
Validation of the MSM and NCI Method for Estimating the Usual Intake of Nutrients and Food According to Four Seasons of Seven Consecutive Daily 24 Hour Dietary Recalls in Chinese Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection and Measurements
2.3. Dietary Intake Assessment
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Characteristics of True Intake (28 Day Mean Intake)
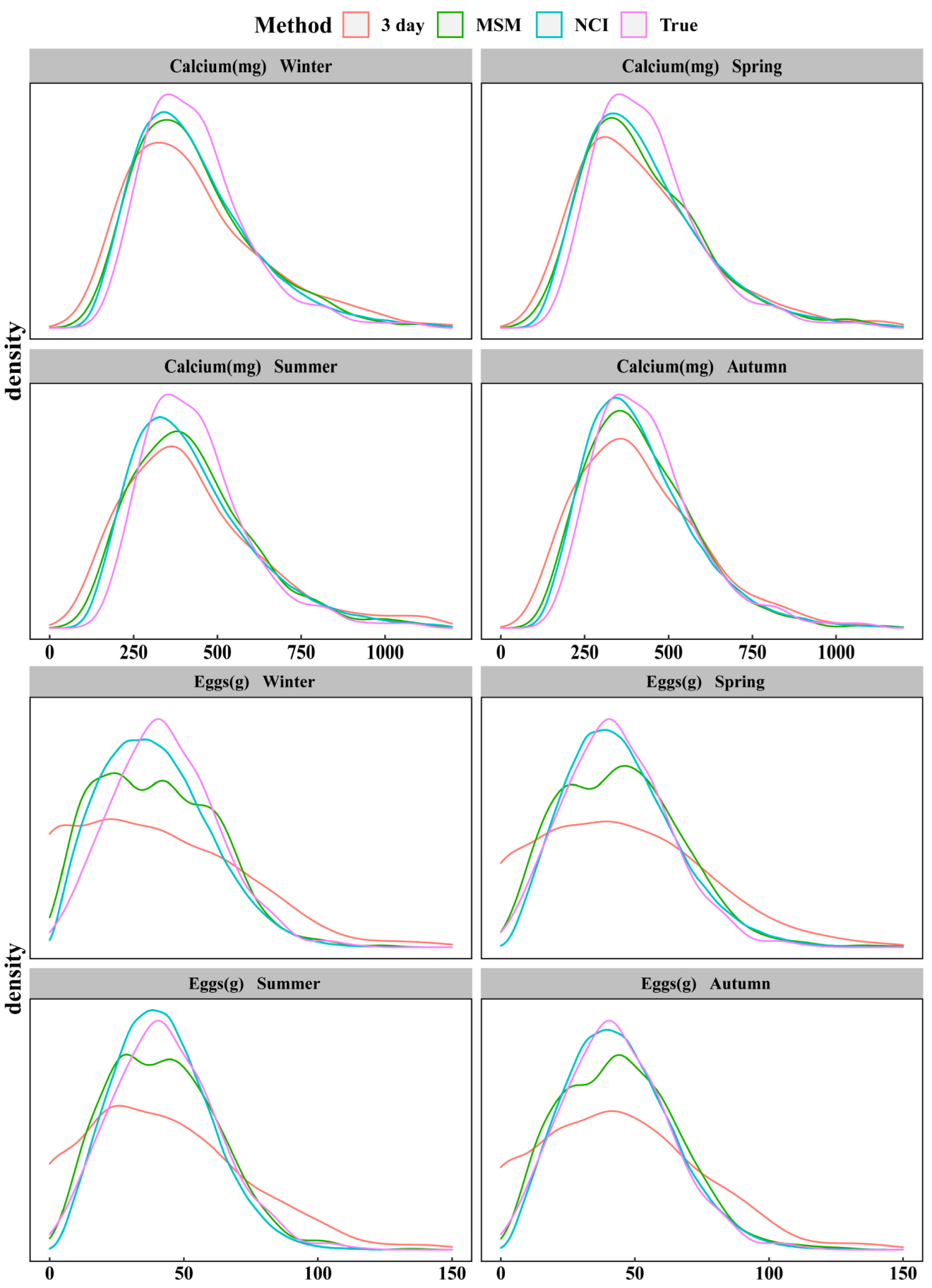
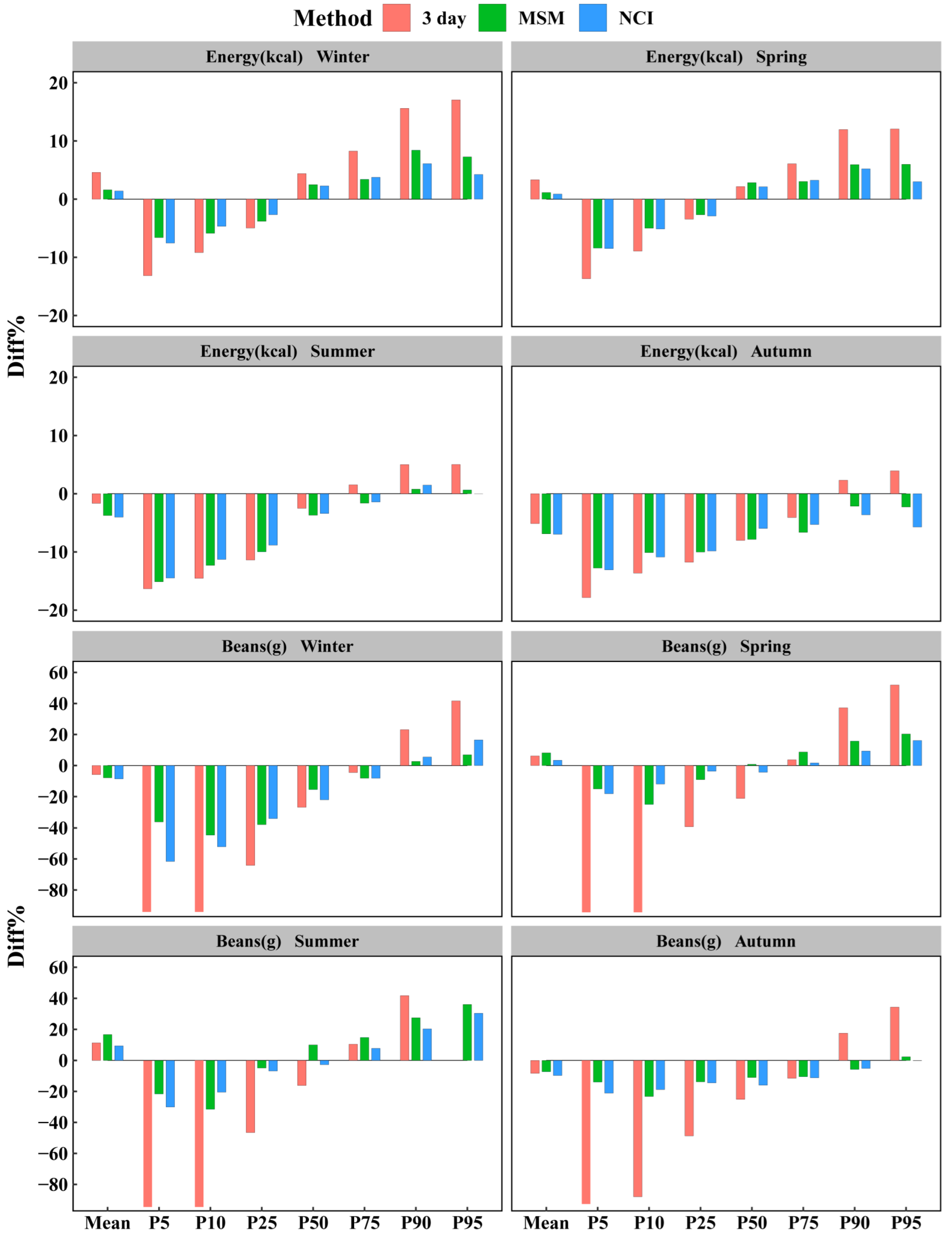
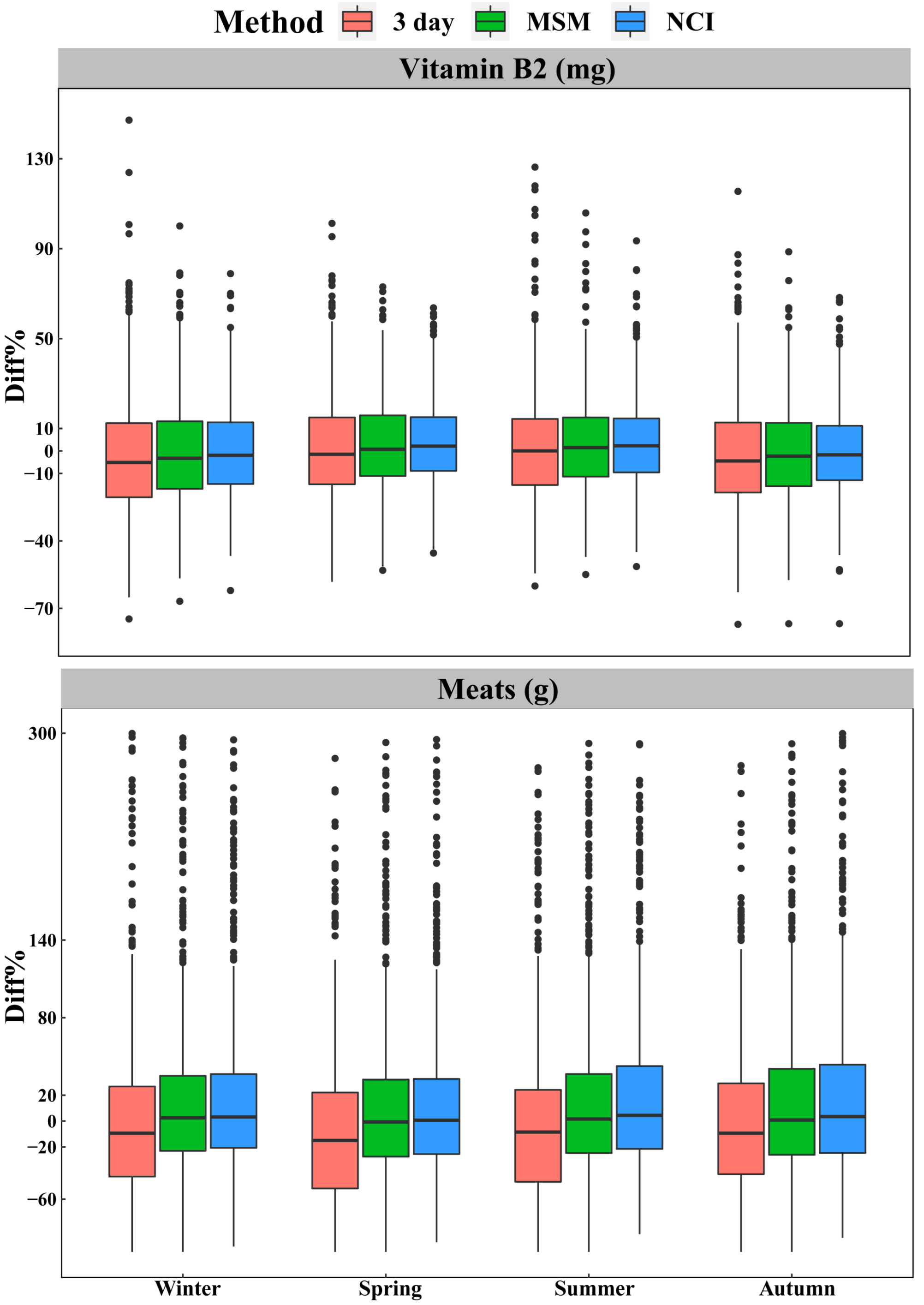
3.3. Comparison for Intake at Group Level
3.4. Comparison for Intake at Individual Level
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Conrad, J.; Nothlings, U. Innovative approaches to estimate individual usual dietary intake in large-scale epidemiological studies. Proc. Nutr. Soc. 2017, 76, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Cogswell, M.E.; Zhang, Z.; Carriquiry, A.L.; Gunn, J.P.; Kuklina, E.V.; Saydah, S.H.; Yang, Q.; Moshfegh, A.J. Sodium and potassium intakes among US adults: NHANES 2003–2008. Am. J. Clin. Nutr. 2012, 96, 647–657. [Google Scholar] [CrossRef] [Green Version]
- Ortega, R.M.; Perez-Rodrigo, C.; Lopez-Sobaler, A.M. Dietary assessment methods: Dietary records. Nutr. Hosp. 2015, 31 (Suppl. 3), 38–45. [Google Scholar] [CrossRef]
- Perez Rodrigo, C.; Aranceta, J.; Salvador, G.; Varela-Moreiras, G. Food frequency questionnaires. Nutr. Hosp. 2015, 31 (Suppl. 3), 49–56. [Google Scholar] [CrossRef] [PubMed]
- Statistics, N.C.F.H. National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 5 July 2018).
- Canada, H. Reference Guide to Understanding and Using the Data—2015 Canadian Community Health Survey—Nutrition. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/food-nutrition-surveillance/health-nutrition-surveys/canadian-community-health-survey-cchs/ (accessed on 15 December 2021).
- Zhao, F.L.; He, L.; Zhao, L.Y.; Guo, Q.Y.; Yu, D.M.; Ju, L.H.; Fang, H.Y. The Status of Dietary Energy and Nutrients Intakes among Chinese Elderly Aged 80 and Above: Data from the CACDNS 2015. Nutrients 2021, 13, 1622. [Google Scholar] [CrossRef] [PubMed]
- Walter, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Luo, H.; Dodd, K.W.; Arnold, C.D.; Engle-Stone, R. A New Statistical Method for Estimating Usual Intakes of Nearly-Daily Consumed Foods and Nutrients Through Use of Only One 24-hour Dietary Recall. J. Nutr. 2019, 149, 1667–1673. [Google Scholar] [CrossRef] [PubMed]
- Laureano, G.H.; Torman, V.B.; Crispim, S.P.; Dekkers, A.L.; Camey, S.A. Comparison of the ISU, NCI, MSM, and SPADE Methods for Estimating Usual Intake: A Simulation Study of Nutrients Consumed Daily. Nutrients 2016, 8, 166. [Google Scholar] [CrossRef]
- Dodd, K.W.; Guenther, P.M.; Freedman, L.S.; Subar, A.F.; Kipnis, V.; Midthune, D.; Tooze, J.A.; Krebs-Smith, S.M. Statistical methods for estimating usual intake of nutrients and foods: A review of the theory. J. Am. Diet. Assoc. 2006, 106, 1640–1650. [Google Scholar] [CrossRef]
- Souverein, O.W.; Dekkers, A.L.; Geelen, A.; Haubrock, J.; de Vries, J.H.; Ocke, M.C.; Harttig, U.; Boeing, H.; van’t Veer, P.; Consortium, E. Comparing four methods to estimate usual intake distributions. Eur. J. Clin. Nutr. 2011, 65 (Suppl. 1), S92–S101. [Google Scholar] [CrossRef] [Green Version]
- Tooze, J.A.; Midthune, D.; Dodd, K.W.; Freedman, L.S.; Krebs-Smith, S.M.; Subar, A.F.; Guenther, P.M.; Carroll, R.J.; Kipnis, V. A new statistical method for estimating the usual intake of episodically consumed foods with application to their distribution. J. Am. Diet. Assoc. 2006, 106, 1575–1587. [Google Scholar] [CrossRef] [Green Version]
- Harttig, U.; Haubrock, J.; Knuppel, S.; Boeing, H.; Consortium, E. The MSM program: Web-based statistics package for estimating usual dietary intake using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65 (Suppl. 1), S87–S91. [Google Scholar] [CrossRef] [Green Version]
- Pereira, J.L.; de Castro, M.A.; Crispim, S.P.; Fisberg, R.M.; Isasi, C.R.; Mossavar-Rahmani, Y.; Van Horn, L.; Carnethon, M.R.; Daviglus, M.L.; Perreira, K.M.; et al. Comparing Methods from the National Cancer Institute vs Multiple Source Method for Estimating Usual Intake of Nutrients in the Hispanic Community Health Study/Study of Latino Youth. J. Acad. Nutr. Diet. 2021, 121, 59–73. [Google Scholar] [CrossRef]
- Xu, X.; Hall, J.; Byles, J.; Shi, Z. Dietary Pattern Is Associated with Obesity in Older People in China: Data from China Health and Nutrition Survey (CHNS). Nutrients 2015, 7, 8170–8188. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Zhao, L.; Zhao, W. Status and trends in consumption of grains and dietary fiber among Chinese adults (1982–2015). Nutr. Rev. 2020, 78, 43–53. [Google Scholar] [CrossRef] [PubMed]
- St George, S.M.; Van Horn, M.L.; Lawman, H.G.; Wilson, D.K. Reliability of 24-Hour Dietary Recalls as a Measure of Diet in African-American Youth. J. Acad. Nutr. Diet. 2016, 116, 1551–1559. [Google Scholar] [CrossRef] [PubMed]
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.X. Chinese Food Composition Tables, 2nd ed.; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Miyazaki, M.; Doi, Y.; Ikeda, F.; Ninomiya, T.; Hata, J.; Uchida, K.; Shirota, T.; Matsumoto, T.; Iida, M.; Kiyohara, Y. Dietary vitamin A intake and incidence of gastric cancer in a general Japanese population: The Hisayama Study. Gastric Cancer 2012, 15, 162–169. [Google Scholar] [CrossRef]
- Kwon, Y.J.; Lee, H.S.; Chang, H.J.; Koh, S.B.; Lee, J.W. Association of dietary lipid intake with low-density lipoprotein cholesterol levels: Analysis of two independent population-based studies. Eur. J. Nutr. 2020, 59, 2557–2567. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, S.; Ghosh, S.; Varghese, J.S.; Sachdev, H.S.; Kurpad, A.V.; Thomas, T. Dietary Iron Intake and Anemia Are Weakly Associated, Limiting Effective Iron Fortification Strategies in India. J. Nutr. 2019, 149, 831–839. [Google Scholar] [CrossRef]
- Comerford, K.B.; Pasin, G. Emerging Evidence for the Importance of Dietary Protein Source on Glucoregulatory Markers and Type 2 Diabetes: Different Effects of Dairy, Meat, Fish, Egg, and Plant Protein Foods. Nutrients 2016, 8, 446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kipnis, V.; Midthune, D.; Buckman, D.W.; Dodd, K.W.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Tooze, J.A.; Carroll, R.J.; Freedman, L.S. Modeling data with excess zeros and measurement error: Application to evaluating relationships between episodically consumed foods and health outcomes. Biometrics 2009, 65, 1003–1010. [Google Scholar] [CrossRef] [Green Version]
- Krebs-Smith, S.M.; Guenther, P.M.; Subar, A.F.; Kirkpatrick, S.I.; Dodd, K.W. Americans do not meet federal dietary recommendations. J. Nutr. 2010, 140, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Haubrock, J.; Nothlings, U.; Volatier, J.L.; Dekkers, A.; Ocke, M.; Harttig, U.; Illner, A.K.; Knuppel, S.; Andersen, L.F.; Boeing, H.; et al. Estimating usual food intake distributions by using the multiple source method in the EPIC-Potsdam Calibration Study. J. Nutr. 2011, 141, 914–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freese, J.; Pricop-Jeckstadt, M.; Heuer, T.; Clemens, M.; Boeing, H.; Knuppel, S.; Nothlings, U. Determinants of consumption-day amounts applicable for the estimation of usual dietary intake with a short 24-h food list. J. Nutr. Sci. 2016, 5, e35. [Google Scholar] [CrossRef] [Green Version]
- Herrick, K.A.; Rossen, L.M.; Parsons, R.; Dodd, K.W. Estimating Usual Dietary Intake From National Health and Nutrition Examination Survey Data Using the National Cancer Institute Method. Vital. Health Stat. 2018, 2, 1–63. [Google Scholar]
- Verly, E., Jr.; Oliveira, D.C.; Fisberg, R.M.; Marchioni, D.M. Performance of statistical methods to correct food intake distribution: Comparison between observed and estimated usual intake. Br. J. Nutr. 2016, 116, 897–903. [Google Scholar] [CrossRef] [Green Version]
- Davis, K.A.; Gonzalez, A.; Loukine, L.; Qiao, C.; Sadeghpour, A.; Vigneault, M.; Wang, K.C.; Ibanez, D. Early Experience Analyzing Dietary Intake Data from the Canadian Community Health Survey-Nutrition Using the National Cancer Institute (NCI) Method. Nutrients 2019, 11, 1908. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dietary Components | Means ± SD | CV% | Percentile | VR | Percentage of Zero Intake | r | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5th | 10th | 25th | 50th | 75th | 90th | 95th | ||||||
| Energy (kcal) | 1631.76 ± 468.63 | 28.72 | 1028.69 | 1121.70 | 1332.30 | 1562.52 | 1881.97 | 2181.79 | 2450.58 | 1.35 | 0.00 | - |
| Protein (g) | 68.48 ± 22.07 | 32.23 | 40.19 | 45.21 | 53.80 | 64.65 | 79.36 | 94.01 | 105.74 | 1.43 | 0.00 | - |
| Fat (g) | 38.86 ± 16.87 | 43.42 | 15.46 | 19.35 | 26.04 | 37.15 | 48.69 | 59.78 | 69.16 | 1.98 | 0.00 | - |
| CHO (g) | 252.91 ± 93.94 | 37.14 | 140.73 | 154.93 | 186.27 | 231.04 | 300.47 | 383.04 | 431.23 | 0.92 | 0.00 | - |
| Cholesterol (g) | 383.49 ± 189.64 | 49.45 | 117.42 | 167.05 | 266.38 | 363.28 | 483.74 | 607.24 | 687.07 | 3.09 | 8.99 | 0.30 |
| Calcium (mg) | 439.03 ± 181.43 | 41.32 | 229.35 | 263.68 | 323.06 | 412.32 | 512.41 | 639.56 | 747.78 | 2.09 | 0.00 | - |
| Iron (mg) | 20.15 ± 6.17 | 30.63 | 12.20 | 13.62 | 16.01 | 19.10 | 23.32 | 27.51 | 31.01 | 2.44 | 0.00 | - |
| Vitamin A(μgRAE) | 424.09 ± 211.53 | 49.88 | 198.04 | 232.12 | 288.46 | 378.39 | 509.77 | 679.63 | 774.51 | 4.26 | 0.07 | - |
| Vitamin E (mg) | 11.99 ± 4.06 | 33.87 | 6.75 | 7.54 | 9.14 | 11.41 | 13.99 | 17.17 | 19.39 | 3.62 | 0.00 | - |
| Vitamin B2 (mg) | 0.83 ± 0.26 | 31.58 | 0.49 | 0.55 | 0.67 | 0.81 | 0.96 | 1.11 | 1.24 | 1.76 | 0.00 | - |
| Rice (g) | 69.18 ± 54.26 | 78.44 | 15.49 | 21.78 | 34.15 | 56.47 | 90.63 | 125.89 | 159.97 | 1.25 | 26.22 | −0.37 |
| Eggs (g) | 43.66 ± 21.96 | 50.29 | 13.26 | 18.70 | 29.63 | 41.66 | 55.53 | 68.28 | 78.43 | 3.94 | 41.82 | 0.12 |
| Beans (g) | 51.37 ± 31.65 | 61.60 | 9.21 | 14.84 | 27.58 | 48.01 | 70.02 | 92.29 | 105.86 | 4.67 | 30.16 | 0.61 * |
| Vegetables (g) | 225.69 ± 102.43 | 45.39 | 95.64 | 117.25 | 151.59 | 207.51 | 278.14 | 349.35 | 416.25 | 2.33 | 3.98 | - |
| Meats (g) | 147.44 ± 131.04 | 88.88 | 4.18 | 9.18 | 37.80 | 120.87 | 229.26 | 313.97 | 381.25 | 0.83 | 26.57 | 0.89 * |
| Dietary Components | Winter | Spring | Summer | Autumn | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | 10th | 50th | 90th | Mean | 10th | 50th | 90th | Mean | 10th | 50th | 90th | Mean | 10th | 50th | 90th | |
| Energy (kcal) | ||||||||||||||||
| 3 day | 1706.86 | 1018.78 | 1631.17 | 2522.07 | 1686.00 | 1021.55 | 1596.21 | 2442.64 | 1604.67 | 958.71 | 1523.27 | 2290.93 | 1548.06 | 968.68 | 1437.18 | 2232.40 |
| MSM | 1657.76 | 1055.86 | 1601.42 | 2365.20 | 1650.34 | 1065.66 | 1606.75 | 2311.27 | 1570.69 | 983.59 | 1504.74 | 2198.98 | 1519.31 | 1008.09 | 1439.81 | 2134.93 |
| NCI | 1654.59 | 1069.43 | 1598.12 | 2314.74 | 1645.94 | 1064.35 | 1595.87 | 2295.62 | 1566.16 | 995.06 | 1509.31 | 2213.90 | 1518.06 | 999.72 | 1469.31 | 2102.41 |
| 3 day (Diff%) | 4.60 | −9.18 | 4.39 | 15.60 | 3.32 | −8.93 | 2.16 | 11.96 | −1.66 | −14.53 | −2.51 | 5.00 | −5.13 | −13.64 | −8.02 | 2.32 |
| MSM (Diff%) | 1.59 | −5.87 | 2.49 | 8.41 | 1.14 | −5.00 | 2.83 | 5.93 | −3.74 | −12.31 | −3.70 | 0.79 | −6.89 | −10.13 | −7.85 | −2.15 |
| NCI (Diff%) | 1.40 | −4.66 | 2.28 | 6.09 | 0.87 | −5.11 | 2.13 | 5.22 | −4.02 | −11.29 | −3.41 | 1.47 | −6.97 | −10.87 | −5.97 | −3.64 |
| Cholesterol (mg) | ||||||||||||||||
| 3 day | 373.25 | 68.69 | 340.67 | 669.87 | 399.79 | 100.15 | 352.06 | 713.71 | 385.71 | 107.96 | 361.26 | 683.42 | 388.63 | 120.12 | 352.90 | 692.27 |
| MSM | 362.71 | 117.18 | 351.76 | 612.40 | 389.47 | 130.92 | 360.12 | 650.03 | 373.07 | 141.94 | 366.08 | 598.38 | 378.42 | 157.21 | 368.19 | 615.76 |
| NCI | 360.28 | 147.26 | 337.57 | 602.74 | 386.59 | 157.20 | 363.42 | 644.91 | 372.53 | 174.71 | 358.91 | 588.87 | 378.93 | 179.00 | 361.82 | 601.18 |
| 3 day (Diff%) | −2.67 | −58.88 | −6.22 | 10.31 | 4.25 | −40.05 | −3.09 | 17.53 | 0.58 | −35.37 | −0.56 | 12.55 | 1.34 | −28.09 | −2.86 | 14.00 |
| MSM (Diff%) | −5.42 | −29.85 | −3.17 | 0.85 | 1.56 | −21.63 | −0.87 | 7.05 | −2.72 | −15.03 | 0.77 | −1.46 | −1.32 | −5.89 | 1.35 | 1.40 |
| NCI (Diff%) | −6.05 | −11.85 | −7.08 | −0.74 | 0.81 | −5.90 | 0.04 | 6.20 | −2.86 | 4.59 | −1.20 | −3.02 | −1.19 | 7.15 | −0.40 | −1.00 |
| Vitamin A (μgRAE) | ||||||||||||||||
| 3 day | 447.06 | 141.17 | 353.31 | 810.93 | 438.82 | 151.01 | 328.13 | 824.68 | 373.91 | 136.50 | 301.82 | 672.43 | 460.76 | 152.21 | 360.83 | 849.18 |
| MSM | 426.33 | 207.37 | 389.98 | 692.78 | 421.00 | 208.79 | 365.43 | 679.43 | 360.08 | 176.11 | 332.64 | 552.62 | 441.40 | 220.58 | 396.09 | 713.24 |
| NCI | 426.15 | 211.00 | 389.22 | 687.24 | 416.32 | 197.08 | 376.81 | 684.42 | 359.03 | 175.70 | 326.77 | 581.95 | 443.95 | 213.73 | 402.01 | 725.85 |
| 3 day (Diff%) | 5.42 | −39.18 | −6.63 | 19.32 | 3.47 | −34.94 | −13.28 | 21.34 | −11.83 | −41.19 | −20.24 | −1.06 | 8.65 | −34.43 | −4.64 | 24.95 |
| MSM (Diff%) | 0.53 | −10.66 | 3.06 | 1.93 | −0.73 | −10.05 | −3.43 | −0.03 | −15.09 | −24.13 | −12.09 | −18.69 | 4.08 | −4.97 | 4.68 | 4.95 |
| NCI (Diff%) | 0.49 | −9.10 | 2.86 | 1.12 | −1.83 | −15.10 | −0.42 | 0.70 | −15.34 | −24.31 | −13.64 | −14.37 | 4.68 | −7.92 | 6.24 | 6.80 |
| Beans (g) | ||||||||||||||||
| 3 day | 48.37 | 0.00 | 35.19 | 113.60 | 54.54 | 0.00 | 37.85 | 126.60 | 57.16 | 0.00 | 40.26 | 130.80 | 47.11 | 1.78 | 35.97 | 108.48 |
| MSM | 47.31 | 8.22 | 40.60 | 94.77 | 55.56 | 11.16 | 48.40 | 106.77 | 59.93 | 10.17 | 52.79 | 117.62 | 47.64 | 11.39 | 42.71 | 86.99 |
| NCI | 46.96 | 7.10 | 37.43 | 97.39 | 53.12 | 13.07 | 45.94 | 100.93 | 56.18 | 11.80 | 46.69 | 111.03 | 46.37 | 12.05 | 40.36 | 87.51 |
| 3 day (Diff%) | −5.84 | −100.00 | −26.70 | 23.09 | 6.17 | −100.00 | −21.16 | 37.18 | 11.27 | −100.00 | −16.14 | 41.73 | −8.29 | −88.01 | −25.08 | 17.54 |
| MSM (Diff%) | −7.90 | −44.61 | −15.43 | 2.69 | 8.16 | −24.80 | 0.81 | 15.69 | 16.66 | −31.47 | 9.96 | 27.45 | −7.26 | −23.25 | −11.04 | −5.74 |
| NCI (Diff%) | −8.58 | −52.16 | −22.04 | 5.53 | 3.41 | −11.93 | −4.31 | 9.36 | 9.36 | −20.49 | −2.75 | 20.31 | −9.73 | −18.80 | −15.93 | −5.18 |
| Meats (g) | ||||||||||||||||
| 3 day | 151.11 | 0.00 | 111.88 | 353.17 | 148.09 | 0.00 | 105.33 | 338.67 | 147.03 | 0.00 | 113.67 | 336.67 | 146.64 | 0.00 | 103.33 | 343.75 |
| MSM | 148.16 | 17.76 | 112.85 | 320.91 | 144.19 | 14.46 | 111.52 | 315.66 | 143.64 | 15.45 | 117.38 | 309.64 | 142.93 | 20.16 | 106.68 | 325.91 |
| NCI | 146.88 | 9.32 | 113.22 | 327.96 | 143.16 | 6.67 | 105.17 | 327.84 | 142.19 | 8.14 | 115.62 | 309.90 | 141.83 | 10.98 | 109.88 | 312.60 |
| 3 day (Diff%) | 2.49 | −100.00 | −7.44 | 12.49 | 0.44 | −100.00 | −12.86 | 7.87 | −0.28 | −100.00 | −5.96 | 7.23 | −0.54 | −100.00 | −14.51 | 9.48 |
| MSM (Diff%) | 0.49 | 93.46 | −6.64 | 2.21 | −2.20 | 57.52 | −7.74 | 0.54 | −2.58 | 68.30 | −2.89 | −1.38 | −3.06 | 119.61 | −11.74 | 3.80 |
| NCI (Diff%) | −0.38 | 1.53 | −6.33 | 4.46 | −2.90 | −27.34 | −12.99 | 4.42 | −3.56 | −11.33 | −4.34 | −1.30 | −3.80 | 19.61 | −9.09 | −0.44 |
| Dietary Components | Method | Bias (Relative Bias%) | |||
|---|---|---|---|---|---|
| Winter | Spring | Summer | Autumn | ||
| Energy (kcal) | 3 day | 281.29 (17.83) | 237.18 (15.03) | 239.73 (15.19) | 250.72 (15.69) |
| MSM | 247.13 (15.80) | 207.66 (13.30) | 211.97 (13.37) | 223.59 (13.85) | |
| NCI | 226.33 (14.67) | 186.86 (12.18) | 191.08 (12.05) | 205.09 (12.62) | |
| Protein (g) | 3 day | 12.84 (19.19) | 12.1 (17.42) | 11.25 (16.87) | 11.72 (17.27) |
| MSM | 11.38 (17.07) | 10.36 (15.26) | 9.91 (14.79) | 10.58 (15.44) | |
| NCI | 10.56 (15.98) | 9.02 (13.70) | 9.13 (13.63) | 9.83 (14.27) | |
| Fat (g) | 3 day | 11.98 (32.15) | 10.01 (26.70) | 10.58 (27.81) | 10.48 (27.65) |
| MSM | 9.73 (27.58) | 7.77 (21.23) | 8.86 (23.87) | 8.82 (23.96) | |
| NCI | 9.00 (27.12) | 7.40 (21.58) | 7.91 (22.61) | 8.11 (23.21) | |
| CHO (g) | 3 day | 46.86 (19.46) | 40.53 (16.89) | 40.46 (16.66) | 40.19 (16.40) |
| MSM | 42.87 (17.95) | 37.04 (15.67) | 37.41 (15.31) | 37.56 (15.13) | |
| NCI | 40.04 (17.05) | 34.16 (14.87) | 34.85 (14.25) | 35.71 (14.27) | |
| Cholesterol (mg) | 3 day | 131.80 (40.89) | 129.06 (37.96) | 116.56 (37.13) | 124.61 (38.72) |
| MSM | 108.15 (33.38) | 105.36 (32.38) | 96.31 (31.34) | 103.59 (33.85) | |
| NCI | 95.04 (32.31) | 89.41 (31.82) | 88.75 (32.34) | 93.95 (35.49) | |
| Calcium (mg) | 3 day | 117.25 (27.00) | 109.00 (24.54) | 108.46 (25.59) | 106.39 (24.49) |
| MSM | 98.69 (23.39) | 92.43 (21.43) | 92.37 (21.55) | 92.72 (21.06) | |
| NCI | 90.19 (21.79) | 80.91 (19.51) | 83.45 (19.62) | 85.67 (19.63) | |
| Iron (mg) | 3 day | 4.62 (23.03) | 4.78 (23.56) | 4.30 (21.49) | 4.34 (21.37) |
| MSM | 3.70 (18.78) | 3.71 (18.76) | 3.42 (17.19) | 3.56 (17.52) | |
| NCI | 3.32 (17.17) | 3.23 (16.94) | 3.02 (15.21) | 3.29 (15.88) | |
| Vitamin A (µgRAE) | 3 day | 187.76 (43.29) | 178.35 (40.45) | 161.82 (37.93) | 183.87 (43.54) |
| MSM | 135.73 (33.82) | 124.80 (30.76) | 122.92 (28.39) | 135.16 (33.44) | |
| NCI | 120.41 (32.07) | 106.36 (27.89) | 110.96 (25.31) | 121.73 (31.72) | |
| Vitamin E (mg) | 3 day | 3.98 (33.61) | 3.69 (30.49) | 3.41 (29.21) | 3.39 (28.68) |
| MSM | 2.99 (26.33) | 2.66 (22.71) | 2.59 (22.06) | 2.45 (20.65) | |
| NCI | 2.63 (24.14) | 2.25 (20.22) | 2.32 (19.66) | 2.23 (18.60) | |
| Vitamin B2 (mg) | 3 day | 0.17 (21.21) | 0.16 (18.70) | 0.15 (19.15) | 0.16 (18.93) |
| MSM | 0.15 (18.43) | 0.13 (16.31) | 0.14 (16.86) | 0.14 (16.44) | |
| NCI | 0.14 (16.90) | 0.12 (14.76) | 0.12 (15.52) | 0.12 (14.95) | |
| Rice (g) | 3 day | 29.13 (54.36) | 28.05 (55.88) | 23.75 (45.46) | 24.67 (45.36) |
| MSM | 24.64 (47.07) | 24.17 (49.88) | 20.51 (38.76) | 21.34 (38.93) | |
| NCI | 21.58 (47.01) | 21.62 (49.15) | 19.26 (37.96) | 20.54 (38.39) | |
| Eggs (g) | 3 day | 20.65 (56.49) | 20.48 (55.29) | 18.38 (51.38) | 19.64 (54.38) |
| MSM | 14.71 (42.36) | 14.81 (44.49) | 12.97 (40.40) | 14.57 (43.93) | |
| NCI | 12.61 (41.31) | 12.33 (46.87) | 11.87 (44.10) | 12.66 (45.80) | |
| Beans (g) | 3 day | 28.87 (64.04) | 30.33 (70.06) | 31.49 (69.63) | 26.55 (62.17) |
| MSM | 22.14 (56.64) | 23.72 (69.07) | 25.17 (70.67) | 19.82 (64.16) | |
| NCI | 21.01 (79.31) | 22.07 (94.69) | 23.70 (96.72) | 19.18 (77.23) | |
| Vegetables (g) | 3 day | 72.38 (34.45) | 66.92 (31.31) | 66.37 (31.57) | 62.65 (29.55) |
| MSM | 63.67 (30.77) | 56.99 (27.05) | 58.49 (27.97) | 54.54 (26.08) | |
| NCI | 57.31 (30.07) | 49.85 (25.60) | 52.36 (26.43) | 49.24 (24.90) | |
| Meats (g) | 3 day | 49.37 (64.84) | 49.36 (51.34) | 46.65 (55.43) | 47.69 (53.01) |
| MSM | 45.55 (114.54) | 42.57 (102.01) | 43.62 (91.89) | 45.18 (117.75) | |
| NCI | 44.63 (105.24) | 40.19 (75.48) | 43.08 (92.01) | 45.14 (91.84) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, K.; Yu, D.; Guo, Q.; Yang, Y.; Wei, X.; Zhao, L.; Fang, H. Validation of the MSM and NCI Method for Estimating the Usual Intake of Nutrients and Food According to Four Seasons of Seven Consecutive Daily 24 Hour Dietary Recalls in Chinese Adults. Nutrients 2022, 14, 445. https://doi.org/10.3390/nu14030445
Huang K, Yu D, Guo Q, Yang Y, Wei X, Zhao L, Fang H. Validation of the MSM and NCI Method for Estimating the Usual Intake of Nutrients and Food According to Four Seasons of Seven Consecutive Daily 24 Hour Dietary Recalls in Chinese Adults. Nutrients. 2022; 14(3):445. https://doi.org/10.3390/nu14030445
Chicago/Turabian StyleHuang, Kun, Dongmei Yu, Qiya Guo, Yuxiang Yang, Xiaoqi Wei, Liyun Zhao, and Hongyun Fang. 2022. "Validation of the MSM and NCI Method for Estimating the Usual Intake of Nutrients and Food According to Four Seasons of Seven Consecutive Daily 24 Hour Dietary Recalls in Chinese Adults" Nutrients 14, no. 3: 445. https://doi.org/10.3390/nu14030445
APA StyleHuang, K., Yu, D., Guo, Q., Yang, Y., Wei, X., Zhao, L., & Fang, H. (2022). Validation of the MSM and NCI Method for Estimating the Usual Intake of Nutrients and Food According to Four Seasons of Seven Consecutive Daily 24 Hour Dietary Recalls in Chinese Adults. Nutrients, 14(3), 445. https://doi.org/10.3390/nu14030445