
Muscle Strength Moderates the Relationship between Nutritional Health Risk and Depression in Korean Older Adults


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
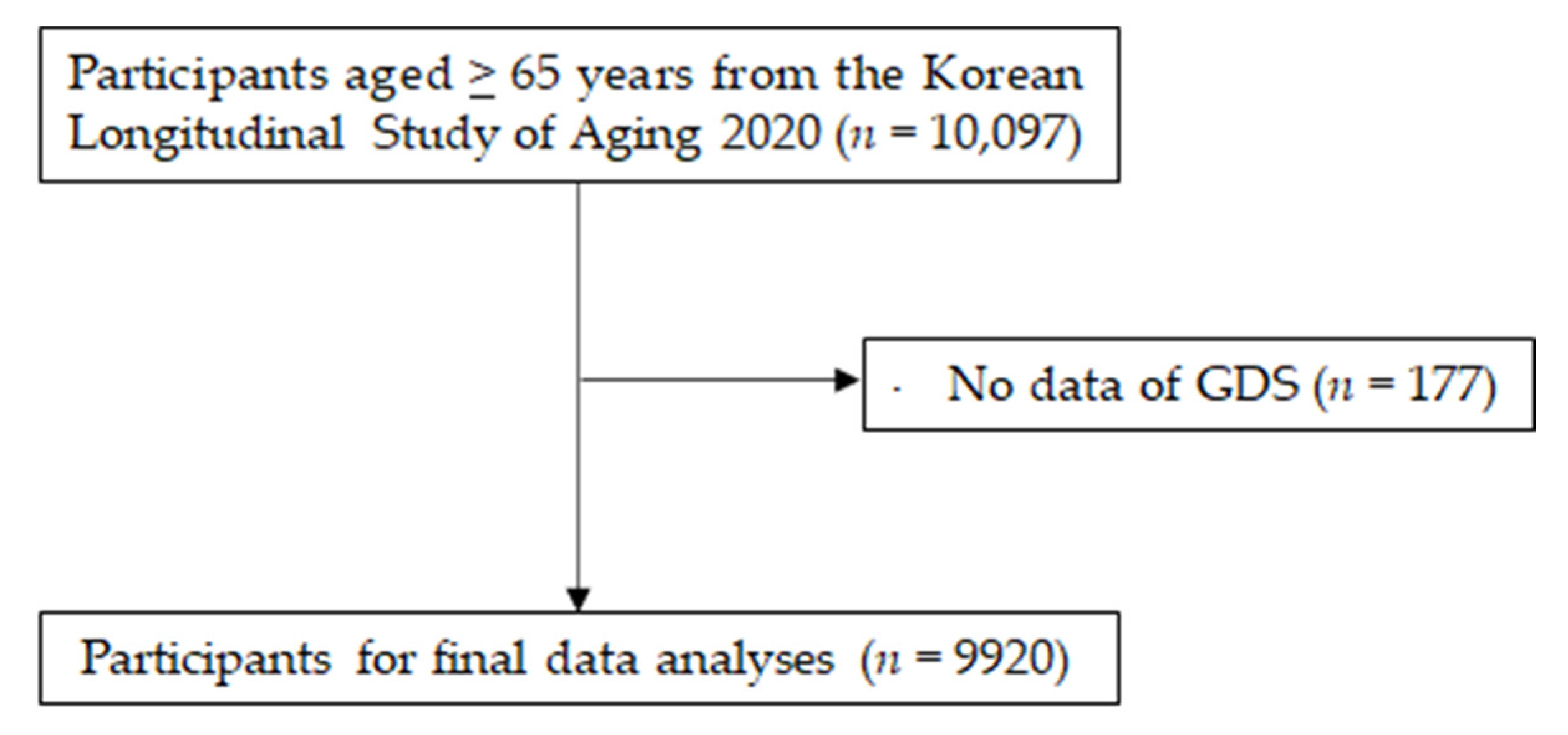
2.1. Data Source and Study Participants
2.2. Variables
2.2.1. Depression
2.2.2. Nutritional Health Risk
2.2.3. Lower Extremity Muscle Strength
2.2.4. Covariates
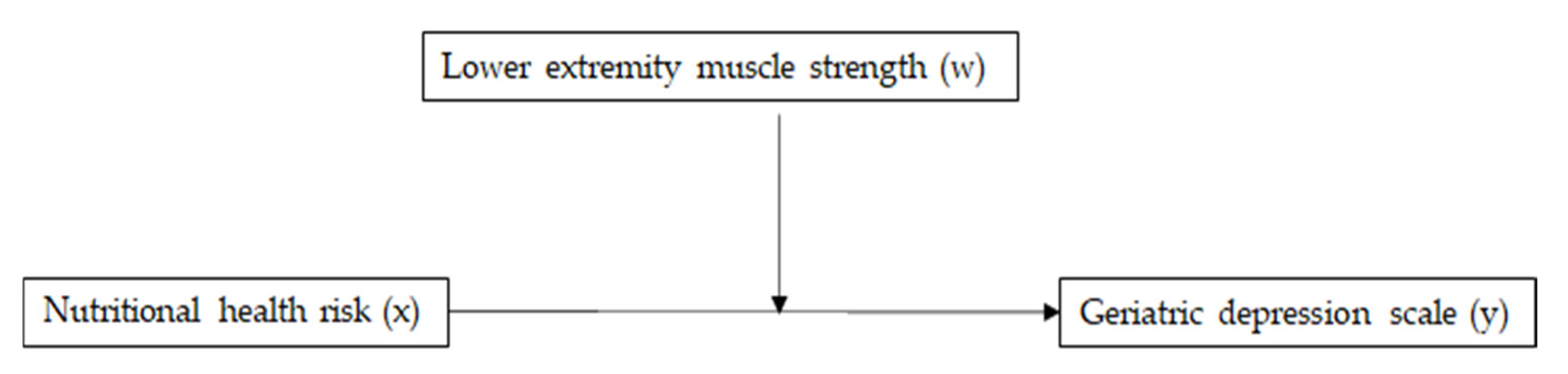
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Song, J.; Koh, T.H.; Park, O.; Kwon, D.; Kang, S.; Kwak, K.; Park, J.T. Association between depression and cardiovascular disease risk in general population of Korea: Results from the Korea national health and nutrition examination survey, 2016. Ann. Occup. Environ. Med. 2019, 31, e10. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Jeong, W.; Kwon, J.; Kim, Y.; Park, E.-C.; Jang, S.-I. Association between depression and the risk of Alzheimer’s disease using the Korean national health insurance service-elderly cohort. Sci. Rep. 2021, 11, 22591. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.J.; Kihl, T. Suicidal ideation associated with depression and social support: A survey-based analysis of older adults in South Korea. BMC Psychiatry 2021, 21, 409. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, S.H.; Cho, Y.J. Combined effects of depression and chronic disease on the risk of mortality: The Korean longitudinal study of aging (2006–2016). J. Korean Med. Sci. 2021, 36, e99. [Google Scholar] [CrossRef]
- Shin, D.; Kim, N.W.; Kim, M.J.; Rhee, S.J.; Park, C.H.K.; Kim, H.; Yang, B.R.; Kim, M.S.; Choi, G.J.; Koh, M.; et al. Cost analysis of depression using the national insurance system in South Korea: A comparison of depression and treatment-resistant depression. BMC Health Serv. Res. 2020, 20, 286. [Google Scholar] [CrossRef] [Green Version]
- He, Q.; Yang, L.; Shi, S.; Gao, J.; Tao, M.; Zhang, K.; Gao, C.; Yang, L.; Li, K.; Shi, J.; et al. Smoking and major depressive disorder in Chinese women. PLoS ONE 2014, 9, e106287. [Google Scholar] [CrossRef]
- Choi, N.G.; Dinitto, D.M. Heavy/binge drinking and depressive symptoms in older adults: Gender differences. Int. J. Geriatr. Psychiatry 2011, 26, 860–868. [Google Scholar] [CrossRef]
- Meng, X.; D’Arcy, C. The projected effect of increasing physical activity on reducing the prevalence of common mental disorders among Canadian men and women: A national population-based community study. Prev. Med. 2013, 56, 59–63. [Google Scholar] [CrossRef]
- Jin, Y.; Kang, S.; Kang, H. Individual and synergistic relationships of low muscle mass and low muscle function with depressive symptoms in Korean older adults. Int. J. Environ. Res. Public Health 2021, 18, 10129. [Google Scholar] [CrossRef]
- Marques, A.; Henriques-Neto, D.; Peralta, M.; Marconcin, P.; Gouveia, É.R.; Ferrari, G.; Martins, J.; Ihle, A. Exploring grip strength as a predictor of depression in middle-aged and older adults. Sci. Rep. 2021, 11, 15946. [Google Scholar] [CrossRef]
- Aarden, J.J.; van der Schaaf, M.; van der Esch, M.; Reichardt, L.A.; van Seben, R.; Bosch, J.A.; Twisk, J.W.R.; Buurman, B.M.; Engelbert, R.H.H.; Hospital-ADL Study Group. Muscle strength is longitudinally associated with mobility among older adults after acute hospitalization: The Hospital-ADL study. PLoS ONE 2019, 14, e0219041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, H.H.; Fang, I.Y.; Yu, Y.C.; Huang, Y.P.; Kuo, I.L.; Wang, L.T.; Tsai, M.C.; Chang, S.H.; Hsueh, M.C. Is functional fitness performance a useful predictor of risk of falls among community-dwelling older adults? Arch. Public Health 2021, 79, 108. [Google Scholar] [CrossRef] [PubMed]
- Bae, E.J.; Park, N.J.; Sohn, H.S.; Kim, Y.H. Handgrip strength and all-cause mortality in middle-aged and older Koreans. Int. J. Environ. Res. Public Health 2019, 16, 740. [Google Scholar] [CrossRef] [Green Version]
- Noh, H.M.; Park, Y.S. Handgrip strength, dynapenia, and mental health in older Koreans. Sci. Rep. 2020, 10, 4004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, K.M.; Lung, Y.; Lin, S.L.; Tong, H.; Kobayashi, K.M.; Fuller-Thomson, E. Depression in middle and older adulthood: The role of immigration, nutrition, and other determinants of health in the Canadian longitudinal study on aging. BMC Psychiatry 2019, 19, 329. [Google Scholar] [CrossRef] [Green Version]
- Taylor, K.L.; Simpson, S., Jr.; Jelinek, G.A.; Neate, S.L.; De Livera, A.M.; Brown, C.R.; O’Kearney, E.; Marck, C.H.; Weiland, T.J. Longitudinal associations of modifiable lifestyle factors with positive depression-screen over 2.5-years in an international cohort of people living with multiple sclerosis. Front. Psychiatry 2018, 9, 526. [Google Scholar] [CrossRef]
- Khosravi, M.; Sotoudeh, G.; Majdzadeh, R.; Nejati, S.; Darabi, S.; Raisi, F.; Esmaillzadeh, A.; Sorayani, M. Healthy and unhealthy dietary patterns are related to depression: A case-control study. Psychiatry Investig. 2015, 12, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.J.; Kim, J.M. Associations between depression and eating behavior factors in Korean adults: The Korea national health and nutrition examination survey 2018. J. Nutr. Health 2021, 54, 152–164. [Google Scholar] [CrossRef]
- Song, E.G.; Yoon, Y.S.; Yang, Y.J.; Lee, E.S.; Lee, J.H.; Lee, J.Y.; Park, W.J.; Park, S.Y. Factors associated with eating alone in Korean adults: Findings from the sixth Korea national health and nutrition examination, 2014. Korean J. Fam. Pract. 2017, 7, 698–706. [Google Scholar] [CrossRef]
- Park, S.; Cho, J.; Kim, D.; Jin, Y.; Lee, I.; Hong, H.; Kang, H. Handgrip strength, depression, and all-cause mortality in Korean older adults. BMC Geriatr. 2019, 19, 127. [Google Scholar] [CrossRef]
- Park, J.H.; Kim, K.W. A review of the epidemiology of depression in Korea. J. Korean Med. Assoc. 2011, 554, 362–369. [Google Scholar] [CrossRef] [Green Version]
- Cavazzana, A.; Röhrborn, A.; Garthus-Niegel, S.; Larsson, M.; Hummel, T.; Croy, I. Sensory-specific impairment among older people. An investigation using both sensory thresholds and subjective measures across the five senses. PLoS ONE 2018, 13, e0202969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leslie, W.; Hankey, C. Aging, nutritional status and health. Healthcare 2015, 3, 648–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, D.J.; Piasecki, M.; Atherton, P.J. The age-related loss of skeletal muscle mass and function: Measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res. Rev. 2018, 47, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Štefan, L.; Petrinović, L.; Sporiš, G.; Vrgoč, G. Frequency of dietary intake and physical activity in older adults: A cross-sectional study. Nutrients 2018, 10, 1960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro-Mejía, J.L.; Khakimov, B.; Krych, Ł.; Bülow, J.; Bechshøft, R.L.; Højfeldt, G.; Mertz, K.H.; Garne, E.S.; Schacht, S.R.; Ahmad, H.F.; et al. Physical fitness in community-dwelling older adults is linked to dietary intake, gut microbiota, and metabolomic signatures. Aging Cell 2020, 19, e13105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, J.N.; Cho, M.J. Development of the Korean version of the geriatric depression scale and its short form among elderly psychiatric patients. J. Psychosom. Res. 2004, 57, 297–305. [Google Scholar] [CrossRef]
- Lee, S.C.; Kim, W.H.; Chang, S.M.; Kim, B.S.; Lee, D.W.; Bae, J.N.; Cho, M.J. The use of the Korean version of short form geriatric depression scale (SGDS-K) in the community dwelling elderly in Korea. J. Korean Geriatr. Psychiatry 2013, 17, 37–43. [Google Scholar]
- Nutrition Screening Initiative. Report of Nutrition Screening 1: Toward a Common View: Executive Summary; A Consensus Conference; Nutrition Screening Initiative: Washington, DC, USA, 1991. [Google Scholar]
- Posner, B.M.; Jette, A.M.; Smith, K.W.; Miller, D.R. Nutrition and health risks in the elderly: The nutritional screening initiative. Am. J. Public Health 1993, 83, 972–978. [Google Scholar] [CrossRef] [Green Version]
- Buatois, S.; Miljkovic, D.; Manckoundia, P.; Gueguen, R.; Miget, P.; Vancon, G.; Perrin, P.; Benetos, A. Five times sit to stand test is a predictor of recurrent falls in healthy community-living subjects aged 65 and older. J. Am. Geriatr. Soc. 2008, 56, 1575–1577. [Google Scholar] [CrossRef]
- Delibaş, D.H.; Eşkut, N.; İlhan, B.; Erdoğan, E.; Top Kartı, D.; Yılmaz Küsbeci, Ö..; Bahat, G. Clarifying the relationship between sarcopenia and depression in geriatric outpatients. Aging Male 2021, 24, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.R.; Karmokar, S.; Reza, S.; Kabir, M.R.; Ghosh, S.; Mamun, M.A.A. Geriatric malnutrition and depression: Evidence from elderly home care population in Bangladesh. Prev. Med. Rep. 2021, 23, 101478. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Fan, L.; Zhang, Y.; Li, S.; Partridge, J.; Claytor, L.; Sulo, S. Association between malnutrition and depression among community-dwelling older Chinese adults. Asia Pac. J. Public Health 2018, 30, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Zhao, A.; Lan, H.; Ren, Z.; Zhang, J.; Szeto, I.M.; Wang, P.; Zhang, Y. Association between dietary quality and postpartum depression in lactating women: A cross-sectional survey in urban China. Front. Nutr. 2021, 8, 705353. [Google Scholar] [CrossRef]
- Shin, S.; Hwang, E. Factors influencing depressive symptoms among Korean older adults with chronic illnesses: Using the 2014 national survey on older adults. Korean J. Adult Nurs. 2018, 30, 577–585. [Google Scholar] [CrossRef]
- Kim, G.E.; Jo, M.W.; Shin, Y.W. Increased prevalence of depression in South Korea from 2002 to 2013. Sci. Rep. 2020, 10, 16979. [Google Scholar] [CrossRef]
- Lang, U.E.; Beglinger, C.; Schweinfurth, N.; Walter, M.; Borgwardt, S. Nutritional aspects of depression. Cell Physiol. Biochem. 2015, 37, 1029–1043. [Google Scholar] [CrossRef]
- Li, Y.; Lv, M.R.; Wei, Y.J.; Sun, L.; Zhang, J.X.; Zhang, H.G.; Li, B. Dietary patterns and depression risk: A meta-analysis. Psychiatry Res. 2017, 253, 373–382. [Google Scholar] [CrossRef]
- Lee, M.R.; Jung, S.M.; Bang, H.; Kim, H.S.; Kim, Y.B. The association between muscular strength and depression in Korean adults: A cross-sectional analysis of the sixth Korea national health and nutrition examination survey (KNHANES VI) 2014. BMC Public Health 2018, 18, 1123. [Google Scholar] [CrossRef] [Green Version]
- Hurh, K.; Park, Y.; Kim, G.R.; Jang, S.I.; Park, E.C. Associations of handgrip strength and handgrip strength asymmetry with depression in the elderly in Korea: A cross-sectional study. J. Prev. Med. Public Health 2021, 54, 63–72. [Google Scholar] [CrossRef]
- Ganasarajah, S.; Sundström Poromaa, I.; Thu, W.P.; Kramer, M.S.; Logan, S.; Cauley, J.A.; Yong, E.L. Objective measures of physical performance associated with depression and/or anxiety in midlife Singaporean women. Menopause 2019, 26, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Zasadzka, E.; Pieczyńska, A.; Trzmiel, T.; Kleka, P.; Pawlaczyk, M. Correlation between handgrip strength and depression in older adults—A systematic review and a meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 4823. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, H.A.; Cerceau, V.R.; Pereira, L.C.; Funghetto, S.S.; de Menezes, R.L. Nutritional intervention and functional exercises improve depression, loneliness and quality of life in elderly women with sarcopenia: A randomized clinical trial. Fisioter. Mov. 2020, 33, e003332. [Google Scholar] [CrossRef]
- Kaburagi, T.; Hirasawa, R.; Yoshino, H.; Odaka, Y.; Satomi, M.; Nakano, M.; Fujimoto, E.; Kabasawa, K.; Sato, K. Nutritional status is strongly correlated with grip strength and depression in community-living elderly Japanese. Public Health Nutr. 2011, 14, 1893–1899. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Liu, M.; Jia, W.P.; Han, K.; Wang, S.S.; He, Y. The association between nutritional status and functional limitations among centenarians: A cross-sectional study. BMC Geriatr. 2021, 21, 376. [Google Scholar] [CrossRef]
- Pigłowska, M.; Guligowska, A.; Kostka, T. Nutritional status plays more important role in determining functional state in older people living in the community than in nursing home residents. Nutrients 2020, 12, 2042. [Google Scholar] [CrossRef]
- Sieber, C.C. Malnutrition and sarcopenia. Aging Clin. Exp. Res. 2019, 31, 793–798. [Google Scholar] [CrossRef]
- Marques, A.; Gomez-Baya, D.; Peralta, M.; Frasquilho, D.; Santos, T.; Martins, J.; Ferrari, G.; Gaspar de Matos, M. The effect of muscular strength on depression symptoms in adults: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 5674. [Google Scholar] [CrossRef]
- Kim, S.; Choe, K.; Lee, K. Depression, loneliness, social support, activities of daily living, and life satisfaction in older adults at high-risk of dementia. Int. J. Environ. Res. Public Health 2020, 17, 9448. [Google Scholar] [CrossRef]
- Dos Santos, L.; Cyrino, E.S.; Antunes, M.; Santos, D.A.; Sardinha, L.B. Sarcopenia and physical independence in older adults: The independent and synergic role of muscle mass and muscle function. J. Cachexia Sarcopenia Muscle 2017, 8, 245–250. [Google Scholar] [CrossRef]
- Santoft, F.; Hedman-Lagerlöf, E.; Salomonsson, S.; Lindsäter, E.; Ljótsson, B.; Kecklund, G.; Lekander, M.; Andreasson, A. Inflammatory cytokines in patients with common mental disorders treated with cognitive behavior therapy. Brain Behav. Immun. Health 2020, 3, 100045. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Choi, J.Y.; Moon, S.; Park, D.H.; Kwak, H.B.; Kang, J.H. Roles of myokines in exercise-induced improvement of neuropsychiatric function. Pflugers Arch. Eur. J. Physiol. 2019, 471, 491–505. [Google Scholar] [CrossRef] [PubMed]
- Sgro, P.; Sansone, M.; Sansone, A.; Sabatini, S.; Borrione, P.; Romanelli, F.; Di Luigi, L. Physical exercise, nutrition, and hormones: Three pillars to fight sarcopenia. Aging Male 2019, 22, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kim, K.W.; Kim, M.H.; Kim, M.D.; Kim, B.J.; Kim, S.K.; Kim, J.L.; Moon, S.W.; Bae, J.N.; Woo, J.I.; et al. A nationwide survey on the prevalence and risk factors of late life depression in South Korea. J. Affect. Disord. 2012, 138, 34–40. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | Not Depressed (n = 9042) | Depressed (n = 878) | Effect Size | p Value | |
|---|---|---|---|---|---|
| Age (years) | −0.217 | <0.001 | |||
| 60–69 | 3246 (35.9) | 265 (30.2) | |||
| 70–74 | 2276 (25.2) | 190 (21.6) | |||
| 75–79 | 1765 (19.5) | 191 (21.8) | |||
| ≥80 | 1755 (19.4) | 232 (26.4) | |||
| Gender, n (%) | 0.025 | 0.013 | |||
| Male | 3654 (92.0) | 317 (8.0) | |||
| Female | 5388 (90.6) | 561 (9.4) | |||
| Body mass index (kg/m2) | 23.6 ± 2.6 | 23.1 ± 2.7 | 0.182 | <0.001 | |
| Education, n (%) | 0.058 | <0.001 | |||
| Elementary or less | 3968 (43.9) | 463 (52.7) | |||
| Middle/high | 4590 (50.8) | 394 (44.9) | |||
| College or higher | 484 (5.4) | 21 (2.4) | |||
| Smoking, n (%) | 0.014 | 0.154 | |||
| Nonsmokers | 8062 (89.2) | 769 (87.6) | |||
| Current/past smokers | 980 (10.8) | 109 (12.4) | |||
| Alcohol intake (times/week) | 0.004 | 0.004 | |||
| 0 | 5735 (63.4) | 508 (57.9) | |||
| 1–6 | 3207 (35.5) | 361 (41.0) | |||
| ≥7 | 100 (1.1) | 9 (1.0) | |||
| Regular exercise, n (%) | 0.053 | <0.001 | |||
| Yes | 4802 (53.1) | 385 (43.8) | |||
| No | 4240 (46.9) | 493 (43.8) | |||
| Multicomorbidity, n (%) | 0.072 | <0.001 | |||
| None | 1598 (17.7) | 80 (9.1) | |||
| Single | 2678 (29.6) | 244 (27.8) | |||
| Multiple | 4766 (52.7) | 554 (63.1) | |||
| Nutritional health, n (%) | 0.296 | <0.001 | |||
| Good | 6688 (74.0) | 370 (42.1) | |||
| Moderate risk | 1753 (19.4) | 190 (21.6) | |||
| High risk | 601 (6.6) | 318 (36.2) | |||
| Lower body muscle strength, n (%) | 0.174 | <0.001 | |||
| Strong | 7588 (84.1) | 530 (60.5) | |||
| Weak | 1437 (15.9) | 346 (39.5) | |||
| Variables | β | 95% CI | r2 part | p Value | VIF |
|---|---|---|---|---|---|
| Age | −0.010 | −0.018~−0.002 | 0.005 | <0.001 | 1.475 |
| Gender | −0.003 | −0.102~0.097 | −0.004 | 0.510 | 1.385 |
| Body mass index | −0.032 | −0.048~−0.016 | −0.041 | <0.001 | 1.024 |
| Education | 0.143 | 0.059~0.227 | 0.001 | <0.001 | 1.409 |
| Smoking | 0.043 | −0.101~0.309 | −0.013 | 0.152 | 1.183 |
| Alcohol intake | 0.217 | −0.126~0.089 | 0.051 | 0.471 | 1.263 |
| Regular exercise | 0.004 | −0.081~0.220 | 0.002 | 0.271 | 1.054 |
| Multicomorbidity | 0.171 | 0.290~0.112 | 0.012 | <0.001 | 1.125 |
| Nutritional health risk | 0.275 | 0.336~0.290 | 0.354 | <0.001 | 1.103 |
| Lower extremity muscle strength | −0.340 | −0.456~−0.224 | −0.117 | <0.001 | 1.157 |
| Predictors | Model 1 | Model 2 | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Nutritional health risk | ||||
| Good | 1 (reference) | 1 (reference) | ||
| Moderate risk | 1.772 (1.472~2.133) | <0.001 | 1.679 (1.385~2.035) | <0.001 |
| High risk | 7.703 (6.450~9.199) | <0.001 | 7.571 (6.285~9.119) | <0.001 |
| Lower extremity muscle strength | ||||
| Strong | 1 (reference) | 1 (reference) | ||
| Weak | 2.412 (2.060~2.824) | <0.001 | 2.094 (1.770~2.476) | <0.001 |
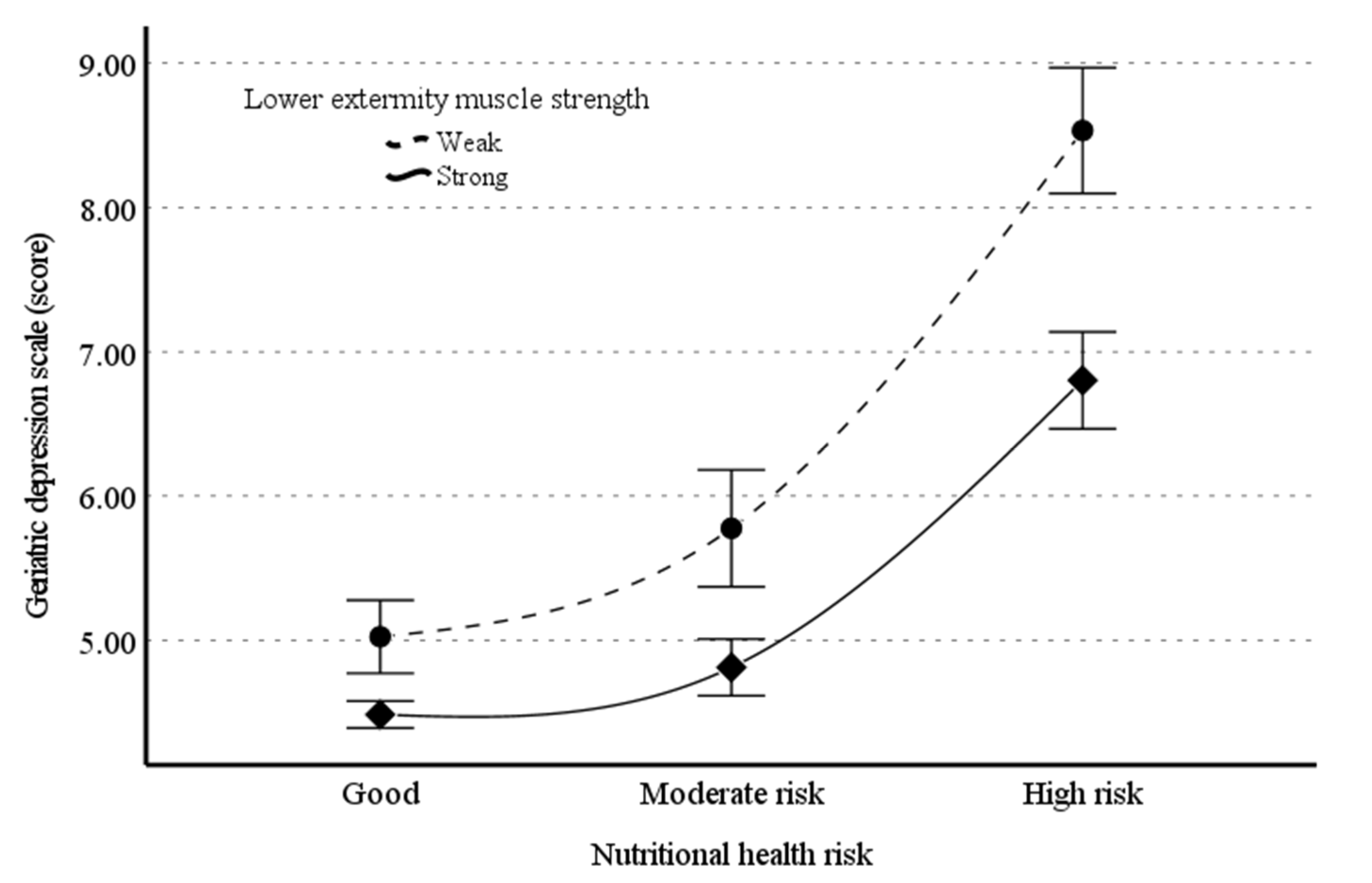
| Predictors | Coefficients | SE | t | p | 95% CI | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Model 1 (R2 = 0.133, F = 506.561, p < 0.001) | ||||||
| Nutritional health | 0.472 | 0.026 | 18.064 | <0.001 | 3.736 | 4.256 |
| Lower body strength | 0.110 | 0.071 | 1.562 | 0.118 | −0.028 | 0.249 |
| Interaction | −0.127 | 0.015 | −8.342 | <0.001 | −0.157 | −0.097 |
| R2 change due to the moderator = 0.006 (F = 69.59, p < 0.001) | ||||||
| Model 2 (R2 = 0.162, F = 71.006, p < 0.001) | ||||||
| Nutritional health | 0.494 | 0.046 | 10.680 | <0.001 | 0.403 | 0.584 |
| Lower body strength | −0.356 | 0.133 | −2.673 | 0.008 | −0.617 | −0.095 |
| Interaction | −0.120 | 0.027 | −4.451 | <0.001 | −0.173 | −0.067 |
| R2 change due to the moderator = 0.005 (F = 19.809, p < 0.001) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Kang, S.; Hong, H.; Kang, H.; Kim, J.-H.; Woo, S.-K. Muscle Strength Moderates the Relationship between Nutritional Health Risk and Depression in Korean Older Adults. Nutrients 2022, 14, 665. https://doi.org/10.3390/nu14030665
Kim J, Kang S, Hong H, Kang H, Kim J-H, Woo S-K. Muscle Strength Moderates the Relationship between Nutritional Health Risk and Depression in Korean Older Adults. Nutrients. 2022; 14(3):665. https://doi.org/10.3390/nu14030665
Chicago/Turabian StyleKim, Jeonghyeon, Seamon Kang, Haeryun Hong, Hyunsik Kang, Ju-Hyoung Kim, and Sang-Koo Woo. 2022. "Muscle Strength Moderates the Relationship between Nutritional Health Risk and Depression in Korean Older Adults" Nutrients 14, no. 3: 665. https://doi.org/10.3390/nu14030665
APA StyleKim, J., Kang, S., Hong, H., Kang, H., Kim, J.-H., & Woo, S.-K. (2022). Muscle Strength Moderates the Relationship between Nutritional Health Risk and Depression in Korean Older Adults. Nutrients, 14(3), 665. https://doi.org/10.3390/nu14030665