 items) | 1.69 | 0.42 | 1.50 | 1.25 | 2.75 | 0.735 |
| App-specific quality (6 items) | 2.86 | 0.61 | 2.83 | 2.00 | 4.00 | 0.894 |
| Number of BCTs (26 items) | 2.3 | 1.4 | 2.0 | 0 | 6 | 0.752 a |
| App Platform | |||||
|---|---|---|---|---|---|
| Apple App Store(n = 15) | Google Play (n = 40) | ||||
| Mean | SD | Mean | SD | p-Value | |
| Engagement | 2.23 | 0.54 | 2.32 | 0.64 | 0.863 |
| Functionality | 3.78 | 0.27 | 3.51 | 0.47 | 0.027 |
| Aesthetics | 2.96 | 0.64 | 2.78 | 0.57 | 0.454 |
| Information | 2.50 | 0.59 | 2.74 | 0.51 | 0.160 |
| App Quality (overall mean) | 2.87 | 0.41 | 2.84 | 0.43 | 0.770 |
| App subjective quality | 1.63 | 0.46 | 1.71 | 0.41 | 0.394 |
| App-specific quality | 2.90 | 0.59 | 2.85 | 0.62 | 0.683 |
| Number of BCTs | 1.9 | 1.4 | 2.4 | 1.4 | 0.084 |
| MARS Domain | Spearman Rank Correlation Coefficients | p-Value |
|---|---|---|
| Engagement | 0.252 | 0.064 |
| Functionality | 0.121 | 0.378 |
| Aesthetics | 0.225 | 0.099 |
| Information | 0.269 | 0.047 |
| App quality (overall mean) | 0.267 | 0.049 |
| Apple App Store app quality (overall mean) | 0.251 | 0.368 |
| Google Play app quality (overall mean) | 0.295 | 0.065 |
| App subjective quality | 0.326 | 0.015 |
| App-specific quality | 0.351 | 0.009 |
| Behavioural Change Techniques | ||||
|---|---|---|---|---|
| 0 or 1 (n = 16) | 2 (n = 24) | ≥3 (n = 15) | ||
| MARS Domain | Mean (SD) | p-Value | ||
| Engagement | 2.23 (0.54) | 2.13 (0.56) | 2.61 (0.66) | 0.046 |
| Functionality | 3.58 (0.55) | 3.49 (0.38) | 3.73 (0.36) | 0.158 |
| Aesthetics | 2.81 (0.58) | 2.64 (0.53) | 3.16 (0.58) | 0.047 |
| Information | 2.63 (0.45) | 2.48 (0.48) | 3.03 (0.56) | 0.017 |
| App Quality (overall mean) | 2.81 (0.37) | 2.69 (0.38) | 3.13 (0.42) | 0.012 |
| App subjective quality | 1.59 (0.38) | 1.58 (0.37) | 1.97 (0.46) | 0.021 |
| App-specific quality | 2.75 (0.38) | 2.64 (0.58) | 3.34 (0.61) | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McAleese, D.; Linardakis, M.; Papadaki, A. Quality and Presence of Behaviour Change Techniques in Mobile Apps for the Mediterranean Diet: A Content Analysis of Android Google Play and Apple App Store Apps. Nutrients 2022, 14, 1290. https://doi.org/10.3390/nu14061290
McAleese D, Linardakis M, Papadaki A. Quality and Presence of Behaviour Change Techniques in Mobile Apps for the Mediterranean Diet: A Content Analysis of Android Google Play and Apple App Store Apps. Nutrients. 2022; 14(6):1290. https://doi.org/10.3390/nu14061290
Chicago/Turabian StyleMcAleese, Daniel, Manolis Linardakis, and Angeliki Papadaki. 2022. "Quality and Presence of Behaviour Change Techniques in Mobile Apps for the Mediterranean Diet: A Content Analysis of Android Google Play and Apple App Store Apps" Nutrients 14, no. 6: 1290. https://doi.org/10.3390/nu14061290
APA StyleMcAleese, D., Linardakis, M., & Papadaki, A. (2022). Quality and Presence of Behaviour Change Techniques in Mobile Apps for the Mediterranean Diet: A Content Analysis of Android Google Play and Apple App Store Apps. Nutrients, 14(6), 1290. https://doi.org/10.3390/nu14061290