
β-Carotene Supplementation and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Collection and Extraction
2.5. Quality Assessment
2.6. Grading of the Evidence
2.7. Statistical Analysis
3. Results
3.1. Study Identification
3.2. Study Characteristics
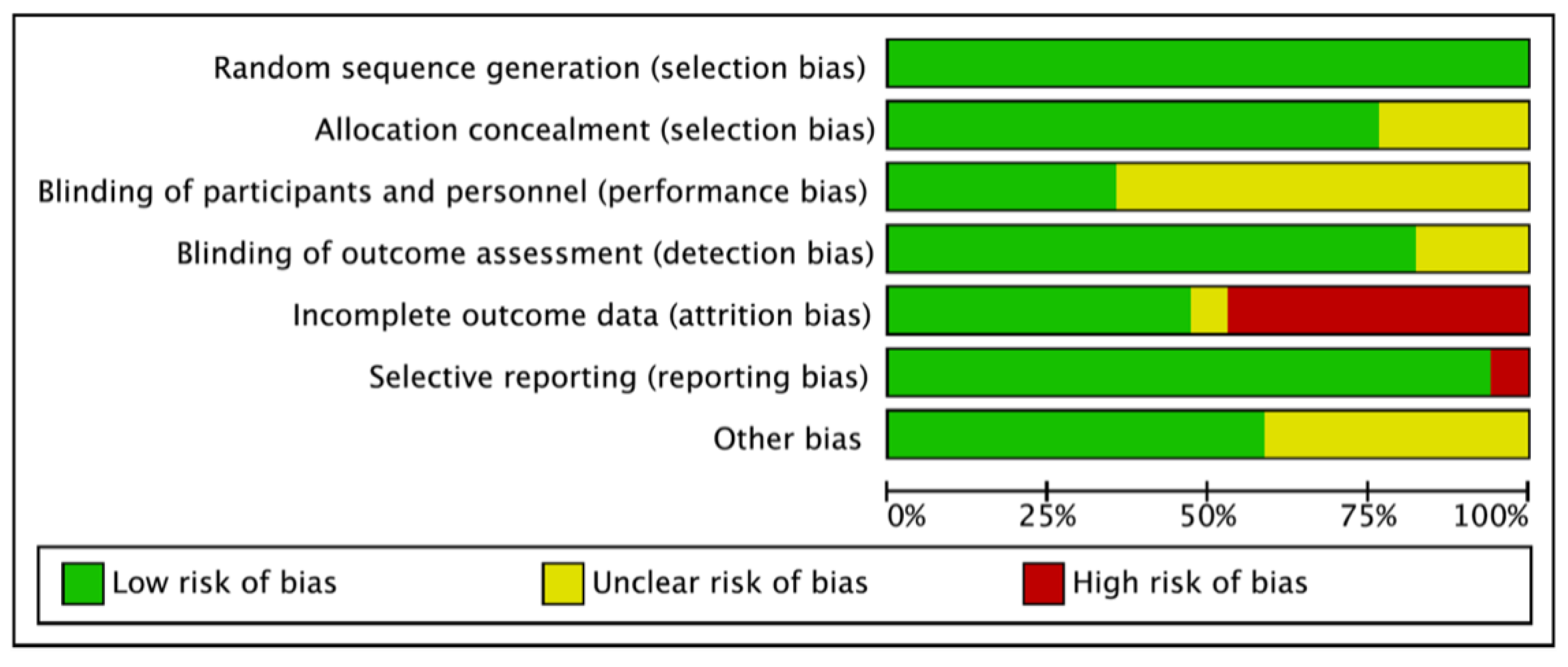
3.3. Risk of Bias
3.4. Incidence
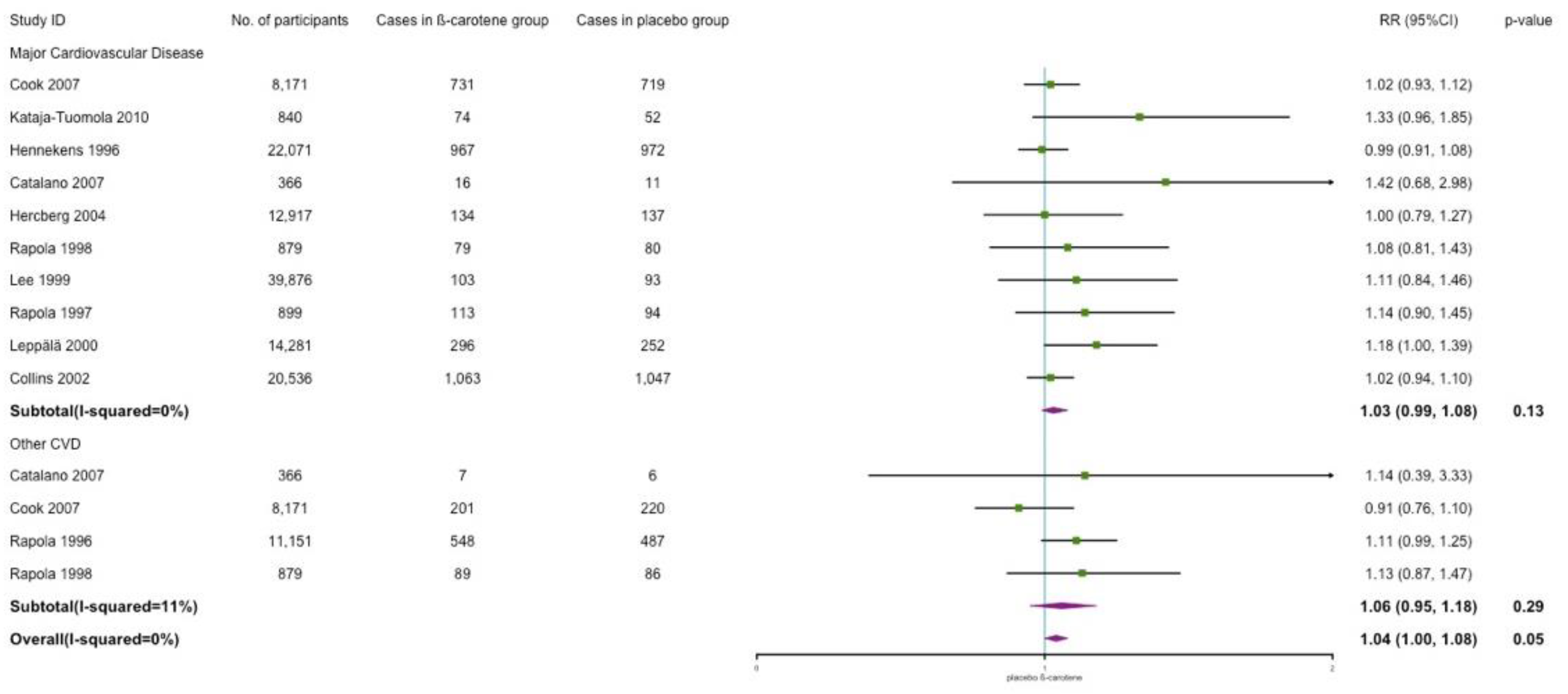
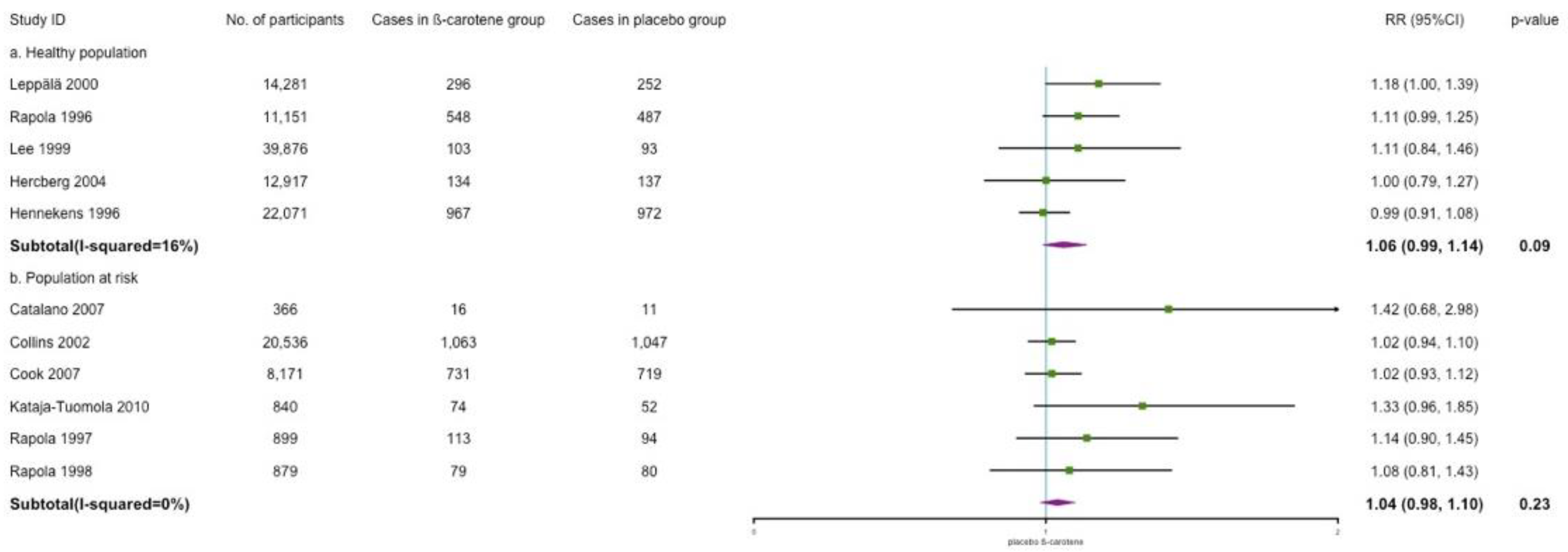
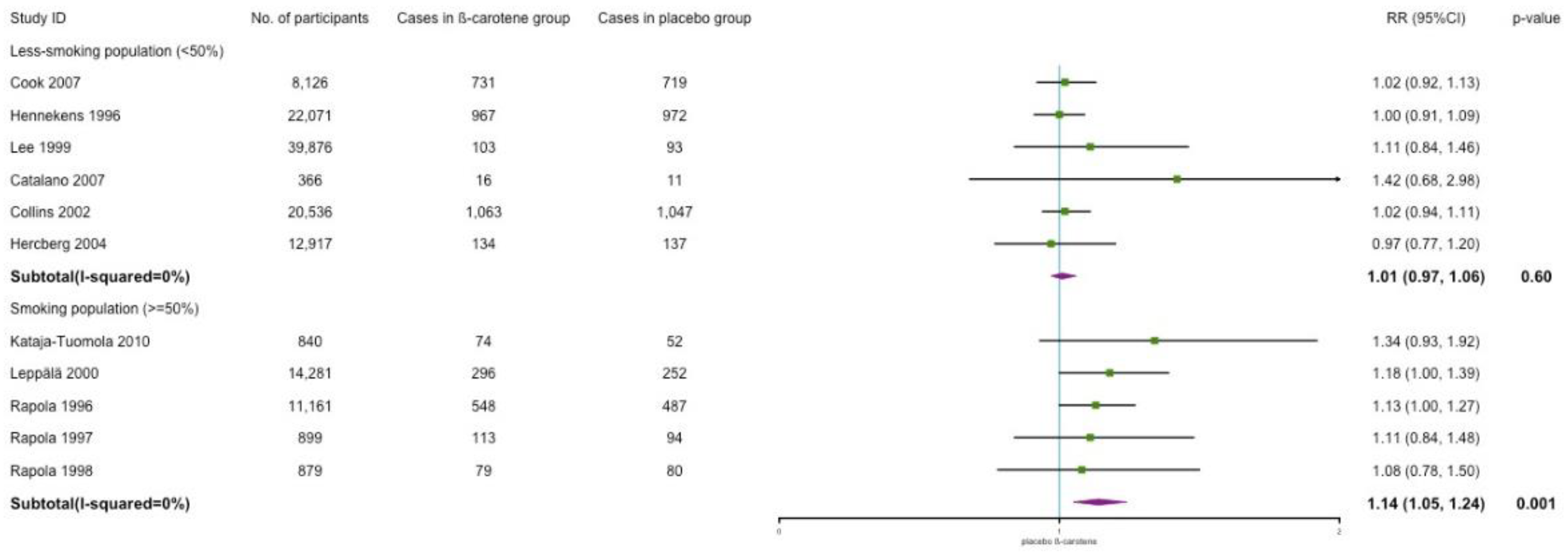
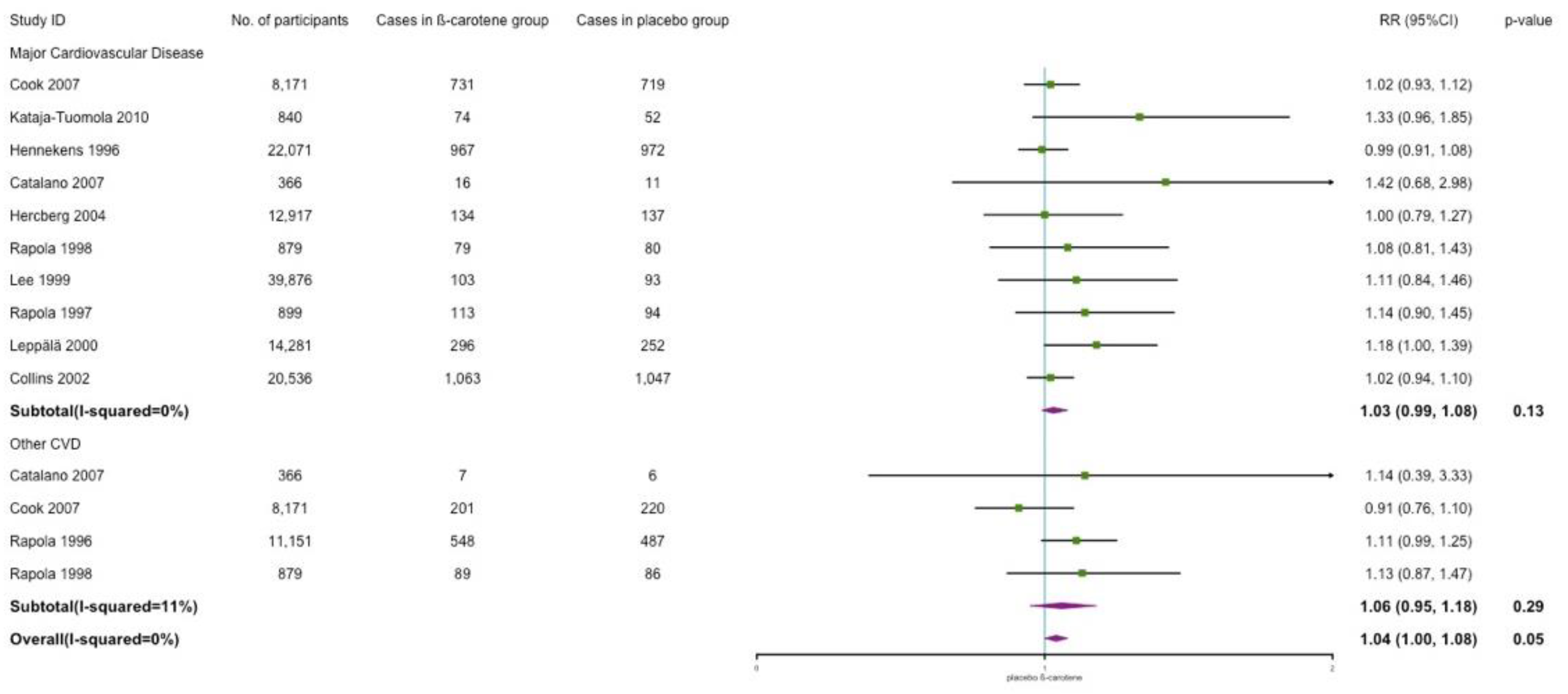
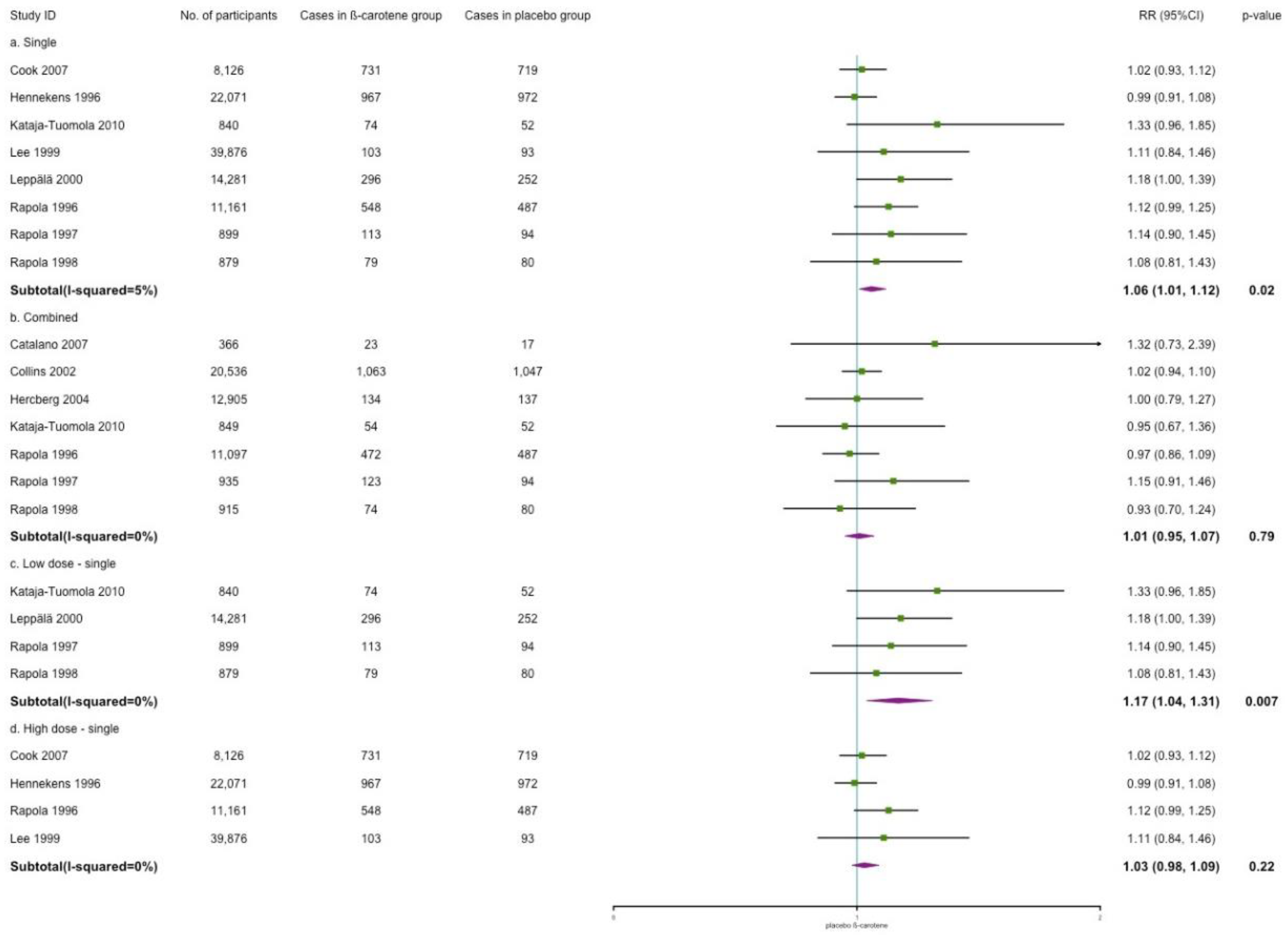
3.4.1. Cardiovascular Disease Incidence
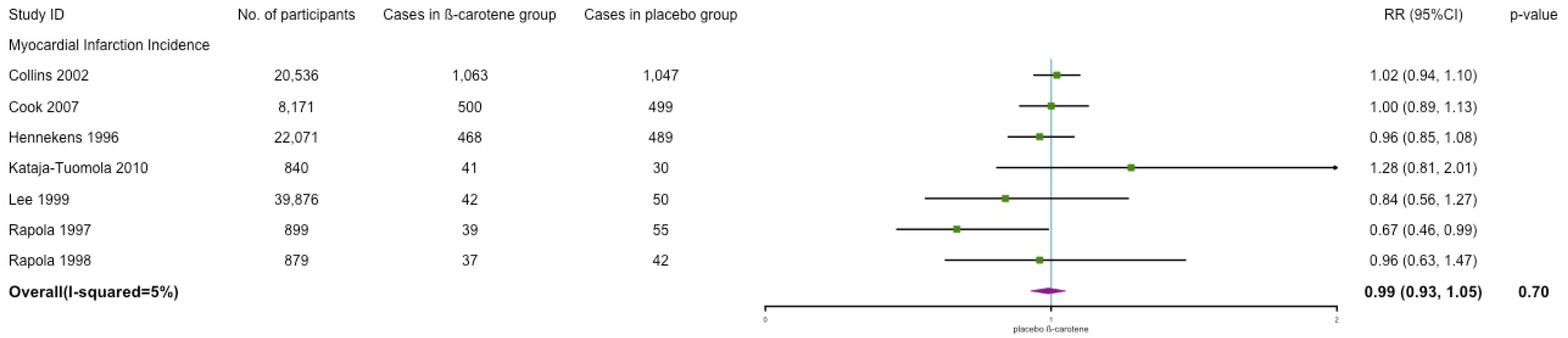
3.4.2. Myocardial Infarction Incidence
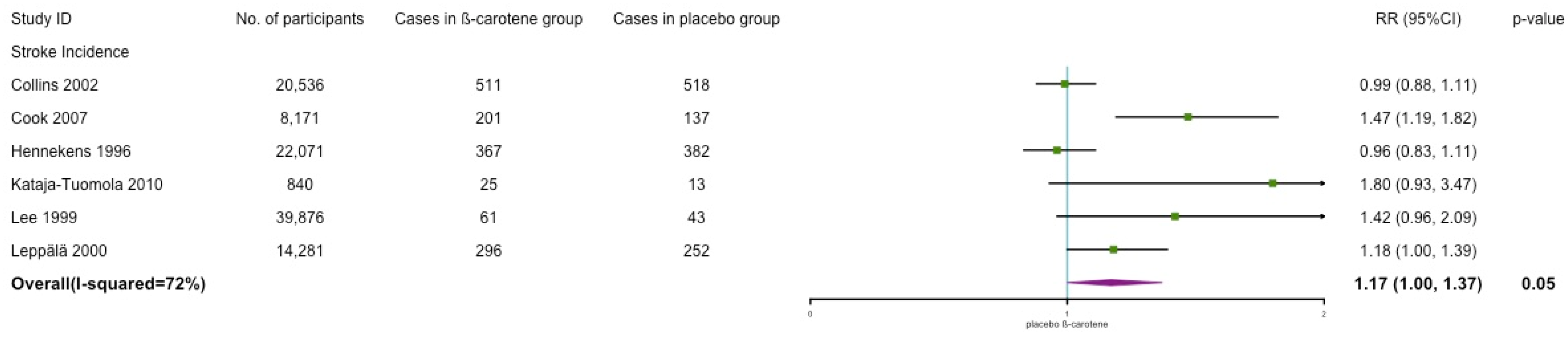
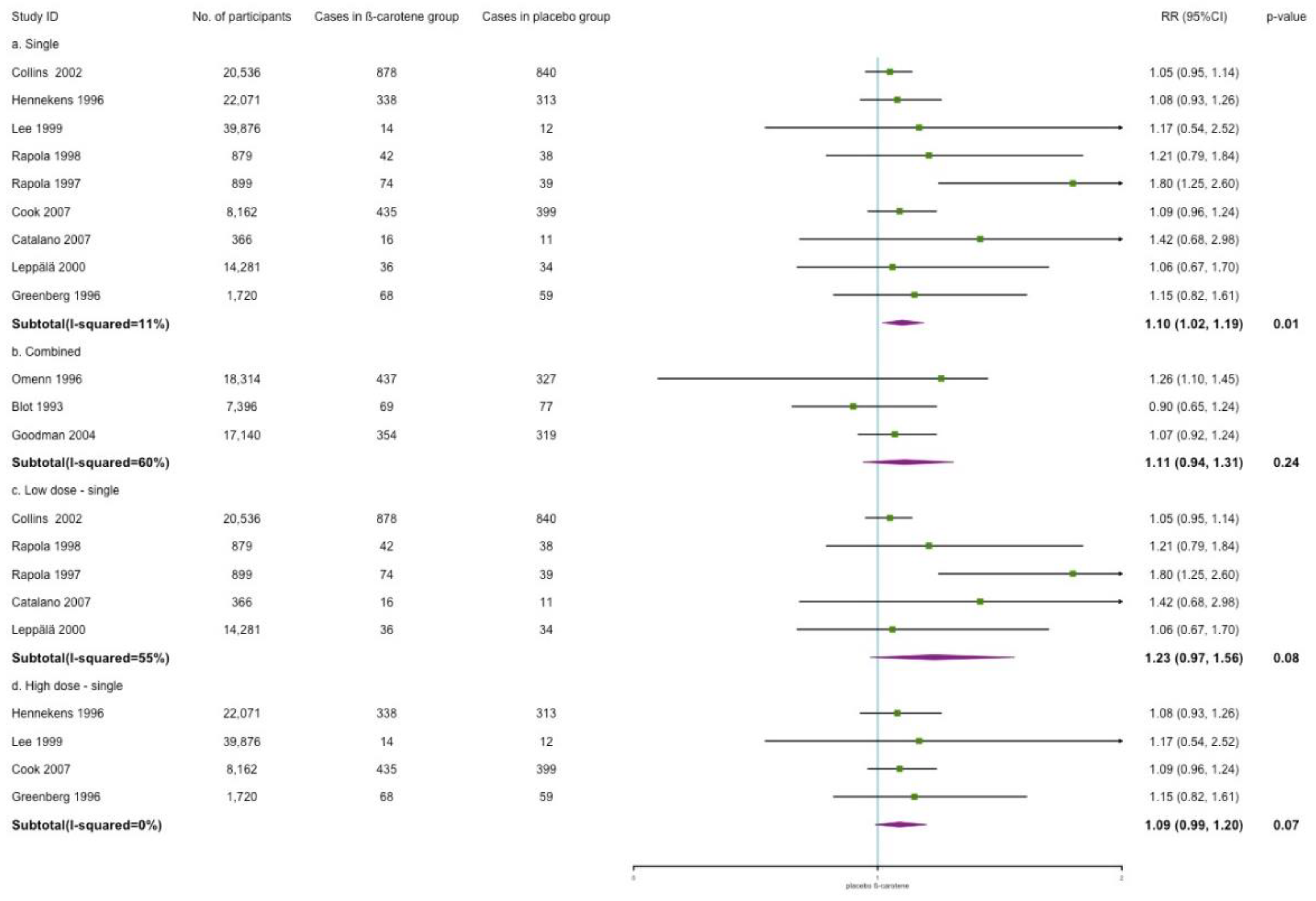
3.4.3. Stroke Incidence
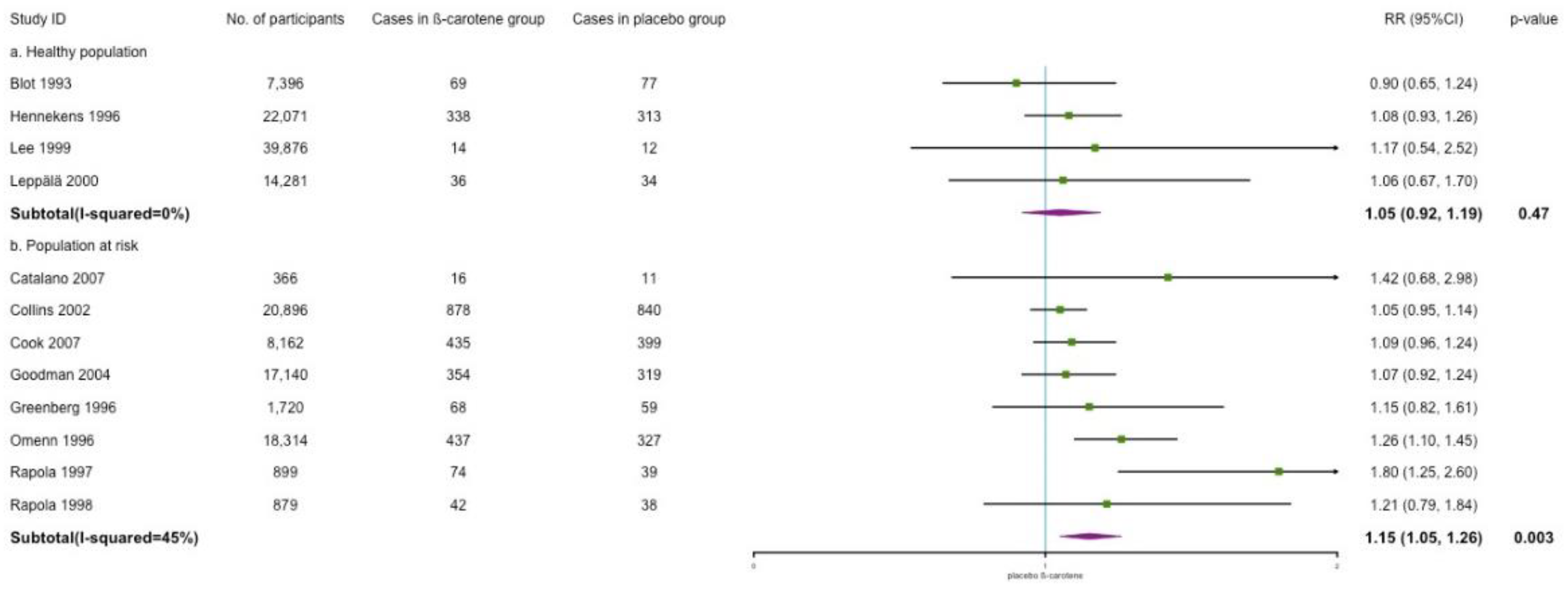
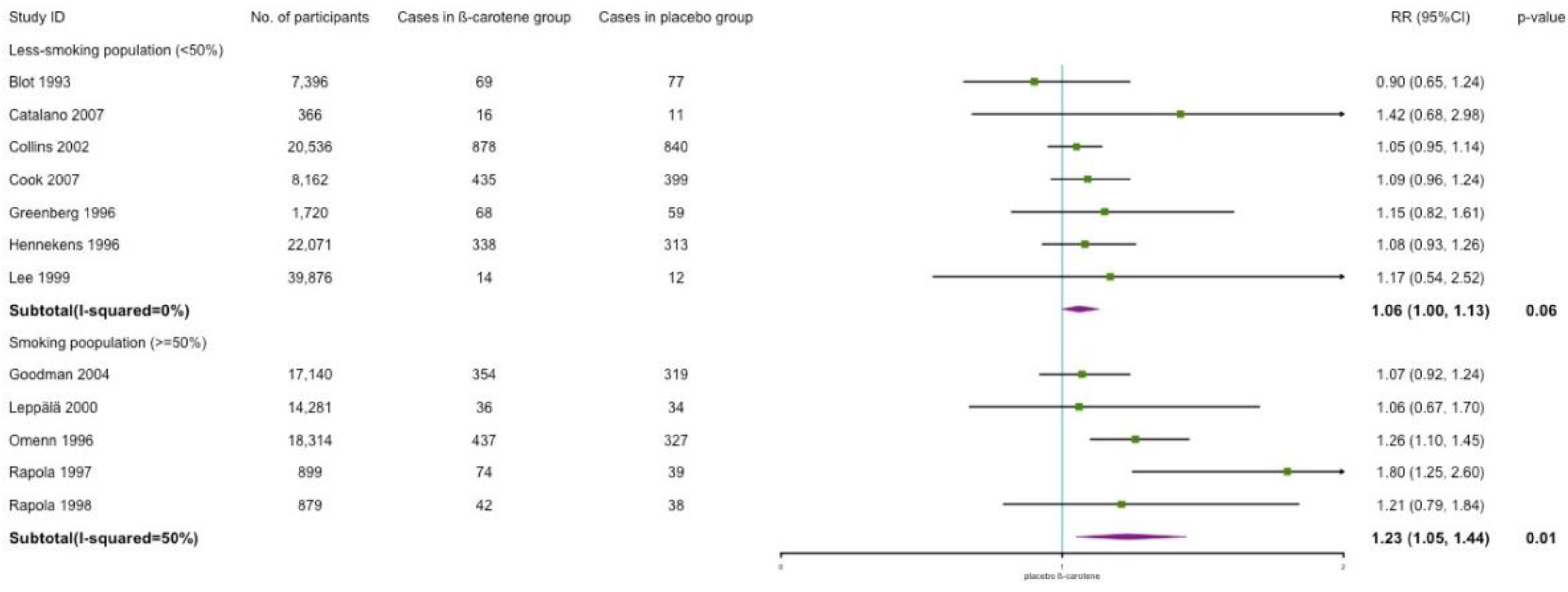
3.5. Mortality
Cardiovascular, All-Cause, and Other Mortality
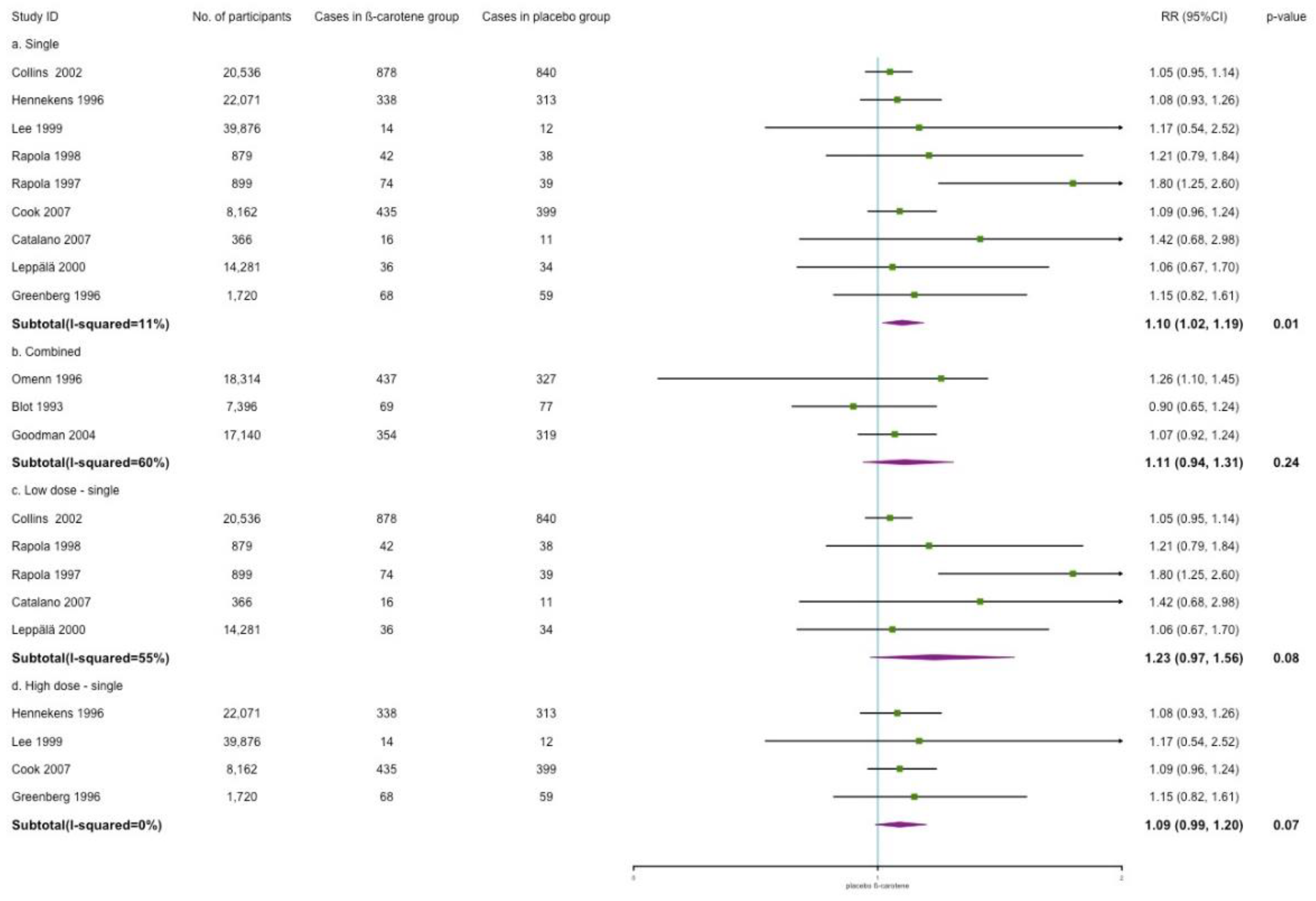
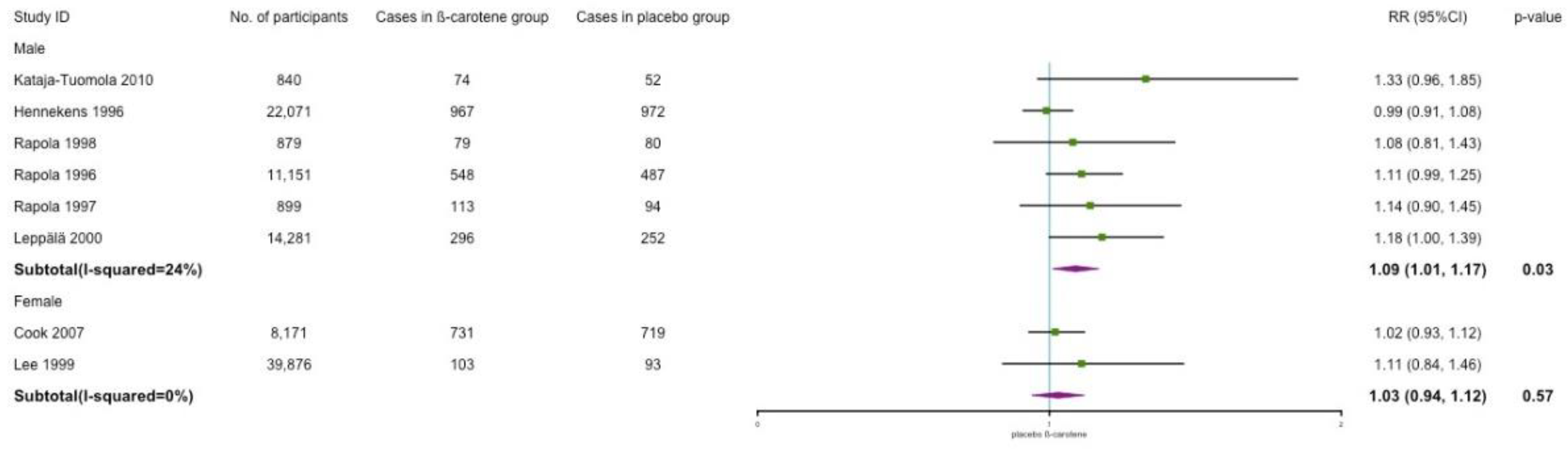
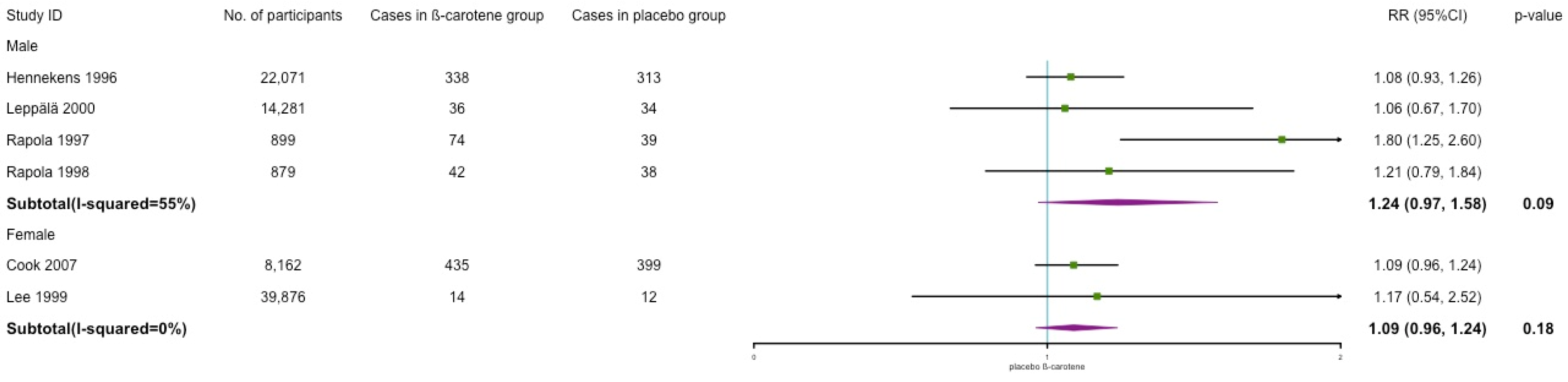
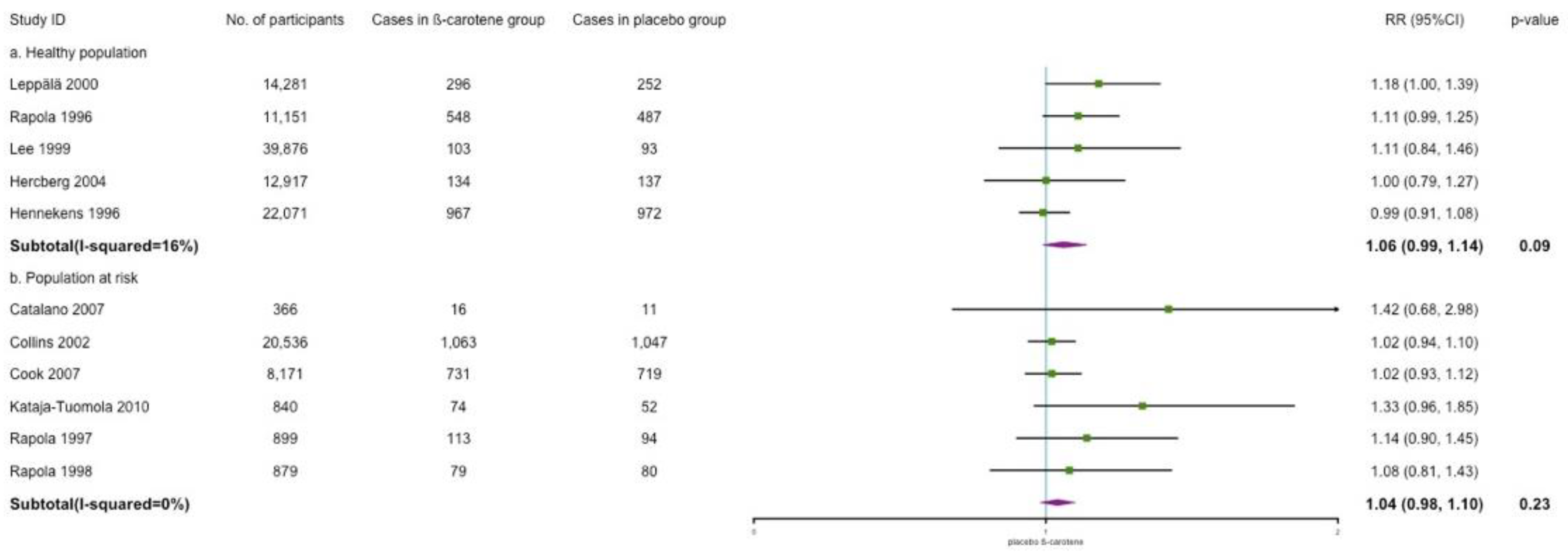
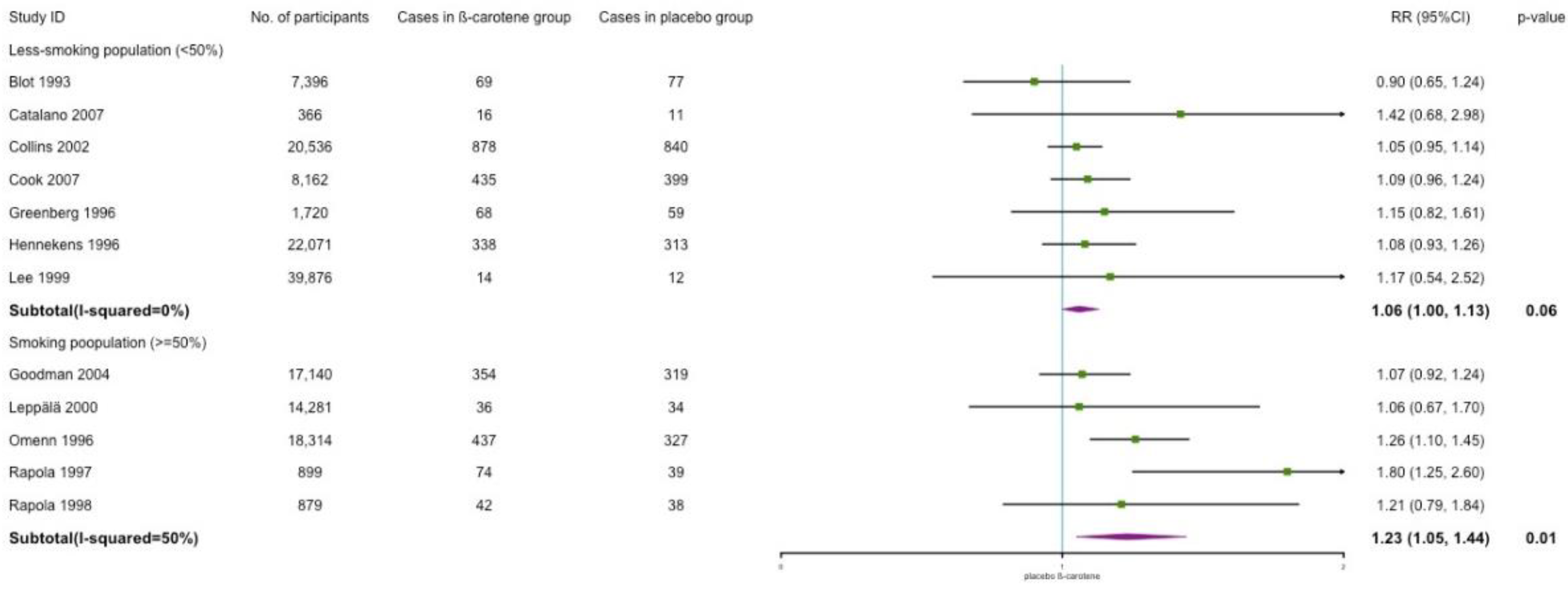
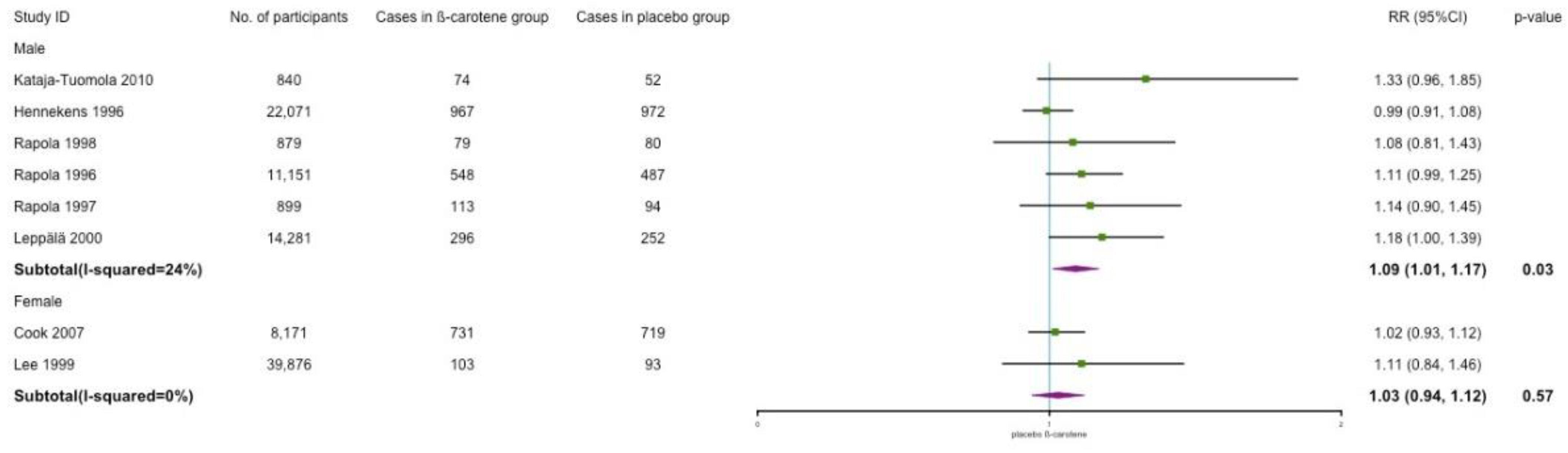
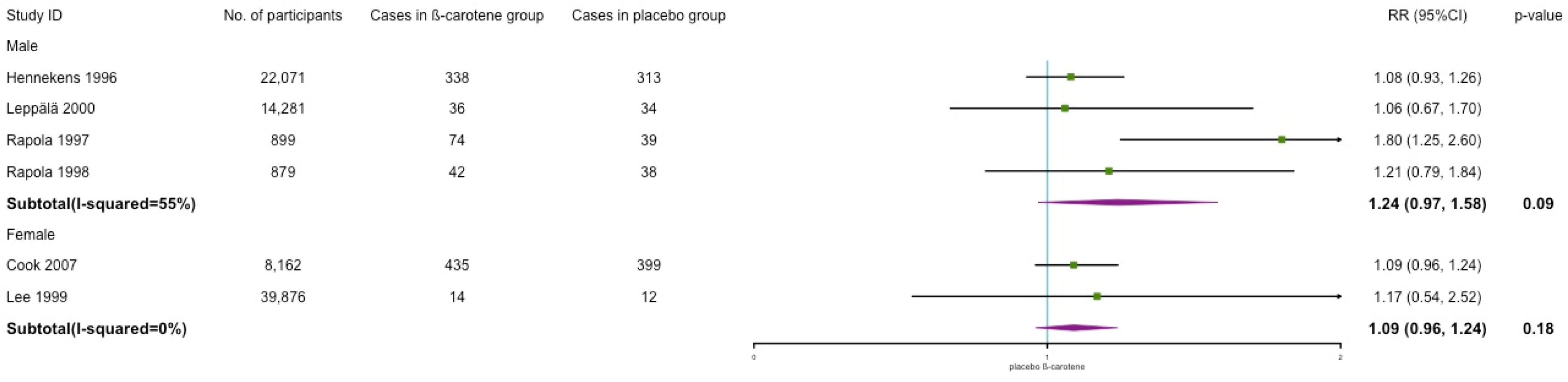
3.6. Subgroup and Sensitivity Analyses
3.7. Publication Bias
4. Discussion
4.1. Effects of β-Carotene on CVD Incidence
4.2. Effects of β-Carotene on CVD Mortality
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CVD | Cardiovascular disease |
| USPSTF | US Preventive Services Task Force |
| RCT | Randomized Controlled Trials |
| RR | Risk Ratio |
| CI | Confidence Interval |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| UL | Tolerable upper intake level |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Keywords |
|---|---|
| 1 | (“beta carotene”(tiab) OR “beta carotene” (mesh) OR “beta-carotene” (tiab) OR “β carotene” (tiab) OR “β-carotene” (tiab)) AND |
| 2 | (“cardiovascular disease *” (tiab) OR “cardiovascular diseases” (mesh) OR CVD (tiab) OR CVDs(tiab) OR angiocardiopathy(tiab) OR angiocardiopathies (tiab) OR “coronary heart disease *” (tiab) OR CHD (tiab) OR “coronary disease *” (tiab) OR “coronary disease” (mesh) OR “coronary artery disease *” (tiab) OR “coronary artery disease” (mesh) OR CAD (tiab) OR “high blood pressure” (tiab) OR hypertension (tiab) OR hypertension (mesh) OR arrhythmia (tiab) OR arrhythmia (tiab) OR “cardiac failure” (tiab) OR “heart failure” (tiab) OR “heart failure”(mesh) OR HF (tiab) OR “viral myocarditis”(tiab) OR VMC(tiab) OR angina (tiab) OR “Angina Pectoris” (tiab) OR “Angina Pectoris” (mesh) OR stenocardia (tiab) OR “angor pectoris” (tiab) OR “rheumatic heart disease *” (tiab) OR “rheumatic heart disease” (mesh) OR “pulmonary heart disease *” (tiab) OR “pulmonary heart disease” (mesh) OR “myocardial infarction” (tiab) OR “myocardial infarction” (mesh)) AND |
| 3 | (“controlled clinical trial” (pt) OR “randomized controlled trial” (pt) OR “clinical trial” (pt) OR random * (tiab) OR trial * (tiab)) |
| Certainty Assessment | No. of Patients | Effect | Certainty | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsistancy | Indirectness | Imprecision | Other Considerations | Experimental | Control | Relative (95% CI) | |
| Major Cardiovascular Disease | ||||||||||
| 10 | Randomized trials | Not serious a | Not serious | Serious c | Not serious | Publicaiton bias strongly suspected d | 3576/60,337 (5.9%) | 3457/60,499 (5.7%) | RR 1.03 (0.99 to 1.08) | ⨁⨁◯◯ Low |
| Myocardial Infarction | ||||||||||
| 7 | Randomized trials | Not serious a | Not serious | Serious c | Not serious | None | 2190/46,643 (4.7%) | 2212/46,629 (4.7%) | RR 0.99 (0.93 to 1.05) | ⨁⨁⨁◯ Moderate |
| Stroke | ||||||||||
| 6 | Randomized trials | Not serious a | Serious b | Serious c | Not serious | None | 1461/52,890 (2.8%) | 1345/52,885 (2.5%) | RR 1.17 (1.00 to 1.37) | ⨁⨁◯◯ Low |
| Other CVD | ||||||||||
| 4 | Randomized trials | Not serious a | Not serious | Serious c | Not serious | None | 845/10,291 (8.2%) | 799/10,276 (7.8%) | RR 1.06 (0.95 to 1.18) | ⨁⨁⨁◯ Moderate |
| CVD Mortality | ||||||||||
| 12 | Randomized trials | Not serious a | Not serious | Not serious | Not serious | None | 2761/76,244 (3.6%) | 2468/75,396 (3.3%) | RR 1.12 (1.04 to 1.19) | ⨁⨁⨁⨁ High |
| All-cause Mortality | ||||||||||
| 6 | Randomized trials | Not serious a | Serious b | Serious c | Not serious | None | 3516/41,836 (8.4%) | 3193/41,105 (7.8%) | RR 1.08 (1.00 to 1.16) | ⨁⨁◯◯ Low |
| Other Mortality | ||||||||||
| 3 | Randomized trials | Not serious | Serious b | Serious c | Not serious | None | 1144/29,200 (3.9%) | 907/28,325 (3.2%) | RR 1.23 (0.98 to 1.53) | ⨁⨁◯◯ Low |


References
- WHO. Cardiovascular Diseases (CVDS). 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 1 February 2022).
- Huang, T.; Yang, B.; Zheng, J.; Li, G.; Wahlqvist, M.L.; Li, D. Cardiovascular disease mortality and cancer incidence in vegetarians: A meta-analysis and systematic review. Ann. Nutr. Metab. 2012, 60, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Kwok, C.S.; Umar, S.; Myint, P.K.; Mamas, M.A.; Loke, Y.K. Vegetarian diet, Seventh Day Adventists and risk of cardiovascular mortality: A systematic review and meta-analysis. Int. J. Cardiol. 2014, 176, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Djoussé, L.; Driver, J.A.; Gaziano, J.M. Relation between modifiable lifestyle factors and lifetime risk of heart failure. Jama 2009, 302, 394–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micha, R.; Peñalvo, J.L.; Cudhea, F.; Imamura, F.; Rehm, C.D.; Mozaffarian, D. Association between dietary factors and mortality from heart disease, stroke, and type 2 diabetes in the United States. Jama 2017, 317, 912–924. [Google Scholar] [CrossRef] [Green Version]
- Sikalidis, A.K.; Kelleher, A.H.; Kristo, A.S. Mediterranean Diet. Encyclopedia 2021, 1, 31. [Google Scholar] [CrossRef]
- Fortmann, S.P.; Burda, B.U.; Senger, C.A.; Lin, J.S.; Whitlock, E.P. Vitamin and mineral supplements in the primary prevention of cardiovascular disease and cancer: An updated systematic evidence review for the US Preventive Services Task Force. Ann. Intern. Med. 2013, 159, 824–834. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Nikolova, D.; Gluud, L.L.; Simonetti, R.G.; Gluud, C. Antioxidant supplements for prevention of mortality in healthy participants and patients with various diseases. Cochrane Database Syst. Rev. 2012, 18, 3. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Boeing, H.; Stelmach-Mardas, M.; Gottschald, M.; Dietrich, S.; Hoffmann, G.; Chaimani, A. Dietary supplements and risk of cause-specific death, cardiovascular disease, and cancer: A systematic review and meta-analysis of primary prevention trials. Adv. Nutr. 2017, 8, 27–39. [Google Scholar] [CrossRef]
- Ye, Y.; Li, J.; Yuan, Z. Effect of antioxidant vitamin supplementation on cardiovascular outcomes: A meta-analysis of randomized controlled trials. PLoS ONE 2013, 8, e56803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, D.J.; Spence, J.D.; Giovannucci, E.L.; Kim, Y.i.; Josse, R.; Vieth, R.; Blanco Mejia, S.; Viguiliouk, E.; Nishi, S.; Sahye-Pudaruth, S.; et al. Supplemental vitamins and minerals for CVD prevention and treatment. J. Am. Coll. Cardiol. 2018, 71, 2570–2584. [Google Scholar] [CrossRef]
- Donhowe, E.G.; Kong, F. Beta-carotene: Digestion, microencapsulation, and in vitro bioavailability. Food Bioprocess Technol. 2014, 7, 338–354. [Google Scholar] [CrossRef]
- Derrick, S.A.; Kristo, A.S.; Reaves, S.K.; Sikalidis, A.K. Effects of Dietary Red Raspberry Consumption on Pre-Diabetes and Type 2 Diabetes Mellitus Parameters. Int. J. Environ. Res. Public Health 2021, 18, 9364. [Google Scholar] [CrossRef]
- Rein, M.J.; Renouf, M.; Cruz-Hernandez, C.; Actis-Goretta, L.; Thakkar, S.K.; da Silva Pinto, M. Bioavailability of bioactive food compounds: A challenging journey to bioefficacy. Br. J. Clin. Pharmacol. 2013, 75, 588–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vivekananthan, D.P.; Penn, M.S.; Sapp, S.K.; Hsu, A.; Topol, E.J. Use of antioxidant vitamins for the prevention of cardiovascular disease: Meta-analysis of randomised trials. Lancet 2003, 361, 2017–2023. [Google Scholar] [CrossRef]
- Leppälä, J.M.; Virtamo, J.; Fogelholm, R.; Albanes, D.; Taylor, P.R.; Heinonen, O.P. Vitamin E and beta carotene supplementation in high risk for stroke: A subgroup analysis of the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study. Arch. Neurol. 2000, 57, 1503–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kataja-Tuomola, M.K.; Kontto, J.P.; Männistö, S.; Albanes, D.; Virtamo, J.R. Effect of alpha-tocopherol and beta-carotene supplementation on macrovascular complications and total mortality from diabetes: Results of the ATBC Study. Ann. Med. 2010, 42, 178–186. [Google Scholar] [CrossRef]
- Rapola, J.M.; Virtamo, J.; Haukka, J.K.; Heinonen, O.P.; Albanes, D.; Taylor, P.R.; Huttunen, J.K. Effect of vitamin E and beta carotene on the incidence of angina pectoris: A randomized, double-blind, controlled trial. Jama 1996, 275, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Rapola, J.; Virtamo, J.; Ripatti, S.; Haukka, J.; Huttunen, J.; Albanes, D.; Taylor, P.; Heinonen, O. Effects of α tocopherol and β carotene supplements on symptoms, progression, and prognosis of angina pectoris. Heart 1998, 79, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Rapola, J.M.; Virtamo, J.; Ripatti, S.; Huttunen, J.K.; Albanes, D.; Taylor, P.R.; Heinonen, O.P. Randomised trial of α-tocopherol and β-carotene supplements on incidence of major coronary events in men with previous myocardial infarction. Lancet 1997, 349, 1715–1720. [Google Scholar] [CrossRef] [Green Version]
- Virtamo, J.; Pietinen, P.; Huttunen, J.K.; Korhonen, P.; Malila, N.; Virtanen, M.J.; Albanes, D.; Taylor, P.R.; Albert, P. Incidence of cancer and mortality following alpha-tocopherol and beta-carotene supplementation: A postintervention follow-up. Jama 2003, 290, 476–485. [Google Scholar] [PubMed] [Green Version]
- Lee, I.M.; Cook, N.R.; Manson, J.E.; Buring, J.E.; Hennekens, C.H. β-Carotene supplementation and incidence of cancer and cardiovascular disease: The Women’s Health Study. J. Natl. Cancer Inst. 1999, 91, 2102–2106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, N.R.; Albert, C.M.; Gaziano, J.M.; Zaharris, E.; MacFadyen, J.; Danielson, E.; Buring, J.E.; Manson, J.E. A randomized factorial trial of vitamins C and E and beta carotene in the secondary prevention of cardiovascular events in women: Results from the Women’s Antioxidant Cardiovascular Study. Arch. Intern. Med. 2007, 167, 1610–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hercberg, S.; Galan, P.; Preziosi, P.; Bertrais, S.; Mennen, L.; Malvy, D.; Roussel, A.M.; Favier, A.; Briançon, S. The SU. VI. MAX Study: A randomized, placebo-controlled trial of the health effects of antioxidant vitamins and minerals. Arch. Intern. Med. 2004, 164, 2335–2342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Group, C.L.I.P.S.C. Prevention of serious vascular events by aspirin amongst patients with peripheral arterial disease: Randomized, double-blind trial. J. Intern. Med. 2007, 261, 276–284. [Google Scholar]
- Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of antioxidant vitamin supplementation in 20,536 high-risk individuals: A randomised placebo-controlled trial. Lancet 2002, 360, 23–33. [Google Scholar] [CrossRef]
- Omenn, G.S.; Goodman, G.E.; Thornquist, M.D.; Balmes, J.; Cullen, M.R.; Glass, A.; Keogh, J.P.; Meyskens, F.L., Jr.; Valanis, B.; Williams, J.H., Jr.; et al. Effects of a combination of beta carotene and vitamin A on lung cancer and cardiovascular disease. N. Engl. J. Med. 1996, 334, 1150–1155. [Google Scholar] [CrossRef] [Green Version]
- Goodman, G.E.; Thornquist, M.D.; Balmes, J.; Cullen, M.R.; Meyskens Jr, F.L.; Omenn, G.S.; Valanis, B.; Williams Jr, J.H. The Beta-Carotene and Retinol Efficacy Trial: Incidence of lung cancer and cardiovascular disease mortality during 6-year follow-up after stopping β-carotene and retinol supplements. J. Natl. Cancer Inst. 2004, 96, 1743–1750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blot, W.J.; Li, J.Y.; Taylor, P.R.; Guo, W.; Dawsey, S.; Wang, G.Q.; Yang, C.S.; Zheng, S.F.; Gail, M.; Li, G.Y.; et al. Nutrition intervention trials in Linxian, China: Supplementation with specific vitamin/mineral combinations, cancer incidence, and disease-specific mortality in the general population. JNCI J. Natl. Cancer Inst. 1993, 85, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Hennekens, C.H.; Buring, J.E.; Manson, J.E.; Stampfer, M.; Rosner, B.; Cook, N.R.; Belanger, C.; LaMotte, F.; Gaziano, J.M.; Ridker, P.M.; et al. Lack of effect of long-term supplementation with beta carotene on the incidence of malignant neoplasms and cardiovascular disease. N. Engl. J. Med. 1996, 334, 1145–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, E.R.; Baron, J.A.; Karagas, M.R.; Stukel, T.A.; Nierenberg, D.W.; Stevens, M.M.; Mandel, J.S.; Haile, R.W. Mortality associated with low plasma concentration of beta carotene and the effect of oral supplementation. Jama 1996, 275, 699–703. [Google Scholar] [CrossRef]
- Shah, R.S.; Cole, J.W. Smoking and stroke: The more you smoke the more you stroke. Expert Rev. Cardiovasc. Ther. 2010, 8, 917–932. [Google Scholar] [CrossRef] [PubMed]
- Burton, G.W.; Ingold, K. Beta-carotene: An unusual type of lipid antioxidant. Science 1984, 224, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Truscott, T. β-Carotene and disease: A suggested pro-oxidant and anti-oxidant mechanism and speculations concerning its role in cigarette smoking. J. Photochem. Photobiol. B Biol. 1996, 35, 233–235. [Google Scholar] [CrossRef]
- Palozza, P. Prooxidant actions of carotenoids in biologic systems. Nutr. Rev. 1998, 56, 257–265. [Google Scholar] [CrossRef]
- Andersen, H.R.; Andersen, O. Effects of dietary α-tocopherol and β-carotene on lipid peroxidation induced by methyl mercuric chloride in mice. Pharmacol. Toxicol. 1993, 73, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Lomnitski, L.; Bergman, M.; Schön, I.; Grossman, S. The effect of dietary vitamin E and ß-carotene on oxidation processes in the rat testis. Biochim. Biophys. Acta (BBA)-Lipids Lipid Metab. 1991, 1082, 101–107. [Google Scholar] [CrossRef]
- Stewart, C.; Christian, P.; Katz, J.; Schulze, K.; Wu, L.; LeClerq, S.; Shakya, T.; Khatry, S.; West, K. Maternal supplementation with vitamin A or β-carotene and cardiovascular risk factors among pre-adolescent children in rural Nepal. J. Dev. Orig. Health Dis. 2010, 1, 262–270. [Google Scholar] [CrossRef]
- CNS. Chinese Dietary Reference Intakes (2013); Science Press: Beijing, China, 2014. [Google Scholar]
- Trumbo, P.; Yates, A.A.; Schlicker, S.; Poos, M. Dietary reference intakes: Vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. J. Am. Diet. Assoc. 2001, 101, 294–301. [Google Scholar] [CrossRef]


| First Author | Study | Country of Origin | Sample Size | Population | Mean Age, y | Health Status | Treatment Regimen | Health Outcome | Follow-Up, y |
|---|---|---|---|---|---|---|---|---|---|
| Leppälä et al. (2000) [16] | Alpha Tocopherol, Beta Carotene Cancer Prevention (ATBC) Study | Finland | 28,519 | Current male smokers (≥5 cigarettes/d) | 50–69 | Stroke-free at baseline | 50 mg/d of α-Tocopherol (Vitamin E), 20 mg/d of β-carotene, both, or placebo | Total stroke, subarachnoid hemorrhage, intracerebral hemorrhage, cerebral infraction | 6.0 |
| Kataja-Tuomola et al.(2010) [17] | ATBC Study | Finland | 1700 | Current male smokers (≥5 cigarettes/d) | 58 | With type 2 diabetes | As described above | Total macrovascular outcomes, major coronary event, total stroke, peripheral arterial disease, total mortality | 19 |
| Rapola et al. (1996) [18] | ATBC Study | Finland | 22,269 | Current male smokers (≥5 cigarettes/d) | 57 | Free of coronary heart disease | As described above | Angina pectoris | 4.7 |
| Rapola et al. (1998) [19] | ATBC Study | Finland | 1795 | Current male smokers (≥5 cigarettes/d) | 58.8 | With angina pectoris at baseline, smoked 20 cigarettes a day | As described above | Recurrences of angina pectoris, major coronary events | 4–5.5 |
| Rapola et al. (1997) [20] | ATBC Study | Finland | 1862 | Current male smokers (≥5 cigarettes/d) | 59–60 | With previous myocardial infarction | As described above | Major coronary events, non-fatal myocardial infarction | 5.3 |
| Virtamo et al. (2003) [21] | ATBC Study | Finland | 25,563 | Current male smokers (≥5 cigarettes/d) | 63.5 | Participants who were still alive by 30 April 1993 | As described above | Cancer incidence, cause-specific mortality, total mortality | 6–8 |
| Lee et al. (1999) [22] | Women’s Health Study | United States | 39,876 | Female health professionals | ≥45 | Apparently healthy | Given on alternate days, 100 mg of aspirin, or 600 IU of vitamin E, or 50 mg of β-carotene | Myocardial infarction, stroke, death from cardiovascular causes, all-cause death | 4.1 |
| Cook et al. (2007) [23] | Women’s Antioxidant Cardiovascular Study | United States | 8171 | Female health professionals | ≥40 | With a history of CVD or ≥3 CVD risk factors | Vitamin C (500 mg/d), vitamin E (600 IU every other day), β-carotene (50 mg every other day), or placebo | Myocardial infarction, coronary revascularization procedures, coronary heart disease, stroke, transient ischemic attack, CVD death | 9.4 |
| Hercberg et al. (2004) [24] | SU.VI.MAX Study | France | 13,017 | French adult volunteers | 49 | Free from diseases | A daily combined capsule of 120 mg of ascorbic acid, 30 mg of vitamin E, 6 mg of β-carotene, 100 g of selenium, and 20 mg of zinc, or a placebo | Cancer incidence, ischemic cardiovascular disease, mortality | 7.5 |
| Catalano et al. (2007) [25] | Critical Leg Ischemia Prevention Study (CLIPS) Group | Italy | 366 | Outpatients | 66 | Peripheral arterial disease | Oral aspirin (100 mg/d); oral antioxidant vitamins (600 mg vitamin E, 250 mg vitamin C and 20 mg β-carotene daily); both or neither (placebo) | Major vascular event, critical limb ischemia | 2 |
| Collins et al. (2002) [26] | Heart Protection Study Collaborative Group | United Kingdom | 20,536 | Patients from 69 hospitals | 40–80 | Coronary disease, other occlusive arterial disease, or diabetes | Antioxidant vitamins (600 mg synthetic vitamin E, 250 mg vitamin C, and 20 mg β-carotene daily) or placebo | Major coronary event, major vascular event | 5 |
| Omenn et al. (1996) [27] | Beta-Carotene and Retinol Efficacy Trial (CARET) | United States | 18,314 | Smokers, former smokers, and workers exposed to asbestos | 57–58 | At least 15 years exposure to asbestos, asbestos-related lung disease, or 5-year work in high-risk trades | A combination of 30 mg of β-carotene per day and 25,000 IU of retinol (vitamin A) | CVD death, all-cause death, lung cancer death | 4 |
| Goodman et al. (2004) [28] | CARET | United States | 18,140 | As described above | 62 | Postintervention | As described above | CVD death, all-cause death, lung cancer death, other-cause death | 6 |
| Blot et al. (1993) [29] | Linxian Study | China | 29,584 | Residents in Linxian communes | 40–69 | No debilitating diseases or prior esophageal or stomach cancer | Retinol and zinc; riboflavin and niacin; vitamin C and molybdenum; β-carotene (15 mg), vitamin E (30 mg), and selenium (50 µg) | Cerebrovascular disease death, cancer death, total death | 5.25 |
| Hennekens et al. (1996) [30] | Physicians’ Health Study | United States | 22,071 | Male physicians | 40–84 | No history of cancer (except nonmelanoma skin cancer), myocardial infarction, stroke, or transient cerebral ischemia | Aspirin (325 mg on alternate days) plus β-carotene placebo, β-carotene (50 mg on alternate days) plus aspirin placebo, both active agents, or both placebos | Myocardial infarction, stroke, all important cardiovascular events, malignant neoplasm | 12 |
| Greenberg et al. (1996) [31] | Skin Cancer Prevention Study | United Kingdom | 1720 | Treated patients | 63.2 | At least one biopsy-proved basal cell or squamous cell skin cancer treated | 50 mg of β-carotene or placebo | CVD death, cancer death, all death | 8.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Zhang, Y.; Na, X.; Zhao, A. β-Carotene Supplementation and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2022, 14, 1284. https://doi.org/10.3390/nu14061284
Yang J, Zhang Y, Na X, Zhao A. β-Carotene Supplementation and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2022; 14(6):1284. https://doi.org/10.3390/nu14061284
Chicago/Turabian StyleYang, Jiaqi, Yulin Zhang, Xiaona Na, and Ai Zhao. 2022. "β-Carotene Supplementation and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 14, no. 6: 1284. https://doi.org/10.3390/nu14061284
APA StyleYang, J., Zhang, Y., Na, X., & Zhao, A. (2022). β-Carotene Supplementation and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients, 14(6), 1284. https://doi.org/10.3390/nu14061284