
The Use of Portion Control Plates to Promote Healthy Eating and Diet-Related Outcomes: A Scoping Review

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Information Sources
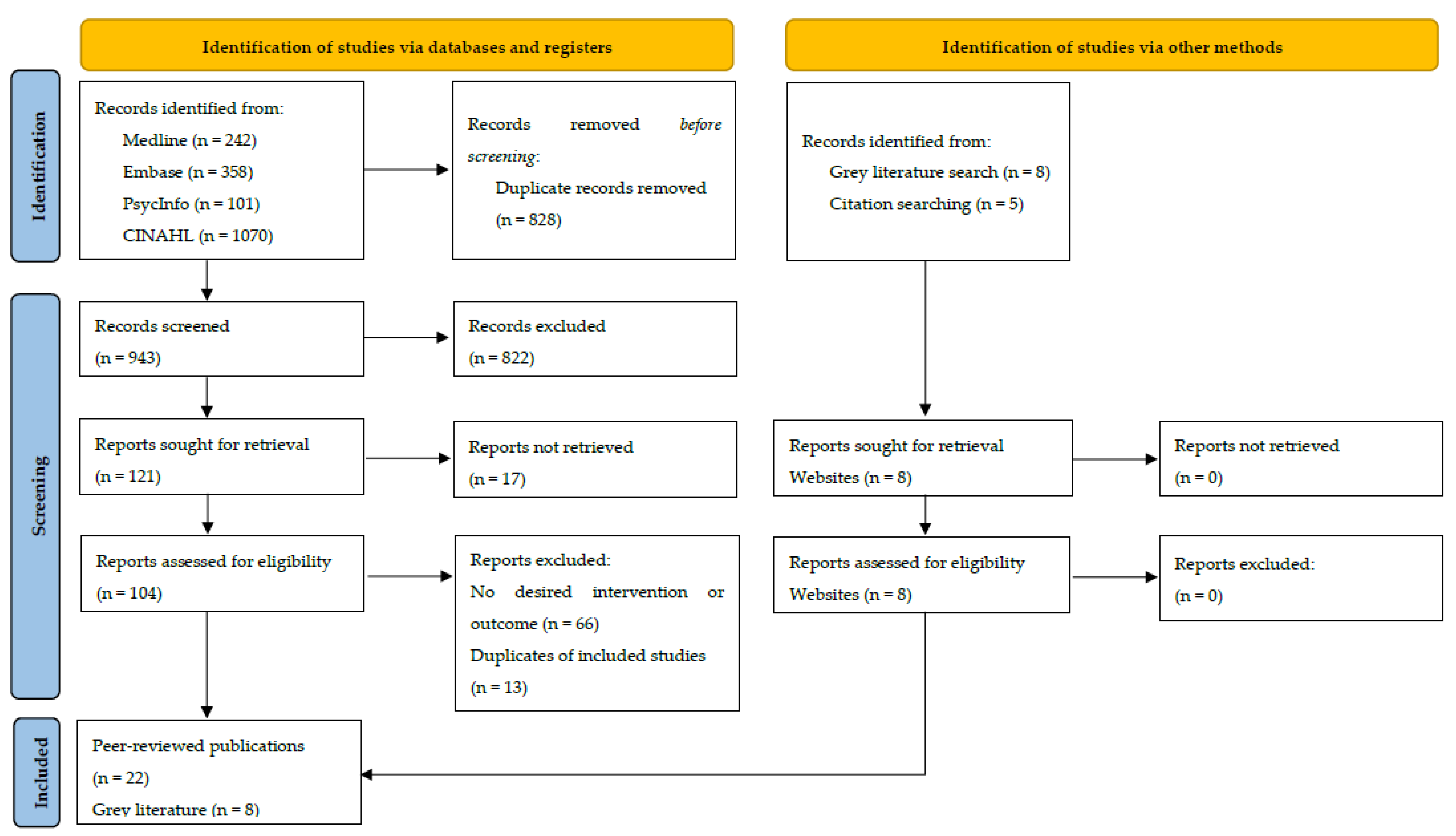
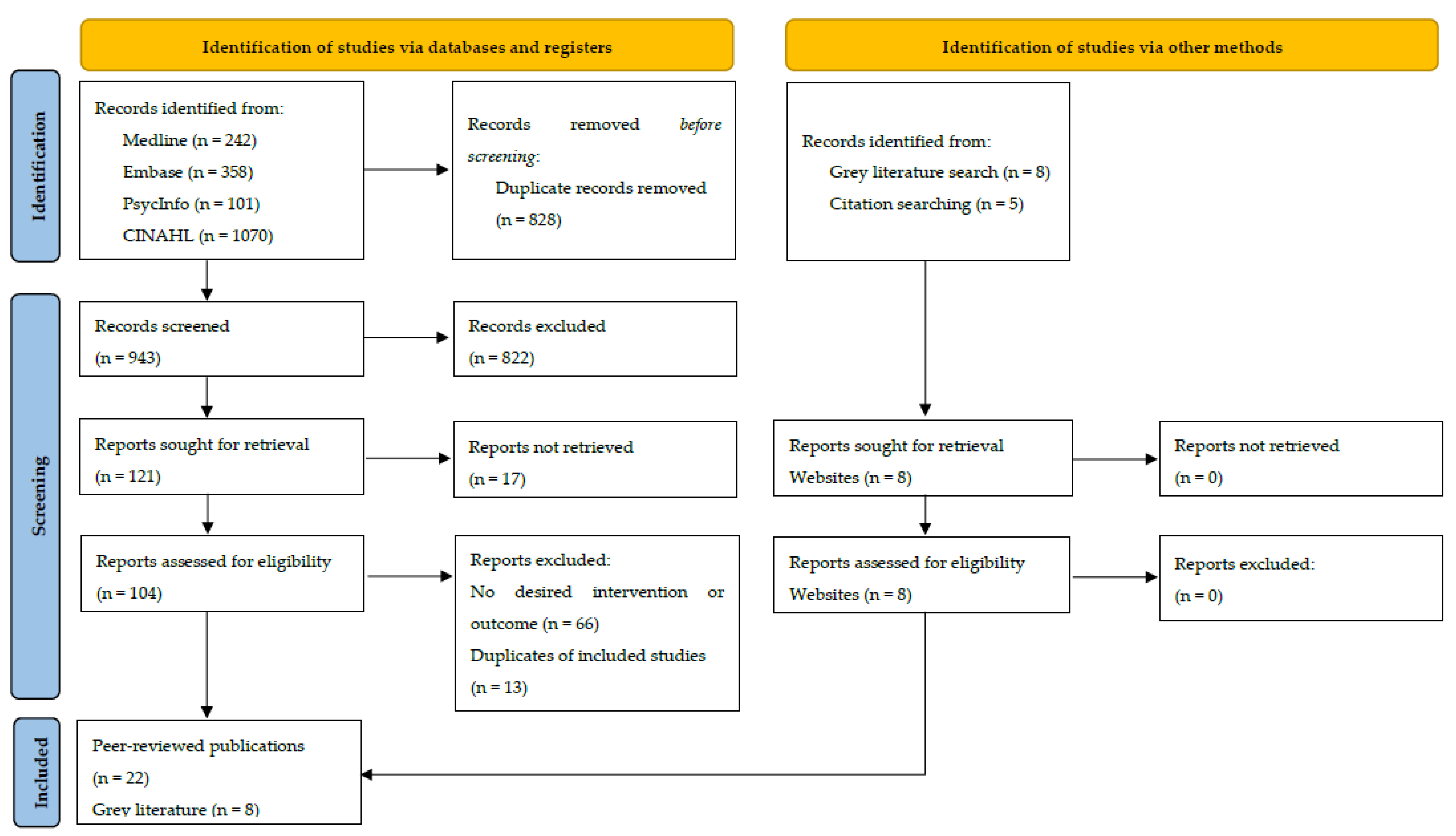
2.3. Screening and Study Selection
2.4. Data Extraction and Presentation of Results
2.5. Quality Appraisal
3. Results
3.1. Changes in Nutrition Knowledge and Dietary Behaviours
3.1.1. Adults (n = 10)
3.1.2. Children and Adolescents (n = 7)
3.1.3. Adults with Obesity and/or Type 2 Diabetes
3.2. Portion Control Plate Characteristics
3.2.1. Plate Size, Proportions, Food Groups, and Imagery
3.2.2. Portion Control Plate Characteristics for Children and Adolescents
3.2.3. Portion Control Plate Characteristics for Weight-Loss Interventions and T2DM
3.2.4. Portion Control Plate Characteristics for Pregnant Women
3.2.5. Portion Control Plate Characteristics for Aboriginal and Torres Strait Islander Peoples
3.3. Primary Uses of Portion Control Plates Identified from Grey Literature
3.3.1. Portion Control Plate for Commercial Purposes
3.3.2. Portion Control Plate Developed by Non-Profit Organisation
4. Discussion
Implications, Strengths, and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Melaku, Y.A.; Renzaho, A.; Gill, T.K.; Taylor, A.W.; Dal Grande, E.; de Courten, B.; Baye, E.; Gonzalez-Chica, D.; Hyppönen, E.; Shi, Z.; et al. Burden and trend of diet-related non-communicable diseases in Australia and comparison with 34 OECD countries, 1990–2015: Findings from the Global Burden of Disease Study 2015. Eur. J. Nutr. 2019, 58, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Australian Dietary Guidelines. In Canberra: National Health and Medical Research Council; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare. Australian Burden of Disease Study: Impact and Causes of Illness and Death in Australia 2011; AIHW: Canberra, Australia, 2016.
- Leenders, M.; Sluijs, I.; Ros, M.M.; Boshuizen, H.C.; Siersema, P.D.; Ferrari, P.; Weikert, C.; Tjønneland, A.; Olsen, A.; Boutron-Ruault, M.-C.; et al. Fruit and Vegetable Consumption and Mortality: European Prospective Investigation into Cancer and Nutrition. Am. J. Epidemiol. 2013, 178, 590–602. [Google Scholar] [CrossRef] [PubMed]
- Ruel, G.; Shi, Z.; Zhen, S.; Zuo, H.; Kröger, E.; Sirois, C.; Lévesque, J.-F.; Taylor, A. Association between nutrition and the evolution of multimorbidity: The importance of fruits and vegetables and whole grain products. Clin. Nutr. 2014, 33, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef]
- Li, J.; Lee, D.H.; Hu, J.; Tabung, F.K.; Li, Y.; Bhupathiraju, S.N.; Rimm, E.B.; Rexrode, K.M.; Manson, J.E.; Willett, W.C.; et al. Dietary Inflammatory Potential and Risk of Cardiovascular Disease Among Men and Women in the U.S. J. Am. Coll. Cardiol. 2020, 76, 2181–2193. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean Diet and Cardiovascular Health. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Moore, L.V.; Thompson, F.E. Adults Meeting Fruit and Vegetable Intake Recommendations—United States, 2013. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 709–713. [Google Scholar]
- Nour, M.; Sui, Z.; Grech, A.; Rangan, A.; McGeechan, K.; Allman-Farinelli, M. The fruit and vegetable intake of young Australian adults: A population perspective. Public Health Nutr. 2017, 20, 2499–2512. [Google Scholar] [CrossRef] [Green Version]
- Food Standards Agency and Public Health England. NDNS: Time Trend and Income Analyses for Years 1 to 9; Public Health England: London, UK, 2019.
- Vandevijvere, S.; Jaacks, L.M.; Monteiro, C.A.; Moubarac, J.-C.; Girling-Butcher, M.; Lee, A.C.; Pan, A.; Bentham, J.; Swinburn, B. Global trends in ultraprocessed food and drink product sales and their association with adult body mass index trajectories. Obes. Rev. 2019, 20, 10–19. [Google Scholar] [CrossRef]
- Hendrie, G.A.; Golley, R.K.; Noakes, M. Compliance with Dietary Guidelines Varies by Weight Status: A Cross-Sectional Study of Australian Adults. Nutrients 2018, 10, 197. [Google Scholar] [CrossRef] [Green Version]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. 1999, 29 Pt 1, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Chandon, P.; Wansink, B. Does food marketing need to make us fat? A review and solutions. Nutr. Rev. 2012, 70, 571–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef] [PubMed]
- The Social Deck Pty Ltd. National Obesity Strategy Consultation Report; COAG Health Council: Canberra, Australia, 2020.
- Mozaffarian, D.; Forouhi, N.G. Dietary guidelines and health-is nutrition science up to the task? BMJ 2018, 360, k822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolodinsky, J.; Harvey-Berino, J.R.; Berlin, L.; Johnson, R.K.; Reynolds, T.W. Knowledge of Current Dietary Guidelines and Food Choice by College Students: Better Eaters Have Higher Knowledge of Dietary Guidance. J. Am. Diet. Assoc. 2007, 107, 1409–1413. [Google Scholar] [CrossRef] [PubMed]
- Spronk, I.; Kullen, C.; Burdon, C.; O’Connor, H. Relationship between nutrition knowledge and dietary intake. Br. J. Nutr. 2014, 111, 1713–1726. [Google Scholar] [CrossRef] [Green Version]
- Paquette, M.C. Perceptions of healthy eating: State of knowledge and research gaps. Can. J. Public Health 2005, 96 (Suppl. S3), S6–S21. [Google Scholar]
- Worsley, A.; Wang, W.C.; Byrne, S.; Yeatman, H. Different patterns of Australian adults’ knowledge of foods and nutrients related to metabolic disease risk. J. Nutr. Sci. 2014, 3, e14. [Google Scholar] [CrossRef] [Green Version]
- Hendrie, G.A.; Coveney, J.; Cox, D. Exploring nutrition knowledge and the demographic variation in knowledge levels in an Australian community sample. Public Health Nutr. 2008, 11, 1365–1371. [Google Scholar] [CrossRef] [Green Version]
- Mötteli, S.; Keller, C.; Siegrist, M.; Barbey, J.; Bucher, T. Consumers’ practical understanding of healthy food choices: A fake food experiment. Br. J. Nutr. 2016, 116, 559–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bucher, T.; Müller, B.; Siegrist, M. What is healthy food? Objective nutrient profile scores and subjective lay evaluations in comparison. Appetite 2015, 95, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Tapsell, L.C.; Neale, E.P.; Satija, A.; Hu, F.B. Foods, Nutrients, and Dietary Patterns: Interconnections and Implications for Dietary Guidelines. Adv. Nutr. 2016, 7, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Ludwig, D.S. Dietary Guidelines in the 21st Century—A Time for Food. JAMA 2010, 304, 681–682. [Google Scholar] [CrossRef] [PubMed]
- Florentino, R.F.; Tee, E.; Hardinsyah, R.; Ismail, M.N.; Suthutvoravut, U.; Hop, L.T. Food-Based Dietary Guidelines of Southeast Asian Countries: Part 2—Analysis of Pictorial Food Guides. Malays. J. Nutr. 2016, 22 (Suppl. S22), S49–S65. [Google Scholar]
- Koenig, J.S. Visualization of Food-Based Dietary Guidelines—Examples. Ann. Nutr. Metab. 2007, 51 (Suppl. S2), 36–43. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for E. Food-Based Dietary Guidelines in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Danmark, 2003. [Google Scholar]
- Montagnese, C.; Santarpia, L.; Iavarone, F.; Strangio, F.; Caldara, A.R.; Silvestri, E.; Contaldo, F.; Pasanisi, F. North and South American countries food-based dietary guidelines: A comparison. Nutrition 2017, 42, 51–63. [Google Scholar] [CrossRef]
- Camelon, K.M.; Hådell, K.; Jämsén, P.T.; Ketonen, K.J.; Kohtamäki, H.M.; Mäkimatilla, S.; Törmälä, M.-L.; Valve, R.H. The Plate Model: A Visual Method of Teaching Meal Planning. J. Am. Diet. Assoc. 1998, 98, 1155–1158. [Google Scholar] [CrossRef]
- Levine, E.; Abbatangelo-Gray, J.; Mobley, A.R.; McLaughlin, G.R.; Herzog, J. Evaluating MyPlate: An Expanded Framework Using Traditional and Nontraditional Metrics for Assessing Health Communication Campaigns. J. Nutr. Educ. Behav. 2012, 44, S2–S12. [Google Scholar] [CrossRef] [Green Version]
- Rolls, B.J. What is the role of portion control in weight management? Int. J. Obes. 2014, 38 (Suppl. S1), S1–S8. [Google Scholar] [CrossRef] [Green Version]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Haddaway, N.R.; Collins, A.; Coughlin, D.; Kirk, S.A. The role of Google Scholar in evidence reviews and its applicability to grey literature searching. PLoS ONE 2015, 10, e0138237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Lukomskyj, N.; Allman-Farinelli, M.; Shi, Y.; Rangan, A. Dietary exposures in childhood and adulthood and cardiometabolic outcomes: A systematic scoping review. J. Hum. Nutr. Diet. 2021, 34, 511–523. [Google Scholar] [CrossRef]
- Huber, J.M.; Shapiro, J.S.; Wieland, M.L.; Croghan, I.T.; Douglas, K.S.V.; Schroeder, D.R.; Hathaway, J.C.; Ebbert, J.O. Telecoaching plus a portion control plate for weight care management: A randomized trial. Trials 2015, 16, 323. [Google Scholar] [CrossRef] [Green Version]
- Kesman, R.L.; Ebbert, J.O.; Harris, K.I.; Schroeder, D.R. Portion control for the treatment of obesity in the primary care setting. BMC Res. Notes 2011, 4, 346. [Google Scholar] [CrossRef] [Green Version]
- Almiron-Roig, E.; Domínguez, A.; Vaughan, D.; Solis-Trapala, I.; Jebb, S.A. Acceptability and potential effectiveness of commercial portion control tools amongst people with obesity. Br. J. Nutr. 2016, 116, 1974–1983. [Google Scholar] [CrossRef] [Green Version]
- Jessica, B.; Joanne, C.; Amy, T.; Diana Cuy, C. Translating MyPlate into Food Selections that Meet Dietary Guidelines Recommendations. J. Hum. Sci. Ext. 2016, 4, 111–123. [Google Scholar]
- Bohnert, A.M.; Randall, E.T.; Tharp, S.; Germann, J. The development and evaluation of a portion plate for youth: A pilot study. J. Nutr. Educ. Behav. 2011, 43, 268–273. [Google Scholar] [CrossRef]
- Hughes, J.W.; Goldstein, C.M.; Logan, C.; Mulvany, J.L.; Hawkins, M.A.W.; Sato, A.F.; Gunstad, J. Controlled testing of novel portion control plate produces smaller self-selected portion sizes compared to regular dinner plate. BMC Obes. 2017, 4, 30. [Google Scholar] [CrossRef] [Green Version]
- Ho, J.; Pedersen, S.D.; Virtanen, H.; Nettel-Aguirre, A.; Huang, C. Family Intervention for Obese/Overweight Children Using Portion Control Strategy (FOCUS) for Weight Control: A Randomized Controlled Trial. Glob. Pediatr. Health 2016, 3, 2333794X16669014. [Google Scholar] [CrossRef] [PubMed]
- Kline, G.A.; Kang, J.; Pedersen, S.D. Portion control plate for weight loss in obese patients with type 2 diabetes mellitus: A controlled clinical trial. Arch. Intern. Med. 2007, 167, 1277–1283. [Google Scholar]
- Amaro, H.; Cortés, D.E.; Garcia, S.; Duan, L.; Black, D.S. Video-based grocery shopping intervention effect on purchasing behaviors among latina shoppers. Am. J. Public Health 2017, 107, 800–806. [Google Scholar] [CrossRef]
- Blondin, J.H.; LoGiudice, J.A. Pregnant women’s knowledge and awareness of nutrition. Appl. Nurs. Res. 2018, 39, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Shukaitis, J.; Elnakib, S.; Cara, C. P41 Yumbox: Bringing MyPlate to Preschoolers’ Lunches. J. Nutr. Educ. Behav. 2021, 53, S43. [Google Scholar] [CrossRef]
- Brown, O.N.; O’Connor, L.E.; Savaiano, D. Mobile MyPlate: A Pilot Study Using Text Messaging to Provide Nutrition Education and Promote Better Dietary Choices in College Students. J. Am. Coll. Health 2014, 62, 320–327. [Google Scholar] [CrossRef]
- Edens, P.L. An Evaluation of the Idaho Plate Method for Adults with Type 2 Diabetes and Limited Health Literacy in Rural West Virginia; West Virginia University: Morgantown, WV, USA, 2013; p. 134. [Google Scholar]
- Melnick, E.M.; Li, M. Association of Plate Design with Consumption of Fruits and Vegetables Among Preschool Children. JAMA Pediatr. 2018, 172, 982–983. [Google Scholar] [CrossRef]
- Ellsworth, D.; Ernst, J.; Snelling, A. A mobile farmers’ market brings nutrition education to low-income students. Health Educ. 2015, 115, 171–177. [Google Scholar] [CrossRef]
- Lara, J.; Turbett, E.; Mckevic, A.; Rudgard, K.; Hearth, H.; Mathers, J.C. The Mediterranean diet among British older adults: Its understanding, acceptability and the feasibility of a randomised brief intervention with two levels of dietary advice. Maturitas 2015, 82, 387–393. [Google Scholar] [CrossRef]
- Arcan, C.; Friend, S.; Flattum, C.F.; Story, M.; Fulkerson, J.A. Fill “half your child’s plate with fruits and vegetables”: Correlations with food-related practices and the home food environment. Appetite 2019, 133, 77–82. [Google Scholar] [CrossRef]
- Nydahl, M.; Gustafsson, I.-B.; Eliasson, M.; Karlström, B. A study of attitudes and use of the plate model among various health professionals giving dietary advice to diabetic patients. J. Hum. Nutr. Diet. 1993, 6, 163–170. [Google Scholar] [CrossRef]
- Tagtow, A.; Raghavan, R. Assessing the Reach of MyPlate using National Health and Nutrition Examination Survey Data. J. Acad. Nutr. Diet. 2017, 117, 181–183. [Google Scholar] [CrossRef] [PubMed]
- Wansink, B.; Kranz, S. Who’s Using MyPlate? J. Nutr. Educ. Behav. 2013, 45, 728–732. [Google Scholar] [CrossRef] [PubMed]
- Almiron-Roig, E.; Majumdar, A.; Vaughan, D.; Jebb, S.A. Exploring the Experiences of People with Obesity Using Portion Control Tools-A Qualitative Study. Nutrients 2019, 11, 1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shilts, M.K.; Johns, M.C.; Lamp, C.; Schneider, C.; Townsend, M.S.; Johns, L. A picture is worth a thousand words: Customizing MyPlate for low-literate, low-income families in 4 steps. J. Nutr. Educ. Behav. 2015, 47, 394–396. [Google Scholar] [CrossRef]
- Victorian Aboriginal Community Controlled Health Organisation Inc. Growing up Healthy and Deadly. 2021. Available online: https://www.vaccho.org.au/wd/nutrition/guhd/ (accessed on 15 July 2021).
- Foodbank, WA. Portion Plate—Food Sensations for Adults. 2021. Available online: https://www.superherofoodshq.org.au/foodsensations/product/portion-plate/ (accessed on 15 July 2021).
- Australian Institute of Sport. Nestle Portion Plate 2021. Available online: https://shop.ais.gov.au/Nestle-Portion-Plate (accessed on 15 July 2021).
- Great Ideas in Nutrition. Portion Perfection Plate—Melamine. 2021. Available online: https://www.greatideas.net.au/portion-perfection-plate-melamine.html (accessed on 15 July 2021).
- beBetter Health, Inc. Announces Educational Portion Plates That Support New USDA Food IconAnnounces Educational Portion Plates That Support New USDA Food Icon. 2011. Available online: https://www.bebetter.com/press_2011.06.02.html (accessed on 15 July 2021).
- OHSU Center for Women’s Health. My Pregnancy Plate. 2021. Available online: https://www.ohsu.edu/womens-health/my-pregnancy-plate (accessed on 15 July 2021).
- Kaiser Permanente. Healthy Pregnancy Plate Portland, Oregon, US. 2015 [4]. Available online: http://healthengagement.kaiserpermanente.org/wp-content/uploads/healthy-pregnancy-plate.pdf (accessed on 15 July 2021).
- Nestle Australia Ltd. Select Committee into the Obesity Epidemic in Australia. Submission from Nestle Australia Ltd. July 2018; Updated 18 July 2018. Available online: www.aph.gov.au/DocumentStore.ashx?id=9ce83d5e-847e-468e-a837-25b59e9d4d4c&subId=612908 (accessed on 15 July 2021).
- Karlstrom, B.; Vessby, B.; Eliasson, M. Diet—A Balanced Approach. Diabetes 1988: Proceedings of the 13th Congress of the International Diabetes Federation ICS800; Diabetes: Amsterdam, The Netherlands, 1989; pp. 923–925. [Google Scholar]
- Ministry of Health Singapore. My Healthy Plate Singapore. 2021. Available online: https://www.healthhub.sg/programmes/55/my-healthy-plate (accessed on 20 July 2021).
- Jayawardena, R.; Swarnamali, H.; Ranasinghe, P.; Hills, A.P. Impact of portion-control plates (PCP) on weight reduction: A systematic review and meta-analysis of intervention studies. Obes. Res. Clin. Pract. 2021, 15, 106–113. [Google Scholar] [CrossRef]
- Hollands, G.J.; Shemilt, I.; Marteau, T.M.; Jebb, S.A.; Lewis, H.B.; Wei, Y.; Higgins, J.P.T.; Ogilvie, D. Portion, package or tableware size for changing selection and consumption of food, alcohol and tobacco. Cochrane Database Syst. Rev. 2015, 2015, CD011045. [Google Scholar] [CrossRef] [Green Version]
- Bilman, E.; van Kleef, E.; van Trijp, H. External cues challenging the internal appetite control system—Overview and practical implications. Crit. Rev. Food Sci. Nutr. 2017, 57, 2825–2834. [Google Scholar] [CrossRef]
- Barte, J.C.; ter Bogt, N.C.; Bogers, R.P.; Teixeira, P.J.; Blissmer, B.; Mori, T.A.; Bemelmans, W.J.E. Maintenance of weight loss after lifestyle interventions for overweight and obesity, a systematic review. Obes. Rev. 2010, 11, 899–906. [Google Scholar] [CrossRef]
- Maula, A.; Kai, J.; Woolley, A.K.; Weng, S.; Dhalwani, N.; Griffiths, F.E.; Khunti, K.; Kendrick, D. Educational weight loss interventions in obese and overweight adults with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Diabet. Med. 2020, 37, 623–635. [Google Scholar] [CrossRef] [Green Version]
- Murimi, M.W.; Moyeda-Carabaza, A.F.; Nguyen, B.; Saha, S.; Amin, R.; Njike, V. Factors that contribute to effective nutrition education interventions in children: A systematic review. Nutr. Rev. 2018, 76, 553–580. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.N.; Matheson, D.M. Environmental strategies for portion control in children. Appetite 2015, 88, 33–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhary, A.; Sudzina, F.; Mikkelsen, B.E. Promoting Healthy Eating among Young People-A Review of the Evidence of the Impact of School-Based Interventions. Nutrients 2020, 12, 2894. [Google Scholar] [CrossRef] [PubMed]
- Lee, A. Ride, K. Review of Nutrition among Aboriginal and Torres Strait Islander People; Australian Indigenous Health Bulletin: Perth, Australia, 2018; Volume 18. [Google Scholar]
- Anderson, I.; Robson, B.; Connolly, M.; Al-Yaman, F.; Bjertness, E.; King, A.; Tynan, M.; Madden, R.; Bang, A.; Coimbra, C.E.A.; et al. Indigenous and tribal peoples’ health (The Lancet-Lowitja Institute Global Collaboration): A population study. Lancet 2016, 388, 131–157. [Google Scholar] [CrossRef]
- de Korne, D.F.; Malhotra, R.; Lim, W.Y.; Ong, C.; Sharma, A.; Tan, T.K.; Tan, T.C.; Chong Ng, K.; Østbye, T. Effects of a portion design plate on food group guideline adherence among hospital staff. J. Nutr. Sci. 2017, 6, e60. [Google Scholar] [CrossRef] [Green Version]
- Vargas-Alvarez, M.; Navas-Carretero, S.; Palla, L.; Martínez, J.; Almiron-Roig, E. Impact of Portion Control Tools on Portion Size Awareness, Choice and Intake: Systematic Review and Meta-Analysis. Nutrients 2021, 13, 1978. [Google Scholar] [CrossRef]
- Almiron-Roig, E.; Forde, C.G.; Hollands, G.; Vargas, M.; Brunstrom, J. A review of evidence supporting current strategies, challenges, and opportunities to reduce portion sizes. Nutr. Rev. 2019, 78, 91–114. [Google Scholar] [CrossRef]

{kind=link}
| First Author, Year, Country | Target Population | Study Design, Risk of Bias | Description of Portion Control Plate | Key Findings |
|---|---|---|---|---|
| Amaro 2017 [49] USA | Latinas (grocery shopping) | Quasi-experimental, Low | 2D MyPlate diagram: 1/2 plate FV, 1/4 plate of grains, 1/4 plate of protein, and 1 serve of dairy. | ↑ Knowledge, self-efficacy, and behaviour related to food purchasing. These were maintained for 2 months in a convenience sample of Latinas who viewed videos based on MyPlate. |
| Bachman 2016 [44] USA | Adults 18–65 y | RCT-Crossover, High | 2D MyPlate diagram: 1/2 plate FV, 1/4 plate of grains, 1/4 plate of protein, and 1 serve of dairy. | Meals planned using MyPlate ↓ in total energy, grains, and dairy, and significantly ↑ in FV compared to the 2010 Dietary guidelines. |
| Blondin 2018 [50] USA | Pregnant women | Quasi-experimental, Low | 2D MyPlate diagram: 1/2 plate of FV, 1/4 plate of grains, 1/4 plate of protein, and 1 serve of dairy. | ↑ Nutrition knowledge by 17% in pregnant women following the nutrition education session (including the MyPlate guidelines). |
| Brown 2014 [52] USA | University students | Quasi-experimental, High | 2D MyPlate diagram: 1/2 plate FV, 1/4 plate of grains, 1/4 plate of protein, and 1 serve of dairy. | The intervention group saw ↑ in fruit consumption and showed trend towards ↑ vegetable consumption, compared with the control group. |
| Hughes 2017 [46] USA | General population | Study 1: RCT-Crossover, High | 3D Portion control plate: a 25 cm foam plastic plate with a border of 2 cm, had serving size indicators for FV, grains/starches, and protein. | The self-selected portion size of protein was ↓ on the portion control plate compared to the regular plate. No significant difference was observed for grains and vegetables. |
| General population | Study 2: RCT-Crossover, two studies assessing lunch quality were conducted over three days, High | 3D Portion control plate: a 25 cm foam plastic plate with a border of 2 cm, had serving size indicators for FV, grains/starches, and protein. | The self-selected portion sizes of protein, vegetables, and grains were ↓ on the portion control plate compared to the regular plate. | |
| Lara 2015 [56] UK | Older adults age >50 y | Cross-sectional, Low | 2D Eatwell plate diagram: 5 portions of FV, 1/3 daily food starchy foods, some dairy, some protein sources, and small amounts of foods and drinks high in fat and sugar. | British older adults rated the plate as comprehensible graphic displays of Mediterranean diet guidelines. |
| Nydahl 1993 [58] Sweden | Health professionals | Cross-sectional, High | 2D Plate model: plate divided into 3 sections; smallest part (1/4 plate) represents proteins, other two parts are equal size, representing FV and starch. | Plate tool favourably received by majority of participants. Perceived advantages: simple, concrete tool, easy to use, useful for many populations, message easy to understand and memorise. Disadvantages: not appropriate for elderly, difficult to (a) follow amounts shown on plate, (b) to eat such large amounts of vegetables. |
| Tagtow 2017 [59] USA | General population aged over 16 | Cross-sectional, High | 2D MyPlate diagram: 1/2 plate of FV, 1/4 plate of grains, 1/4 plate of protein, and 1 serve of dairy. | Familiarity with MyPlate appears to be positively correlated with self-perceived diet quality. Familiarity with MyPlate is positively associated with using nutrition information on the menu while ordering foods. |
| Wansink 2013 [60] USA | Adult women (≥2 children at home) | Cross-sectional, High | 2D MyPlate diagram: 1/2 plate of FV, 1/4 plate of grains, 1/4 plate of protein, and 1 serve of dairy. | Early MyPlate adopters found it clear and easy to use, MyPlate familiarity was highest among those who found it easy to understand and who were also familiar with MyPyramid. |
| First Author, Year, Country | Target Population | Study Design, Risk of Bias | Description of Portion Control Plate | Key Findings |
|---|---|---|---|---|
| Shukaitis 2021 [51] USA | Preschool children | Quasi- experimental, Low | 3D Yumbox: bento-style box with labelled compartments (vegetable, fruit, dairy, grain, protein). | Yumbox had a positive influence on the types of foods caretakers pack for their children’s lunches (↑ variety of components, ↑ fruit, ↑ protein, and ↑ dairy across all 3 days, and ↑ vegetables for the first 2 days). |
| Arcan 2019 [57] USA | Children 8–12 y and caregivers | Cross-sectional, High | 2D MyPlate diagram: 1/2 plate of FV, 1/4 plate of grains, 1/4 plate of protein, and 1 serve of dairy. | The ’half plate FV’ message was positively associated with daily FV intake, diet quality, and home food environment (additional weekly family meal, higher parent and child cooking skills, higher home availability of FV). |
| Melnick 2018 [54] USA | Preschool children 3–5 y | Quasi-experimental, High | 3D Segmented plate: plates with segments of FV sections, FV pictures in designated sections. | Segmented plates with FV pictures resulted in a significant ↑ vegetables taken and vegetables consumed, no significant changes to fruit taken or consumed) over 3 days. |
| Ho 2016 [47] Canada | Children 8–16 y, BMI > 85 percentile | RCT, High | 3D Diet plate: commercially available dinner plate with tape-partitioned sections for carbohydrates, proteins, sauces; remainder of plate for vegetables. | Addition of a portion control tool to standard nutritional counselling did not result in a significant change in BMI z score, anthropometric measures, or laboratory markers after 6 months compared to standard nutrition counselling. |
| Shilts 2015 [62] USA | Low literate, low-income families | Qualitative, High | 2D MyPlate diagram: 1/2 FV, 1/4 grains, 1/4 protein, and 1 serve of dairy. | The My Healthy Plate lessons improved parents’ child feeding-related behaviours. My Healthy Plate was perceived as useful and frequently used by parents. A fast-food poster showing common fast-food options (pizza, hamburger, and taco) in MyPlate proportions was developed based on parents’ feedback. |
| Ellsworth 2014 [55] USA | Low-income middle-school students | Quasi-experimental, High | 2D MyPlate diagram: 1/2 plate of FV, 1/4 plate of grains, 1/4 plate of protein, and 1 serve of dairy. | ↑ Nutrition knowledge in middle school students who used a mobile farmers’ market and received nutrition education that involved MyPlate guidelines. |
| Bohnert 2011 [45] USA | African American adolescents | RCT, High | 3D Nutri-plate: brighter colour balanced with more neutral ones; text that was easy to read; designated sections for vegetables, protein, wholegrains, oils; designated visual representations in sections for vegetables, protein, wholegrains, oils. | Quantitative findings: Dining with the Nutri-plate did not appear to influence healthy food selected by participants overall. The Nutri-plate appeared to facilitate ↑ fruit, ↑ unhealthy broccoli, ↓ steamed broccoli, ↓ overall food. Qualitative findings: Participants’ preferences for plate characteristics including: (i) space to put food shown; (ii) recommended portion size shown; (iii) proportion of food groups shown; (iv) brighter colours, food icons, text that was easy to read, and written messages about healthy eating. |
| First Author, Year, Country | Target Population | Study Design, Risk of Bias | Description of Portion Control Plate | Key Findings |
|---|---|---|---|---|
| Almiron-Roig, 2016 [43] UK (Phase 2) | Adults with obesity | RCT-Crossover, High | Guided calibrated crockery set: guided bowl, guided glass, and 3D 23 cm guided plate (three sectors: 1/2 non-starchy vegetables, 1/4 protein, 1/4 plate starch). | Both portion control tools led to significant weight loss and positive dietary behaviours (↑ raw and cooked vegetables, ↓ potatoes and chips) among obese population. Tool type did not show a significant difference on outcome measures. |
| Almiron-Roig, 2019 [61] UK | Adults with obesity | Qualitative, High | Guided calibrated crockery set: guided bowl, guided glass, and 3D 23 cm guided plate (three sectors: 1/2 non-starchy vegetables, 1/4 protein, 1/4 plate starch). | Strong educational benefits were clearly identified: learned appropriate portion sizes, became aware of difference between habitual portions and recommended ones, useful visual aid to compare portions against. |
| Edens, 2013 [53] USA | Adults with T2DM | Quasi-experimental, High | 3D Idaho plate method (IPM): a meal-planning education program for T2DM consumers, including a colourful-illustrated foam placemat (1/2 plate vegetables, 1/4 plate bread/starch/grain, 1/4 plate meat/protein). | The IPM was frequently used in meal planning for all meals, leading to ↑ FV and milk, ↓ high-fat energy dense foods (fried potatoes, French fries, margarine or butter, hotdog. |
| Huber, 2015 [41] USA | Adults with obesity | RCT, Low | 3D Portion control plate: a clear glass plate with black print dividing it into three sections (1/2 ‘vegetables’, 1/4 ‘fish, lean meat, chicken, nuts’, 1/4 ‘potatoes, pasta, rice, beans and wholegrains’). | Participants in intervention group (tele-coaching and portion control plate) had a significant weight loss at 3 months (compared to baseline), but this difference was not significant at 6 months. |
| Kesman, 2011 [42] USA | Adults with obesity | RCT, Low | 3D Portion control plate: clear glass plate with black print dividing it into three sections (1/2 ‘vegetables’, 1/4 ‘fish, lean meat, chicken, nuts’, 1/4 ‘potatoes, pasta, rice, beans and wholegrains’). | Participants in the intervention group (dietary counselling and portion control plate) had a more significant weight reduction at 3 months compared to those in the control group; this difference was not significant at 6 months. |
| Kline 2007 [48] Canada | People with obesity | RCT, High | 3D Diet plate: commercially available dinner plate with tape-partitioned sections for carbohydrates, proteins, and sauces, remainder of the plate for vegetables, plus a breakfast bowl. | Participants in the intervention group lost significantly more weight and had a significantly greater decrease in non-HDL lipoprotein than control group. A greater proportion of intervention group participants required a decrease in hypoglycaemic medication/had a significant decrease in daily insulin dose use at 6 months. |
| Name of Portion Control Plate/Country | Target Population | Branding/Manufacturer | Proportions/Serves/Portions of Major Food Groups | Style of Imagery/Key Messages/Website Link |
|---|---|---|---|---|
| Portion Perfection. Australia. | General population. | Designed by a dietitian. Great Ideas in Nutrition. Commercial. | 1/4 protein, 1/4 low GI carbs, 1/2 salad or free veg, 1 tsp oil or 1 tbsp low fat sauce. | Art imagery: arrows delineate portions. Rim: strategic reminders on plate border for meal satisfaction with Enjoy! Presentation, Variety, Aromas, Textures, Temperature, Flavours. https://www.greatideas.net.au/portion-perfection-plate-melamine.html, accessed 15 July 2021 |
| The Adult Portion Plate. United States of America. | Adults. | BeBetter: Take a better look at your portions. Commercial. | 1/4 meat/proteins, 1/4 wholegrains, 1/2 FV, 1 central portion for fats/oils. | Realistic imagery. Rim: icons engaging in physical activity such as weightlifting, golf, stretching, hula-hooping. https://www.bebetter.com/press_2011.06.02.html, accessed 15 July 2021 |
| Growing up healthy and deadly ‘Healthy Portion Plate’. Australia. | Aboriginal and Torres Strait Islander Children. | Victorian Aboriginal Community Controlled Health Organisation. Non-profit. | 1/4 lean meat/proteins, 1/4 carbs/wholegrains. 1/2 veg/salads. | Indigenous art imagery. https://www.vaccho.org.au/wd/nutrition/guhd/, accessed 15 July 2021 |
| Nestlé® Portion Plate for Kids. Australia. | Children < 8 years. | Australian Institute of Sport and Nestlé® Healthy Active Kids. Commercial. | 1/3 veg/salads, 1/3 protein, 1/3 carbs. | Art imagery. Rim: What’s on your plate kids? Healthy Eating is as easy as 1,2,3. Salad and Veggies section: Keep it Colourful https://shop.ais.gov.au/Nestle-Portion-Plate, accessed 15 July 2021 |
| Nestlé® Portion Plate for Adults. Australia. | Adults. | Nestlé® Choose Wellness: Good Food, Good Life. Commercial. | 1/4 protein (1 serve), 1/4 carbs (2 serves), 1/2 veg (3 serves). | Art imagery. Rim: Know your Portions. Protein section: Choose lean cuts of meat, trim visible fat and take skin off chicken. Carbohydrate section: Choose Low GI or wholegrain varieties. Vegetables section: Choose variety of colours. https://shop.ais.gov.au/Nestle-Portion-Plate, accessed 15 July 2021 |
| Foodbank WA Portion Plate. Australia. | Low-middle income general population. | Foodbank WA. Non-profit. | 1/4 lean meat and alternatives, 1/4 grain foods, 1/2 veg. | Art imagery. https://www.superherofoodshq.org.au/foodsensations/product/portion-plate/, accessed 15 July 2021 |
| My Pregnancy Plate United States of America | Pregnant women | Oregon Health & Science University. Non-profit. | 1/4 protein, 1/4 wholegrains, legumes, 3/8 non-starchy veg, 1/8 fruit. | Realistic imagery. Recommendations for types of proteins, wholegrains, starchy and non-starchy veg and fruit to choose. Recommendations for healthy oils and dairy. https://www.ohsu.edu/womens-health/my-pregnancy-plate, accessed 15 July 2021 |
| Healthy Pregnancy Plate United States of America | Pregnant women | Kaiser Permanente, Foundation. Non-profit. | 1/4 protein, 1/4 grains/starches, 1/2 FV. | Realistic imagery. Recommendations for practicing mindful eating, hydration, physical activity, and limiting added sugar. https://healthy.kaiserpermanente.org/content/dam/kporg/final/documents/health-education-materials/instructions/healthy-pregnancy-plate-hi-en.pdf, accessed 15 July 2021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jia, S.S.; Liu, Q.; Allman-Farinelli, M.; Partridge, S.R.; Pratten, A.; Yates, L.; Stevens, M.; McGill, B. The Use of Portion Control Plates to Promote Healthy Eating and Diet-Related Outcomes: A Scoping Review. Nutrients 2022, 14, 892. https://doi.org/10.3390/nu14040892
Jia SS, Liu Q, Allman-Farinelli M, Partridge SR, Pratten A, Yates L, Stevens M, McGill B. The Use of Portion Control Plates to Promote Healthy Eating and Diet-Related Outcomes: A Scoping Review. Nutrients. 2022; 14(4):892. https://doi.org/10.3390/nu14040892
Chicago/Turabian StyleJia, Si Si, Qingzhou Liu, Margaret Allman-Farinelli, Stephanie R. Partridge, Amy Pratten, Lisa Yates, Matthew Stevens, and Bronwyn McGill. 2022. "The Use of Portion Control Plates to Promote Healthy Eating and Diet-Related Outcomes: A Scoping Review" Nutrients 14, no. 4: 892. https://doi.org/10.3390/nu14040892
APA StyleJia, S. S., Liu, Q., Allman-Farinelli, M., Partridge, S. R., Pratten, A., Yates, L., Stevens, M., & McGill, B. (2022). The Use of Portion Control Plates to Promote Healthy Eating and Diet-Related Outcomes: A Scoping Review. Nutrients, 14(4), 892. https://doi.org/10.3390/nu14040892