
Reference Ranges of Glycemic Variability in Infants after Surgery—A Prospective Cohort Study

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
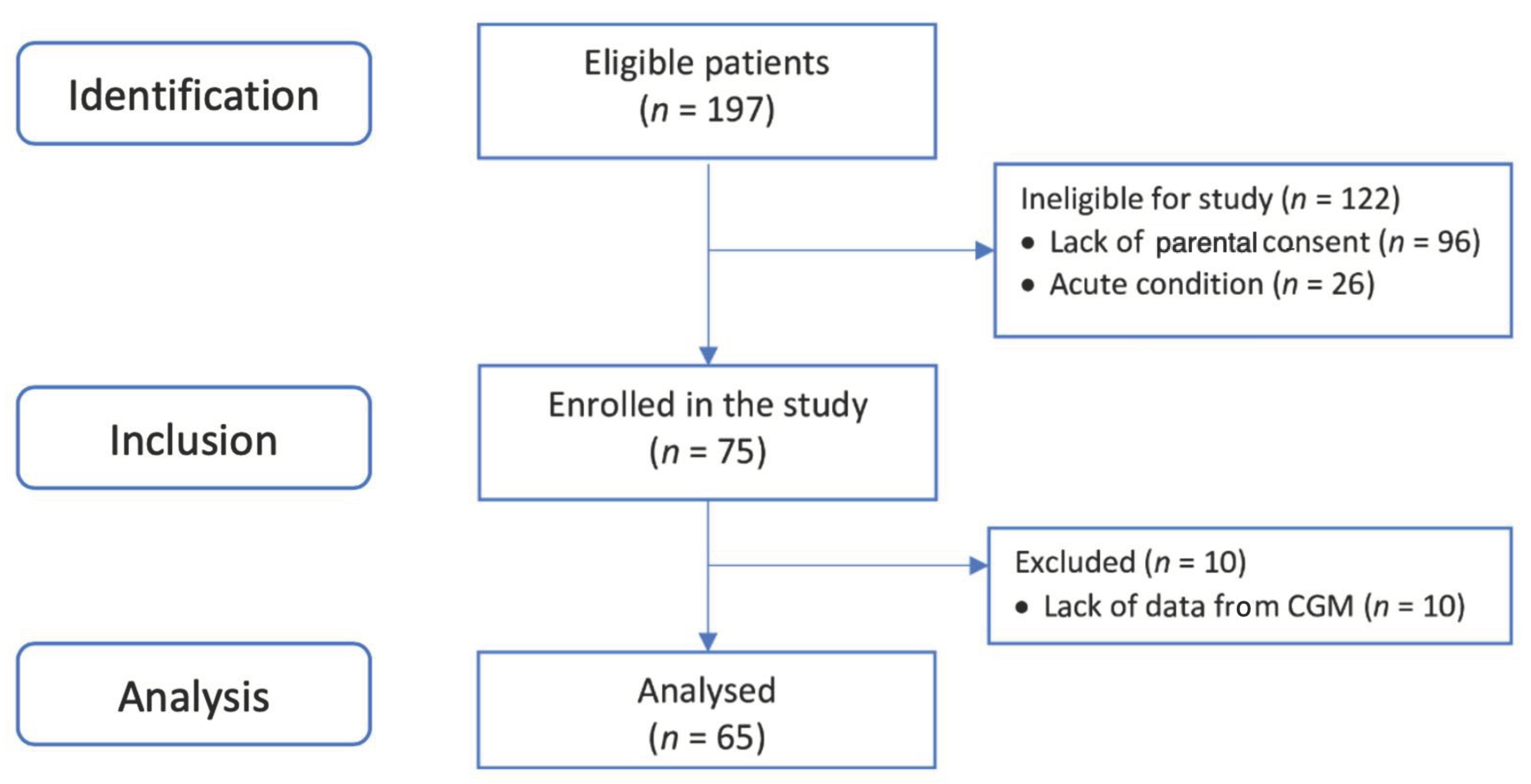
2.1. Participants
2.2. rt-CGM Metrics Analysis
2.3. Statistical Analysis
3. Results
3.1. Study Group Characteristics
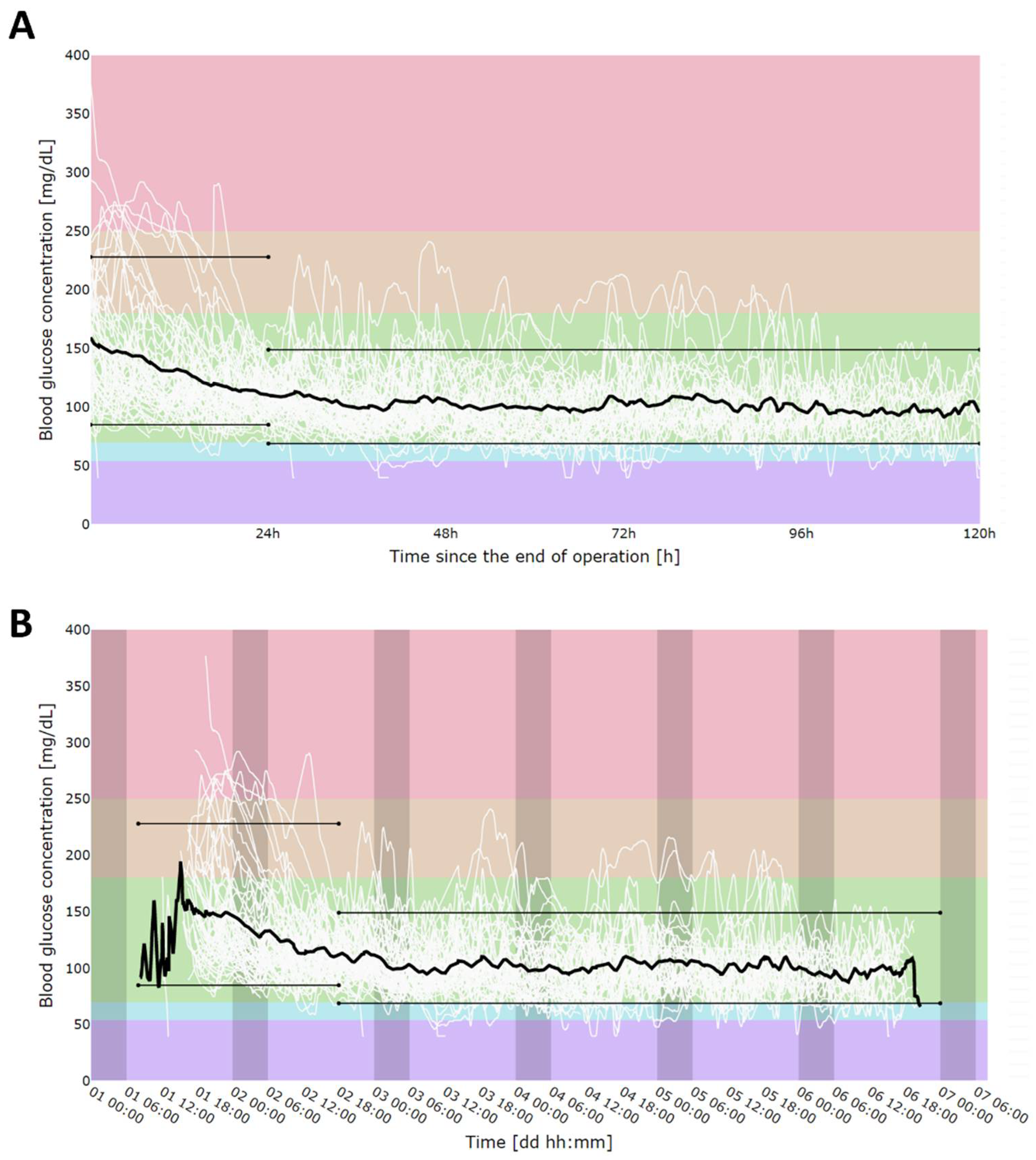
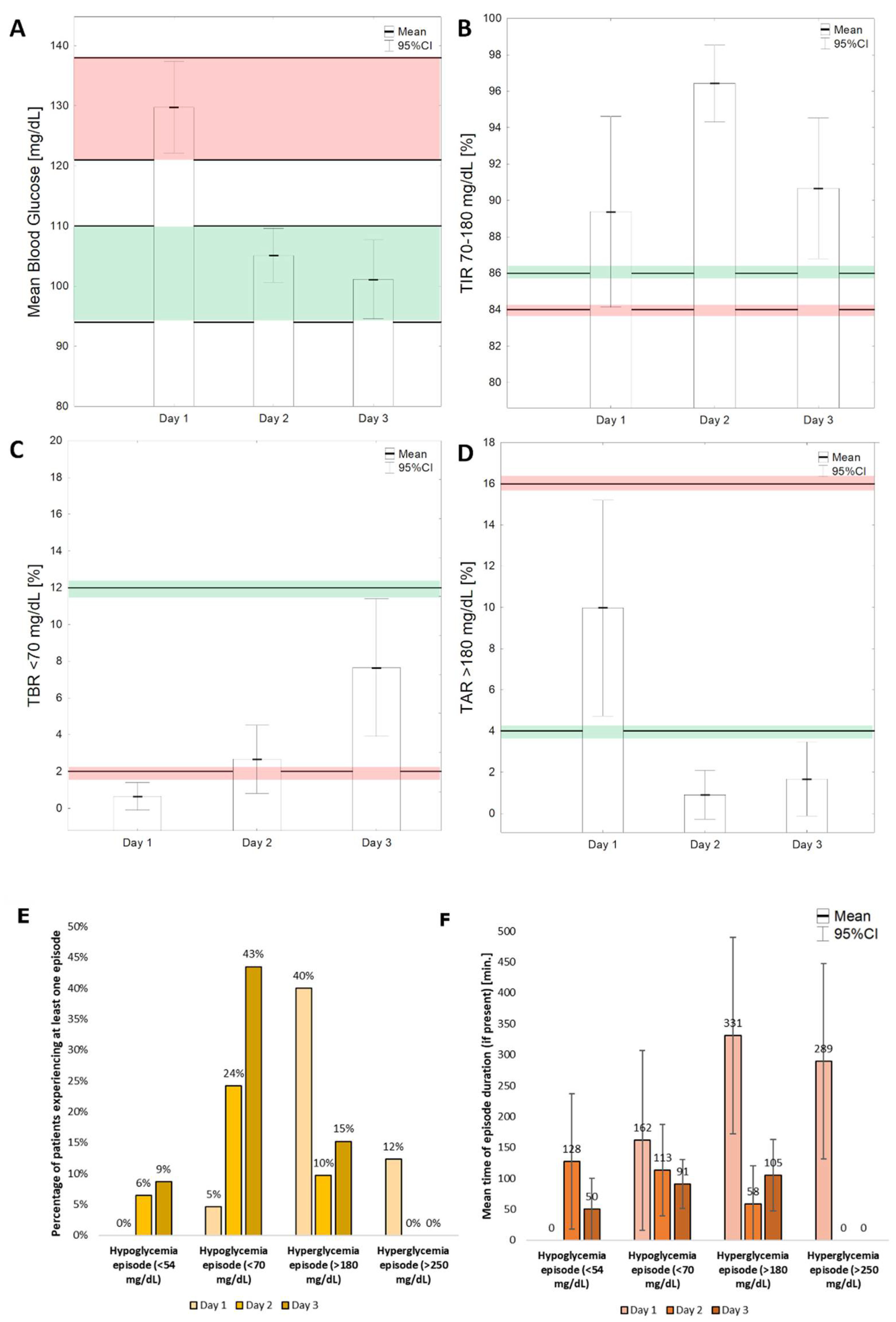
3.2. rt-CGM Metrics
3.3. Hypo- and Hyperglycemia Episodes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van den Berghe, G.; Wouters, P.; Weekers, F.; Verwaest, C.; Bruyninckx, F.; Schetz, M.; Vlasselaers, D.; Ferdinande, P.; Lauwers, P.; Bouillon, R. Intensive insulin therapy in critically ill patients. N. Engl. J. Med. 2001, 345, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Agus, M.S.; Steil, G.M.; Wypij, D.; Costello, J.M.; Laussen, P.C.; Langer, M.; Alexander, J.L.; Scoppettuolo, L.A.; Pigula, F.A.; Charpie, J.R.; et al. Tight Glycemic Control versus Standard Care after Pediatric Cardiac Surgery. N. Engl. J. Med. 2012, 367, 1208–1219. [Google Scholar] [CrossRef] [Green Version]
- Uettwiller, F.; Chemin, A.; Bonnemaison, E.; Favrais, G.; Saliba, E.; Labarthe, F. Real-Time Continuous Glucose Monitoring Reduces the Duration of Hypoglycemia Episodes: A Randomized Trial in Very Low Birth Weight Neonates. PLoS ONE 2015, 10, e0116255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranger, M.; Chau, C.M.; Garg, A.; Woodward, T.S.; Beg, M.F.; Bjornson, B.; Poskitt, K.; Fitzpatrick, K.; Synnes, A.R.; Miller, S.P.; et al. Neonatal Pain-Related Stress Predicts Cortical Thickness at Age 7 Years in Children Born Very Preterm. PLoS ONE 2013, 8, e76702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bochicchio, G.V.; Nasraway, S.A.; Moore, L.J.; Furnary, A.P.; Nohra, E.A.; Bochicchio, K.M.; Boyd, J.C.; Bruns, D.I.; Hirsch, I.B.; Preiser, J.C.; et al. Fifteen-minute Frequency of Glucose Measurements and the Use of Threshold Alarms: Impact on Mitigating Dysglycemia in Critically Ill Patients. J. Diabetes Sci. Technol. 2021, 15, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Krinsley, J.S.; Chase, J.G.; Gunst, J.; Martensson, J.; Schultz, M.J.; Taccone, F.S.; Wernerman, J.; Bohe, J.; De Block, C.; Desaive, T.; et al. Continuous glucose monitoring in the ICU: Clinical considerations and consensus. Crit. Care 2017, 21, 197. [Google Scholar] [CrossRef] [Green Version]
- Jacobi, J.; Bircher, N.; Krinsley, J.; Agus, M.; Braithwaite, S.S.; Deutschman, C.; Freire, A.X.; Geehan, D.; Kohl, B.; Nasraway, S.A.; et al. Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit. Care Med. 2012, 40, 3251–3276. [Google Scholar] [CrossRef] [PubMed]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations from the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyd, J.C.; Bruns, D.E. Effects of Measurement Frequency on Analytical Quality Required for Glucose Measurements in Intensive Care Units: Assessments by Simulation Models. Clin. Chem. 2014, 60, 644–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, R.; Harding, J.; Brown, J.; McKinlay, C. Neonatal Glycaemia and Neurodevelopmental Outcomes: A Systematic Review and Meta-Analysis. Neonatology 2019, 115, 116–126. [Google Scholar] [CrossRef]
- Singh, M.; Upreti, V.; Singh, Y.; Kannapur, A.; Nakra, M.; Kotwal, N. Effect of glycemic variability on mortality in ICU settings: A prospective observational study. Indian J. Endocrinol. Metab. 2018, 22, 632–635. [Google Scholar] [PubMed]
- Griesdale, D.E.; de Souza, R.J.; van Dam, R.M.; Heyland, D.K.; Cook, D.J.; Malhotra, A.; Dhaliwal, R.; Henderson, W.R.; Chittock, D.R.; Finfer, S.; et al. Intensive insulin therapy and mortality among critically ill patients: A meta-analysis including NICE-SUGAR study data. CMAJ 2009, 180, 821–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arabi, Y.M.; Casaer, M.P.; Chapman, M.; Heyland, D.K.; Ichai, C.; Marik, P.E.; Martindale, R.G.; McClave, S.A.; Preiser, J.C.; Reignier, J.; et al. The intensive care medicine research agenda in nutrition and metabolism. Intensive Care Med. 2017, 43, 1239–1256. [Google Scholar] [CrossRef] [PubMed]
- Duggan, E.W.; Carlson, K.; Umpierrez, G.E. Perioperative Hyperglycemia Management: An Update. Anesthesiology 2017, 126, 547–560. [Google Scholar] [CrossRef] [Green Version]
- Wallace, C.R. Postoperative management of hypoglycemia. Orthop. Nurs. 2012, 31, 328–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blood, D.W. Severe postoperative hypoglycemia. J. Am. Med. Assoc. 1946, 130, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Y.; Hu, S.F.; Ying, H.M.; Chen, L.; Li, H.L.; Tian, F.; Zhou, Z.F. Postoperative tight glycemic control significantly reduces postoperative infection rates in patients undergoing surgery: A meta-analysis. BMC Endocr. Disord. 2018, 18, 42. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clement, K.C.; Suarez-Pierre, A.; Sebestyen, K.; Alejo, D.; DiNatale, J.; Whitman, G.J.R.; Matthew, T.L.; Lawton, J.S. Increased Glucose Variability Is Associated with Major Adverse Events After Coronary Artery Bypass. Ann. Thorac. Surg. 2019, 108, 1307–1313. [Google Scholar] [CrossRef]
- Li, X.; Zhou, X.; Wei, J.; Mo, H.; Lou, H.; Gong, N.; Zhang, M. Effects of Glucose Variability on Short-Term Outcomes in Non-Diabetic Patients After Coronary Artery Bypass Grafting: A Retrospective Observational Study. Heart Lung. Circ. 2019, 28, 1580–1586. [Google Scholar] [CrossRef]
- Subramaniam, B.; Lerner, A.; Novack, V.; Khabbaz, K.; Paryente-Wiesmann, M.; Hess, P.; Talmor, D. Increased glycemic variability in patients with elevated preoperative HbA1C predicts adverse outcomes following coronary artery bypass grafting surgery. Anesth. Analg. 2014, 118, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Mistry, M.; Dobransky, J.; Malcolm, J.; Feibel, R.J. 147—The Influence of Post-Operative Blood Glucose Management on Reoperation for Infection Following Total Joint Arthroplasty. Can. J. Diabetes 2018, 42, S50. [Google Scholar] [CrossRef]
- Gunst, J.; Van den Berghe, G. Blood glucose control in the ICU: How tight? Ann. Transl. Med. 2017, 5, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, G.; Dodek, P. Intravenous insulin nomogram improves blood glucose control in the critically ill. Crit. Care Med. 2001, 29, 1714–1719. [Google Scholar] [CrossRef] [PubMed]
- Orlowski, J.P.; Cramer, C.L.; Fiallos, M.R. Diabetic ketoacidosis in the pediatric ICU. Pediatr. Clin. N. Am. 2008, 55, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.I.; Souter, M.J. Equipment-related electrocardiographic artifacts: Causes, characteristics, consequences, and correction. Anesthesiology 2008, 108, 138–148. [Google Scholar] [CrossRef] [Green Version]
- van Lieshout, E.J.; van der Veer, S.N.; Hensbroek, R.; Korevaar, J.C.; Vroom, M.B.; Schultz, M.J. Interference by new-generation mobile phones on critical care medical equipment. Crit. Care 2007, 11, R98. [Google Scholar] [CrossRef] [Green Version]
- Thomson, L.; Howlett, J.; Bond, S.; Hovorka, R.; Dunger, D.; Beardsall, K. Feasibility of Real Time Continuous Glucose Monitoring in Neonatal Intensive Care. In Proceedings of the Neonatal Society 2017 Spring Meeting, London, UK, 30 March 2017. [Google Scholar]
- Vincent, E.; Faustino, S.; Hirshberg, E.L.; Bogue, C.W. Hypoglycemia in critically ill children. J. Diabetes Sci. Technol. 2012, 6, 48–57. [Google Scholar]
- Cely, C.M.; Arora, P.; Quartin, A.A.; Kett, D.H.; Schein, R.M.H. Relationship of baseline glucose homeostasis to hyperglycemia during medical critical illness. Chest 2004, 126, 879–887. [Google Scholar] [CrossRef]
- Ouattara, A.; Lecomte, P.; Le Manach, Y.; Landi, M.; Jacqueminet, S.; Platonov, I.; Bonnet, N.; Riou, B.; Coriat, P. Poor intraoperative blood glucose control is associated with a worsened hospital outcome after cardiac surgery in diabetic patients. Anesthesiology 2005, 103, 687–694. [Google Scholar] [CrossRef]
- Johnston, L.E.; Kirby, J.L.; Downs, E.A.; LaPar, D.J.; Ghanta, R.K.; Ailawadi, G.; Kozower, B.D.; Kron, I.L.; McCall, A.L.; Isbell, J.M.; et al. Postoperative Hypoglycemia Is Associated With Worse Outcomes After Cardiac Operations. Ann. Thorac. Surg. 2017, 103, 526–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, A.E.; Abd-Elsayed, A.; Maheshwari, A.; Xu, M.; Soltesz, E.; Koch, C.G. Role of intraoperative and postoperative blood glucose concentrations in predicting outcomes after cardiac surgery. Anesthesiology 2010, 112, 860–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kauffman, R.E. Clinical trials in children: Problems and pitfalls. Paediatr. Drugs 2000, 2, 411–418. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Clinical Parameters | N (%) or Mean ± SD |
|---|---|
| N Total = 65 | |
| Gender, male | 33 (50.8%) |
| Cardioplegia type: | |
| Crystalloid | 46 (66.2%) |
| del Nido | 13 (20.0%) |
| None | 6 (9.2%) |
| Body mass, g | 5323.9 ± 1767.0 |
| Height, cm | 64.1 ± 8.6 |
| BSA, m2 | 0.30 ± 0.08 |
| Age, days | 128.6 ± 89.3 |
| APGAR | 8.9 ± 1.5 |
| Gestational age, weeks | 38.5 ± 1.7 |
| Birth weight, g | 3111.3 ± 563.3 |
| Glucose concentration before surgery, mg/dL | 84.8 ± 13.8 |
| Time of surgery, min. | 219.6 ± 76.1 |
| Time of aortic cleft, min. | 48.5 ± 23.8 |
| GV Indices | Day 1 | Day 2 | Day 3 | |||
|---|---|---|---|---|---|---|
| Mean | 95%CI | Mean | 95%CI | Mean | 95%CI | |
| MBG, mg/dL | 129.78 | 122.15–137.41 | 105.12 | 100.66–109.58 | 101.12 | 94.54–107.71 |
| Median, mg/dL | 129.13 | 120.88–137.38 | 103.89 | 99.32–108.45 | 99.98 | 93.48–106.48 |
| SD, mg/dL | 23.50 | 19.73–27.26 | 14.99 | 13.19–16.79 | 15.12 | 12.59–17.64 |
| CV | 17.36 | 15.19–19.54 | 14.14 | 12.67–15.62 | 14.70 | 12.57–16.82 |
| GMI | 6.41 | 6.23–6.60 | 5.82 | 5.72–5.93 | 5.73 | 5.57–5.89 |
| Conga 6 h | 23.88 | 20.70–27.06 | 19.49 | 16.53–22.44 | 19.58 | 15.72–23.43 |
| ADRR | 0.0028 | 0.0025–0.0032 | 0.0027 | 0.0023–0.0032 | 0.0032 | 0.0026–0.0038 |
| HBGI | 4.25 | 2.85–5.65 | 1.13 | 0.74–1.52 | 1.31 | 0.69–1.94 |
| LBGI | 0.5980 | 0.37–0.82 | 1.36 | 0.80–1.93 | 1.97 | 1.45–2.49 |
| J | 25.26 | 21.39–29.14 | 14.90 | 13.41–16.39 | 14.26 | 12.12–16.41 |
| GRADE | 4.26 | 3.29–5.23 | 1.87 | 1.44–2.31 | 2.08 | 1.53–2.62 |
| GRADEhyper | 27.14 | 20.00–34.28 | 8.22 | 4.41–12.02 | 7.99 | 2.80–13.19 |
| TIR70–180 (%) | 89.37 | 84.13–94.62 | 96.42 | 94.31–98.54 | 90.66 | 86.80–94.53 |
| TIR70–250 (%) | 96.44 | 94.16–98.71 | 97.33 | 95.49–99.17 | 92.34 | 88.61–96.08 |
| TAR > 180 (%) | 9.97 | 4.73–15.21 | 0.90 | −0.27–2.08 | 1.68 | −0.12–3.47 |
| TAR > 250 (%) | 2.91 | 0.71–5.11 | 0.00 | NA | 0.00 | NA |
| TBR < 54 (%) | 0.00 | NA | 0.62 | −0.03–1.27 | 0.34 | −0.02–0.70 |
| TBR < 70 (%) | 0.66 | −0.09–1.40 | 2.67 | 0.83–4.51 | 7.66 | 3.92–11.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaminska, H.; Wieczorek, P.; Zalewski, G.; Malachowska, B.; Kucharski, P.; Fendler, W.; Szarpak, L.; Jarosz-Chobot, P. Reference Ranges of Glycemic Variability in Infants after Surgery—A Prospective Cohort Study. Nutrients 2022, 14, 740. https://doi.org/10.3390/nu14040740
Kaminska H, Wieczorek P, Zalewski G, Malachowska B, Kucharski P, Fendler W, Szarpak L, Jarosz-Chobot P. Reference Ranges of Glycemic Variability in Infants after Surgery—A Prospective Cohort Study. Nutrients. 2022; 14(4):740. https://doi.org/10.3390/nu14040740
Chicago/Turabian StyleKaminska, Halla, Pawel Wieczorek, Grzegorz Zalewski, Beata Malachowska, Przemyslaw Kucharski, Wojciech Fendler, Lukasz Szarpak, and Przemyslawa Jarosz-Chobot. 2022. "Reference Ranges of Glycemic Variability in Infants after Surgery—A Prospective Cohort Study" Nutrients 14, no. 4: 740. https://doi.org/10.3390/nu14040740
APA StyleKaminska, H., Wieczorek, P., Zalewski, G., Malachowska, B., Kucharski, P., Fendler, W., Szarpak, L., & Jarosz-Chobot, P. (2022). Reference Ranges of Glycemic Variability in Infants after Surgery—A Prospective Cohort Study. Nutrients, 14(4), 740. https://doi.org/10.3390/nu14040740