
Inverse Regulation of Serum Osteoprotegerin and B-Type Natriuretic Peptide Concentrations by Free Fatty Acids Elevation in Young Healthy Humans

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Glucose Tolerance and Insulin Sensitivity
2.3. Biochemical Procedures
2.4. Statistical Analysis
3. Results
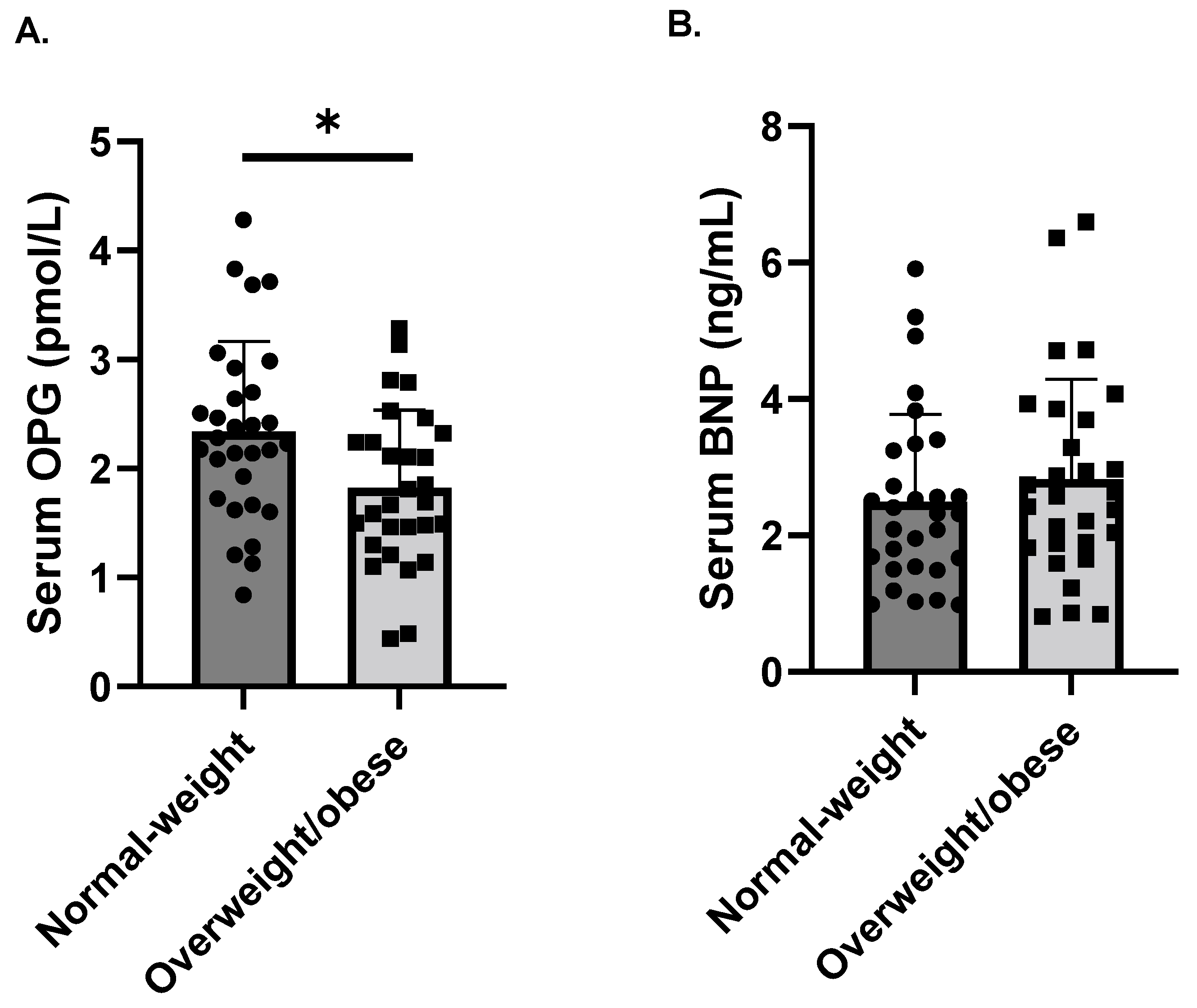
3.1. The Relationship of Circulating OPG and BNP with Other Estimated Parameters
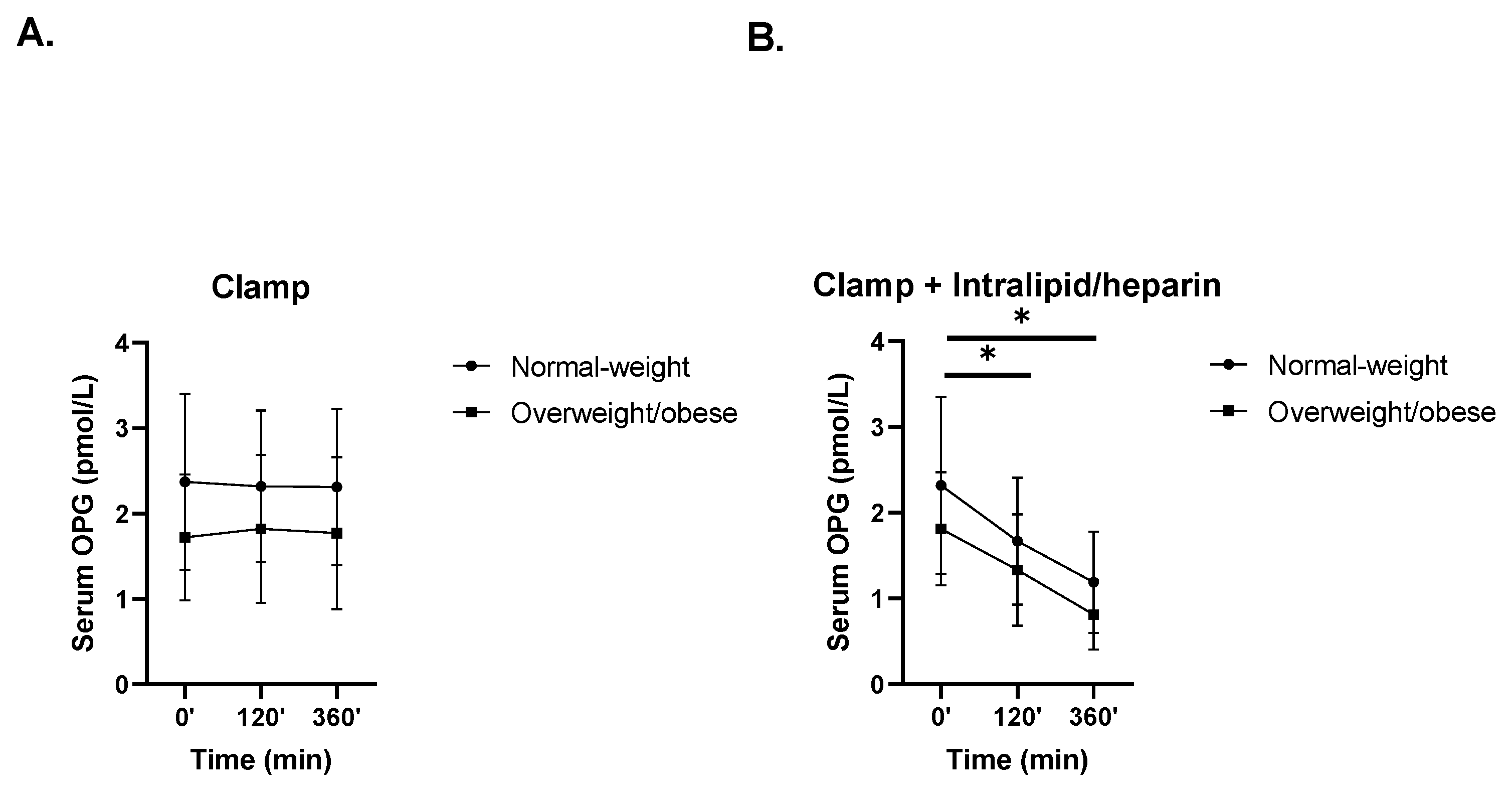
3.2. The Effects of Hyperinsulinemia without or with Intralipid/Heparin Infusion on Circulating OPG Levels
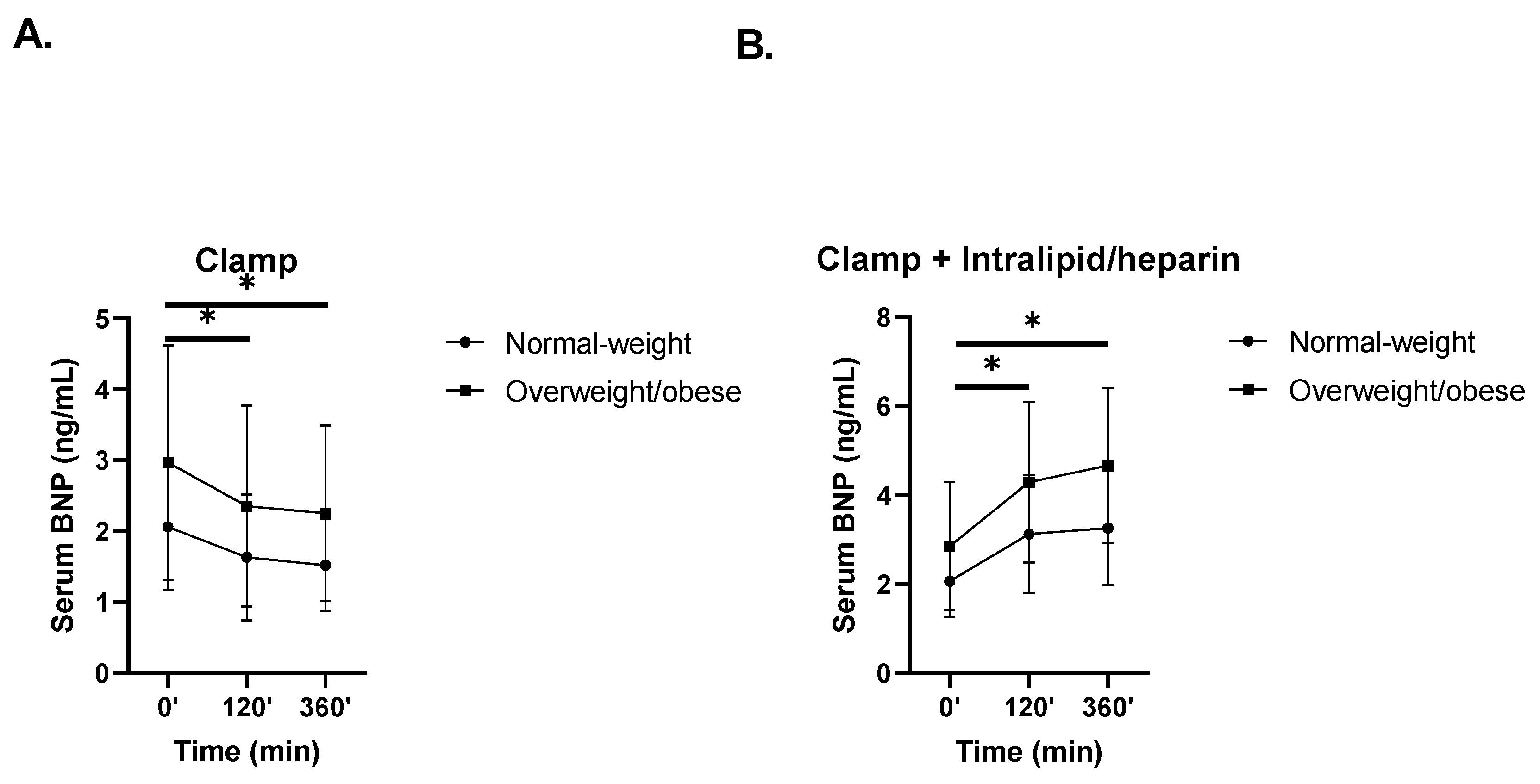
3.3. The Effects of Hyperinsulinemia without or with Intralipid/Heparin Infusion on Circulating BNP Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adeva-Andany, M.M.; Martínez-Rodríguez, J.; González-Lucán, M.; Fernández-Fernández, C.; Castro-Quintela, E. Insulin resistance is a cardiovascular risk factor in humans. Diabetes Metab. Syndr. 2019, 13, 1449–1455. [Google Scholar] [CrossRef]
- di Giuseppe, R.; Biemann, R.; Wirth, J.; Menzel, J.; Isermann, B.; Stangl, G.I.; Fritsche, A.; Boeing, H.; Schulze, M.B.; Weikert, C. Plasma osteoprotegerin, its correlates, and risk of heart failure: A prospective cohort study. Eur. J. Epidemiol. 2017, 32, 113–123. [Google Scholar] [CrossRef]
- Boyce, B.F.; Xing, L. Biology of RANK, RANKL, and osteoprotegerin. Arthritis Res. Ther. 2007, 9 (Suppl. S1), S1. [Google Scholar] [CrossRef] [Green Version]
- Esteghamati, A.; Aflatoonian, M.; Rad, M.V.; Mazaheri, T.; Mousavizadeh, M.; Nakhjavani, M.; Noshad, S. Association of osteoprotegerin with peripheral artery disease in patients with type 2 diabetes. Arch. Cardiovasc. Dis. 2015, 108, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Lieb, W.; Gona, P.; Larson, M.; Massaro, J.; Lipinska, I.; Keaney, J.; Rong, J.; Corey, D.; Hoffmann, U.; Fox, C.S.; et al. Biomarkers of the osteoprotegerin pathway: Clinical correlates, subclinical disease, incident cardiovascular disease, and mortality. Arter. Thromb. Vasc. Biol. 2010, 30, 1849–1854. [Google Scholar] [CrossRef]
- Reinhard, H.; Lajer, M.; Gall, M.-A.; Tarnow, L.; Parving, H.-H.; Rasmussen, L.M.; Rossing, P. Osteoprotegerin and Mortality in Type 2 Diabetic Patients. Diabetes Care 2010, 33, 2561–2566. [Google Scholar] [CrossRef] [Green Version]
- Knudsen, S.T.; Foss, C.H.; Poulsen, P.L.; Andersen, N.H.; Mogensen, C.E.; Rasmussen, L.M. Increased plasma concentrations of osteoprotegerin in type 2 diabetic patients with microvascular complications. Eur. J. Endocrinol. 2003, 149, 39–42. [Google Scholar] [CrossRef] [Green Version]
- Duan, P.; Yang, M.; Wei, M.; Liu, J.; Tu, P. Serum Osteoprotegerin Is a Potential Biomarker of Insulin Resistance in Chinese Postmenopausal Women with Prediabetes and Type 2 Diabetes. Int. J. Endocrinol. 2017, 2017, 8724869. [Google Scholar] [CrossRef]
- Ugur-Altun, B.; Altun, A.; Gerenli, M.; Tugrul, A. The relationship between insulin resistance assessed by HOMA-IR and serum osteoprotegerin levels in obesity. Diabetes Res. Clin. Pract. 2005, 68, 217–222. [Google Scholar] [CrossRef]
- Oh, E.S.; Rhee, E.-J.; Oh, K.W.; Lee, W.Y.; Baek, K.H.; Yoon, K.H.; Kang, M.I.; Yun, E.J.; Park, C.Y.; Choi, M.G.; et al. Circulating osteoprotegerin levels are associated with age, waist-to-hip ratio, serum total cholesterol, and low-density lipoprotein cholesterol levels in healthy Korean women. Metabolism 2005, 54, 49–54. [Google Scholar] [CrossRef]
- Gannage-Yared, M.-H.; Fares, F.; Semaan, M.; Khalife, S.; Jambart, S. Circulating osteoprotegerin is correlated with lipid profile, insulin sensitivity, adiponectin and sex steroids in an ageing male population. Clin. Endocrinol. 2006, 64, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Kotanidou, E.P.; Kotanidis, C.P.; Giza, S.; Serbis, A.; Tsinopoulou, V.-R.; Karalazou, P.; Tzimagiorgis, G.; Galli-Tsinopoulou, A. Osteoprotegerin increases parallel to insulin resistance in obese adolescents. Endocr. Res. 2019, 44, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Musialik, K.; Szulińska, M.; Hen, K.; Skrypnik, D.; Bogdański, P. The relation between osteoprotegerin, inflammatory processes, and atherosclerosis in patients with metabolic syndrome. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 4379–4385. [Google Scholar] [PubMed]
- Hall, C. Essential biochemistry and physiology of (NT-pro) BNP. Eur. J. Heart Fail. 2004, 6, 257–260. [Google Scholar] [CrossRef]
- Chopra, S.; Cherian, D.; Verghese, P.P.; Jacob, J.J. Physiology and clinical significance of natriuretic hormones. Indian J. Endocrinol. Metab. 2013, 17, 83–90. [Google Scholar] [CrossRef]
- Cao, Z.; Jia, Y.; Zhu, B. BNP and NT-proBNP as Diagnostic Biomarkers for Cardiac Dysfunction in Both Clinical and Forensic Medicine. Int. J. Mol. Sci. 2019, 20, 1820. [Google Scholar] [CrossRef] [Green Version]
- York, M.K.; Gupta, D.K.; Reynolds, C.F.; Farber-Eger, E.; Wells, Q.S.; Bachmann, K.N.; Xu, M.; Harrell, F.E.; Wang, T. B-Type Natriuretic Peptide Levels and Mortality in Patients with and Without Heart Failure. J. Am. Coll. Cardiol. 2018, 71, 2079–2088. [Google Scholar] [CrossRef]
- Madamanchi, C.; Alhosaini, H.; Sumida, A.; Runge, M.S. Obesity and natriuretic peptides, BNP and NT-proBNP: Mechanisms and diagnostic implications for heart failure. Int. J. Cardiol. 2014, 176, 611–617. [Google Scholar] [CrossRef] [Green Version]
- Baldassarre, S.; Fragapani, S.; Panero, A.; Fedele, D.; Pinach, S.; Lucchiari, M.; Vitale, A.R.; Mengozzi, G.; Gruden, G.; Bruno, G. NTproBNP in insulin-resistance mediated conditions: Overweight/obesity, metabolic syndrome and diabetes. The population-based Casale Monferrato Study. Cardiovasc. Diabetol. 2017, 16, 119. [Google Scholar] [CrossRef] [Green Version]
- Von Scholten, B.J.; Reinhard, H.; Hansen, T.W.; Lindhardt, M.; Petersen, C.L.; Wiinberg, N.; Hansen, P.R.; Parving, H.-H.; Jacobsen, P.K.; Rossing, P. Additive prognostic value of plasma N-terminal pro-brain natriuretic peptide and coronary artery calcification for cardiovascular events and mortality in asymptomatic patients with type 2 diabetes. Cardiovasc. Diabetol. 2015, 14, 59. [Google Scholar] [CrossRef] [Green Version]
- Mavinkurve, M.; O’Gorman, C.S. Can Brain Natriuretic Peptides and Osteoprotegerin Serve as Biochemical Markers for the Detection of Aortic Pathology in Children and Adolescents with Turner Syndrome? Front. Endocrinol. 2017, 8, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loncar, G.; Bozic, B.; Cvorovic, V.; Radojicic, Z.; Dimkovic, S.; Markovic, N.; Prodanovic, N.; Lepic, T.; Putnikovic, B.; Popovic-Brkic, V. Relationship between RANKL and neuroendocrine activation in elderly males with heart failure. Endocrine 2010, 37, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Makarović, S.; Makarović, Z.; Bilic-Curcic, I.; Milas-Ahić, J.; Mihaljevic, I.; Franceschi, M.; Jukić, T. Serum Osteoprotegerin in Patients with Calcified Aortic Valve Stenosis in Relation to Heart Failure. Acta Clin. Croat. 2017, 56, 733–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palazzuoli, A.; Ascione, R.; Gallotta, M.; Calabrò, A.; Gonnelli, S.; Quatrini, I.; Campagna, M.S.; Franci, B.; Nuti, R. Osteoprotegerin and B-type natriuretic peptide in acute coronary syndromes with preserved systolic function: Relation to coronary artery disease extension. Int. J. Cardiol. 2009, 137, 295–298. [Google Scholar] [CrossRef]
- Karczewska-Kupczewska, M.; Kowalska, I.; Nikolajuk, A.; Adamska, A.; Zielinska, M.; Kaminska, N.; Otziomek, E.; Gorska, M.; Strczkowski, M. Circulating Brain-Derived Neurotrophic Factor Concentration Is Downregulated by Intralipid/Heparin Infusion or High-Fat Meal in Young Healthy Male Subjects. Diabetes Care 2012, 35, 358–362. [Google Scholar] [CrossRef] [Green Version]
- Karczewska-Kupczewska, M.; Stefanowicz, M.; Matulewicz, N.; Nikołajuk, A.; Straczkowski, M. Wnt signaling genes in adipose tissue and skeletal muscle of humans with different degree of insulin sensitivity. J. Clin. Endocrinol. Metab. 2016, 101, 3079–3087. [Google Scholar] [CrossRef] [Green Version]
- Karczewska-Kupczewska, M.; Nikolajuk, A.; Filarski, R.; Majewski, R.; Tarasów, E. Intralipid/Heparin Infusion Alters Brain Metabolites Assessed With 1H-MRS Spectroscopy in Young Healthy Men. J. Clin. Endocrinol. Metab. 2018, 103, 2563–2570. [Google Scholar] [CrossRef]
- Gaudio, A.; Rapisarda, R.; Xourafa, A.; Zanoli, L.; Manfrè, V.; Catalano, A.; Signorelli, S.S.; Castellino, P. Effects of competitive physical activity on serum irisin levels and bone turnover markers. J. Endocrinol. Investig. 2021, 44, 2235–2241. [Google Scholar] [CrossRef]
- Amato, G.; Mazziotti, G.; Sorvillo, F.; Piscopo, M.; Lalli, E.; Biondi, B.; Iorio, S.; Molinari, A.; Giustina, A.; Carella, C. High serum osteoprotegerin levels in patients with hyperthyroidism: Effect of medical treatment. Bone 2004, 35, 785–791. [Google Scholar] [CrossRef]
- Rochette, L.; Meloux, A.; Rigal, E.; Zeller, M.; Cottin, Y.; Vergely, C. The role of osteoprotegerin in the crosstalk between vessels and bone: Its potential utility as a marker of cardiometabolic diseases. Pharmacol. Ther. 2018, 182, 115–132. [Google Scholar] [CrossRef]
- Bernardi, S.; Fabris, B.; Thomas, M.; Toffoli, B.; Tikellis, C.; Candido, R.; Catena, C.; Mulatero, P.; Barbone, F.; Radillo, O.; et al. Osteoprotegerin increases in metabolic syndrome and promotes adipose tissue proinflammatory changes. Mol. Cell. Endocrinol. 2014, 394, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Akinci, B.; Celtik, A.; Yuksel, F.; Genc, S.; Yener, S.; Secil, M.; Ozcan, M.A.; Yesil, S. Increased osteoprotegerin levels in women with previous gestational diabetes developing metabolic syndrome. Diabetes Res. Clin. Pract. 2011, 91, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Bilgir, O.; Yavuz, M.; Bilgir, F.; Akan, O.Y.; Bayindir, A.G.; Calan, M.; Bozkaya, G.; Yuksel, A. Relationship between insulin resistance, hs-CRP, and body fat and serum osteoprotegerin/RANKL in prediabetic patients. Minerva Endocrinol. 2018, 43, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, G.M.; Vind, B.; Nybo, M.; Rasmussen, L.M.; Højlund, K. Acute hyperinsulinemia decreases plasma osteoprotegerin with diminished effect in type 2 diabetes and obesity. Eur. J. Endocrinol. 2009, 161, 95–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dresner, A.; Laurent, D.; Marcucci, M.; Griffin, M.E.; Dufour, S.; Cline, G.W.; Slezak, L.A.; Andersen, D.K.; Hundal, R.S.; Rothman, D.L.; et al. Effects of free fatty acids on glucose transport and IRS-1–associated phosphatidylinositol 3-kinase activity. J. Clin. Investig. 1999, 103, 253–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, E.R.; Musani, S.K.; Bidulescu, A.; Nagarajarao, H.S.; Samdarshi, T.E.; Gebreab, S.Y.; Sung, J.H.; Steffes, M.W.; Wang, T.; Taylor, H.A.; et al. Relation of Obesity to Circulating B-Type Natriuretic Peptide Concentrations in Blacks: The Jackson Heart Study. Circulation 2011, 124, 1021–1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazo, M.; Young, J.H.; Brancati, F.L.; Coresh, J.; Whelton, S.; Ndumele, C.E.; Hoogeveen, R.; Ballantyne, C.M.; Selvin, E. NH2-Terminal Pro–Brain Natriuretic Peptide and Risk of Diabetes. Diabetes 2013, 62, 3189–3193. [Google Scholar] [CrossRef] [Green Version]
- Gruden, G.; Landi, A.; Bruno, G. Natriuretic Peptides, Heart, and Adipose Tissue: New Findings and Future Developments for Diabetes Research. Diabetes Care 2014, 37, 2899–2908. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.J.; Larson, M.; Levy, D.; Benjamin, E.; Leip, E.P.; Wilson, P.W.; Vasan, R.S. Impact of Obesity on Plasma Natriuretic Peptide Levels. Circulation 2004, 109, 594–600. [Google Scholar] [CrossRef] [Green Version]
- Costello-Boerrigter, L.C.; Boerrigter, G.; Redfield, M.M.; Rodeheffer, R.J.; Urban, L.H.; Mahoney, D.W.; Jacobsen, S.; Heublein, D.M.; Burnett, J.C. Amino-Terminal Pro-B-Type Natriuretic Peptide and B-Type Natriuretic Peptide in the General Community: Determinants and Detection of Left Ventricular Dysfunction. J. Am. Coll. Cardiol. 2006, 47, 345–353. [Google Scholar] [CrossRef] [Green Version]
- Kohno, M.; Horio, T.; Yokokawa, K.; Murakawa, K.-I.; Yasunari, K.; Akioka, K.; Tahara, A.; Toda, I.; Takeuchi, K.; Kurihara, N.; et al. Brain natriuretic peptide as a cardiac hormone in essential hypertension. Am. J. Med. 1992, 92, 29–34. [Google Scholar] [CrossRef]
- Halbirk, M.; Nørrelund, H.; Møller, N.; Schmitz, O.; Bøtker, H.E.; Wiggers, H. Short-term changes in circulating insulin and free fatty acids affect Nt-pro-BNP levels in heart failure patients. Int. J. Cardiol. 2010, 144, 140–142. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Tsukada, H.; Seki, G.; Satoh, N.; Mizuno, T.; Fujii, W.; Horita, S.; Moriya, K.; Sato, Y.; Kume, H.; et al. Insulin promotes sodium transport but suppresses gluconeogenesis via distinct cellular pathways in human and rat renal proximal tubules. Kidney Int. 2020, 97, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Nannipieri, M.; Seghieri, G.; Catalano, C.; Prontera, T.; Baldi, S.; Ferrannini, E. Defective Regulation and Action of Atrial Natriuretic Peptide in Type 2 Diabetes. Horm. Metab. Res. 2002, 34, 265–270. [Google Scholar] [CrossRef]
- Zhang, H.; Thoonen, R.; Yao, V.; Buys, E.S.; Popovich, J.; Su, Y.R.; Wang, T.; Scherrer-Crosbie, M. Regulation of B-type natriuretic peptide synthesis by insulin in obesity in male mice. Exp. Physiol. 2016, 101, 113–123. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.P.; Catalano, K.J.; Hsu, I.R.; Chiu, J.D.; Richey, J.M.; Bergman, R.N. Nocturnal free fatty acids are uniquely elevated in the longitudinal development of diet-induced insulin resistance and hyperinsulinemia. Am. J. Physiol. Endocrinol. Metab. 2007, 292, E1590–E1598. [Google Scholar] [CrossRef]
- Jono, S.; Ikari, Y.; Shioi, A.; Mori, K.; Miki, T.; Hara, K.; Nishizawa, Y. Serum Osteoprotegerin Levels Are Associated with the Presence and Severity of Coronary Artery Disease. Circulation 2002, 106, 1192–1194. [Google Scholar] [CrossRef] [Green Version]
- Ueland, T.; Yndestad, A.; Øie, E.; Florholmen, G.; Halvorsen, B.; Frøland, S.S.; Simonsen, S.; Christensen, G.; Gullestad, L.; Aukrust, P. Dysregulated Osteoprotegerin/RANK Ligand/RANK Axis in Clinical and Experimental Heart Failure. Circulation 2005, 111, 2461–2468. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, V.E. Impact of Nutrition on Cardiovascular Function. Curr. Probl. Cardiol. 2020, 45, 100391. [Google Scholar] [CrossRef]
- Cunha, J.S.; Ferreira, V.M.; Maquigussa, E.; Naves, M.A.; Boim, M.A. Effects of high glucose and high insulin concentrations on osteoblast function in vitro. Cell Tissue Res. 2014, 358, 249–256. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Normal-Weight (n = 30) | Overweight/Obese (n = 29) | |
|---|---|---|
| Age (years) | 23.20 ± 2.65 | 23.79 ± 2.55 |
| BMI (kg/m2) | 22.77 ± 1.58 | 28.72 ± 3.05 * |
| Waist circumference (cm) | 82.38 ± 4.41 | 97.14 ± 10.27 * |
| % body fat | 14.23 ± 3.93 | 25.67 ± 7.05 * |
| Systolic blood pressure (mmHg) | 122.0 ± 7.72 | 127.96 ± 6.38 * |
| Diastolic blood pressure (mmHg) | 77.1 ± 6.09 | 81.0 ± 6.9 * |
| Fasting plasma glucose (mg/dL) | 84.21 ± 8.33 | 84.17 ± 7.63 |
| Fasting serum insulin (μIU/mL) | 8.51 ± 3.80 | 13.13 ± 4.80 * |
| Insulin sensitivity (mg/kg ffm/min) | 7.36 ± 2.54 | 5.82 ± 1.92 * |
| Cholesterol (mg/dL) | 163.23 ± 34.10 | 177.96 ± 30.76 |
| Triglycerides (mg/dL) | 76.67 ± 28.17 | 104.84 ± 58.90 * |
| HDL-cholesterol (mg/dL) | 59.49 ± 8.22 | 54.41 ± 7.98 * |
| LDL-cholesterol (mg/dL) | 99.06 ± 37.16 | 104.96 ± 28.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrzycka, M.; Kołakowski, A.; Stefanowicz, M.; Matulewicz, N.; Nikołajuk, A.; Karczewska-Kupczewska, M. Inverse Regulation of Serum Osteoprotegerin and B-Type Natriuretic Peptide Concentrations by Free Fatty Acids Elevation in Young Healthy Humans. Nutrients 2022, 14, 837. https://doi.org/10.3390/nu14040837
Dobrzycka M, Kołakowski A, Stefanowicz M, Matulewicz N, Nikołajuk A, Karczewska-Kupczewska M. Inverse Regulation of Serum Osteoprotegerin and B-Type Natriuretic Peptide Concentrations by Free Fatty Acids Elevation in Young Healthy Humans. Nutrients. 2022; 14(4):837. https://doi.org/10.3390/nu14040837
Chicago/Turabian StyleDobrzycka, Marta, Adrian Kołakowski, Magdalena Stefanowicz, Natalia Matulewicz, Agnieszka Nikołajuk, and Monika Karczewska-Kupczewska. 2022. "Inverse Regulation of Serum Osteoprotegerin and B-Type Natriuretic Peptide Concentrations by Free Fatty Acids Elevation in Young Healthy Humans" Nutrients 14, no. 4: 837. https://doi.org/10.3390/nu14040837
APA StyleDobrzycka, M., Kołakowski, A., Stefanowicz, M., Matulewicz, N., Nikołajuk, A., & Karczewska-Kupczewska, M. (2022). Inverse Regulation of Serum Osteoprotegerin and B-Type Natriuretic Peptide Concentrations by Free Fatty Acids Elevation in Young Healthy Humans. Nutrients, 14(4), 837. https://doi.org/10.3390/nu14040837