
Dietary Copper Intake and Risk of Stroke in Adults: A Case-Control Study Based on National Health and Nutrition Examination Survey 2013–2018


Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Copper Intake
2.3. Definition of Disease and Covariates
2.4. Ethics Statement
2.5. Statistical Analysis
3. Results
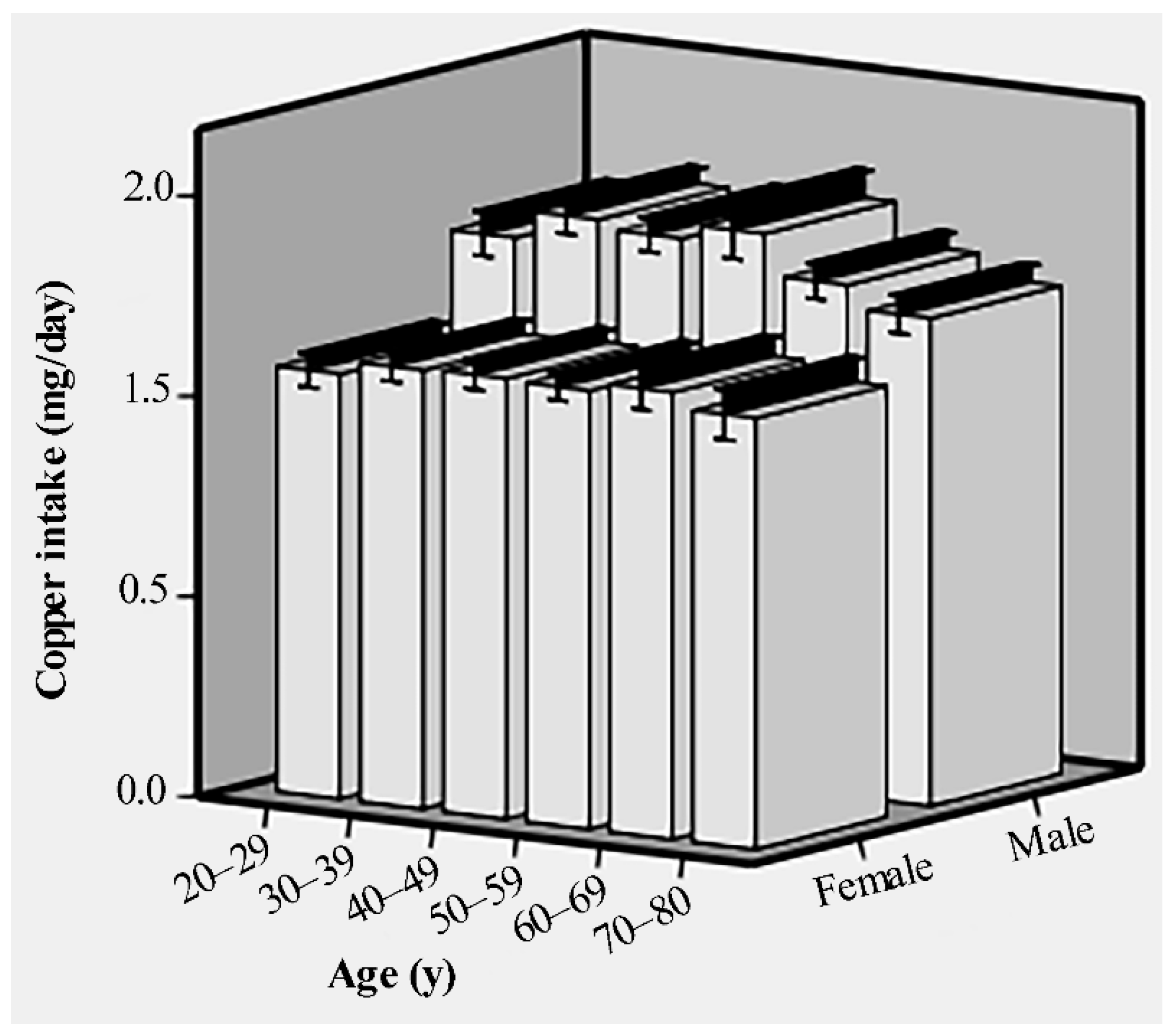
3.1. Participant Characteristics
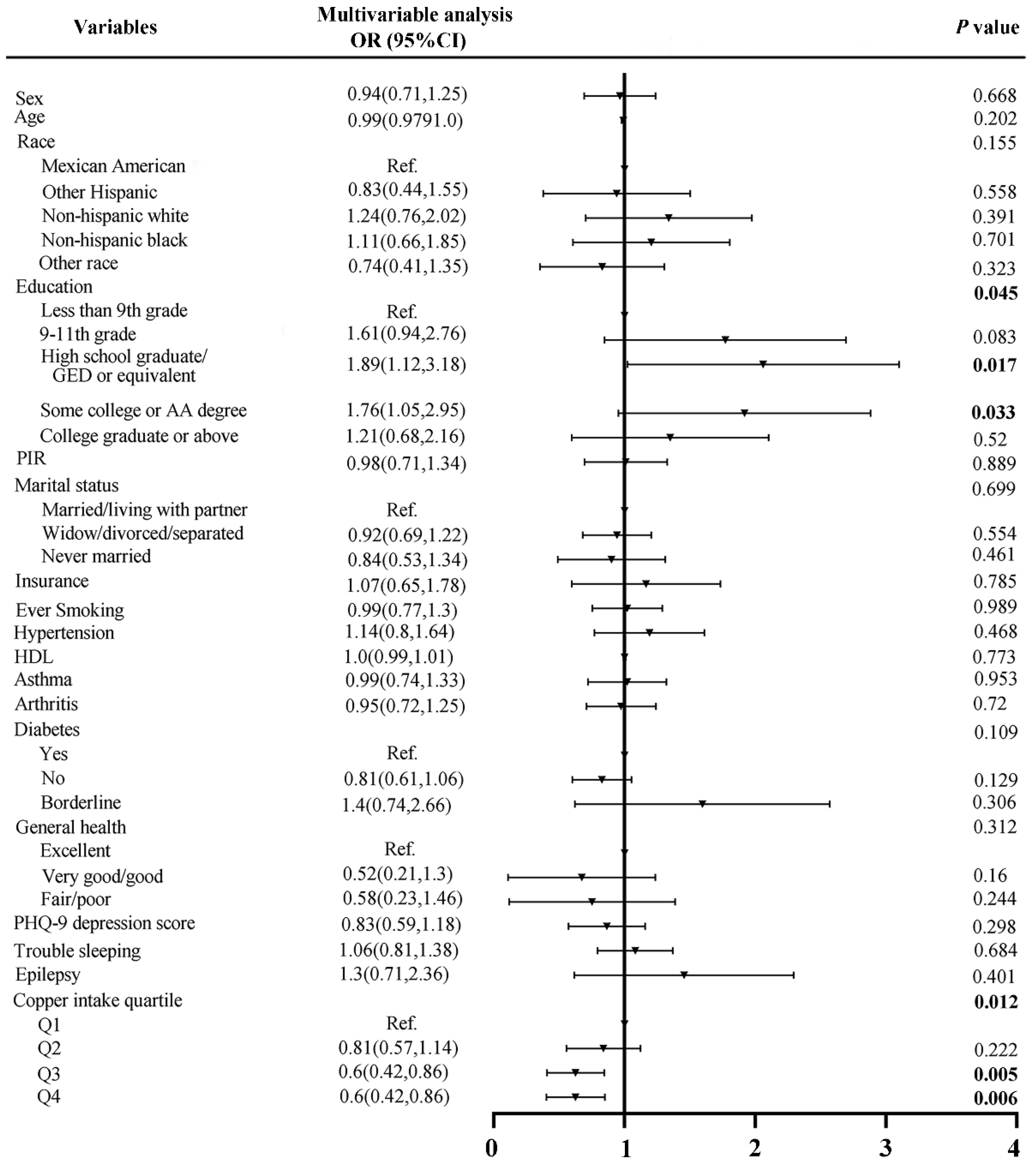
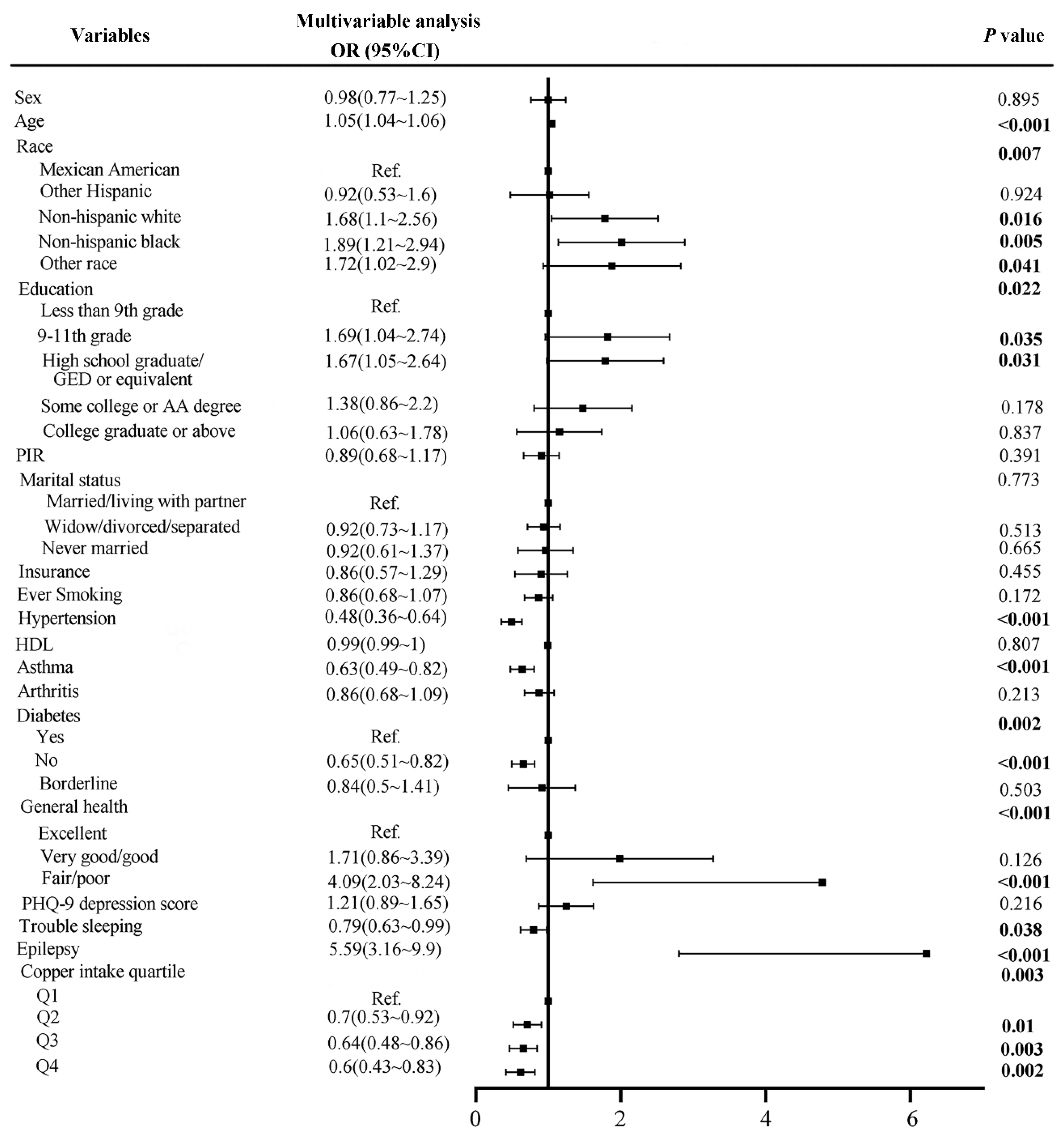
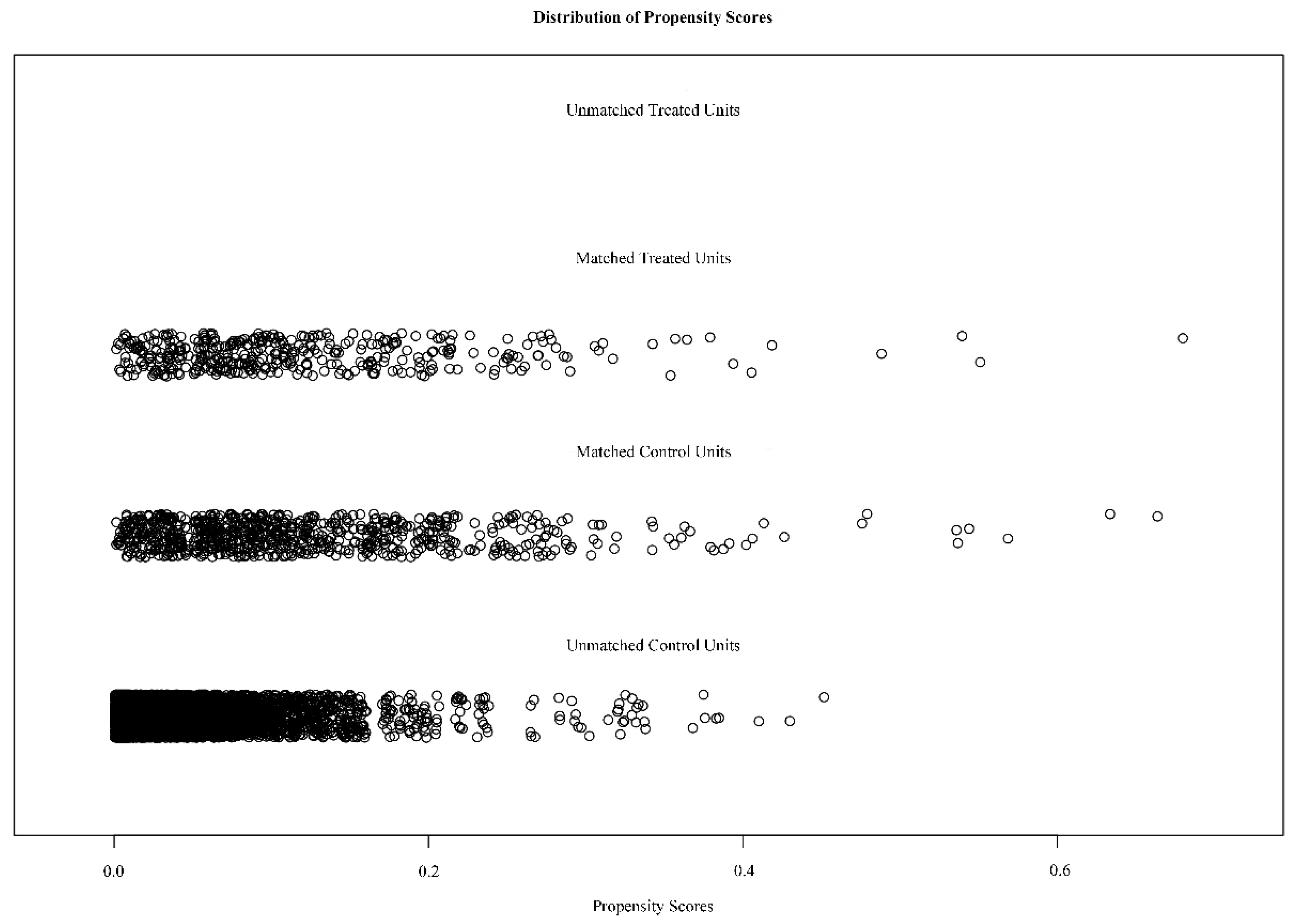
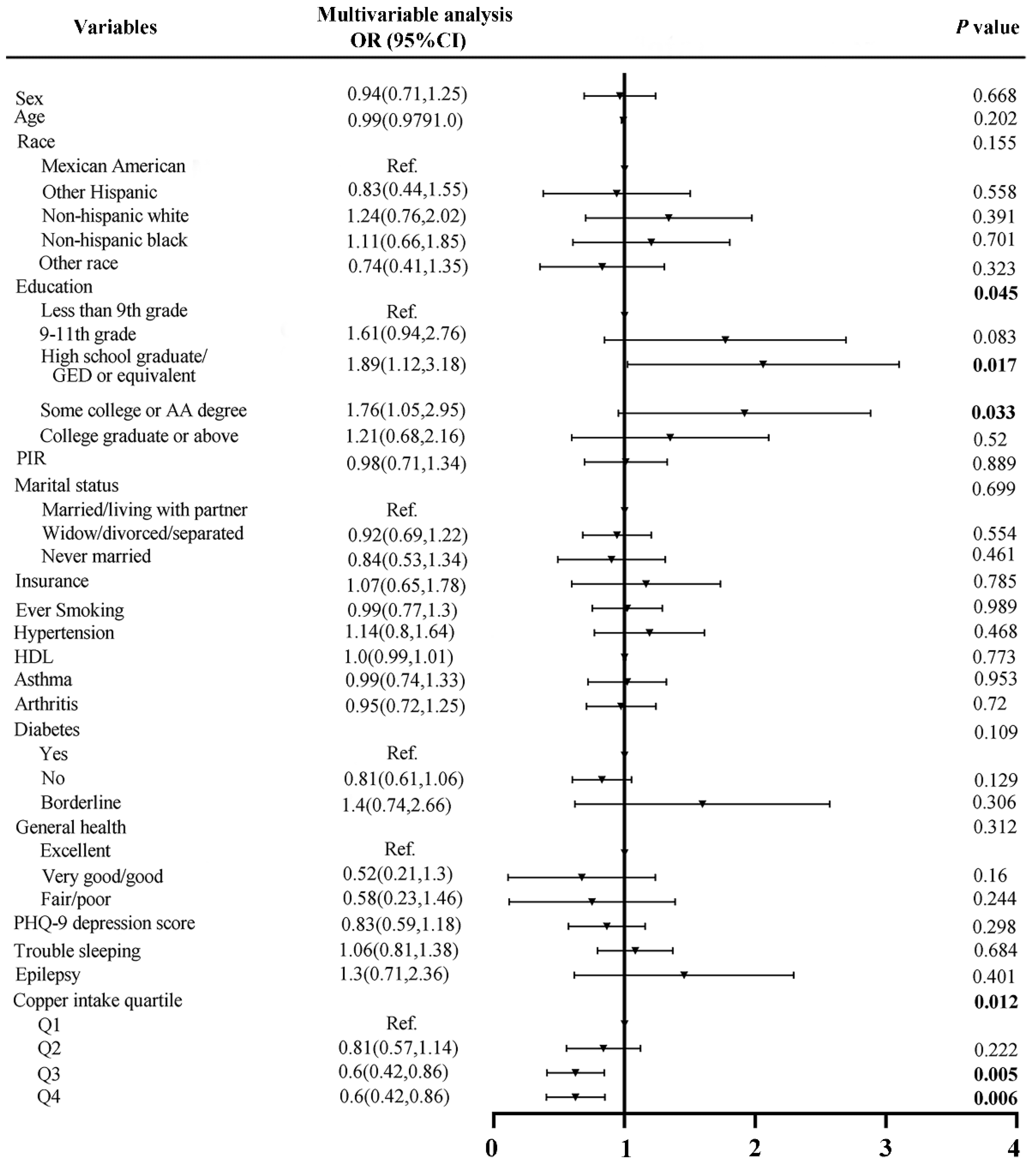
3.2. Analysis of Risk Factors for Stroke before and after Matching
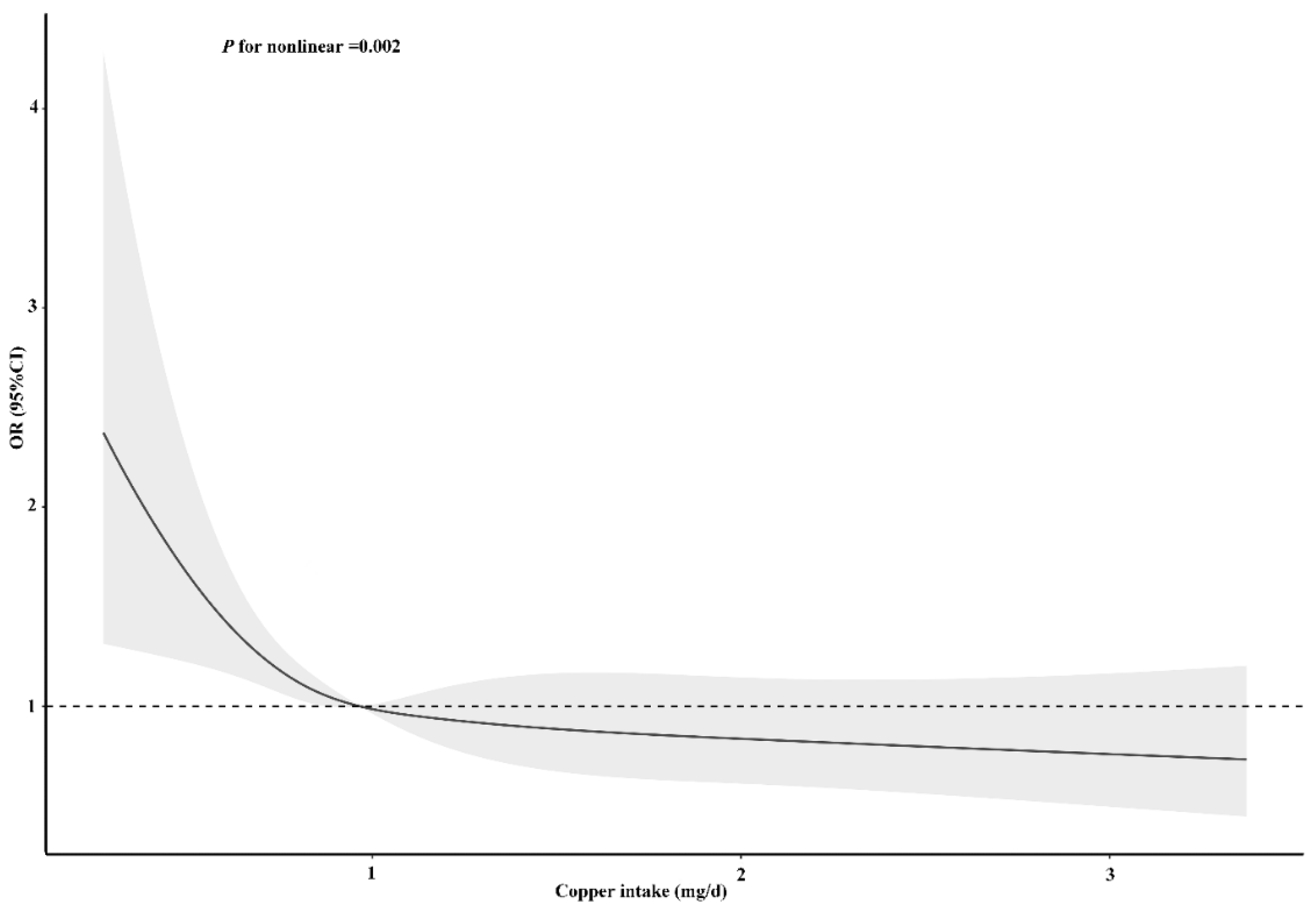
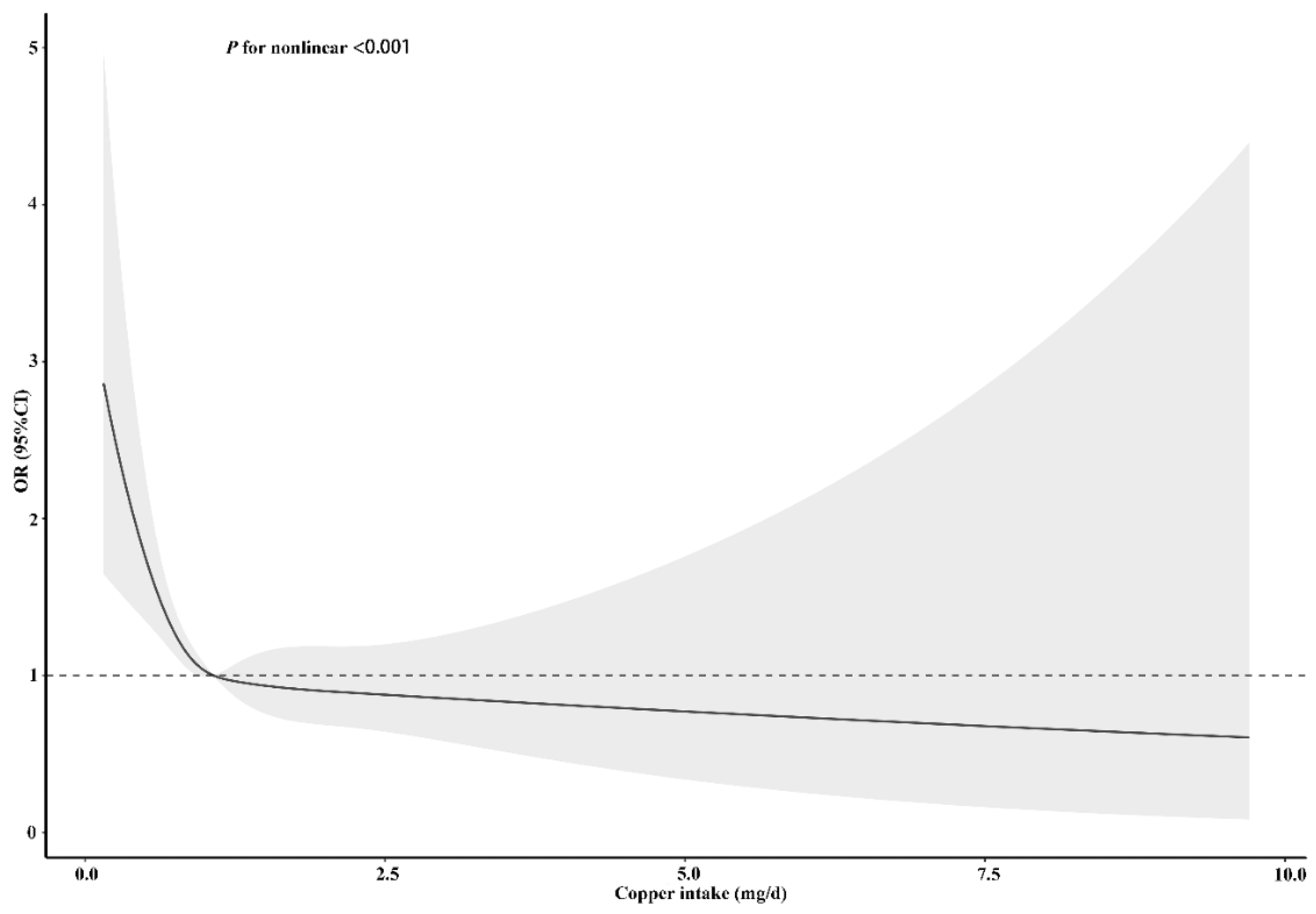
3.3. Nonlinear Association
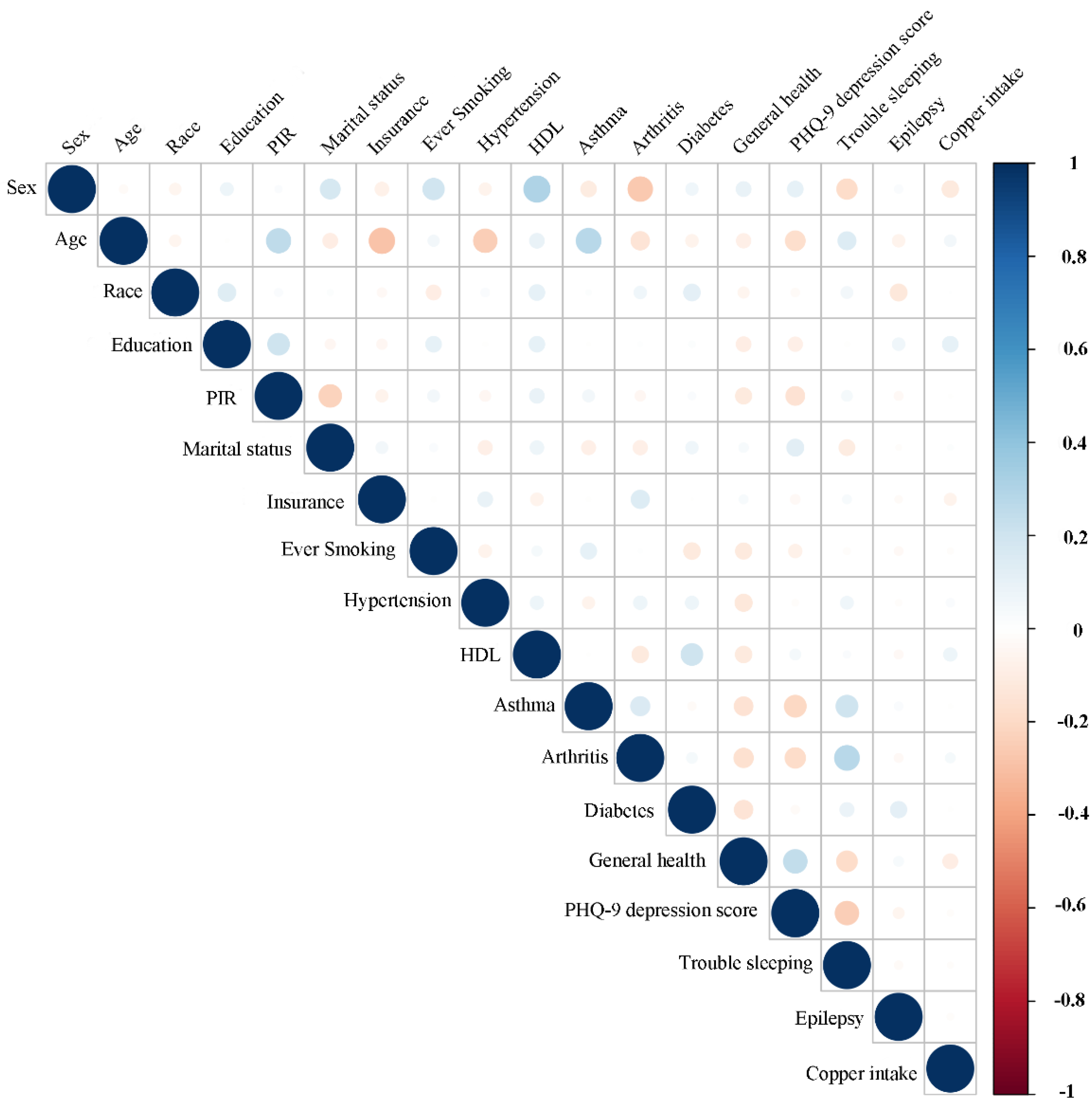
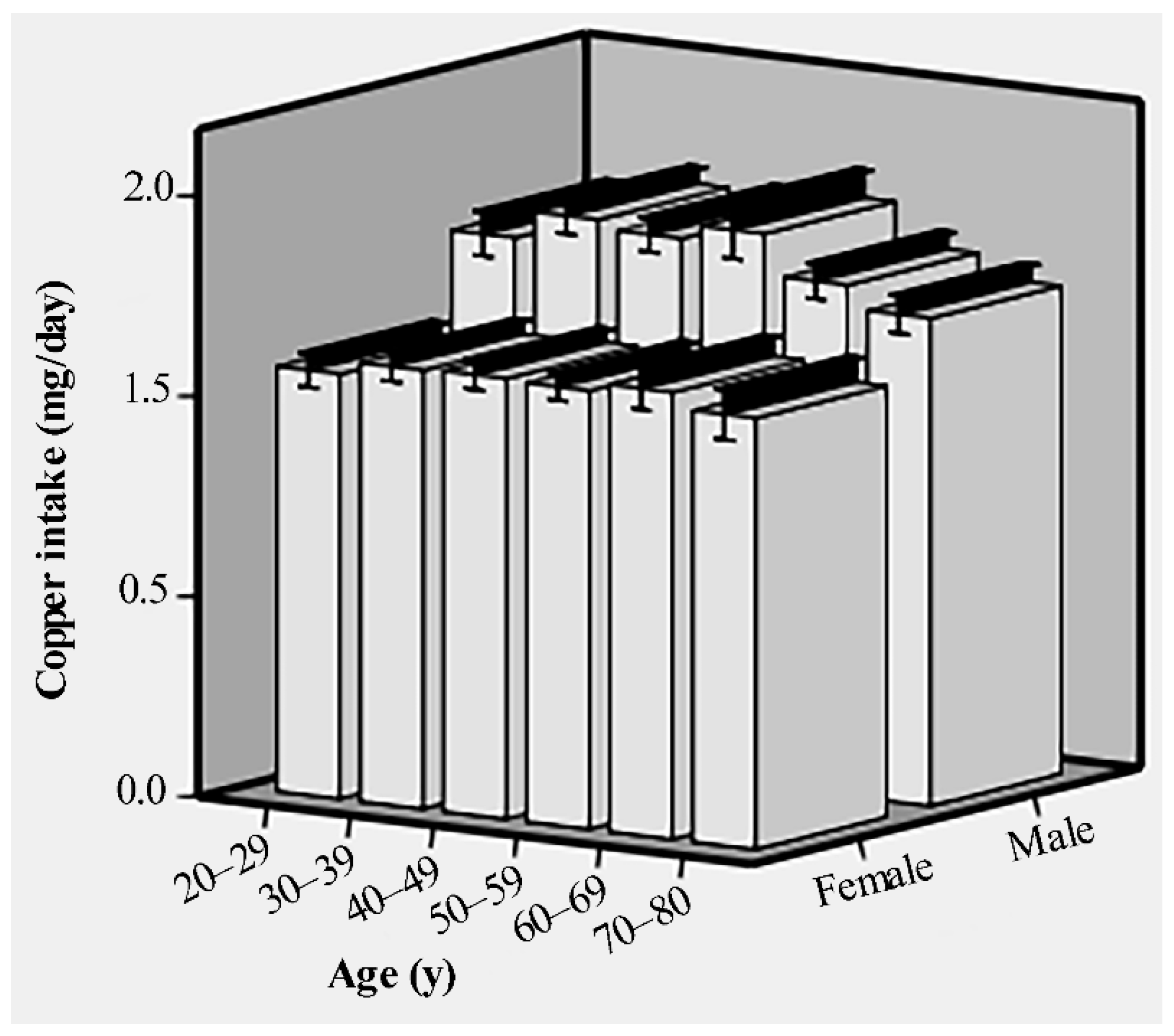
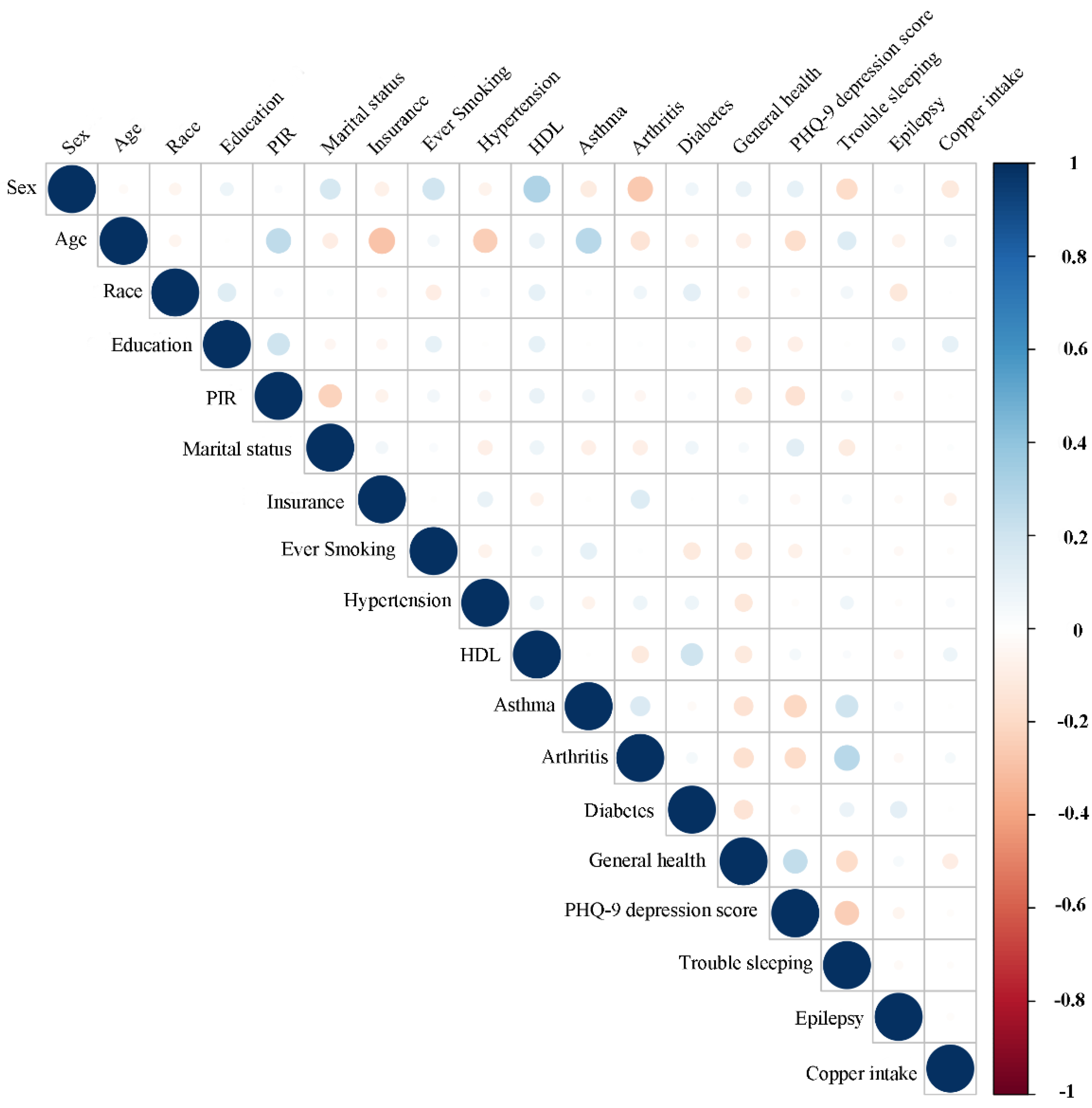
3.4. Associations between Copper Intake and Baseline Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mironczuk, A.; Kapica-Topczewska, K.; Socha, K.; Soroczynska, J.; Jamiolkowski, J.; Kulakowska, A.; Kochanowicz, J. Selenium, Copper, Zinc Concentrations and Cu/Zn, Cu/Se Molar Ratios in the Serum of Patients with Acute Ischemic Stroke in Northeastern Poland-A New Insight into Stroke Pathophysiology. Nutrients 2021, 13, 2139. [Google Scholar] [CrossRef] [PubMed]
- Mai, X.; Liang, X. Risk Factors for Stroke Based on the National Health and Nutrition Examination Survey. J. Nutr. Health Aging 2020, 24, 791–795. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.W.; Chi, W.C.; Chang, K.H.; Yen, C.F.; Liao, H.F.; Escorpizo, R.; Liou, T.-H. World health organization disability assessment schedule 2.0 as an objective assessment tool for predicting return to work after a stroke. Disabil. Rehabil. 2017, 40, 2592–2597. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Xu, G.; Fang, J. Association Between Serum Copper and Stroke Risk Factors in Adults: Evidence from the National Health and Nutrition Examination Survey, 2011–2016. Biol. Trace Elem. Res. 2021, 1–6. [Google Scholar] [CrossRef]
- Ackerman, C.M.; Chang, C.J. Copper signaling in the brain and beyond. J. Biol. Chem. 2018, 293, 4628–4635. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.; Bi, C.; Lin, T.; Liu, L.; Song, Y.; Wang, P.; Wang, B.; Fang, C.; Ma, H.; Huang, X.; et al. Association between plasma copper levels and first stroke: A community-based nested case-control study. Nutr. Neurosci. 2021, 1–10. [Google Scholar] [CrossRef]
- Scheiber, I.F.; Mercer, J.F.; Dringen, R. Metabolism and functions of copper in brain. Prog. Neurobiol. 2014, 116, 33–57. [Google Scholar] [CrossRef]
- Witt, B.; Schaumloffel, D.; Schwerdtle, T. Subcellular Localization of Copper-Cellular Bioimaging with Focus on Neurological Disorders. Int. J. Mol. Sci. 2020, 21, 2341. [Google Scholar] [CrossRef] [Green Version]
- Bagheri, B.; Akbari, N.; Tabiban, S.; Habibi, V.; Mokhberi, V. Serum level of copper in patients with coronary artery disease. Niger. Med. J. 2015, 56, 39–42. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Cao, J.; Zhang, H.; Jiang, C.; Lin, T.; Zhou, Z.; Song, Y.; Li, Y.; Liu, C.; Liu, L.; et al. Plasma copper and the risk of first stroke in hypertensive patients: A nested case-control study. Am. J. Clin. Nutr. 2019, 110, 212–220. [Google Scholar] [CrossRef]
- Xiao, Y.; Yuan, Y.; Liu, Y.; Yu, Y.; Jia, N.; Zhou, L.; Wang, H.; Huang, S.; Zhang, Y.; Yang, H.; et al. Circulating Multiple Metals and Incident Stroke in Chinese Adults. Stroke 2019, 50, 1661–1668. [Google Scholar] [CrossRef]
- Karadas, S.; Sayın, R.; Aslan, M.; Gonullu, H.; Katı, C.; Dursun, R.; Duran, L.; Gonullu, E.; Demir, H. Serum levels of trace elements and heavy metals in patients with acute hemorrhagic stroke. J. Membr. Biol. 2014, 247, 175–180. [Google Scholar] [CrossRef]
- Jiang, Y.; Wang, L.-P.; Dong, X.-H.; Cai, J.; Jiang, G.-J.; Zhang, C.; Xie, H.-H. Trace Amounts of Copper in Drinking Water Aggravate Cerebral Ischemic Injury via Impairing Endothelial Progenitor Cells in Mice. CNS Neurosci. Ther. 2015, 21, 677–680. [Google Scholar] [CrossRef] [PubMed]
- Juul, F.; Parekh, N.; Martinez-Steele, E.; Monteiro, C.A.; Chang, V.W. Ultra-processed food consumption among US adults from 2001 to 2018. Am. J. Clin. Nutr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mei, Z.; Addo, O.Y.; Jefferds, M.E.; Sharma, A.J.; Flores-Ayala, R.C.; Brittenham, G.M. Physiologically based serum ferritin thresholds for iron deficiency in children and non-pregnant women: A US National Health and Nutrition Examination Surveys (NHANES) serial cross-sectional study. Lancet Haematol. 2021, 8, e572–e582. [Google Scholar] [CrossRef]
- Li, S.; Sun, W.; Zhang, D. Association of Zinc, Iron, Copper, and Selenium Intakes with Low Cognitive Performance in Older Adults: A Cross-Sectional Study from National Health and Nutrition Examination Survey (NHANES). J. Alzheimers Dis. 2019, 72, 1145–1157. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, S.; Sanika, G.H.A.; Zhao, J.; Zhang, H.; Zhao, L.; Wang, W. Association between Serum 25-Hydroxyvitamin D Level and Stroke Risk: An Analysis Based on the National Health and Nutrition Examination Survey. Behav. Neurol. 2021, 2021, 5457881. [Google Scholar] [CrossRef]
- Al-Ibrahim, A.A.; Jackson, R.T. Healthy eating index versus alternate healthy index in relation to diabetes status and health markers in U.S. adults: NHANES 2007-2010. Nutr. J. 2019, 18, 26. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Yu, B.; Zhang, X.; Wang, C.; Sun, M.; Jin, L.; Liu, X. Trends in depression among Adults in the United States, NHANES 2005-2016. J. Affect. Disord. 2020, 263, 609–620. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Wang, Y.; Chen, X.; Zhang, C.; Chen, J.; Cheng, H.; Zhang, L. Risk Factors for Epilepsy: A National Cross-Sectional Study from National Health and Nutrition Examination Survey 2013 to 2018. Int. J. Gen. Med. 2021, 14, 4405–4411. [Google Scholar] [CrossRef] [PubMed]
- Semenov, Y.R.; Herbosa, C.M.; Rogers, A.T.; Huang, A.; Kwatra, S.G.; Cohen, B.; Anadkat, M.J.; Silverberg, J.I. Psoriasis and mortality in the United States: Data from the National Health and Nutrition Examination Survey. J. Am. Acad. Dermatol. 2021, 85, 396–403. [Google Scholar] [CrossRef]
- Cho, S.-M.; Mehaffey, J.H.; Meyers, S.L.; Cantor, R.S.; Starling, R.C.; Kirklin, J.K.; Jacobs, J.P.; Kern, J.; Uchino, K.; Yarboro, L.T. Cerebrovascular Events in Patients With Centrifugal-Flow Left Ventricular Assist Devices: Propensity Score-Matched Analysis From the Intermacs Registry. Circulation 2021, 144, 763–772. [Google Scholar] [CrossRef]
- Kaster, T.S.; Vigod, S.N.; Gomes, T.; Sutradhar, R.; Wijeysundera, D.N.; Blumberger, D.M. Risk of serious medical events in patients with depression treated with electroconvulsive therapy: A propensity score-matched, retrospective cohort study. Lancet Psychiatry 2021, 8, 686–695. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The Central Role of the Propensity Score in Observational Studies for Causal Effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Desquilbet, L.; Mariotti, F. Dose-response analyses using restricted cubic spline functions in public health research. Stat. Med. 2010, 29, 1037–1057. [Google Scholar] [CrossRef]
- Lee, D.H.; Keum, N.; Hu, F.B.; Orav, E.J.; Rimm, E.B.; Willett, W.C.; Giovannucci, E.L. Predicted lean body mass, fat mass, and all cause and cause specific mortality in men: Prospective US cohort study. BMJ 2018, 362, k2575. [Google Scholar] [CrossRef] [Green Version]
- Dong, X.; Li, S.; Sun, J.; Li, Y.; Zhang, D. Association of Coffee, Decaffeinated Coffee and Caffeine Intake from Coffee with Cognitive Performance in Older Adults: National Health and Nutrition Examination Survey (NHANES) 2011-2014. Nutrients 2020, 12, 840. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Li, W.; Wang, Y.; Wang, T.; Ma, M.; Tian, C. Association Between the Change of Serum Copper and Ischemic Stroke: A Systematic Review and Meta-Analysis. J. Mol. Neurosci. 2019, 70, 475–480. [Google Scholar] [CrossRef]
- Wells, E.M.; Navas-Acien, A.; Apelberg, B.J.; Herbstman, J.B.; Jarrett, J.M.; Lin, Y.H.; Verdon, C.P.; Ward, C.; Caldwell, K.L.; Hibbeln, J.R.; et al. Association of selenium and copper with lipids in umbilical cord blood. J. Dev. Orig. Health Dis. 2014, 5, 281–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klevay, L.M. Cardiovascular disease from copper deficiency—A history. J. Nutr. 2000, 130 (Suppl. S2), 489S–492S. [Google Scholar] [CrossRef]
- Reunanen, A.; Knekt, P.; Marniemi, J.; Maki, J.; Maatela, J.; Aromaa, A. Serum calcium, magnesium, copper and zinc and risk of cardiovascular death. Eur. J. Clin. Nutr. 1996, 50, 431–437. [Google Scholar] [PubMed]
- Festa, R.A.; Thiele, D.J. Copper: An essential metal in biology. Curr. Biol. 2011, 21, R877–R883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salonen, J.T.; Salonen, R.; Korpela, H.; Suntioinen, S.; Tuomilehto, J. Serum copper and the risk of acute myocardial infarction: A prospective population study in men in eastern Finland. Am. J. Epidemiol. 1991, 134, 268–276. [Google Scholar] [CrossRef] [Green Version]
- Lamb, D.J.; Avades, T.Y.; Ferns, G.A. Biphasic modulation of atherosclerosis induced by graded dietary copper supplementation in the cholesterol-fed rabbit. Int. J. Exp. Pathol. 2008, 82, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Bost, M.; Houdart, S.; Oberli, M.; Kalonji, E.; Huneau, J.F.; Margaritis, I. Dietary copper and human health: Current evidence and unresolved issues. J. Trace Elem. Med. Biol. 2016, 35, 107–115. [Google Scholar] [CrossRef]
- Knuppel, S.; Norman, K.; Boeing, H. Is a Single 24-hour Dietary Recall per Person Sufficient to Estimate the Population Distribution of Usual Dietary Intake? J. Nutr. 2019, 149, 1491–1492. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Subjects (N = 10,550) | Copper Intake Quartile, mg/day | |||
|---|---|---|---|---|---|
| Q1 (<0.799) | Q2 (≥0.799 to <1.072) | Q3 (≥1.072 to <1.42) | Q4 (≥1.42) | ||
| Sex (%) | |||||
| Male | 5036 (47.7) | 932 (35.4) | 1156 (43.8) | 1325 (50.3) | 1623 (61.5) |
| Female | 5514 (52.3) | 1703 (64.6) | 1483 (56.2) | 1310 (49.7) | 1018 (38.5) |
| Age (y), Mean (SD) | 50 (17.35) | 50.07 (17.99) | 50.57 (17.8) | 50.22 (17.11) | 49.14 (16.43) |
| Race (%) | |||||
| Mexican American | 1452 (13.8) | 278 (10.6) | 402 (15.2) | 386 (14.6) | 386 (14.6) |
| Other Hispanic | 1040 (9.9) | 279 (10.6) | 250 (9.5) | 250 (9.5) | 261 (9.9) |
| Non-hispanic white | 4374 (41.5) | 1012 (38.4) | 1144 (43.3) | 1123 (42.6) | 1095 (41.5) |
| Non-hispanic black | 2183 (20.7) | 809 (30.7) | 538 (20.4) | 490 (18.6) | 346 (13.1) |
| Other race | 1501 (14.2) | 257 (9.8) | 305 (11.6) | 386 (14.6) | 553 (20.9) |
| Education (%) | |||||
| Less than 9th grade | 695 (6.6) | 222 (8.4) | 186 (7.0) | 167 (6.3) | 120 (4.5) |
| 9–11th grade | 1177 (11.2) | 390 (14.8) | 319 (12.1) | 244 (9.3) | 224 (8.5) |
| High school graduate/GED or equivalent | 2441 (23.1) | 777 (29.5) | 652 (24.7) | 554 (21) | 458 (17.3) |
| Some college or AA degree | 3425 (32.5) | 880 (33.4) | 863 (32.7) | 867 (32.9) | 815 (30.9) |
| College graduate or above | 2812 (26.7) | 366 (13.9) | 619 (23.5) | 803 (30.5) | 1024 (38.8) |
| PIR (%) | |||||
| <1 | 2036 (19.3) | 741 (28.1) | 509 (19.3) | 432 (16.4) | 354 (13.4) |
| ≥1 | 8514 (80.7) | 1894 (71.9) | 2130 (80.7) | 2203 (83.6) | 2287 (86.6) |
| Marital status (%) | |||||
| Married/living with partner | 6399 (60.7) | 1365 (51.8) | 1575 (59.7) | 1694 (64.3) | 1765 (66.8) |
| Widow/divorced/separated | 2293 (21.7) | 717 (27.2) | 621 (23.5) | 520 (19.7) | 435 (16.5) |
| Never married | 1858 (17.6) | 553 (21) | 443 (16.8) | 421 (16) | 441 (16.7) |
| Insurance (%) | |||||
| Yes | 8789 (83.3) | 2146 (84.4) | 2184 (82.8) | 2192 (83.2) | 2267 (85.8) |
| No | 1761 (16.7) | 489 (18.6) | 455 (17.2) | 443 (16.8) | 374 (14.2) |
| Ever Smoking (%) | |||||
| Yes | 4574 (43.4) | 1261 (47.9) | 1139 (43.2) | 1109 (42.1) | 1065 (40.3) |
| no | 5976 (56.6) | 1374 (52.1) | 1500 (56.8) | 1526 (57.9) | 1576 (59.7) |
| Hypertension (%) | |||||
| Yes | 4700 (44.5) | 1257 (47.7) | 1214 (46) | 1152 (43.7) | 1077 (40.8) |
| No | 5850 (55.5) | 1378 (52.3) | 1425 (54) | 1483 (56.3) | 1564 (59.2) |
| HDL (mg/dL), Mean (SD) | 53.36 (16.35) | 53.43 (16.47) | 53.30 (16.35) | 53.51 (16.36) | 53.21 (16.21) |
| Asthma (%) | |||||
| Yes | 1650 (15.6) | 514 (19.5) | 404 (15.3) | 361 (13.7) | 371 (14) |
| No | 8900 (84.4) | 2121 (80.5) | 2235 (84.7) | 2274 (86.3) | 2270 (86) |
| Arthritis (%) | |||||
| Yes | 3050 (28.9) | 858 (32.6) | 761 (28.8) | 764 (29) | 667 (25.3) |
| No | 7500 (71.1) | 1777 (67.4) | 1878 (71.2) | 1871 (71) | 1974 (74.7) |
| Stroke (%) | |||||
| Yes | 399 (3.8) | 155 (5.9) | 99 (3.8) | 83 (3.1) | 62 (2.3) |
| No | 10,151 (96.2) | 2480 (94.1) | 2540 (96.2) | 2552 (96.9) | 2579 (97.7) |
| Diabetes (%) | |||||
| Yes | 1602 (15.2) | 443 (16.8) | 441 (16.7) | 389 (14.8) | 329 (12.5) |
| No | 8646 (82) | 2135 (81) | 2121 (80.4) | 2168 (82.3) | 2222 (84.1) |
| Borderline | 302 (2.9) | 57 (2.2) | 77 (2.9) | 78 (3) | 90 (3.4) |
| General health (%) | |||||
| Excellent | 934 (8.9) | 176 (6.7) | 224 (8.5) | 223 (8.5) | 311 (11.8) |
| Very good/good | 7121 (67.5) | 1662 (63.1) | 1760 (66.7) | 1816 (68.9) | 1883 (71.3) |
| Fair/poor | 2495 (23.6) | 797 (30.2) | 655 (24.8) | 596 (22.6) | 447 (16.9) |
| PHQ-9 depression score (%) | |||||
| <10 | 9608 (91.1) | 2297 (87.2) | 2407 (91.2) | 2434 (92.4) | 2469 (93.5) |
| ≥10 | 942 (8.9) | 337 (12.8) | 232 (8.8) | 201 (7.6) | 172 (6.5) |
| Trouble sleeping (%) | |||||
| Yes | 3104 (29.4) | 872 (33.1) | 795 (30.1) | 720 (27.3) | 717 (27.1) |
| No | 7446 (70.6) | 1763 (66.9) | 1844 (69.9) | 1915 (72.7) | 1924 (72.9) |
| Epilepsy (%) | |||||
| No | 10,459 (99.1) | 2603 (98.8) | 2617 (99.2) | 2612 (99.1) | 2627 (99.5) |
| Yes | 91 (0.9) | 32 (1.2) | 22 (0.8) | 23 (0.9) | 14 (0.5) |
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| Variables | Control Group (n = 10,151) | Stroke Group (n = 399) | p | Control Group (n = 798) | Stroke Group (n = 399) | p |
| Sex (%) | 0.509 | 0.967 | ||||
| Male | 4852 (47.8) | 184 (46.1) | 3367 (46) | 184 (46.1) | ||
| Female | 5299 (52.2) | 215 (53.9) | 431 (54) | 215 (53.9) | ||
| Age (y), Mean (SD) | 49.41 (17.25) | 65.01 (12.7) | <0.001 | 65.76 (11.79) | 65.01 (12.7) | 0.309 |
| Race (%) | <0.001 | 0.048 | ||||
| Mexican American | 1419 (14) | 33 (8.3) | 77 (9.6) | 33 (8.3) | ||
| Other Hispanic | 1015 (10) | 25 (6.3) | 71 (8.9) | 25 (6.3) | ||
| Non-hispanic white | 4178 (41.2) | 196 (49.1) | 352 (44.1) | 196 (49.1) | ||
| Non-hispanic black | 2073 (20.4) | 110 (27.6) | 194 (24.3) | 110 (27.6) | ||
| Other race | 1466 (14.4) | 35 (8.8) | 104 (13) | 35 (8.8) | ||
| Education (%) | <0.001 | 0.01 | ||||
| Less than 9th grade | 655 (6.6) | 30 (7.5) | 95 (11.9) | 30 (7.5) | ||
| 9-11th grade | 1110 (10.9) | 67 (16.8) | 123 (15.4) | 67 (16.8) | ||
| High school graduate/GED or equivalent | 2319 (22.8) | 122 (30.6) | 202 (25.3) | 122 (30.6) | ||
| Some college or AA degree | 3302 (32.5) | 123 (30.8) | 221 (27.7) | 123 (30.8) | ||
| College graduate or above | 2755 (27.1) | 57 (14.3) | 157 (19.7) | 57 (14.3) | ||
| PIR (%) | 0.014 | 0.773 | ||||
| <1 | 1940 (19.1) | 96 (24.1) | 186 (23.3) | 96 (24.1) | ||
| ≥1 | 8211 (80.9) | 303 (75.9) | 612 (76.7) | 303 (75.9) | ||
| Marital status (%) | <0.001 | 0.934 | ||||
| Married/living with partner | 6178 (60.9) | 221 (55.4) | 433 (54.3) | 221 (55.4) | ||
| Widow/divorced/separated | 2150 (21.2) | 143 (35.8) | 293 (36.7) | 143 (35.8) | ||
| Never married | 1823 (18) | 35 (8.8) | 72 (9) | 35 (8.8) | ||
| Insurance (%) | <0.001 | 0.631 | ||||
| Yes | 8420 (82.9) | 369 (92.5) | 744 (93.2) | 369 (92.5) | ||
| No | 1731 (17.1) | 30 (7.5) | 54 (6.8) | 30 (7.5) | ||
| Ever Smoking (%) | <0.001 | 0.563 | ||||
| Yes | 4341 (42.8) | 233 (58.4) | 452 (56.6) | 233 (58.4) | ||
| no | 5810 (57.2) | 166 (41.6) | 346 (43.4) | 166 (41.6) | ||
| Hypertension (%) | <0.001 | |||||
| Yes | 4371 (43.1) | 329 (82.5) | 670 (84) | 329 (82.5) | ||
| No | 5780 (56.9) | 70 (17.5) | 128 (16) | 70 (17.5) | ||
| HDL (mg/dL) Mean (SD) | 53.38 (16.34) | 52.82 (16.5) | 0.503 | 53.14 (16.27) | 52.82 (16.5) | 0.751 |
| Asthma (%) | <0.001 | 0.741 | ||||
| Yes | 1548 (15.2) | 102 (25.6) | 197 (24.7) | 102 (25.6) | ||
| No | 8603 (84.8) | 297 (74.4) | 601 (75.3) | 297 (74.4) | ||
| Arthritis (%) | <0.001 | 0.741 | ||||
| Yes | 2818 (27.8) | 232 (58.1) | 456 (57.1) | 232 (58.1) | ||
| No | 7333 (72.2) | 167 (41.9) | 342 (42.9) | 167 (41.9) | ||
| Diabetes (%) | <0.001 | 0.194 | ||||
| Yes | 1451 (14.3) | 151 (37.8) | 277 (34.7) | 151 (37.8) | ||
| No | 8417 (82.9) | 229 (57.4) | 495 (62) | 229 (57.4) | ||
| Borderline | 283 (2.8) | 19 (4.8) | 26 (3.3) | 19 (4.8) | ||
| General health (%) | <0.001 | 0.473 | ||||
| Excellent | 925 (9.1) | 9 (2.3) | 12 (1.5) | 9 (2.3) | ||
| Very good/good | 6942 (68.4) | 179 (44.9) | 380 (47.6) | 179 (44.9) | ||
| Fair/poor | 2284 (22.5) | 211 (52.9) | 406 (50.9) | 211 (52.9) | ||
| PHQ-9 depression score (%) | <0.001 | 0.504 | ||||
| <10 | 9283 (91.4) | 325 (81.5) | 637 (79.8) | 325 (81.5) | ||
| ≥10 | 868 (8.6) | 74 (18.5) | 161 (20.2) | 74 (18.5) | ||
| Trouble Sleeping (%) | <0.001 | 0.682 | ||||
| Yes | 2909 (28.7) | 195 (48.9) | 380 (47.6) | 195 (48.9) | ||
| No | 7242 (71.3) | 204 (51.1) | 418 (52.4) | 204 (51.1) | ||
| Epilepsy (%) | <0.001 | 0.257 | ||||
| No | 10080 (99.3) | 379 (95) | 769 (96.4) | 379 (95) | ||
| Yes | 71 (0.7) | 20 (5) | 29 (3.6) | 20 (5) | ||
| Copper intake quartile (%) | <0.001 | 0.007 | ||||
| Q1 | 2480 (24.4) | 155 (38.8) | 178 (22.3) | 121 (30.3) | ||
| Q2 | 2540 (25) | 99 (24.8) | 195 (24.4) | 104 (26.1) | ||
| Q3 | 2552 (25.1) | 83 (20.8) | 211 (26.4) | 88 (22.1) | ||
| Q4 | 2579 (25.4) | 62 (15.5) | 214 (26.8) | 86 (21.6) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, L.; Chen, X.; Cheng, H.; Zhang, L. Dietary Copper Intake and Risk of Stroke in Adults: A Case-Control Study Based on National Health and Nutrition Examination Survey 2013–2018. Nutrients 2022, 14, 409. https://doi.org/10.3390/nu14030409
Yang L, Chen X, Cheng H, Zhang L. Dietary Copper Intake and Risk of Stroke in Adults: A Case-Control Study Based on National Health and Nutrition Examination Survey 2013–2018. Nutrients. 2022; 14(3):409. https://doi.org/10.3390/nu14030409
Chicago/Turabian StyleYang, Lixiang, Xun Chen, Huilin Cheng, and Lihua Zhang. 2022. "Dietary Copper Intake and Risk of Stroke in Adults: A Case-Control Study Based on National Health and Nutrition Examination Survey 2013–2018" Nutrients 14, no. 3: 409. https://doi.org/10.3390/nu14030409
APA StyleYang, L., Chen, X., Cheng, H., & Zhang, L. (2022). Dietary Copper Intake and Risk of Stroke in Adults: A Case-Control Study Based on National Health and Nutrition Examination Survey 2013–2018. Nutrients, 14(3), 409. https://doi.org/10.3390/nu14030409