
Maternal Zinc, Copper, and Selenium Intakes during Pregnancy and Congenital Heart Defects

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Dietary Assessment
2.3. Covariates
2.4. Statistical Analysis
3. Results
3.1. Basic Characteristics of the Study Sample
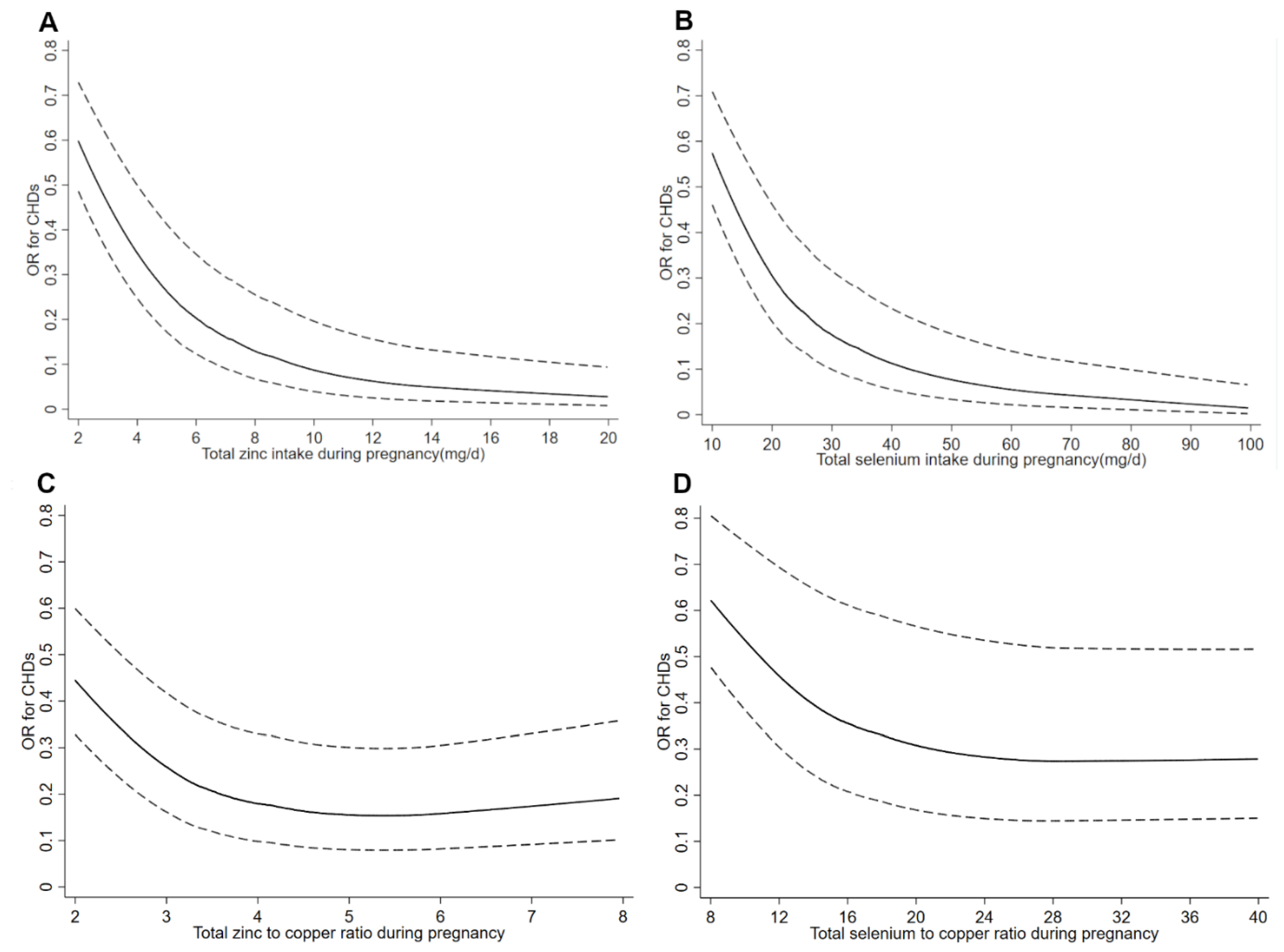
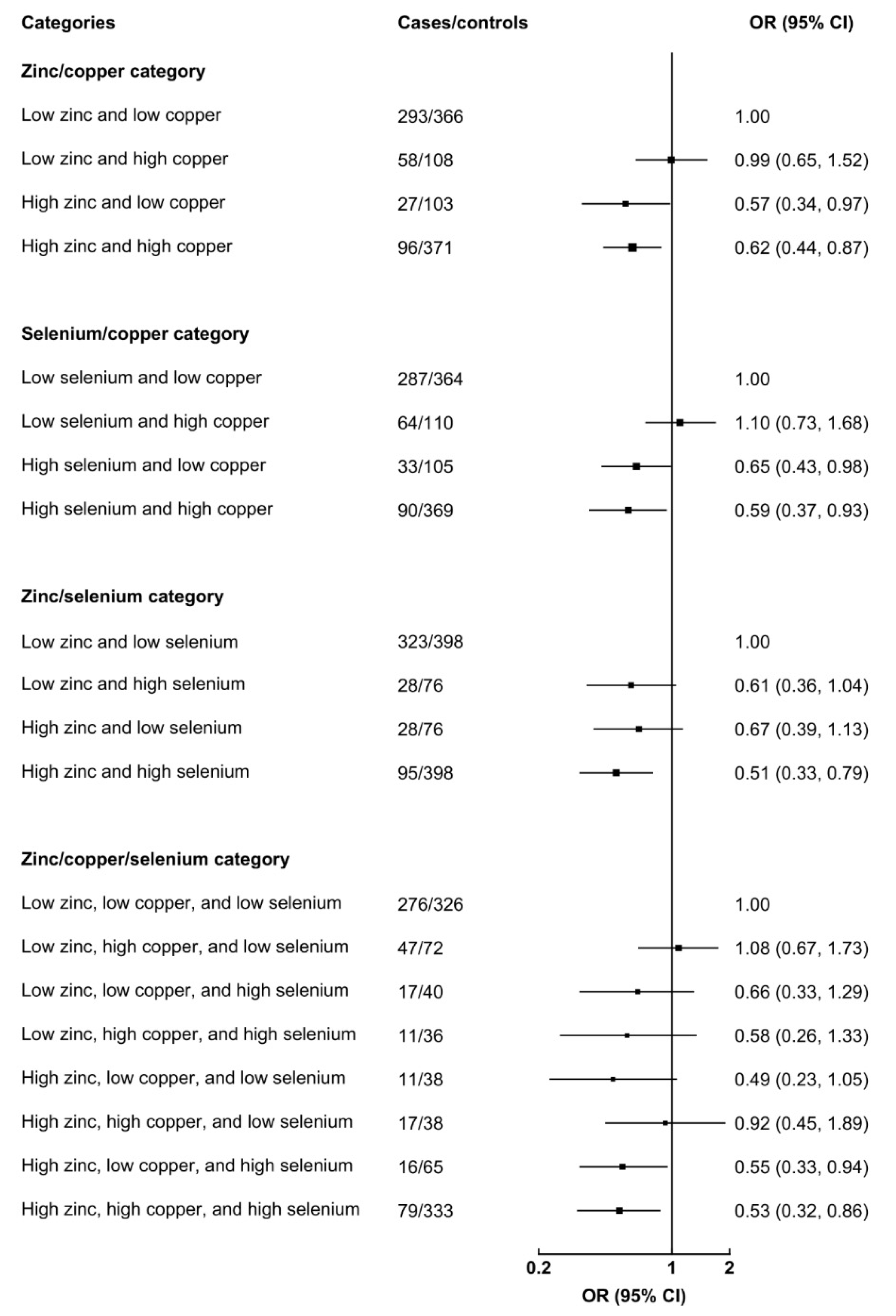
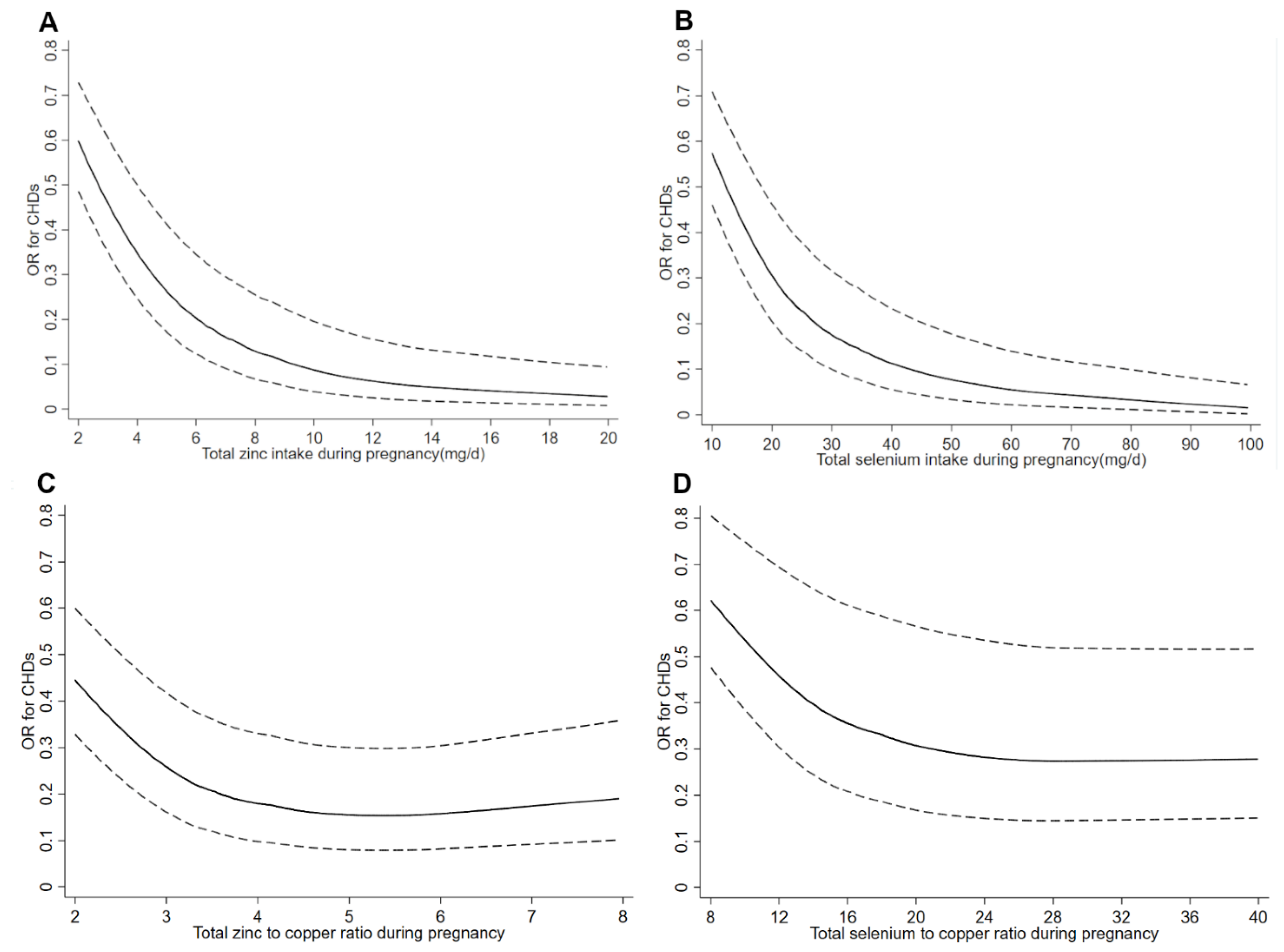
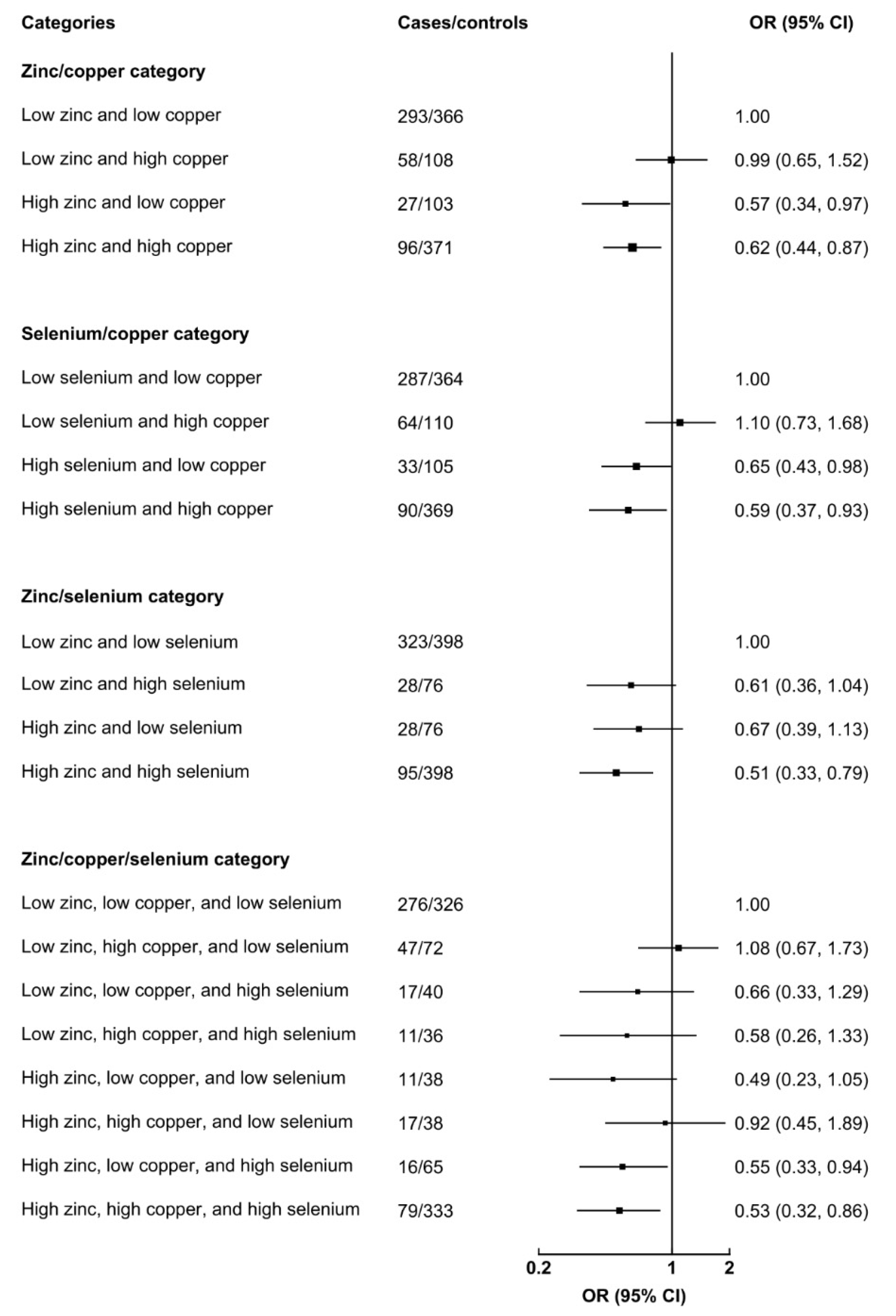
3.2. Maternal Total and Dietary Zinc, Copper, and Selenium Intakes during Pregnancy and CHDs
3.3. Maternal Zinc, Copper, and Selenium Supplements Uses during Pregnancy and CHDs
4. Discussion
4.1. Comparisons with Other Studies
4.2. Possible Mechanisms
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, Y.; Chen, S.; Zuhlke, L.; Black, G.C.; Choy, M.K.; Li, N.; Keavney, B.D. Global birth prevalence of congenital heart defects 1970–2017, updated systematic review and meta-analysis of 260 studies. Int. J. Epidemiol. 2019, 48, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Donofrio, M.T.; Moon-Grady, A.J.; Hornberger, L.K.; Copel, J.A.; Sklansky, M.S.; Abuhamad, A.; Cuneo, B.F.; Huhta, J.C.; Jonas, R.A.; Krishnan, A.; et al. Diagnosis and treatment of fetal cardiac disease: A scientific statement from the American Heart Association. Circulation 2014, 129, 2183–2242. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.M.; Liu, F.; Wu, L.; Ma, X.J.; Niu, C.; Huang, G.Y. Prevalence of congenital heart disease at live birth in China. J. Pediatr. 2019, 204, 53–58. [Google Scholar] [CrossRef]
- Mousa, A.; Naqash, A.; Lim, S. Macronutrient and micronutrient intake during pregnancy: An overview of recent evidence. Nutrients 2019, 11, 443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez, V.; Keen, C.L.; Lanoue, L. Prenatal zinc deficiency: Influence on heart morphology and distribution of key heart proteins in a rat model. Biol. Trace Elem. Res. 2008, 122, 238–255. [Google Scholar] [CrossRef] [PubMed]
- Beckers-Trapp, M.E.; Lanoue, L.; Keen, C.L.; Rucker, R.B.; Uriu-Adams, J.Y. Abnormal development and increased 3-nitrotyrosine in copper-deficient mouse embryos. Free Radic. Biol. Med. 2006, 40, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Huang, W.; Liu, J.; Ye, Z.; Dou, S. Toxicity of short-term copper exposure to early life stages of red sea bream. Pagrus major. Environ. Toxicol. Chem. 2010, 29, 2044–2052. [Google Scholar] [CrossRef] [PubMed]
- Ojeda, M.L.; Nogales, F.; Romero-Herrera, I.; Carreras, O. Fetal programming is deeply related to maternal selenium status and oxidative balance; Experimental offspring health repercussions. Nutrients 2021, 13, 2085. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P.; Wijnen, H.; Vader, H.; Kooistra, L.; Pop, V. Maternal selenium status during early gestation and risk for preterm birth. Cmaj 2011, 183, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Zachara, B.A. Selenium in complicated pregnancy. A review. Adv. Clin. Chem. 2018, 86, 157–178. [Google Scholar] [PubMed]
- Dilli, D.; Doğan, N.N.; Örün, U.A.; Koç, M.; Zenciroğlu, A.; Karademir, S.; Akduman, H. Maternal and neonatal micronutrient levels in newborns with CHD. Cardiol. Young. 2018, 28, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Yu, P.; Zhu, J.; Yang, S.; Yu, J.; Deng, Y.; Li, N.; Liu, Z. High maternal selenium levels are associated with increased risk of congenital heart defects in the offspring. Prenat. Diagn. 2019, 39, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Liu, Z.; Li, J.; Li, S.; Tian, X.; Lin, Y.; Chen, X.; Yang, J.; Deng, Y.; Li, N.; et al. Correlation between congenital heart defects and maternal copper and zinc concentrations. Birth Defects Res. A Clin. Mol. Teratol. 2014, 100, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Ou, Y.; Bloom, M.S.; Nie, Z.; Han, F.; Mai, J.; Chen, J.; Lin, S.; Liu, X.; Zhuang, J. Associations between toxic and essential trace elements in maternal blood and fetal congenital heart defects. Env. Int. 2017, 106, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Yalçin, S.S.; Dönmez, Y.; Aypar, E.; Yalçin, S. Element profiles in blood and teeth samples of children with congenital heart diseases in comparison with healthy ones. J. Trace Elem. Med. Biol. 2021, 63, 126662. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Xu, C.; Zhang, Y.; Xie, Z.; Shu, Y.; Lu, C.; Mo, X. Associations of trace elements in blood with the risk of isolated ventricular septum defects and abnormal cardiac structure in children. Env. Sci. Pollut. Res. Int. 2019, 26, 10037–10043. [Google Scholar] [CrossRef] [PubMed]
- Mares-Perlman, J.A.; Subar, A.F.; Block, G.; Greger, J.L.; Luby, M.H. Zinc intake and sources in the US adult population: 1976–1980. J. Am. Coll. Nutr. 1995, 14, 349–357. [Google Scholar] [CrossRef]
- House, W.A.; Welch, R.M. Bioavailability of and interactions between zinc and selenium in rats fed wheat grain intrinsically labeled with 65Zn and 75Se. J. Nutr. 1989, 119, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Ojo, A.A.; Nadella, S.R.; Wood, C.M. In vitro examination of interactions between copper and zinc uptake via the gastrointestinal tract of the rainbow trout (Oncorhynchus mykiss). Arch. Env. Contam. Toxicol. 2009, 56, 244–252. [Google Scholar] [CrossRef]
- Schwarz, M.; Lossow, K.; Schirl, K.; Hackler, J.; Renko, K.; Kopp, J.F.; Schwerdtle, T.; Schomburg, L.; Kipp, A.P. Copper interferes with selenoprotein synthesis and activity. Redox. Biol. 2020, 37, 101746. [Google Scholar] [CrossRef]
- Yang, J.; Kang, Y.; Cheng, Y.; Zeng, L.; Shen, Y.; Shi, G.; Liu, Y.; Qu, P.; Zhang, R.; Yan, H.; et al. Iron intake and iron status during pregnancy and risk of congenital heart defects: A case-control study. Int. J. Cardiol. 2020, 301, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Kang, Y.; Cheng, Y.; Zeng, L.; Yan, H.; Dang, S. Maternal dietary patterns during pregnancy and congenital heart defects: A case-control study. Int. J. Env. Res. Public Health 2019, 16, 2957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, L. Soil Trace Elements in China; Phoenix Science Press: Nanjing, China, 1996. [Google Scholar]
- Crozier, S.R.; Robinson, S.M.; Godfrey, K.M.; Cooper, C.; Inskip, H.M. Women’s dietary patterns change little from before to during pregnancy. J. Nutr. 2009, 139, 1956–1963. [Google Scholar] [CrossRef] [PubMed]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Willett, W.C.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Changes in dietary intake from the first to the second trimester of pregnancy. Paediatr. Perinat. Epidemiol. 2006, 20, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Cheng, Y.; Zeng, L.; Dang, S.; Yan, H. Maternal dietary diversity during pregnancy and congenital heart defects: A case-control study. Eur. J. Clin. Nutr. 2021, 75, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Yan, H.; Dibley, M.J.; Shen, Y.; Li, Q.; Zeng, L. Validity and reproducibility of a semi-quantitative food frequency questionnaire for use among pregnant women in rural China. Asia Pac. J. Clin. Nutr. 2008, 17, 166–177. [Google Scholar] [PubMed]
- Yang, J.; Dang, S.; Cheng, Y.; Qiu, H.; Mi, B.; Jiang, Y.; Qu, P.; Zeng, L.; Wang, Q.; Li, Q.; et al. Dietary intakes and dietary patterns among pregnant women in Northwest China. Public Health Nutr. 2017, 20, 282–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute of Nutrition and Food Safety, China Center for Disease Control. China Food Composition Book 2; Peking University Medical Press: Beijing, China, 2005. [Google Scholar]
- Institute of Nutrition and Food Safety, China Center for Disease Control. China Food Composition Book 1, 2nd ed.; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- FAO; FHI 360. Minimum Dietary Dieversity for Women: A Guide for Measurement; FAO: Rome, Italy, 2016. [Google Scholar]
- Chinese Nutrition Society. Chinese Dietary Guideline; People’s Medical Publishing House: Beijing, China, 2016. [Google Scholar]
- Feng, Y.; Cai, J.; Tong, X.; Chen, R.; Zhu, Y.; Xu, B.; Mo, X. Non-inheritable risk factors during pregnancy for congenital heart defects in offspring: A matched case-control study. Int. J. Cardiol. 2018, 264, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Pei, L.; Kang, Y.; Zhao, Y.; Yan, H. Prevalence and risk factors of congenital heart defects among live births: A population-based cross-sectional survey in Shaanxi province, Northwestern China. BMC Pediatr. 2017, 17, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mickey, R.M.; Greenland, S. The impact of confounder selection criteria on effect estimation. Am. J. Epidemiol. 1989, 129, 125–137. [Google Scholar] [CrossRef]
- Nakamura, M.; Miura, A.; Nagahata, T.; Shibata, Y.; Okada, E.; Ojima, T. Low Zinc, Copper, and manganese intake is associated with depression and anxiety symptoms in the Japanese working population: Findings from the eating habit and well-being study. Nutrients 2019, 11, 847. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, S.; Ali, I.; Rust, P.; Kundi, M.; Ekmekcioglu, C. Selenium, zinc, and manganese status in pregnant women and its relation to maternal and child complications. Nutrients 2020, 12, 725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehdi, Y.; Hornick, J.L.; Istasse, L.; Dufrasne, I. Selenium in the environment, metabolism and involvement in body functions. Molecules 2013, 18, 3292–3311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, D.; Sachdev, H.P. Zinc deficiency in pregnancy and fetal outcome. Nutr. Rev. 2006, 64, 15–30. [Google Scholar] [CrossRef]
- Juriol, L.V.; Gobetto, M.N.; Mendes Garrido Abregú, F.; Dasso, M.E.; Pineda, G.; Güttlein, L.; Carranza, A.; Podhajcer, O.; Toblli, J.E.; Elesgaray, R.; et al. Cardiac changes in apoptosis, inflammation, oxidative stress, and nitric oxide system induced by prenatal and postnatal zinc deficiency in male and female rats. Eur. J. Nutr. 2018, 57, 569–583. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.D.; Vijaya, M.; Samy, R.P.; Dheen, S.T.; Ren, M.; Watt, F.; Kang, Y.J.; Bay, B.H.; Tay, S.S. Zinc supplementation prevents cardiomyocyte apoptosis and congenital heart defects in embryos of diabetic mice. Free Radic. Biol. Med. 2012, 53, 1595–1606. [Google Scholar] [CrossRef] [PubMed]
- Peña, M.M.; Lee, J.; Thiele, D.J. A delicate balance: Homeostatic control of copper uptake and distribution. J. Nutr. 1999, 129, 1251–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, J.Y.; Overmann, G.J.; Keen, C.L.; Clegg, M.S.; Daston, G.P. Cardiac abnormalities induced by zinc deficiency are associated with alterations in the expression of genes regulated by the zinc-finger transcription factor GATA-4. Birth Defects Res. B Dev. Reprod. Toxicol. 2004, 71, 102–109. [Google Scholar] [CrossRef]
- Yuasa, S.; Onizuka, T.; Shimoji, K.; Ohno, Y.; Kageyama, T.; Yoon, S.H.; Egashira, T.; Seki, T.; Hashimoto, H.; Nishiyama, T.; et al. Zac1 is an essential transcription factor for cardiac morphogenesis. Circ. Res. 2010, 106, 1083–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martín, I.; Gibert, M.J.; Pintos, C.; Noguera, A.; Besalduch, A.; Obrador, A. Oxidative stress in mothers who have conceived fetus with neural tube defects: The role of aminothiols and selenium. Clin. Nutr. 2004, 23, 507–514. [Google Scholar] [CrossRef]
- Cengiz, B.; Söylemez, F.; Oztürk, E.; Cavdar, A.O. Serum zinc, selenium, copper, and lead levels in women with second-trimester induced abortion resulting from neural tube defects: A preliminary study. Biol. Trace. Elem. Res. 2004, 97, 225–235. [Google Scholar] [CrossRef]
- Hammouda, S.A.; Abd Al-Halim, O.A.; Mohamadin, A.M. Serum levels of some micronutrients and congenital malformations: A prospective cohort study in healthy saudi-arabian first-trimester pregnant women. Int. J. Vitam. Nutr. Res. 2013, 83, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Pi, X.; Wei, Y.; Li, Z.; Jin, L.; Liu, J.; Zhang, Y.; Wang, L.; Ren, A. Higher concentration of selenium in placental tissues is associated with reduced risk for orofacial clefts. Clin. Nutr. 2019, 38, 2442–2448. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.D.; Uthus, E.O.; Finley, J.W. Dietary selenium and arsenic affect DNA methylation in vitro in Caco-2 cells and in vivo in rat liver and colon. J. Nutr. 2000, 130, 2903–2909. [Google Scholar] [CrossRef] [PubMed]
- Pilsner, J.R.; Hall, M.N.; Liu, X.; Ahsan, H.; Ilievski, V.; Slavkovich, V.; Levy, D.; Factor-Litvak, P.; Graziano, J.H.; Gamble, M.V. Associations of plasma selenium with arsenic and genomic methylation of leukocyte DNA in Bangladesh. Environ. Health Perspect. 2011, 119, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Bosco, J.L.; Tseng, M.; Spector, L.G.; Olshan, A.F.; Bunin, G.R. Reproducibility of reported nutrient intake and supplement use during a past pregnancy: A report from the Children’s Oncology Group. Paediatr. Perinat. Epidemiol. 2010, 24, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunin, G.R.; Gyllstrom, M.E.; Brown, J.E.; Kahn, E.B.; Kushi, L.H. Recall of diet during a past pregnancy. Am. J. Epidemiol. 2001, 154, 1136–1142. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Cases (N = 474) | Controls (N = 948) | p | |
|---|---|---|---|
| Socio-demographic characteristics, % | |||
| Maternal age ≥ 30 years | 33.5 | 34.2 | 0.812 |
| Urban residence | 66.0 | 71.6 | 0.030 |
| Maternal education, senior high school or above | 58.9 | 80.7 | <0.001 |
| Maternal work, farmers | 49.5 | 21.0 | <0.001 |
| Nulliparity | 57.8 | 80.3 | <0.001 |
| Maternal health-related factors in the first trimester, % | |||
| Folate/iron supplements use | 76.6 | 89.2 | <0.001 |
| Passive smoking | 33.5 | 9.3 | <0.001 |
| Medication use | 41.6 | 30.4 | <0.001 |
| Anemia | 16.9 | 10.9 | <0.001 |
| Neonatal gender, male, % | 52.3 | 49.7 | 0.348 |
| Dietary diversity score, median (25th percentile, 75th percentile) | 5.0 (3.0, 6.0) | 6.0 (4.0, 8.0) | <0.001 |
| Daily components intake during pregnancy, median (25th percentile, 75th percentile) | |||
| Total energy, kcal | 1753.2 (1452.4, 2086.1) | 1907.1 (1563.3, 2415.9) | 0.001 |
| Total zinc, mg | 5.1 (3.2, 7.3) | 7.2 (5.1, 10.9) | <0.001 |
| Dietary zinc, mg | 4.7 (3.1, 6.8) | 6.4 (4.6, 9.1) | <0.001 |
| Total copper, mg | 1.6 (1.1, 2.1) | 2.0 (1.4, 2.7) | <0.001 |
| Dietary copper, mg | 1.6 (1.1, 2.1) | 1.9 (1.2, 2.5) | <0.001 |
| Total selenium, mg | 23.2 (15.4, 32.8) | 32.5 (22.7, 46.6) | <0.001 |
| Dietary selenium, mg | 22.7 (15.1, 32.6) | 30.9 (21.9, 43.7) | <0.001 |
| Total zinc to copper ratio | 3.2 (2.4, 4.4) | 3.8 (3.1, 4.8) | <0.001 |
| Dietary zinc to copper ratio | 3.1 (2.4, 4.2) | 3.6 (3.0, 4.5) | <0.001 |
| Total selenium to copper ratio | 14.7 (10.8, 20.7) | 16.7 (13.5, 21.6) | <0.001 |
| Dietary selenium to copper ratio | 14.7 (10.8, 20.9) | 17.2 (13.7, 22.7) | <0.001 |
| Total zinc to selenium ratio | 0.21 (0.18, 0.25) | 0.22 (0.19, 0.27) | 0.280 |
| Dietary zinc to selenium ratio | 0.21 (0.18, 0.25) | 0.21 (0.18, 0.23) | 0.270 |
| Cutoffs | Total CHDs (Ncases = 474) | VSD (Ncases = 223) | ASD (Ncases = 218) | |||
|---|---|---|---|---|---|---|
| Cases/Controls | Unadjusted OR (95%CI) | Adjusted OR (95%CI) 1 | Adjusted OR (95%CI) 1 | Adjusted OR (95%CI) 1 | ||
| Total zinc intake (mg/d) | ||||||
| Quartile 1 | <5.09 | 241/236 | 1 | 1 | 1 | 1 |
| Quartile 2 | 5.09–7.21 | 110/238 | 0.45 (0.34, 0.60) | 0.65 (0.45, 0.94) | 0.71 (0.39, 1.27) | 0.61 (0.36, 1.03) |
| Quartile 3 | 7.21–10.86 | 82/237 | 0.34 (0.25, 0.46) | 0.57 (0.36, 0.91) | 0.53 (0.32, 0.86) | 0.55 (0.32, 0.96) |
| Quartile 4 | ≥10.86 | 41/237 | 0.17 (0.12, 0.25) | 0.22 (0.12, 0.42) | 0.14 (0.05, 0.35) | 0.21 (0.09, 0.48) |
| p for trend 2 | <0.001 | <0.001 | 0.002 | 0.001 | ||
| Total copper intake (mg/d) | ||||||
| Quartile 1 | <1.37 | 153/237 | 1 | 1 | 1 | 1 |
| Quartile 2 | 1.37–1.95 | 167/237 | 1.10 (0.82, 1.46) | 1.26 (0.90, 1.77) | 1.30 (0.84, 2.03) | 1.19 (0.77, 1.85) |
| Quartile 3 | 1.95–2.70 | 103/237 | 0.66 (0.48, 0.90) | 1.24 (0.82, 1.85) | 1.37 (0.81, 2.31) | 1.13 (0.68, 1.88) |
| Quartile 4 | ≥2.70 | 51/237 | 0.33 (0.23, 0.47) | 0.66 (0.38, 1.16) | 0.77 (0.37, 1.64) | 0.54 (0.26, 1.14) |
| p for trend 2 | <0.001 | 0.534 | 0.943 | 0.344 | ||
| Total selenium intake (mg/d) | ||||||
| Quartile 1 | <22.68 | 227/237 | 1 | 1 | 1 | 1 |
| Quartile 2 | 22.68–32.45 | 124/237 | 0.55 (0.41, 0.73) | 0.70 (0.50, 0.99) | 0.64 (0.40, 1.01) | 0.71 (0.45, 1.13) |
| Quartile 3 | 32.45–46.61 | 76/237 | 0.33 (0.24, 0.46) | 0.52 (0.33, 0.81) | 0.47 (0.26, 0.85) | 0.55 (0.31, 0.98) |
| Quartile 4 | ≥46.51 | 47/237 | 0.21 (0.14, 0.30) | 0.29 (0.15, 0.54) | 0.13 (0.05, 0.34) | 0.25 (0.11, 0.59) |
| P for trend 2 | <0.001 | 0.009 | <0.001 | 0.003 | ||
| Total zinc to copper ratio | ||||||
| Quartile 1 | <3.10 | 225/237 | 1 | 1 | 1 | 1 |
| Quartile 2 | 3.10–3.84 | 92/237 | 0.41 (0.30, 0.55) | 0.59 (0.41, 0.84) | 0.64 (0.41, 1.00) | 0.67 (0.43, 1.05) |
| Quartile 3 | 3.84–4.81 | 69/237 | 0.31 (0.22, 0.42) | 0.43 (0.29, 0.63) | 0.42 (0.26, 0.70) | 0.40 (0.24, 0.67) |
| Quartile 4 | ≥4.81 | 88/237 | 0.39 (0.29, 0.53) | 0.58 (0.41, 0.82) | 0.49 (0.30, 0.78) | 0.66 (0.44, 0.98) |
| p for trend 2 | <0.001 | <0.001 | <0.001 | 0.017 | ||
| Total selenium to copper ratio | ||||||
| Quartile 1 | <13.48 | 197/237 | 1 | 1 | 1 | 1 |
| Quartile 2 | 13.48–16.68 | 101/237 | 0.51 (0.38, 0.69) | 0.65 (0.46, 0.92) | 0.58 (0.37, 0.91) | 0.96 (0.62, 1.48) |
| Quartile 3 | 16.68–21.61 | 75/237 | 0.38 (0.28, 0.52) | 0.45 (0.31, 0.65) | 0.36 (0.22, 0.59) | 0.48 (0.29, 0.78) |
| Quartile 4 | ≥21.61 | 101/237 | 0.51 (0.38, 0.69) | 0.65 (0.46, 0.93) | 0.48 (0.30, 0.77) | 0.70 (0.44, 1.10) |
| p for trend 2 | <0.001 | 0.002 | <0.001 | 0.019 | ||
| Total zinc to selenium ratio | ||||||
| Quartile 1 | <0.19 | 139/237 | 1 | 1 | 1 | 1 |
| Quartile 2 | 0.19–0.22 | 127/237 | 0.91 (0.68, 1.23) | 0.86 (0.60, 1.22) | 0.94 (0.59, 1.50) | 0.88 (0.56, 1.38) |
| Quartile 3 | 0.22–0.27 | 119/237 | 0.86 (0.63, 1.16) | 1.02 (0.71, 1.45) | 1.34 (0.84, 2.14) | 0.99 (0.63, 1.56) |
| Quartile 4 | ≥0.27 | 89/237 | 0.64 (0.46, 0.88) | 0.84 (0.58, 1.23) | 1.07 (0.65, 1.76) | 0.94 (0.59, 1.50) |
| p for trend 2 | 0.008 | 0.588 | 0.451 | 0.925 | ||
| Total CHDs (Ncases = 474) | VSD (Ncases = 223) | ASD (Ncases = 218) | |||
|---|---|---|---|---|---|
| Cases/Controls | Unadjusted OR (95%CI) | Adjusted OR (95%CI) 1 | Adjusted OR (95%CI) 1 | Adjusted OR (95%CI) 1 | |
| Total zinc intake | |||||
| Below the RNI | 406/639 | 1 | 1 | 1 | 1 |
| Met the RNI | 68/309 | 0.35 (0.26, 0.46) | 0.56 (0.37, 0.84) | 0.46 (0.26, 0.82) | 0.53 (0.31, 0.91) |
| p | <0.001 | 0.006 | 0.009 | 0.021 | |
| Total copper intake | |||||
| Below the RNI | 72/80 | 1 | 1 | 1 | 1 |
| Met the RNI | 402/868 | 0.51 (0.37, 0.72) | 0.96 (0.63, 1.47) | 0.91 (0.53, 1.55) | 0.85 (0.50, 1.44) |
| p | <0.001 | 0.860 | 0.728 | 0.540 | |
| Total selenium intake | |||||
| Below the RNI | 460/837 | 1 | 1 | 1 | 1 |
| Met the RNI | 14/111 | 0.23 (0.13, 0.40) | 0.23 (0.11, 0.49) | 0.17 (0.05, 0.51) | 0.18 (0.07, 0.47) |
| p | <0.001 | <0.001 | 0.002 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Kang, Y.; Chang, Q.; Zhang, B.; Liu, X.; Zeng, L.; Yan, H.; Dang, S. Maternal Zinc, Copper, and Selenium Intakes during Pregnancy and Congenital Heart Defects. Nutrients 2022, 14, 1055. https://doi.org/10.3390/nu14051055
Yang J, Kang Y, Chang Q, Zhang B, Liu X, Zeng L, Yan H, Dang S. Maternal Zinc, Copper, and Selenium Intakes during Pregnancy and Congenital Heart Defects. Nutrients. 2022; 14(5):1055. https://doi.org/10.3390/nu14051055
Chicago/Turabian StyleYang, Jiaomei, Yijun Kang, Qianqian Chang, Binyan Zhang, Xin Liu, Lingxia Zeng, Hong Yan, and Shaonong Dang. 2022. "Maternal Zinc, Copper, and Selenium Intakes during Pregnancy and Congenital Heart Defects" Nutrients 14, no. 5: 1055. https://doi.org/10.3390/nu14051055
APA StyleYang, J., Kang, Y., Chang, Q., Zhang, B., Liu, X., Zeng, L., Yan, H., & Dang, S. (2022). Maternal Zinc, Copper, and Selenium Intakes during Pregnancy and Congenital Heart Defects. Nutrients, 14(5), 1055. https://doi.org/10.3390/nu14051055