
Today’s Mediterranean Diet in Greece: Findings from the National Health and Nutrition Survey—HYDRIA (2013–2014)



Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Energy Intake
3.2. Macronutrients Intake
3.3. Foods Intake
3.4. Adherence to the Greek Traditional Mediterranean Diet
4. Discussion
4.1. Comparison with Nutrient Reference Values
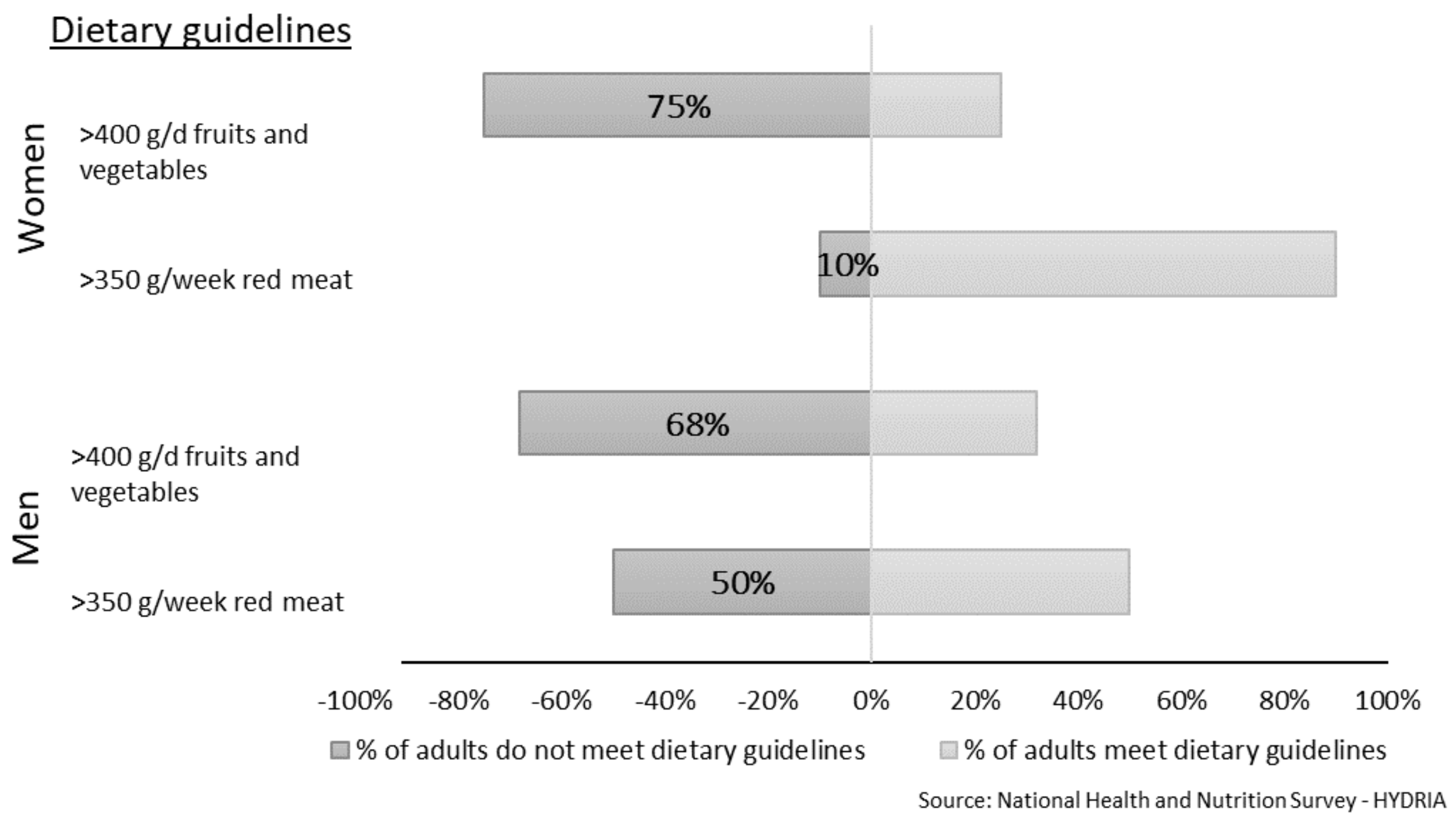
4.2. Comparison with Dietary Food Guidelines
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. European Food and Nutrition Action Plan 2015. WHO Regional Office for Europe: Copenhagen, Denmark, 2015. Available online: https://www.euro.who.int/__data/assets/pdf_file/0003/294474/European-Food-Nutrition-Action-Plan-20152020-en.pdf (accessed on 13 September 2021).
- Rippin, H.; Hutchinson, J.; Evans, C.; Jewell, J.; Breda, J.; Cade, J. National nutrition surveys in Europe: A review on the current status in the 53 countries of the WHO European region. Food Nutr. Res. 2018, 62, 62. [Google Scholar] [CrossRef] [PubMed]
- Hellenic Health Foundation. HYDRIA. Programme and targeted action on the diet and health of the Greek population: Development and implementation of methodology and documentation. 2017. Available online: http://www.hhf-greece.gr/media/projects/hydria-results-eng.pdf (accessed on 16 September 2021).
- Martimianaki, G.; Naska, A.; Papatesta, M.E.; Peppa, E.; Orfanos, P.; Trichopoulou, A. Methods and introductory results of the Greek national health and nutrition survey—HYDRIA. Epidemiol. Biostat. Public Health 2018, 15, 2. Available online: https://riviste.unimi.it/index.php/ebph/article/view/17382/15302 (accessed on 9 January 2022).
- Karageorgou, D.; Magriplis, E.; Bakogianni, I.; Mitsopoulou, A.V.; Dimakopoulos, I.; Micha, R.; Michas, G.; Ntouroupi, T.; Tsaniklidou, S.M.; Argyri, K.; et al. Dietary patterns and cardiovascular disease in Greek adults: The Hellenic National Nutrition and Health Survey (HNNHS). Nutr. Metab. Cardiovasc. Dis. 2020, 30, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Karageorgou, D.; Magriplis, E.; Mitsopoulou, A.; Dimakopoulos, I.; Bakogianni, I.; Micha, R.; Michas, G.; Chourdakis, M.; Ntouroupi, T.; Tsaniklidou, S.; et al. Dietary patterns and lifestyle characteristics in adults: Results from the Hellenic National Nutrition and Health Survey (HNNHS). Public Health 2019, 171, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Magriplis, E.; Contributors, H.; Dimakopoulos, I.; Karageorgou, D.; Mitsopoulou, A.-V.; Bakogianni, I.; Micha, R.; Michas, G.; Ntouroupi, T.; Tsaniklidou, S.-M.; et al. Aims, design and preliminary findings of the Hellenic National Nutrition and Health Survey (HNNHS). BMC Med. Res. Methodol. 2019, 19, 1–13. [Google Scholar] [CrossRef]
- Touloumi, G.; Karakatsani, A.; Karakosta, A.; Sofianopoulou, E.; Koustenis, P.; Gavana, M.; Alamanos, Y.; Kantzanou, M.; Konstantakopoulos, G.; Chryssochoou, X.; et al. National Survey of Morbidity and Risk Factors (EMENO): Protocol for a Health Examination Survey Representative of the Adult Greek Population. JMIR Res. Protoc. 2019, 8, e10997. [Google Scholar] [CrossRef]
- Touloumi, G.; on behalf of the EMENO study group; Karakosta, A.; Kalpourtzi, N.; Gavana, M.; Vantarakis, A.; Kantzanou, M.; Hajichristodoulou, C.; Chlouverakis, G.; Tryp-sianis, G.; et al. High prevalence of cardiovascular risk factors in adults living in Greece: The EMENO National Health Examination Survey. BMC Public Health 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Makrilakis, K.; Kalpourtzi, N.; Ioannidis, I.; Iraklianou, S.; Raptis, A.; Sotiropoulos, A.; Gavana, M.; Vantarakis, A.; Kantzanou, M.; Hadjichristodoulou, C.; et al. Prevalence of diabetes and pre-diabetes in Greece. Results of the First National Survey of Morbidity and Risk Factors (EMENO) study. Diabetes Res. Clin. Pr. 2021, 172, 108646. [Google Scholar] [CrossRef]
- Trichopoulou, A.O.P.; Valanou, E.; Martimianaki, G.; Peppa, E.; Androulidaki, A.; Anifantis, E.; Katsoulis, M.; Kritikou, M.; Pantzarlis, E.; Vidalis, P.; et al. The EFSA-funded collection of dietary and related data in the general population aged 10–74 years in Greece. EFSA Supporting Publ. 2018, 15, 1499E. [Google Scholar]
- Valanou, E.; Naska, A.; Barbouni, A.; Katsoulis, M.; Peppa, E.; Vidalis, P.; Trichopoulou, A. Evaluation of food photographs assessing the dietary intake of children up to 10 years old. Public Health Nutr. 2018, 21, 888–895. [Google Scholar] [CrossRef]
- Skourlis, N.; Patsis, I.; Martimianaki, G.; Peppa, E.; Trichopoulou, A.; Katsouyanni, K. Changes in the Dietary Habits of the Greek EPIC Cohort Participants during a 14-Year Follow-Up Period (1997–2011). Nutrients 2020, 12, 2148. [Google Scholar] [CrossRef] [PubMed]
- Bousiou, A.; Konstantopoulou, K.; Martimianaki, G.; Peppa, E.; Trichopoulou, A.; Polychronopoulou, A.; Halazonetis, D.J.; Schimmel, M.; Kossioni, A.E. Oral factors and adherence to Mediterranean diet in an older Greek population. Aging Clin. Exp. Res. 2021, 33, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Koutsonida, M.; Kanellopoulou, A.; Markozannes, G.; Gousia, S.; Doumas, M.T.; Sigounas, D.E.; Tzovaras, V.T.; Vakalis, K.; Tzoulaki, I.; Evangelou, E.; et al. Adherence to Mediterranean Diet and Cognitive Abilities in the Greek Cohort of Epirus Health Study. Nutrients 2021, 13, 3363. [Google Scholar] [CrossRef]
- Tsiampalis, T.; Faka, A.; Kouvari, M.; Psaltopoulou, T.; Pitsavos, C.; Chalkias, C.; Panagiotakos, D.B. The impact of socioeconomic and environmental determinants on Mediterranean diet adherence: A municipal-level spatial analysis in Athens metropolitan area, Greece. Int. J. Food Sci. Nutr. 2021, 72, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- European Health Examination Survey. Guidelines for Health Examination Surveys: The EHES Manual, 2nd ed.; European Health Examination Survey: Helsinki, Finland, 2016; Available online: http://www.ehes.info/manuals.htm#manual (accessed on 13 September 2021).
- European Food Safety Authority. Guidance on the EU Menu methodology. EFSA J. 2014, 12, 3944. [Google Scholar]
- LanguaL™—The International Framework for Food Description. LanguaL™ is a Food Description Thesaurus. Available online: http://www.langual.org/ (accessed on 8 December 2021).
- Naska, A.; Valanou, E.; Peppa, E.; Katsoulis, M.; Barbouni, A.; Trichopoulou, A. Evaluation of a digital food photography atlas used as portion size measurement aid in dietary surveys in Greece. Public Health Nutr. 2016, 19, 2369–2376. [Google Scholar] [CrossRef]
- Ambrus, A.; Árpád; Horváth, Z.; Farkas, Z.; Dorogházi, E.; Cseh, J.; Petrova, S.; Dimitrov, P.; Duleva, V.; Rangelova, L.; et al. Pilot study in the view of a Pan-European dietary survey—Adolescents, adults and elderly. EFSA Support. Publ. 2013, 10, 508. [Google Scholar] [CrossRef]
- EuroFIR. European Food Information Resource. List of EuroFIR Databases. Databases available on FoodExplorer. Available online: https://www.eurofir.org/food-information/food-composition-databases/ (accessed on 12 December 2021).
- Trichopoulou, A.G.K. Composition Tables of Foods and Greek Dishes, 3rd ed.; Parisianou Publications: Athens, Greece, 2004. [Google Scholar]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate: A practical guide to its calculation, use and limitations. Int. J. Obes. 2000, 24, 1119–1130. [Google Scholar] [CrossRef]
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: Derivation of cut-off limits to identify under-recording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. 1), 5–41. [Google Scholar] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. General principles for the collection of national food consumption data in the view of a pan-European dietary survey. EFSA J. 2009, 7, 1435. [Google Scholar] [CrossRef]
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef]
- Tooze, J.A.; Midthune, D.; Dodd, K.W.; Freedman, L.S.; Krebs-Smith, S.M.; Subar, A.F.; Guenther, P.M.; Carroll, R.J.; Kipnis, V. A New Statistical Method for Estimating the Usual Intake of Episodically Consumed Foods with Application to Their Distribution. J. Am. Diet. Assoc. 2006, 106, 1575–1587. [Google Scholar] [CrossRef] [PubMed]
- Kipnis, V.; Subar, A.F.; Midthune, D.; Freedman, L.S.; Ballard-Barbash, R.; Troiano, R.P.; Bingham, S.; Schoeller, D.A.; Schatzkin, A.; Carroll, R.J. Structure of Dietary Measurement Error: Results of the OPEN Biomarker Study. Am. J. Epidemiol. 2003, 158, 14–21, discussion 22–16. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Guenther, P.M.; Kirkpatrick, S.; Reedy, J.; Krebs-Smith, S.M.; Buckman, D.W.; Dodd, K.W.; Casavale, K.O.; Carroll, R.J. The Healthy Eating Index-2010 Is a Valid and Reliable Measure of Diet Quality According to the 2010 Dietary Guidelines for Americans. J. Nutr. 2014, 144, 399–407. [Google Scholar] [CrossRef]
- Zhang, S.; Carroll, R.J.; Midthune, D.; Guenther, P.M.; Krebs-Smith, S.M.; Kipnis, V.; Dodd, K.W.; Buckman, D.W.; Tooze, J.A.; Freedman, L. A new multivariate measurement error model with zero-inflated dietary data, and its application to dietary assessment. Ann. Appl. Stat. 2011, 5, 1456–1487. [Google Scholar] [CrossRef]
- Naska, A.O.P.; Chloptsios, Y.; Trichopoulou, A. Dietary habits in Greece: The European Prospective Investigation into Cancer and nutrition (the EPIC project). Arch. Hell. Med. 2005, 22, 259–269. [Google Scholar]
- Benetou, V.; Trichopoulou, A.; Orfanos, P.; Naska, A.; Lagiou, P.; Boffetta, P.; Trichopoulos, D. Conformity to traditional Mediterranean diet and cancer incidence: The Greek EPIC cohort. Br. J. Cancer 2008, 99, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Dilis, V.; Katsoulis, M.; Lagiou, P.; Trichopoulos, D.; Naska, A.; Trichopoulou, A. Mediterranean diet and CHD: The Greek European Prospective Investigation into Cancer and Nutrition cohort. Br. J. Nutr. 2012, 108, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Magriplis, E.; Panagiotakos, D.; Kyrou, I.; Tsioufis, C.; Mitsopoulou, A.-V.; Karageorgou, D.; Dimakopoulos, I.; Bakogianni, I.; Chourdakis, M.; Micha, R.; et al. Presence of Hypertension Is Reduced by Mediterranean Diet Adherence in All Individuals with a More Pronounced Effect in the Obese: The Hellenic National Nutrition and Health Survey (HNNHS). Nutrients 2020, 12, 853. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.; Pitsavos, C.; Chrysohoou, C.; Palliou, K.; Lentzas, I.; Skoumas, I.; Stefanadis, C. Dietary patterns and 5-year incidence of cardiovascular disease: A multivariate analysis of the ATTICA study. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Couto, E.; Boffetta, P.; Lagiou, P.; Ferrari, P.; Buckland, G.; Overvad, K.; Dahm, C.; Tjonneland, A.; Olsen, A.; Clavelchapelon, F.; et al. Mediterranean dietary pattern and cancer risk in the EPIC cohort. Br. J. Cancer 2011, 104, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Stampfer, M.J.; Manson, J.E.; Rexrode, K.M.; Willett, W.C.; Hu, F.B. Prospective Study of Major Dietary Patterns and Stroke Risk in Women. Stroke 2004, 35, 2014–2019. [Google Scholar] [CrossRef] [PubMed]
- Heidemann, C.; Schulze, M.B.; Franco, O.; van Dam, R.; Mantzoros, C.S.; Hu, F.B. Dietary Patterns and Risk of Mortality from Cardiovascular Disease, Cancer, and All Causes in a Prospective Cohort of Women. Circulation 2008, 118, 230–237. [Google Scholar] [CrossRef]
- Pala, V.; Krogh, V.; Berrino, F.; Sieri, S.; Grioni, S.; Tjonneland, A.; Olsen, A.; Jakobsen, M.U.; Overvad, K.; Clavel-Chapelon, F.; et al. Meat, eggs, dairy products, and risk of breast cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. Am. J. Clin. Nutr. 2009, 90, 602–612. [Google Scholar] [CrossRef]
- Rohrmann, S.; Overvad, K.; Bueno-De-Mesquita, H.B.; Jakobsen, M.U.; Egeberg, R.; Tjønneland, A.; Nailler, L.; Boutron-Ruault, M.-C.; Clavel-Chapelon, F.; Krogh, V.; et al. Meat consumption and mortality—Results from the European Prospective Investigation into Cancer and Nutrition. BMC Med. 2013, 11, 63. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-De-Mesquita, B.; Ocké, M.C.; Peeters, P.H.; Van Der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified Mediterranean diet and survival: EPIC-elderly prospective cohort study. BMJ 2005, 330, 991. [Google Scholar] [CrossRef]
- Mertens, E.; Kuijsten, A.; Dofková, M.; Mistura, L.; D’Addezio, L.; Turrini, A.; Dubuisson, C.; Favret, S.; Havard, S.; Trolle, E.; et al. Geographic and socioeconomic diversity of food and nutrient intakes: A comparison of four European countries. Eur. J. Nutr. 2019, 58, 1475–1493. [Google Scholar] [CrossRef] [PubMed]
- Rippin, H.L.; Hutchinson, J.; Jewell, J.; Breda, J.J.; Cade, J.E. Adult Nutrient Intakes from Current National Dietary Surveys of European Populations. Nutreints 2017, 9, 1288. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. Dietary Reference Values for the EU. DRV Finder. Available online: https://multimedia.efsa.europa.eu/drvs/index.htm (accessed on 13 September 2021).
- Agostoni, C.; Bresson, J.-L.; Fairweather-Tait, S.; Flynn, A.; Golly, I.; Korhonen, H.; Lagiou, P.; Løvik, M.; Marchelli, R.; Martin, A.; et al. Scientific Opinion on Dietary Reference Values for protein. EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). EFSA J. 2012, 10, 2557. [Google Scholar]
- Joint WHO/FAO/UNU Expert Consultation. Protein and Amino Acid Requirements in Human Nutrition. World Health Organ. Tech. Rep. Ser. 2007, 935, 1–265. [Google Scholar]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M.; Food and Nutrition Board of the Institute of Medicine; The National Academies. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids. J. Am. Diet. Assoc. 2002, 102, 1621–1630. [Google Scholar] [CrossRef]
- Richter, M.; Baerlocher, K.; Bauer, J.M.; Elmadfa, I.; Heseker, H.; Leschik-Bonnet, E.; Stangl, G.; Volkert, D.; Stehle, P.; on behalf of the German Nutrition Society (DGE). Revised Reference Values for the Intake of Protein. Ann. Nutr. Metab. 2019, 74, 242–250. [Google Scholar] [CrossRef]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012: Integrating Nutrition and Physical Activity, 5th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2014; pp. 349–384. [Google Scholar]
- World Health Organization. Healthy Diet. Fact Sheet N°394. Available online: https://www.who.int/docs/default-source/healthy-diet/healthy-diet-fact-sheet-394.pdf (accessed on 13 September 2021).
- World Cancer Research Fund; American Institute for Cancer Research. Continuous Update Project Expert Report Recommendations and public health and policy implications. 2018. Available online: https://www.wcrf.org/dietandcancer (accessed on 13 September 2021).
- Elmadfa, I.; Meyer, A.; Nowak, V.; Hasenegger, V.; Putz, P.; Verstraeten, R.; Remaut-DeWinter, A.M.; Kolsteren, P.; Dostálová, J.; Dlouhý, P.; et al. European nutrition and health report 2009. Forum Nutr. 2009, 62, 1–405. [Google Scholar]
- Meybeck, A.R.S.; Paoletti, F.; Strassner, C. Office of Assistant Director-General (Agriculture Department). Assessing sustainable diets within the sustainability of food systems. In Proceedings of the International Workshop: Mediterranean Diet, Organic Food: New Challenges, Rome, Italy, 15–16 September 2014; Available online: https://it.scribd.com/document/334871835/tmp669E-tmp (accessed on 14 January 2022).
- The Swedish National Food Agency (Livsmedelsverket). Find Your way to Eat Greener, Not too Much and to Be Active! (Hitta Ditt Sätt Att Äta Grönare, Lagom Mycket Och Röra På Dig!). Livesmedelsverket, Uppsala. 2017. Available online: https://www.livsmedelsverket.se/en/food-habits-health-and-environment/dietary-guidelines/adults (accessed on 13 September 2021).
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Li, Z.; Heber, D. Ketogenic Diets. JAMA 2020, 323, 386. [Google Scholar] [CrossRef]

{kind=link}
| Men, % | Women, % | |
|---|---|---|
| Age | ||
| 18–64 years | 77.0 | 73.1 |
| ≥65 years | 23.0 | 26.9 |
| Education level 1 | ||
| Low | 34.9 | 44.1 |
| Intermediate | 41.1 | 35.7 |
| High | 24.0 | 20.2 |
| Employment status 2 | ||
| Employed | 52.0 | 31.7 |
| Unemployed | 14.6 | 14.6 |
| Students | 5.4 | 5.0 |
| Pensioners | 28.0 | 22.1 |
| Housewives | 0.0 | 26.6 |
| Geographic area 3 | ||
| Attiki | 35.9 | 36.7 |
| Northern Greece | 28.4 | 28.6 |
| Central Greece | 25.5 | 24.6 |
| Egeo and Kriti | 10.2 | 10.1 |
| Physical activity 4 | ||
| Sedentary | 30.2 | 18.3 |
| Light-intensity | 66.1 | 80.5 |
| Moderate-intensity | 3.7 | 1.2 |
| Smoking status | ||
| Never smoker | 30.3 | 54.8 |
| Former smoker | 30.3 | 12.8 |
| Current smoker | 39.4 | 32.4 |
| BMI 5 | ||
| Obese | 34.0 | 35.6 |
| Overweight | 43.4 | 31.0 |
| Normal weight | 22.3 | 31.1 |
| Underweight | 0.2 | 1.5 |
| 18+ Years | 18–64 Years | 65+ Years | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | p25 | Median | p75 | Mean | p25 | Median | p75 | Mean | p25 | Median | p75 | |
| Energy | ||||||||||||
| Men | 2192 | 1718 | 2109 | 2559 | 2331 | 1863 | 2237 | 2673 | 1727 | 1388 | 1683 | 2031 |
| Women | 1530 | 1221 | 1473 | 1763 | 1611 | 1304 | 1553 | 1838 | 1309 | 1057 | 1264 | 1502 |
| Age Group | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| %EI | p25 | Median | p75 | %EI | p25 | Median | p75 | |
| Protein | ||||||||
| 18+ years | 15.1 | 64 | 80 | 99 | 15.2 | 47 | 57 | 67 |
| 18–64 years | 15.3 | 69 | 85 | 104 | 15.1 | 50 | 60 | 70 |
| 65+ years | 15.1 | 51 | 64 | 78 | 15.3 | 41 | 49 | 58 |
| Glycaemic carbohydrates | ||||||||
| 18+ years | 35.2 | 144 | 183 | 229 | 38.2 | 114 | 140 | 170 |
| 18–64 years | 35.2 | 155 | 195 | 240 | 37.9 | 122 | 147 | 177 |
| 65+ years | 35.0 | 116 | 147 | 183 | 38.2 | 100 | 121 | 146 |
| Fibre | ||||||||
| 18+ years | 1.7 | 14 | 18 | 23 | 1.9 | 11 | 14 | 17 |
| 18–64 years | 1.7 | 14 | 18 | 23 | 1.9 | 11 | 14 | 18 |
| 65+ years | 2.0 | 13 | 17 | 21 | 2.2 | 11 | 13 | 17 |
| Total fat | ||||||||
| 18+ years | 42.3 | 80 | 99 | 121 | 42.9 | 57 | 70 | 85 |
| 18–64 years | 42.1 | 86 | 105 | 126 | 42.5 | 61 | 73 | 88 |
| 65+ years | 43.3 | 65 | 80 | 98 | 43.3 | 49 | 60 | 72 |
| Saturated fatty acids, SFA | ||||||||
| 18+ years | 13.1 | 24 | 31 | 38 | 13.5 | 18 | 23 | 28 |
| 18–64 years | 13.1 | 26 | 33 | 40 | 13.4 | 18 | 24 | 29 |
| 65+ years | 12.5 | 19 | 24 | 29 | 13.1 | 15 | 19 | 23 |
| Monounsaturated fatty acids, MUFA | ||||||||
| 18+ years | 20.3 | 38 | 47 | 58 | 20.6 | 26 | 33 | 40 |
| 18–64 years | 20.1 | 41 | 50 | 60 | 20.1 | 28 | 34 | 41 |
| 65+ years | 21.9 | 32 | 40 | 49 | 21.3 | 23 | 29 | 36 |
| Polyunsaturated fatty acids, PUFA | ||||||||
| 18+ years | 5.7 | 10 | 13 | 17 | 5.9 | 7 | 9 | 12 |
| 18–64 years | 5.8 | 11 | 14 | 18 | 6.1 | 7 | 10 | 12 |
| 65+ years | 5.7 | 8 | 11 | 13 | 5.5 | 6 | 8 | 10 |
| Alcohol | ||||||||
| 18+ years | 5.4 | 3 | 10 | 23 | 1.8 | 0.6 | 2 | 5 |
| 18–64 years | 5.7 | 3 | 10 | 25 | 2.2 | 0.9 | 3 | 6 |
| 65+ years | 4.5 | 2 | 8 | 18 | 1.1 | 0.3 | 0.9 | 3 |
| Age Group | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean | p25 | Median | p75 | Mean | p25 | Median | p75 | |
| Vegetables (without potatoes) | ||||||||
| 18+ years | 198 | 147 | 203 | 270 | 217 | 116 | 158 | 206 |
| 18–64 years | 186 | 146 | 202 | 268 | 204 | 115 | 157 | 204 |
| 65+ years | 251 | 148 | 208 | 279 | 260 | 118 | 161 | 211 |
| Potatoes | ||||||||
| 18+ years | 43 | 28 | 44 | 64 | 43 | 17 | 27 | 41 |
| 18–64 years | 43 | 32 | 47 | 68 | 43 | 18 | 29 | 43 |
| 65+ years | 42 | 21 | 33 | 49 | 43 | 15 | 24 | 36 |
| Legumes | ||||||||
| 18+ years | 16 | 12 | 17 | 23 | 18 | 5 | 10 | 18 |
| 18–64 years | 14 | 12 | 16 | 21 | 16 | 5 | 9 | 17 |
| 65+ years | 25 | 17 | 22 | 29 | 23 | 6 | 11 | 20 |
| Fruit (without fruit juices) | ||||||||
| 18+ years | 112 | 25 | 75 | 166 | 168 | 33 | 90 | 180 |
| 18–64 years | 98 | 20 | 63 | 147 | 144 | 26 | 76 | 160 |
| 65+ years | 177 | 50 | 119 | 224 | 249 | 61 | 133 | 223 |
| Cereals and products | ||||||||
| 18+ years | 224 | 166 | 223 | 292 | 209 | 117 | 151 | 190 |
| 18–64 years | 227 | 183 | 240 | 308 | 209 | 124 | 159 | 199 |
| 65+ years | 211 | 127 | 169 | 223 | 211 | 102 | 131 | 164 |
| Bread | ||||||||
| 18+ years | 127 | 98 | 134 | 175 | 110 | 60 | 78 | 97 |
| 18–64 years | 118 | 103 | 141 | 183 | 110 | 63 | 81 | 100 |
| 65+ years | 133 | 87 | 116 | 147 | 110 | 55 | 70 | 85 |
| Pasta | ||||||||
| 18+ years | 53 | 28 | 47 | 73 | 48 | 31 | 39 | 48 |
| 18–64 years | 51 | 34 | 53 | 79 | 48 | 34 | 42 | 50 |
| 65+ years | 42 | 18 | 29 | 47 | 49 | 26 | 33 | 40 |
| Rice | ||||||||
| 18+ years | 19 | 13 | 18 | 23 | 21 | 8 | 13 | 21 |
| 18–64 years | 17 | 13 | 18 | 23 | 20 | 8 | 13 | 20 |
| 65+ years | 22 | 11 | 16 | 21 | 26 | 9 | 14 | 22 |
| Dairy and products | ||||||||
| 18+ years | 188 | 104 | 181 | 284 | 251 | 113 | 180 | 270 |
| 18–64 years | 176 | 104 | 180 | 283 | 243 | 116 | 184 | 275 |
| 65+ years | 240 | 103 | 182 | 285 | 281 | 105 | 169 | 256 |
| Milk | ||||||||
| 18+ years | 112 | 23 | 82 | 188 | 162 | 37 | 96 | 189 |
| 18–64 years | 103 | 22 | 79 | 185 | 154 | 37 | 96 | 190 |
| 65+ years | 152 | 28 | 92 | 199 | 188 | 37 | 95 | 187 |
| Yoghurt | ||||||||
| 18+ years | 22 | 2 | 7 | 24 | 38 | 2 | 18 | 40 |
| 18–64 years | 17 | 1 | 6 | 21 | 36 | 2 | 18 | 39 |
| 65+ years | 41 | 3 | 12 | 39 | 46 | 2 | 20 | 43 |
| Cheese | ||||||||
| 18+ years | 49 | 12 | 50 | 74 | 47 | 13 | 37 | 50 |
| 18–64 years | 47 | 15 | 55 | 79 | 50 | 16 | 40 | 53 |
| 65+ years | 46 | 8 | 37 | 57 | 41 | 9 | 28 | 39 |
| Meat and products | ||||||||
| 18+ years | 99 | 66 | 96 | 134 | 81 | 43 | 58 | 74 |
| 18–64 years | 104 | 78 | 108 | 145 | 84 | 50 | 64 | 79 |
| 65+ years | 73 | 42 | 61 | 85 | 70 | 31 | 43 | 56 |
| Poultry | ||||||||
| 18+ years | 26 | 14 | 23 | 37 | 24 | 8 | 13 | 21 |
| 18–64 years | 27 | 15 | 25 | 40 | 25 | 10 | 16 | 24 |
| 65+ years | 21 | 10 | 17 | 27 | 17 | 5 | 8 | 13 |
| Red meat | ||||||||
| 18+ years | 54 | 37 | 51 | 69 | 44 | 25 | 38 | 55 |
| 18–64 years | 57 | 44 | 57 | 75 | 45 | 28 | 42 | 60 |
| 65+ years | 42 | 27 | 34 | 42 | 44 | 19 | 28 | 40 |
| Fish (including seafood) and products | ||||||||
| 18+ years | 24 | 8 | 16 | 34 | 26 | 8 | 14 | 26 |
| 18–64 years | 21 | 7 | 16 | 32 | 22 | 7 | 13 | 23 |
| 65+ years | 35 | 9 | 19 | 37 | 38 | 11 | 20 | 33 |
| Eggs | ||||||||
| 18+ years | 15 | 8 | 13 | 21 | 16 | 6 | 10 | 15 |
| 18–64 years | 15 | 9 | 14 | 23 | 15 | 7 | 11 | 16 |
| 65+ years | 13 | 5 | 9 | 15 | 14 | 5 | 8 | 13 |
| Fats and oils | ||||||||
| 18+ years | 44 | 35 | 44 | 56 | 44 | 25 | 32 | 40 |
| 18–64 years | 42 | 36 | 46 | 57 | 43 | 25 | 32 | 41 |
| 65+ years | 51 | 31 | 40 | 51 | 49 | 23 | 30 | 38 |
| Olive oil | ||||||||
| 18+ years | 35 | 24 | 34 | 44 | 35 | 18 | 25 | 31 |
| 18–64 years | 33 | 25 | 35 | 45 | 33 | 19 | 25 | 31 |
| 65+ years | 43 | 23 | 32 | 42 | 40 | 18 | 24 | 30 |
| Nonalcoholic beverages | ||||||||
| 18+ years | 124 | 46 | 104 | 243 | 121 | 26 | 55 | 117 |
| 18–64 years | 136 | 62 | 136 | 302 | 137 | 37 | 73 | 145 |
| 65+ years | 73 | 24 | 47 | 89 | 69 | 13 | 26 | 48 |
| Sugar and products | ||||||||
| 18+ years | 26 | 11 | 22 | 39 | 39 | 13 | 24 | 41 |
| 18–64 years | 27 | 14 | 25 | 43 | 42 | 16 | 28 | 47 |
| 65+ years | 21 | 7 | 14 | 25 | 29 | 8 | 15 | 26 |
| Alcoholic beverages | ||||||||
| 18+ years | 172 | 27 | 101 | 256 | 68 | 8 | 25 | 64 |
| 18–64 years | 179 | 32 | 114 | 281 | 76 | 12 | 32 | 74 |
| 65+ years | 133 | 14 | 68 | 178 | 40 | 3 | 12 | 34 |
| Wine | ||||||||
| 18+ years | 80 | 5 | 23 | 95 | 34 | 4 | 11 | 28 |
| 18–64 years | 78 | 6 | 23 | 95 | 36 | 5 | 13 | 31 |
| 65+ years | 89 | 3 | 19 | 96 | 26 | 2 | 5 | 18 |
| Beer | ||||||||
| 18+ years | 71 | 4 | 18 | 81 | 29 | 2 | 5 | 19 |
| 18–64 years | 80 | 5 | 26 | 103 | 32 | 2 | 7 | 25 |
| 65+ years | 32 | 1 | 5 | 25 | 12 | 1 | 3 | 8 |
| Low (Score of 0–3 Points) | Intermediate (Score of 4–5 Points) | High (Score of 6–9 Points) | |
|---|---|---|---|
| Total, % | 32.6 | 39.1 | 28.3 |
| Sex, % | |||
| Men | 29.7 | 39.0 | 31.3 |
| Women | 35.1 | 39.2 | 25.7 |
| Age, % | |||
| <65 years | 35.8 | 38.7 | 25.5 |
| ≥65 years | 19.5 | 40.8 | 39.7 |
| Geographic area 1, % | |||
| Attiki | 35.6 | 38.7 | 25.7 |
| Northern Greece | 30.0 | 39.7 | 30.3 |
| Central Greece | 31.2 | 39.0 | 29.7 |
| Egeo and Kriti | 33.1 | 39.2 | 27.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martimianaki, G.; Peppa, E.; Valanou, E.; Papatesta, E.M.; Klinaki, E.; Trichopoulou, A. Today’s Mediterranean Diet in Greece: Findings from the National Health and Nutrition Survey—HYDRIA (2013–2014). Nutrients 2022, 14, 1193. https://doi.org/10.3390/nu14061193
Martimianaki G, Peppa E, Valanou E, Papatesta EM, Klinaki E, Trichopoulou A. Today’s Mediterranean Diet in Greece: Findings from the National Health and Nutrition Survey—HYDRIA (2013–2014). Nutrients. 2022; 14(6):1193. https://doi.org/10.3390/nu14061193
Chicago/Turabian StyleMartimianaki, Georgia, Eleni Peppa, Elisavet Valanou, Eleni M. Papatesta, Eleni Klinaki, and Antonia Trichopoulou. 2022. "Today’s Mediterranean Diet in Greece: Findings from the National Health and Nutrition Survey—HYDRIA (2013–2014)" Nutrients 14, no. 6: 1193. https://doi.org/10.3390/nu14061193
APA StyleMartimianaki, G., Peppa, E., Valanou, E., Papatesta, E. M., Klinaki, E., & Trichopoulou, A. (2022). Today’s Mediterranean Diet in Greece: Findings from the National Health and Nutrition Survey—HYDRIA (2013–2014). Nutrients, 14(6), 1193. https://doi.org/10.3390/nu14061193