
Clinical Manifestation and Diagnostic Process of Celiac Disease in Poland—Comparison of Pediatric and Adult Patients in Retrospective Study

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
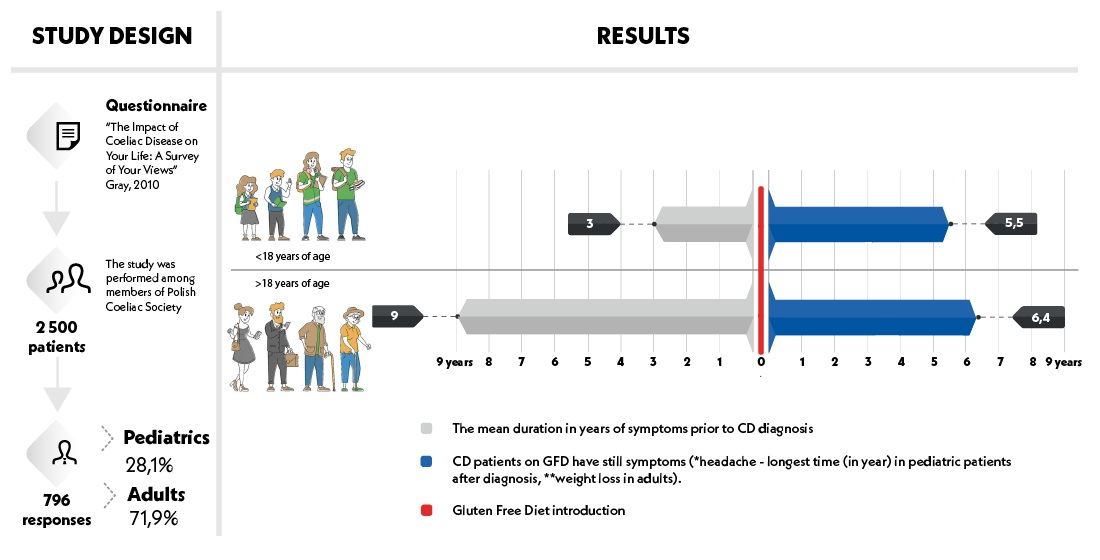
2.1. Study Design
2.2. Questionnaires
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Paediatric and Adult Patients
3.2. Clinical Symptoms
3.3. Duration of Symptoms before CD Diagnosis
3.4. The Effect of GFD on CD Symptoms
3.5. Comorbidity
3.6. Diagnostic Process
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, J.C.; Fried, M.; Corazza, G.R.; Schuppan, D.; Farthing, M.; Catassi, C.; Greco, L.; Cohen, H.; Ciacci, C.; Eliakim, R.; et al. World Gastroenterology Organisation Global Guidelines on Celiac Disease. J. Clin. Gastroenterol. 2013, 47, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelkowski, T.D.; Viera, A.J. Celiac disease: Diagnosis and management. Am. Fam. Physician 2014, 89, 99–105. [Google Scholar] [PubMed]
- Fuchs, V.; Kurppa, K.; Huhtala, H.; Mäki, M.; Kekkonen, L.; Kaukinen, K. Delayed celiac disease diagnosis predisposes to reduced quality of life and incremental use of health care services and medicines: A prospective nationwide study. United Eur. Gastroenterol. J. 2018, 6, 567–575. [Google Scholar] [CrossRef]
- Parzanese, I.; Qehajaj, D.; Patrinicola, F.; Aralica, M.; Chiriva-Internati, M.; Stifter, S.; Elli, L.; Grizzi, F. Celiac disease: From pathophysiology to treatment. World J. Gastrointest. Pathophysiol. 2017, 8, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Mooney, P.D.; Evans, K.E.; Singh, S.; Sanders, D.S. Treatment failure in coeliac disease: A practical guide to investigation and treatment of non-responsive and refractory coeliac disease. J. Gastrointest. Liver Dis. 2012, 21, 197–203. [Google Scholar]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; de Giorgio, R.; Catassi, C.; Fasano, A. Celiac disease: A comprehensive current review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majsiak, E.; Choina, M.; Cukrowska, B. The knowledge of medical professions on celiac disease in opinion of Polish patients with celiac disease. In Proceedings of the Abstract#: ICDS00123 Final Poster ID: P2-15 on International Coeliac Disease Symposium (ICDS), Paris, France, 5–7 September 2019. [Google Scholar]
- Majsiak, E.; Choina, M.; Golicki, D.; Gray, A.M.; Cukrowska, B. The impact of symptoms on quality of life before and after diagnosis of coeliac disease: The results from a Polish population survey and comparison with the results from the United Kingdom. BMC Gastroenterol. 2021, 21, 99. [Google Scholar] [CrossRef]
- Gray, A.M.; Papanicolas, I.N. Impact of symptoms on quality of life before and after diagnosis of coeliac disease: Results from a UK population survey. BMC Health Serv. Res. 2010, 10, 105. [Google Scholar] [CrossRef] [Green Version]
- Vavricka, S.R.; Vadasz, N.; Stotz, M.; Lehmann, R.; Studerus, D.; Greuter, T.; Frei, P.; Zeitz, J.; Scharl, M.; Misselwitz, B.; et al. Celiac disease diagnosis still significantly delayed—Doctor’s but not patients’ delay responsive for the increased total delay in women. Dig. Liver Dis. 2016, 48, 1148–1154. [Google Scholar] [CrossRef]
- Trovato, C.M.; Raucci, U.; Valitutti, F.; Montuori, M.; Villa, M.P.; Cucchiara, S.; Parisi, P. Neuropsychiatric manifestations in celiac disease. Epilepsy Behav. 2019, 99, 106393. [Google Scholar] [CrossRef] [PubMed]
- Jericho, H.; Sansotta, N.; Guandalini, S. Extraintestinal Manifestations of Celiac Disease: Effectiveness of the Gluten-Free Diet. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.R.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition Guidelines for the Diagnosis of Coeliac Disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, A.; Laszkowska, M.; Sundstrom, J.; Lebwohl, B.; Green, P.H.; Kämpe, O.; Ludvigsson, J.F. Prevalence of Celiac Disease in Patients with Autoimmune Thyroid Disease: A Meta-Analysis. Thyroid 2016, 26, 880–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, M.A.; Blanshard, R.J.; Naylor, G.; Penny, H.A.; Mooney, P.D.; Sanders, D.S. Do gastroenterologists have medical inertia towards coeliac disease? A UK multicentre secondary care study. BMJ Open Gastroenterol. 2021, 8, e000544. [Google Scholar] [CrossRef]
- Choroby Wewnętrzne: Podręcznik dla Studentów; Red. Kokot F. wyd. V; PZWL: Warsaw, Poland, 1991; p. 220.
- Choroby Wewnętrzne: Podręcznik dla Studentów; Red. Kokot F. wyd. VI; PZWL: Warsaw, Poland, 1996.
- Choung, R.S.; Lamba, A.; Marietta, E.V.; See, J.A.; Larson, J.J.; King, K.S.; Van Dyke, C.T.; Rubio-Tapia, A.; Murray, J.A. Effect of a Gluten-free Diet on Quality of Life in Patients With Nonclassical Versus Classical Presentations of Celiac Disease. J. Clin. Gastroenterol. 2019, 54, 620–625. [Google Scholar] [CrossRef]
- Aaron, L.; Torsten, M. Gluten-free Diet-Tough Alley in Torrid Time. Int. J. Celiac Dis. 2017, 5, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Lerner, A.; O’Bryan, T.; Matthias, T. Navigating the Gluten-Free Boom: The Dark Side of Gluten Free Diet. Front. Pediatr. 2019, 7, 414. [Google Scholar] [CrossRef] [Green Version]
- Midhagen, G.; Aberg, A.-K.; Olcén, P.; Järnerot, G.; Valdimarsson, T.; Dahlbom, I.; Hansson, T.; Ström, M. Antibody levels in adult patients with coeliac disease during gluten-free diet: A rapid initial decrease of clinical importance. J. Intern. Med. 2004, 256, 519–524. [Google Scholar] [CrossRef]
- McAllister, B.P.; Williams, E.; Clarke, K. A Comprehensive Review of Celiac Disease/Gluten-Sensitive Enteropathies. Clin. Rev. Allergy Immunol. 2019, 57, 226–243. [Google Scholar] [CrossRef]
- Husby, S.; Murray, J.A.; Katzka, D.A. AGA Clinical Practice Update on Diagnosis and Monitoring of Celiac Disease—Changing Utility of Serology and Histologic Measures: Expert Review. Gastroenterology 2019, 156, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Lundin, K.E.A.; Wijmenga, C. Coeliac disease and autoimmune disease—Genetic overlap and screening. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Chang, C.; Gershwin, M.E. IgA deficiency and autoimmunity. Autoimmun. Rev. 2014, 13, 163–177. [Google Scholar] [CrossRef] [PubMed]
- Ventura, A.; Magazzù, G.; Greco, L. Duration of exposure to gluten and risk for autoimmune disorders in patients with celiac disease. SIGEP Study Group for Autoimmune Disorders in Celiac Disease. Gastroenterology 1999, 117, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Cosnes, J.; Cellier, C.; Viola, S.; Colombel, J.-F.; Michaud, L.; Sarles, J.; Hugot, J.-P.; Ginies, J.-L.; Dabadie, A.; Mouterde, O.; et al. Incidence of Autoimmune Diseases in Celiac Disease: Protective Effect of the Gluten-Free Diet. Clin. Gastroenterol. Hepatol. 2008, 6, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Guidetti, C.S.; Solerio, E.; Scaglione, N.; Aimo, G.; Mengozzi, G. Duration of gluten exposure in adult coeliac disease does not correlate with the risk for autoimmune disorders. Gut 2001, 49, 502–505. [Google Scholar] [CrossRef] [Green Version]
- Cervio, E.; Volta, U.; Verri, M.; Boschi, F.; Pastoris, O.; Granito, A.; Barbara, G.; Parisi, C.; Felicani, C.; Tonini, M.; et al. Sera of Patients With Celiac Disease and Neurologic Disorders Evoke a Mitochondrial-Dependent Apoptosis In Vitro. Gastroenterology 2007, 133, 195–206. [Google Scholar] [CrossRef]
- Tovoli, F.; Negrini, G.; Sansone, V.; Faggiano, C.; Catenaro, T.; Bolondi, L.; Granito, A. Celiac Disease Diagnosed through Screening Programs in At-Risk Adults Is Not Associated with Worse Adherence to the Gluten-Free Diet and Might Protect from Osteopenia/Osteoporosis. Nutrients 2018, 10, 1940. [Google Scholar] [CrossRef] [Green Version]
- Eudy, A.M.; McDaniel, G.; Clowse, M.E.B. Pregnancy in rheumatoid arthritis: A retrospective study. Clin. Rheumatol. 2017, 37, 789–794. [Google Scholar] [CrossRef]
- Fuchs, V.; Kurppa, K.; Huhtala, H.; Collin, P.; Mäki, M.; Kaukinen, K. Factors associated with long diagnostic delay in celiac disease. Scand. J. Gastroenterol. 2014, 49, 1304–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norström, F.; Lindholm, L.; Sandström, O.; Nordyke, K.; Ivarsson, A. Delay to celiac disease diagnosis and its implications for health-related quality of life. BMC Gastroenterol. 2011, 11, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Variables | All Patients | Children | Adults | |
|---|---|---|---|---|
| No. of included questionnaires | 796 | 224 (28.1%) | 572 (71.9%) | |
| Sex—No. (%) | Female | 642 (80.7%) | 131 (58.5%) | 511 (89.3%) |
| Male | 127 (19.3%) | 93 (41.5%) | 61 (10.7%) 1 | |
| Average age at survey in years—Mean (SD) | 29.4 (16.0) | 9.7 (3.8) | 37.2 (11.7) | |
| Average age at diagnosis in years—Mean (SD) | 24.1 (15.9) | 6.8 (4.2) | 34.3 (10.6) | |
| Symptoms | Number and Percentage of Patients Reporting Each Symptom | Mean Duration in Years Prior to CD Diagnosis | ||||||
|---|---|---|---|---|---|---|---|---|
| All Patients (n = 796) | Children (n = 294) 1 | Adults (n = 502) 1 | p | All Patients (n = 796) | Children (n = 294) 1 | Adults (n = 502) 1 | p | |
| Flatulence | 465 (58.4%) | 152 (51.7%) | 313 (62.4%) | 0.003 | 8.1 | 3.6 | 10.3 | <0.001 |
| Abdominal pain/Bloating | 552 (69.3%) | 207 (70.4%) | 345 (68.7%) | 0.619 | 7.1 | 3.1 | 9.4 | <0.001 |
| Chronic fatigue | 486 (61.0%) | 112 (38.1%) | 374 (74.5%) | <0.001 | 6.3 | 2.9 | 7.3 | <0.001 |
| Anemia | 440 (55.2%) | 120 (40.8%) | 320 (63.7%) | <0.001 | 9.2 | 2.8 | 11.6 | <0.001 |
| Diarrhea | 434 (54.5%) | 143 (48.6%) | 291 (58.0%) | 0.011 | 4.7 | 2.4 | 5.8 | 0.001 |
| Headaches | 350 (43.9%) | 80 (27.2%) | 270 (53.8%) | <0.001 | 8.6 | 3.1 | 10.3 | <0.001 |
| Weight loss | 337 (42.3%) | 118 (40.1%) | 219 (43.6%) | <0.001 | 5.2 | 3.0 | 6.4 | 0.014 |
| Skin rash | 289 (36.3%) | 105 (35.7%) | 184 (36.7%) | 0.790 | 7.4 | 3.9 | 9.3 | <0.001 |
| Joint pains | 269 (33.7%) | 60 (20.4%) | 209 (41.6%) | <0.001 | 7.6 | 3.7 | 8.8 | <0.001 |
| Constipation | 271 (34.0%) | 83 (28.2%) | 188 (37.5%) | 0.008 | 8.5 | 2.7 | 11.1 | <0.001 |
| Mouth ulcer | 256 (32.1%) | 58 (19.7%) | 198 (39.4%) | <0.001 | 7.2 | 2.8 | 8.5 | <0.001 |
| Depression | 145 (18.2%) | 17 (5.8%) | 128 (25.5%) | <0.001 | 5.8 | 4.1 | 6.0 | 0.298 |
| Ataxia | 58 (7.2%) | 21 (7.1%) | 37 (7.4%) | 0.905 | 5.6 | 2.9 | 7.1 | 0.465 |
| Osteoporosis | 53 (6.6%) | 10 (3.4%) | 43 (8.6%) | 0.005 | 6.5 | 0.6 | 7.9 | <0.001 |
| No symptoms | 26 (3.2%) | 13 (4.4%) | 13 (2.6%) | 0.160 | NA 2 | NA | NA | NA |
| Symptoms | Number and Percentage of Patients Reporting Each Symptom | Mean Duration in Years after CD Diagnosis | ||||||
|---|---|---|---|---|---|---|---|---|
| All Patients (n = 796) | Children (n = 294) 1 | Adults (n = 502) 1 | p | All Patients (n = 796) | Children (n = 294) 1 | Adults (n = 502) 1 | p | |
| Flatulence | 333 (41.8%) | 93 (31.6%) | 240 (47.8%) | <0.001 | 3.7 | 2.7 | 4.1 | 0.055 |
| Abdominal pain/Bloating | 311 (39.0%) | 109 (37.0%) | 202 (40.2%) | 0.377 | 2.1 | 2.0 | 2.2 | 0.719 |
| Chronic fatigue | 278 (34.9%) | 57 (19.3%) | 221 (44.0%) | <0.001 | 2.7 | 2.5 | 2.8 | 0.656 |
| Anemia | 214 (26.8%) | 5 (1.7%) | 161 (32.0%) | <0.001 | 3.0 | 1.4 | 3.6 | 0.001 |
| Diarrhea | 203 (25.5%) | 54 (18.3%) | 149 (29.6%) | <0.001 | 1.6 | 1.5 | 1.6 | 0.876 |
| Headaches | 225 (28.2%) | 59 (20.0%) | 166 (33.0%) | <0.001 | 4.7 | 5.5 | 4.4 | 0.363 |
| Weight loss | 129 (16.2%) | 36 (12.2%) | 93 (18.5%) | 0.020 | 2.4 | 3.0 | 6.4 | 0.260 |
| Skin rash | 176 (22.1%) | 57 (19.3%) | 119 (23.7%) | 0.157 | 2.9 | 2.8 | 2.9 | 0.871 |
| Joint pains | 181 (22.7%) | 43 (14.6%) | 138 (27.4%) | <0.001 | 3.6 | 4.6 | 3.3 | 0.244 |
| Constipation | 185 (23.2%) | 53 (18.0%) | 132 (26.2%) | 0.008 | 2.7 | 1.8 | 3.0 | 0.256 |
| Mouth ulcer | 117 (14.6%) | 27 (9.1%) | 90 (17.9%) | 0.001 | 2.3 | 2.1 | 2.4 | 0.759 |
| Depression | 90 (11.3%) | 21 (7.1%) | 69 (13.7%) | 0.005 | 3.1 | 3.2 | 3.1 | 0.916 |
| Ataxia | 32 (4.0%) | 11 (3.7%) | 21 (4.1%) | 0.759 | 3.0 | 4.2 | 2.4 | 0.336 |
| Osteoporosis | 46 (5.7%) | 8 (2.7%) | 38 (7.5%) | 0.005 | 5.2 | 1.3 | 6.0 | 0.163 |
| No symptoms | 155 (19.4%) | 80 (27.2%) | 75 (14.9%) | <0.001 | - | - | - | - |
| Comorbid Diseases | All Respondents (n = 796) | Children (n = 224) | Adults (n = 572) | p |
|---|---|---|---|---|
| Thyroid diseases | 23.4% | 9.8% | 28.8% | <0.001 |
| Depression | 12.6% | 2.2% | 16.7% | <0.001 |
| IgA 1 deficiency | 10.7% | 13.3% | 9.6% | 0.128 |
| Miscarriages | 9.4% | 0.0% | 13.2% | <0.001 |
| Liver diseases | 4.2% | 0.9% | 5.4% | 0.004 |
| Infertility | 4.2% | 0.0% | 5.4% | 0.004 |
| Type 1 diabetes mellitus | 3.5% | 5.3% | 2.8% | 0.082 |
| Oncological diseases | 1.9% | 0.0% | 2.6% | 0.014 |
| Genetic syndrome | 1.1% | 3.1% | 0.4% | 0.001 |
| Attention-deficit hyperactivity disorder | 1.0% | 2.2% | 0.5% | 0.031 |
| Myocardial infarction | 0.6% | 0.0% | 0.9% | 0.159 |
| Stroke | 0.4% | 0.0% | 0.5% | 0.276 |
| Other diseases 2 | 40.3% | 34.2% | 42.7% | 0.028 |
| No comorbid disease | 16.8% | 29.8% | 11.7% | <0.001 |
| All Respondents (n = 796) | Children (n = 294) 1 | Adults (n = 502) 1 | p | |
|---|---|---|---|---|
| Serological tests | 667 (83.7%) | 270 (91.8%) | 397 (79.0%) | 0.0001 |
| Duodenal biopsy | 645 (81.0%) | 227 (77.2%) | 418 (83.2%) | 0.0394 |
| Genetic tests (HLA-typing) | 211 (26.5%) | 117 (39.7%) | 94 (18.7%) | 0.0001 |
| Duration of Symptoms before the Diagnosis in Years | All Patients (n = 796) | Children (n = 224) | Adults (n = 572) | |||
|---|---|---|---|---|---|---|
| Number of Appointments | Mean | Number of Appointments | Mean | Number of Appointments | Mean | |
| <1 | 94 | 7.6 | 63 | 9.0 | 31 | 4.7 |
| 1–5 | 367 | 13.5 | 189 | 15.9 | 178 | 11.0 |
| 5–10 | 164 | 20.2 | 31 | 19.8 | 133 | 20.3 |
| 10–20 | 124 | 28.0 | 9 | 20.7 | 115 | 28.5 |
| >20 | 43 | 36.5 | 0 | - | 43 | 36.5 |
| In total | 792 2 | 17.7 | 293 | 15.2 | 500 | 19.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Majsiak, E.; Choina, M.; Gray, A.M.; Wysokiński, M.; Cukrowska, B. Clinical Manifestation and Diagnostic Process of Celiac Disease in Poland—Comparison of Pediatric and Adult Patients in Retrospective Study. Nutrients 2022, 14, 491. https://doi.org/10.3390/nu14030491
Majsiak E, Choina M, Gray AM, Wysokiński M, Cukrowska B. Clinical Manifestation and Diagnostic Process of Celiac Disease in Poland—Comparison of Pediatric and Adult Patients in Retrospective Study. Nutrients. 2022; 14(3):491. https://doi.org/10.3390/nu14030491
Chicago/Turabian StyleMajsiak, Emilia, Magdalena Choina, Alastair M. Gray, Mariusz Wysokiński, and Bożena Cukrowska. 2022. "Clinical Manifestation and Diagnostic Process of Celiac Disease in Poland—Comparison of Pediatric and Adult Patients in Retrospective Study" Nutrients 14, no. 3: 491. https://doi.org/10.3390/nu14030491
APA StyleMajsiak, E., Choina, M., Gray, A. M., Wysokiński, M., & Cukrowska, B. (2022). Clinical Manifestation and Diagnostic Process of Celiac Disease in Poland—Comparison of Pediatric and Adult Patients in Retrospective Study. Nutrients, 14(3), 491. https://doi.org/10.3390/nu14030491