
Utility of an Isotonic Beverage on Hydration Status and Cardiovascular Alterations




Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Procedures
2.4. Beverages and Beverage Preparation
2.5. Urinary Hydration Measures
2.6. Anthropometrics and Body Water Compartmentalization
2.7. Cardiovascular Measures
2.8. Statistical Analysis
3. Results
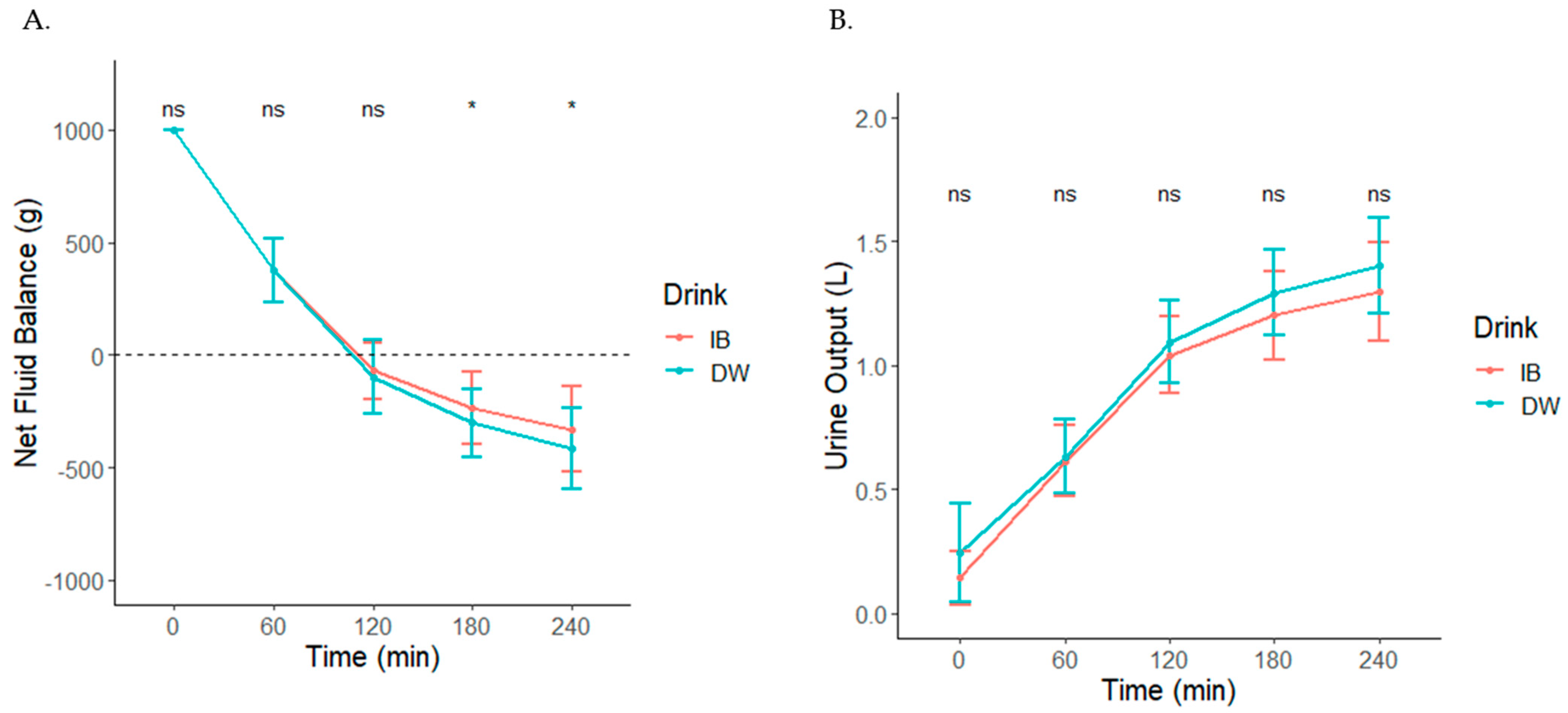
3.1. Beverage Hydration Index, Net Fluid Balance, and Cumulative Urine Output
3.2. Total Body Water, Intracellular Water, and Extracellular Water Measures
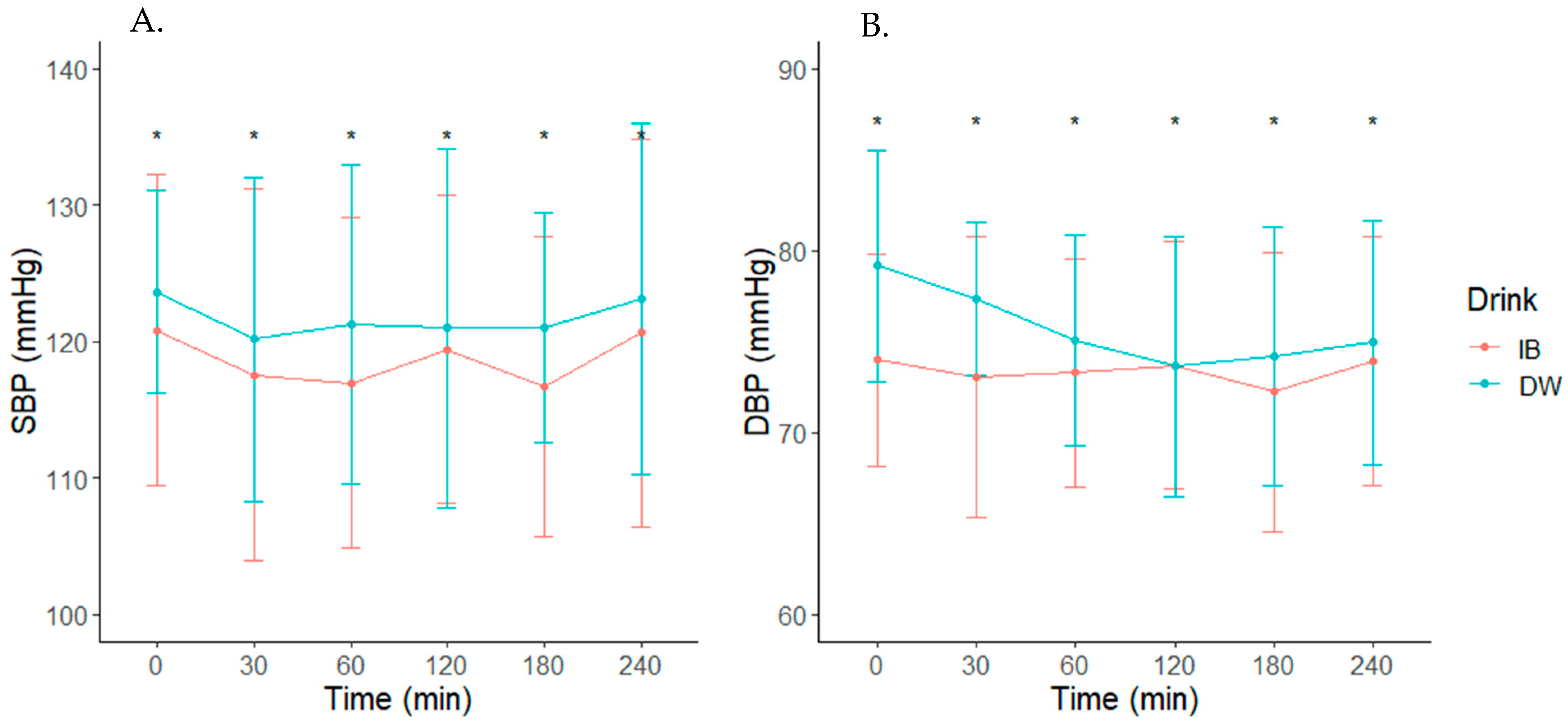
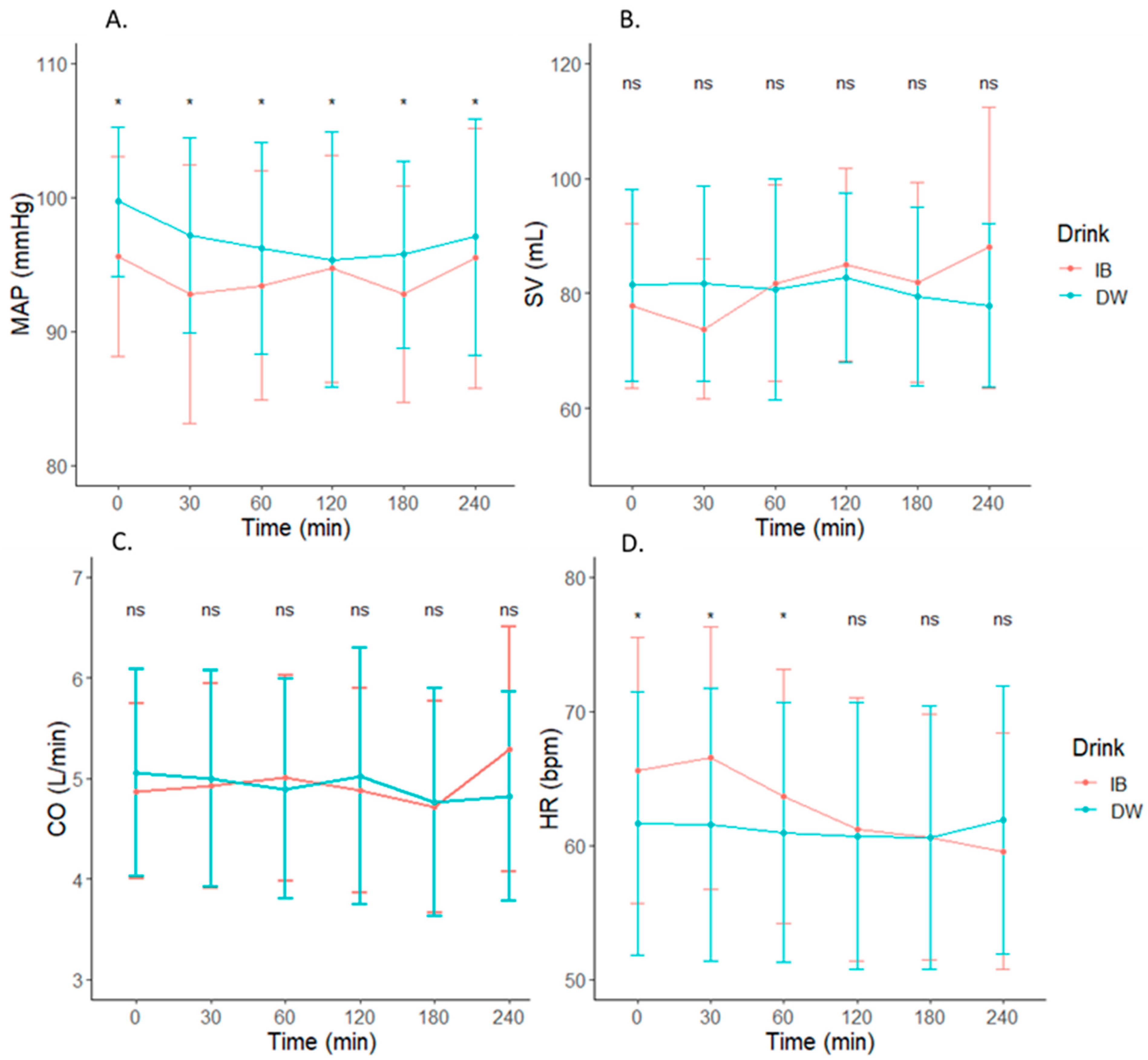
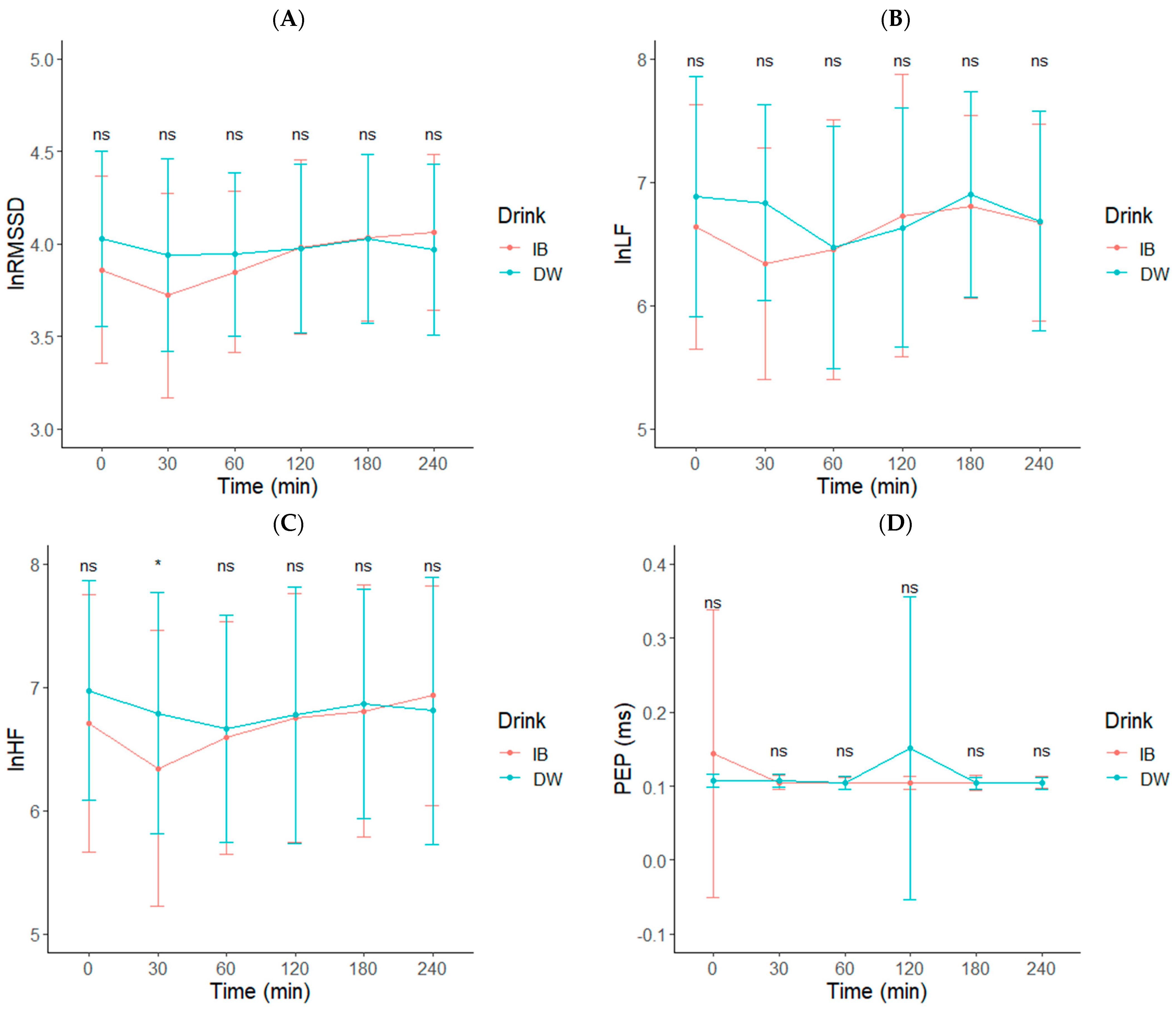
3.3. Cardiovascular Measures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, J. Water, Other Fluids, and Fatal Coronary Heart Disease|American Journal of Epidemiology|Oxford Academic. Am. J. Epidemiol. 2002, 155, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Perini, R.; Veicsteinas, A. Heart Rate Variability and Autonomic Activity at Rest and during Exercise in Various Physiological Conditions. Eur. J. Appl. Physiol. 2003, 90, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.D.; Scott, D.M.; Brand, N.A.; Suh, H.-G.; Seal, A.D.; McDermott, B.P.; Ganio, M.S.; Kavouras, S.A. Mild Hypohydration Impairs Cycle Ergometry Performance in the Heat: A Blinded Study. Scand. J. Med. Sci. Sports 2019, 29, 686–695. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.; Jeukendrup, A. Optimal Composition of Fluid-Replacement Beverages. Compr. Physiol. 2014, 4, 575–620. [Google Scholar] [CrossRef]
- Piil, J.F.; Lundbye-Jensen, J.; Christiansen, L.; Ioannou, L.; Tsoutsoubi, L.; Dallas, C.N.; Mantzios, K.; Flouris, A.D.; Nybo, L. High Prevalence of Hypohydration in Occupations with Heat Stress-Perspectives for Performance in Combined Cognitive and Motor Tasks. PLoS ONE 2018, 13, e0205321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belval, L.N.; Hosokawa, Y.; Casa, D.J.; Adams, W.M.; Armstrong, L.E.; Baker, L.B.; Burke, L.; Cheuvront, S.; Chiampas, G.; González-Alonso, J.; et al. Practical Hydration Solutions for Sports. Nutrients 2019, 11, 1550. [Google Scholar] [CrossRef] [Green Version]
- Morrissey, M.C.; Casa, D.J.; Brewer, G.J.; Adams, W.M.; Hosokawa, Y.; Benjamin, C.L.; Grundstein, A.J.; Hostler, D.; McDermott, B.P.; McQuerry, M.L.; et al. Heat Safety in the Workplace: Modified Delphi Consensus to Establish Strategies and Resources to Protect the US Workers. GeoHealth 2021, 5, e2021GH000443. [Google Scholar] [CrossRef]
- Wansink, B.; Cardello, A.; North, J. Fluid Consumption and the Potential Role of Canteen Shape in Minimizing Dehydration. Mil. Med. 2005, 170, 871–873. [Google Scholar] [CrossRef] [Green Version]
- Rogers, R.; Cole, R. Hydration Status in US Military Officer Students. US Army Med. Dep. J. 2016, 24–30. [Google Scholar]
- Murray, R. Rehydration Strategies—Balancing Substrate, Fluid, and Electrolyte Provision. Int. J. Sports Med. 1998, 19, S133–S135. [Google Scholar] [CrossRef]
- Maughan, R.J.; Watson, P.; Cordery, P.A.; Walsh, N.P.; Oliver, S.J.; Dolci, A.; Rodriguez-Sanchez, N.; Galloway, S.D. A Randomized Trial to Assess the Potential of Different Beverages to Affect Hydration Status: Development of a Beverage Hydration Index. Am. J. Clin. Nutr. 2016, 103, 717–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maughan, R.J.; Watson, P.; Cordery, P.A.A.; Walsh, N.P.; Oliver, S.J.; Dolci, A.; Rodriguez-Sanchez, N.; Galloway, S.D.R. Sucrose and Sodium but Not Caffeine Content Influence the Retention of Beverages in Humans Under Euhydrated Conditions. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sollanek, K.J.; Tsurumoto, M.; Vidyasagar, S.; Kenefick, R.W.; Cheuvront, S.N. Neither Body Mass nor Sex Influences Beverage Hydration Index Outcomes during Randomized Trial When Comparing 3 Commercial Beverages. Am. J. Clin. Nutr. 2018, 107, 544–549. [Google Scholar] [CrossRef]
- Clarke, M.M.; Stanhewicz, A.E.; Wolf, S.T.; Cheuvront, S.N.; Kenefick, R.W.; Kenney, W.L. A Randomized Trial to Assess Beverage Hydration Index in Healthy Older Adults. Am. J. Clin. Nutr. 2019, 109, 1640–1647. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J. Effect of Water Drinking on Sympathetic Nervous Activity and Blood Pressure. Curr. Hypertens. Rep. 2005, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.; Shannon, J.R.; Black, B.K.; Ali, Y.; Farley, M.; Costa, F.; Diedrich, A.; Robertson, R.M.; Biaggioni, I.; Robertson, D. The Pressor Response to Water Drinking in Humans. Circulation 2000, 101, 504–509. [Google Scholar] [CrossRef]
- Scott, E.M.; Greenwood, J.P.; Gilbey, S.G.; Stoker, J.B.; Mary, D.A.S.G. Water Ingestion Increases Sympathetic Vasoconstrictor Discharge in Normal Human Subjects. Clin. Sci. 2001, 100, 335–342. [Google Scholar] [CrossRef]
- Grasser, E.K. Dose-Dependent Heart Rate Responses to Drinking Water: A Randomized Crossover Study in Young, Non-Obese Males. Clin. Auton. Res. 2020, 30, 567–570. [Google Scholar] [CrossRef]
- Brown, C.M.; Barberini, L.; Dulloo, A.G.; Montani, J.-P. Cardiovascular Responses to Water Drinking: Does Osmolality Play a Role? Am. J. Physiol. Regul. Integr. Comp. Physiol. 2005, 289, R1687–R1692. [Google Scholar] [CrossRef] [Green Version]
- Routledge, H.C.; Chowdhary, S.; Coote, J.H.; Townend, J.N. Cardiac Vagal Response to Water Ingestion in Normal Human Subjects. Clin. Sci. 2002, 103, 157–162. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monnard, C.R.; Montani, J.-P.; Grasser, E.K. Short-Term Cardiovascular Responses to Ingestion of Mineral Water in Healthy Non-Obese Adults: Impact of Mineral Components. J. Funct. Foods 2020, 71, 104017. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Berntson, G.G.; Binkley, P.F.; Quigley, K.S.; Uchino, B.N.; Fieldstone, A. Autonomic Cardiac Control. II. Noninvasive Indices and Basal Response as Revealed by Autonomic Blockades. Psychophysiology 1994, 31, 586–598. [Google Scholar] [CrossRef]
- Fei, L.; Copie, X.; Malik, M.; Camm, A.J. Short- and Long-Term Assessment of Heart Rate Variability for Risk Stratification after Acute Myocardial Infarction. Am. J. Cardiol. 1996, 77, 681–684. [Google Scholar] [CrossRef]
- Billman, G.E. The LF/HF Ratio Does Not Accurately Measure Cardiac Sympatho-Vagal Balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millard-Stafford, M.; Snow, T.K.; Jones, M.L.; Suh, H. The Beverage Hydration Index: Influence of Electrolytes, Carbohydrate and Protein. Nutrients 2021, 13, 2933. [Google Scholar] [CrossRef]
- Berry, C.W.; Wolf, S.T.; Murray, B.; Kenney, W.L. Hydration Efficacy of a Milk Permeate-Based Oral Hydration Solution. Nutrients 2020, 12, 1502. [Google Scholar] [CrossRef]
- Stachenfeld, N.S. Sex Hormone Effects on Body Fluid Regulation. Exerc. Sport Sci. Rev. 2008, 36, 152–159. [Google Scholar] [CrossRef] [Green Version]
- Stachenfeld, N.S.; Keefe, D.L. Estrogen Effects on Osmotic Regulation of AVP and Fluid Balance. Am. J. Physiol. Endocrinol. Metab. 2002, 283, E711–E721. [Google Scholar] [CrossRef]
- Stachenfeld, N.S.; Silva, C.; Keefe, D.L.; Kokoszka, C.A.; Nadel, E.R. Effects of Oral Contraceptives on Body Fluid Regulation. J. Appl. Physiol. 1999, 87, 1016–1025. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA) Scientific Opinion on Dietary Reference Values for Water. EFSA J. 2010, 8, 1459. [CrossRef] [Green Version]
- Armstrong, L.E. Bioimpedance Spectroscopy Technique: Intra-, Extracellular, and Total Body Water. Med. Sci. Sports Exerc. 1997, 29, 1657. [Google Scholar] [CrossRef]
- Nakamura, Y.; Yamamoto, Y.; Muraoka, I. Autonomic Control of Heart Rate during Physical Exercise and Fractal Dimension of Heart Rate Variability. J. Appl. Physiol. 1993, 74, 875–881. [Google Scholar] [CrossRef]
- Bernardi, L.; Salvucci, F.; Suardi, R.; Soldá, P.L.; Calciati, A.; Perlini, S.; Falcone, C.; Ricciardi, L. Evidence for an Intrinsic Mechanism Regulating Heart Rate Variability in the Transplanted and the Intact Heart during Submaximal Dynamic Exercise? Cardiovasc. Res. 1990, 24, 969–981. [Google Scholar] [CrossRef]
- Siow, P.C.; Tan, W.S.K.; Henry, C.J. Impact of Isotonic Beverage on the Hydration Status of Healthy Chinese Adults in Air-Conditioned Environment. Nutrients 2017, 9, 242. [Google Scholar] [CrossRef]
- Matthews, E.L.; Hosick, P.A. Bioelectrical Impedance Analysis Does Not Detect an Increase in Total Body Water Following Isotonic Fluid Consumption. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2019, 44, 1116–1120. [Google Scholar] [CrossRef]
- Monnard, C.R.; Grasser, E.K. Water Ingestion Decreases Cardiac Workload Time-Dependent in Healthy Adults with No Effect of Gender. Sci. Rep. 2017, 7, 7939. [Google Scholar] [CrossRef] [Green Version]
- Christiani, M.; Grosicki, G.J.; Flatt, A.A. Cardiac-Autonomic and Hemodynamic Responses to a Hypertonic, Sugar-Sweetened Sports Beverage in Physically Active Men. Appl. Physiol. Nutr. Metab. 2021, 46, 1189–1195. [Google Scholar] [CrossRef]
- Heathers, J.; Quintana, D.; Angus, D.; Krygier, J.; Kemp, A.H.; de Rosnay, M. Water Consumption as a Source of Error in the Measurement of Heart Rate Variability. OSF Preprints 2018. [Google Scholar] [CrossRef]
- Scott, E.M.; Greenwood, J.P.; Vacca, G.; Stoker, J.B.; Gilbey, S.G.; Mary, D.A.S.G. Carbohydrate Ingestion, with Transient Endogenous Insulinaemia, Produces Both Sympathetic Activation and Vasodilatation in Normal Humans. Clin. Sci. 2002, 102, 523–529. [Google Scholar] [CrossRef]
- Welle, S.; Lilavivat, U.; Campbell, R.G. Thermic Effect of Feeding in Man: Increased Plasma Norepinephrine Levels Following Glucose but Not Protein or Fat Consumption. Metabolism 1981, 30, 953–958. [Google Scholar] [CrossRef]
- Kimura, T.; Abe, K.; Ota, K.; Omata, K.; Shoji, M.; Kudo, K.; Matsui, K.; Inoue, M.; Yasujima, M.; Kaoru, Y. Effects of Acute Water Load, Hypertonic Saline Infusion, and Furosemide Administration on Atrial Natriuretic Peptide and Vasopressin Release in Humans. J. Clin. Endocrinol. Metab. 1986, 62, 1003–1010. [Google Scholar] [CrossRef]
- Kasamaki, Y.; Izumi, Y.; Ozawa, Y.; Ohta, M.; Tano, A.; Watanabe, I.; Hirayama, A.; Nakayama, T.; Kawamura, H.; Himit, D.; et al. Relationship between Status of Plasma Atrial Natriuretic Peptide and Heart Rate Variability in Human Subjects. Heart Vessels 2013, 28, 208–214. [Google Scholar] [CrossRef]
- Shirreffs, S.M.; Taylor, A.J.; Leiper, J.B.; Maughan, R.J. Post-Exercise Rehydration in Man: Effects of Volume Consumed and Drink Sodium Content. Med. Sci. Sports Exerc. 1996, 28, 1260–1271. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IB (N = 22) | DW (N = 22) | p-Value | |
|---|---|---|---|
| Height (cm) | |||
| Mean (SD) | 169.1 (±12.59) | 169.1 (±12.59) | |
| Body Mass (kg) | |||
| Mean (SD) | 73.27 (±13.83) | 73.27 (±13.83) | |
| Age (years) | |||
| Mean (SD) | 27.1 (±3.5) | 27.1 (±3.5) | |
| Sex | |||
| Female | 11 (50%) | 11 (50%) | |
| Male | 11 (50%) | 11 (50%) | |
| Arrival USG | |||
| Mean (SD) | 1.016 (±0.008) | 1.013 (±0.009) | 0.1879 |
| Missing | 0 (0%) | 2 (9.1%) | |
| 24h USG | |||
| Mean (SD) | 1.013 (±0.006) | 1.013 (±0.005) | 0.8655 |
| 24h Urine Volume (L) | |||
| Mean (SD) | 2.128 (±1.040) | 2.153 (±1.161) | 0.9402 |
| Arrival Body Mass (kg) | |||
| Mean (SD) | 73.30 (±14.14) | 73.68 (±14.34) | 0.9312 |
| 60 (min) | 120 (min) | 180 (min) | 240 (min) | |||||
|---|---|---|---|---|---|---|---|---|
| IB | DW | IB | DW | IB | DW | IB | DW | |
| (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | |
| BHI | 00A0 | |||||||
| Mean (SD) | 1.05 (±0.23) | 1.00 (±0) | 1.06 (±0.15) | 1.00 (±0) | 1.09 (±0.16) * | 1.00 (±0) | 1.10 (±0.17) * | 1.00 (±0) |
| Urine Output (L) | ||||||||
| Mean (SD) | 0.6157 (±0.1428) | 0.6327 (±0.1478) | 1.043 (±0.1528) | 1.094 (±0.1678) | 1.202 (±0.1788) | 1.292 (±0.1724) | 1.299 (±0.1995) | 1.405 (±0.1939) |
| TBW (L) | ||||||||
| Mean (SD) | 37.59 (±8.43) | 37.19 (±7.77) | 37.54 (±8.22) | 37.02 (±7.65) | 37.37 (±8.20) | 36.93 (±7.48) | 37.30 (±8.25) | 36.79 (±7.64) |
| Missing | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) |
| ICW (L) | ||||||||
| Mean (SD) | 20.88 (±5.27) | 20.69 (±4.98) | 20.85 (±5.19) | 20.60 (±4.90) | 20.79 (±5.18) | 20.59 (±4.78) | 20.76 (±5.20) | 20.51 (±4.89) |
| Missing | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) |
| ECW (L) | ||||||||
| Mean (SD) | 16.71 (±3.47) | 16.49 (±3.11) | 16.69 (±3.35) | 16.42 (±3.08) | 16.58 (±3.33) | 16.34 (±3.04) | 16.54 (±3.37) | 16.28 (±3.08) |
| Missing | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) | 5 (22.7%) |
| 0 (min) | 30 (min) | 60 (min) | 120 (min) | 180 (min) | 240 (min) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IB | DW | IB | DW | IB | DW | IB | DW | IB | DW | IB | DW | |
| (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | (N = 22) | |
| CO (L/min) | ||||||||||||
| Mean (SD) | 4.871 (±0.8707) | 5.061 (±1.028) | 4.929 (±1.020) | 5.000 (±1.078) | 5.005 (±1.028) | 4.895 (±1.094) | 4.886 (±1.017) | 5.025 (±1.275) | 4.719 (±1.055) | 4.763 (±1.138) | 5.289 (±1.216) | 4.825 (±1.040) |
| Missing | 1 (4.5%) | 4 (18.2%) | 5 (22.7%) | 7 (31.8%) | 2 (9.1%) | 2 (9.1%) | 1 (4.5%) | 2 (9.1%) | 1 (4.5%) | 3 (13.6%) | 3 (13.6%) | 2 (9.1%) |
| SV (mL/beat) | ||||||||||||
| Mean (SD) | 80.36 (±14.64) | 85.36 (±21.09) | 77.44 (±16.52) | 83.04 (±16.16) | 85.32 (±17.47) | 84.99 (±22.60) | 87.57 (±17.31) | 87.78 (±22.56) | 84.00 (±16.77) | 81.78 (±18.91) | 93.79 (±26.46) | 82.16 (±17.11) |
| Missing | 1 (4.5%) | 4 (18.2%) | 5 (22.7%) | 7 (31.8%) | 2 (9.1%) | 2 (9.1%) | 1 (4.5%) | 2 (9.1%) | 1 (4.5%) | 3 (13.6%) | 3 (13.6%) | 2 (9.1%) |
| MAP (mmHg) | ||||||||||||
| Mean (SD) | 95.33 (±7.351) | 99.40 (±5.567) | 93.67 (±10.02) | 96.59 (±7.467) | 93.24 (±8.396) | 96.00 (±7.760) | 94.67 (±8.272) | 95.25 (±9.262) | 92.52 (±7.960) | 95.65 (±6.784) | 95.16 (±9.553) | 96.95 (±8.593) |
| Missing | 1 (4.5%) | 2 (9.1%) | 4 (18.2%) | 5 (22.7%) | 1 (4.5%) | 2 (9.1%) | 1 (4.5%) | 2 (9.1%) | 1 (4.5%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) |
| Systole (mmHg) | ||||||||||||
| Mean (SD) | 120.9 (±11.40) | 123.7 (±7.464) | 117.6 (±13.63) | 120.2 (±11.88) | 117.0 (±12.16) | 121.3 (±11.71) | 119.4 (±11.30) | 121.0 (±13.15) | 116.7 (±11.02) | 121.1 (±8.457) | 120.6 (±14.26) | 123.2 (±12.91) |
| Missing | 1 (4.5%) | 2 (9.1%) | 4 (18.2%) | 5 (22.7%) | 1 (4.5%) | 2 (9.1%) | 1 (4.5%) | 2 (9.1%) | 1 (4.5%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) |
| Diastole (mmHg) | ||||||||||||
| Mean (SD) | 73.71 (±5.824) | 78.85 (±6.352) | 73.61 (±7.875) | 76.82 (±4.653) | 73.24 (±6.107) | 74.70 (±5.850) | 73.62 (±6.614) | 73.55 (±6.932) | 71.95 (±7.619) | 74.25 (±6.950) | 73.63 (±6.809) | 74.75 (±6.632) |
| Missing | 1 (4.5%) | 2 (9.1%) | 4 (18.2%) | 5 (22.7%) | 1 (4.5%) | 2 (9.1%) | 1 (4.5%) | 2 (9.1%) | 1 (4.5%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) |
| lnRMSSD | ||||||||||||
| Mean (SD) | 3.862 (±0.5067) | 4.029 (±0.4758) | 3.723 (±0.5523) | 3.938 (±0.5201) | 3.848 (±0.4349) | 3.945 (±0.4407) | 3.984 (±0.4683) | 3.974 (±0.4568) | 4.035 (±0.4520) | 4.029 (±0.4570) | 4.063 (±0.4230) | 3.967 (±0.4618) |
| Missing | 2 (9.1%) | 2 (9.1%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) | 4 (18.2%) | 2 (9.1%) |
| lnHF | ||||||||||||
| Mean (SD) | 6.710 (±1.047) | 6.977 (±0.8894) | 6.342 (±1.119) * | 6.793 (±0.9807) | 6.592 (±0.9440) | 6.666 (±0.9251) | 6.753 (±1.010) | 6.775 (±1.042) | 6.808 (±1.021) | 6.866 (±0.9305) | 6.936 (±0.8913) | 6.812 (±1.081) |
| Missing | 2 (9.1%) | 2 (9.1%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) | 4 (18.2%) | 2 (9.1%) |
| lnLF | ||||||||||||
| Mean (SD) | 6.639 (±0.9908) | 6.883 (±0.9713) | 6.343 (±0.9375) | 6.837 (±0.7925) | 6.454 (±1.055) | 6.473 (±0.9820) | 6.730 (±1.145) | 6.632 (±0.9689) | 6.802 (±0.7407) | 6.902 (±0.8313) | 6.675 (±0.7989) | 6.685 (±0.8903) |
| Missing | 2 (9.1%) | 2 (9.1%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) | 3 (13.6%) | 2 (9.1%) | 4 (18.2%) | 2 (9.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bechke, E.E.; Zaplatosch, M.E.; Choi, J.-Y.; Adams, W.M. Utility of an Isotonic Beverage on Hydration Status and Cardiovascular Alterations. Nutrients 2022, 14, 1286. https://doi.org/10.3390/nu14061286
Bechke EE, Zaplatosch ME, Choi J-Y, Adams WM. Utility of an Isotonic Beverage on Hydration Status and Cardiovascular Alterations. Nutrients. 2022; 14(6):1286. https://doi.org/10.3390/nu14061286
Chicago/Turabian StyleBechke, Emily E., Mitchell E. Zaplatosch, Ji-Yeon Choi, and William M. Adams. 2022. "Utility of an Isotonic Beverage on Hydration Status and Cardiovascular Alterations" Nutrients 14, no. 6: 1286. https://doi.org/10.3390/nu14061286
APA StyleBechke, E. E., Zaplatosch, M. E., Choi, J.-Y., & Adams, W. M. (2022). Utility of an Isotonic Beverage on Hydration Status and Cardiovascular Alterations. Nutrients, 14(6), 1286. https://doi.org/10.3390/nu14061286