
Correlation between 25-hydroxyvitamin D/D3 Deficiency and COVID-19 Disease Severity in Adults from Northern Colorado

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
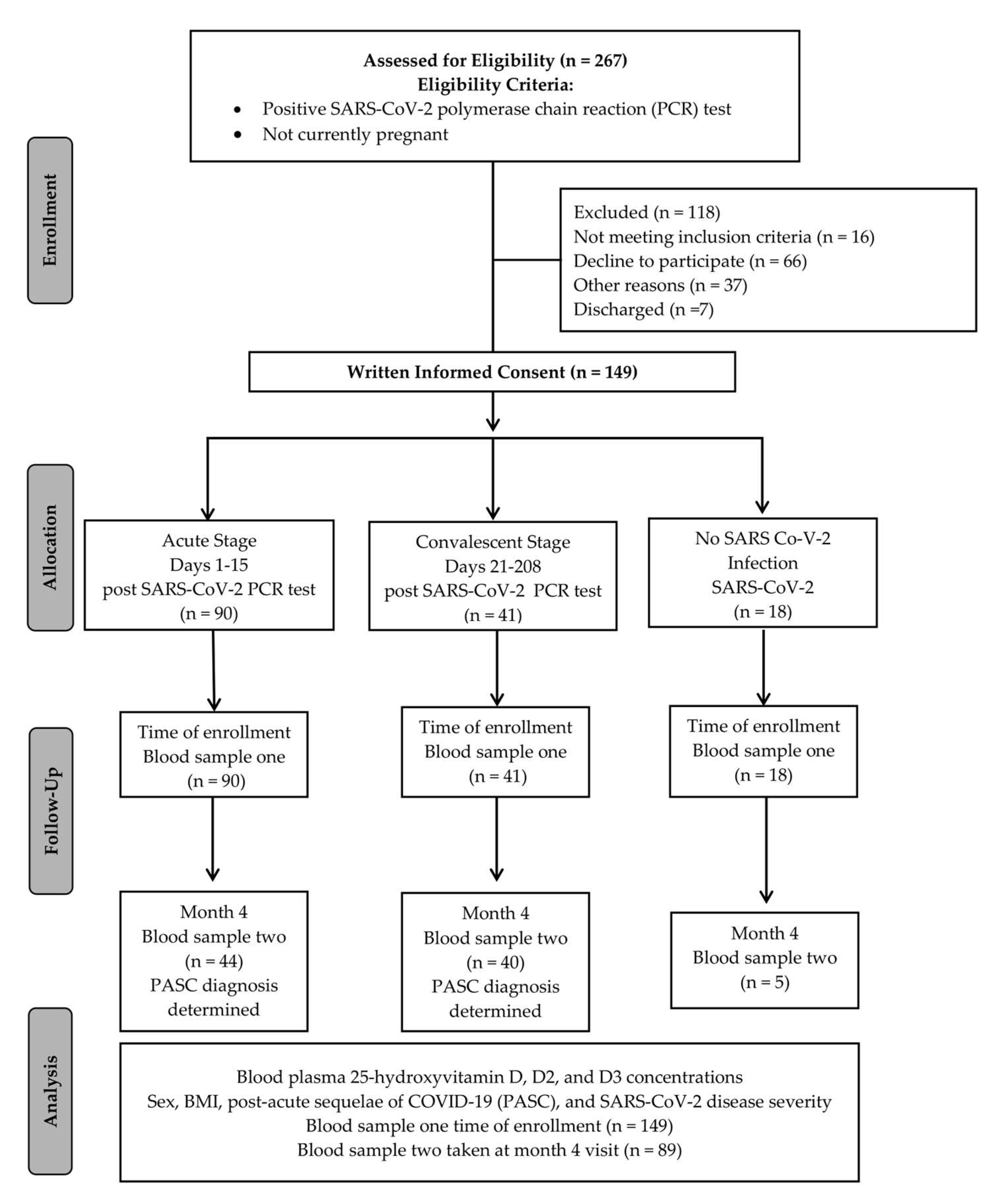
2.1. Study Design
2.2. Participants
2.3. Biospecimen Collection
2.4. Materials
2.5. Preparation of Calibration Standards
2.6. Preparation of Standards and Samples
2.7. LC-MS
2.8. Data Analysis
2.9. Statistical Analysis
3. Results
3.1. Participant and Longitudinal Biorepository Cohort Demographics
3.2. 25-hydroxyvitamin D and D3 Differences by Sex at Time of Enrollment
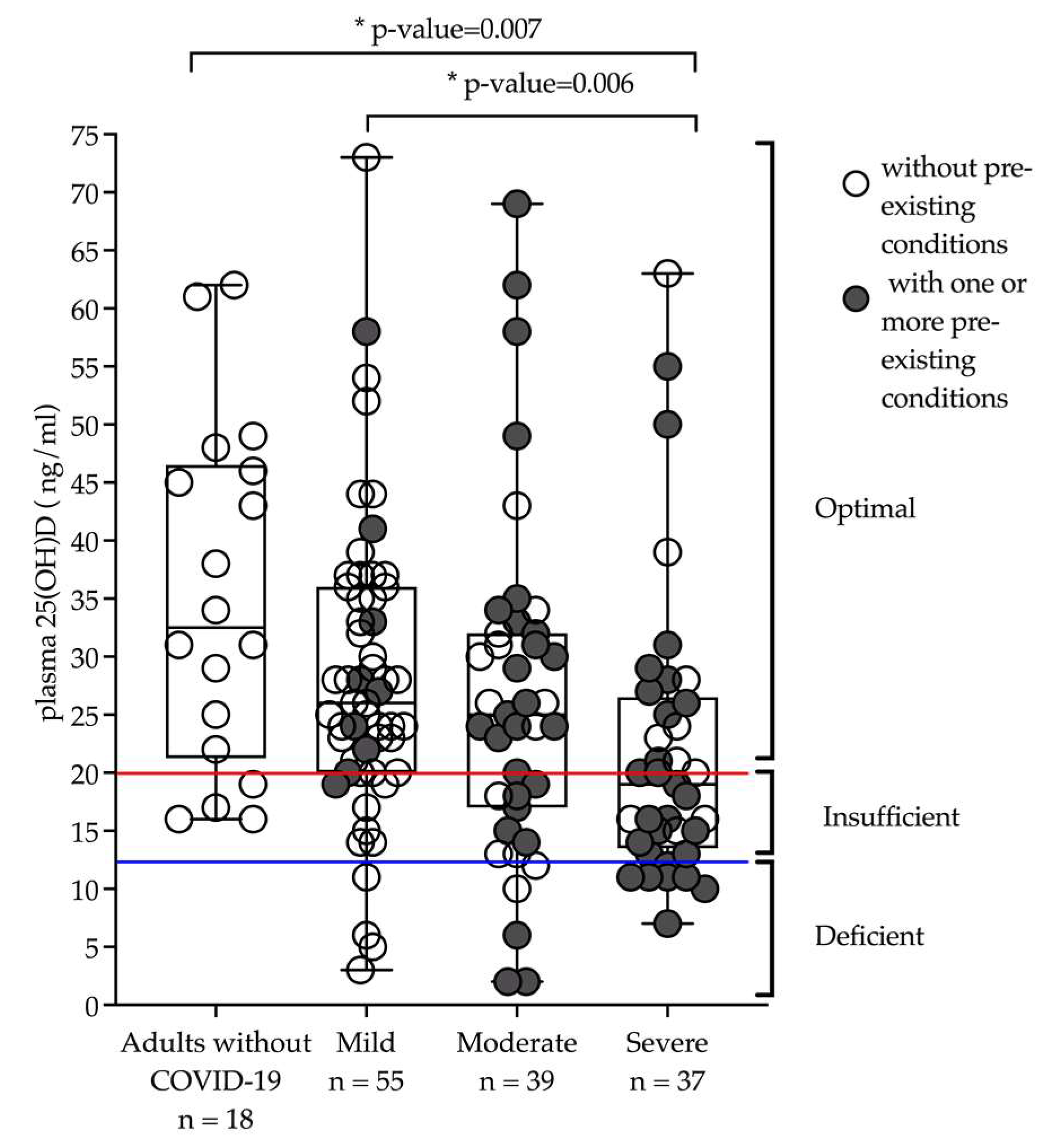
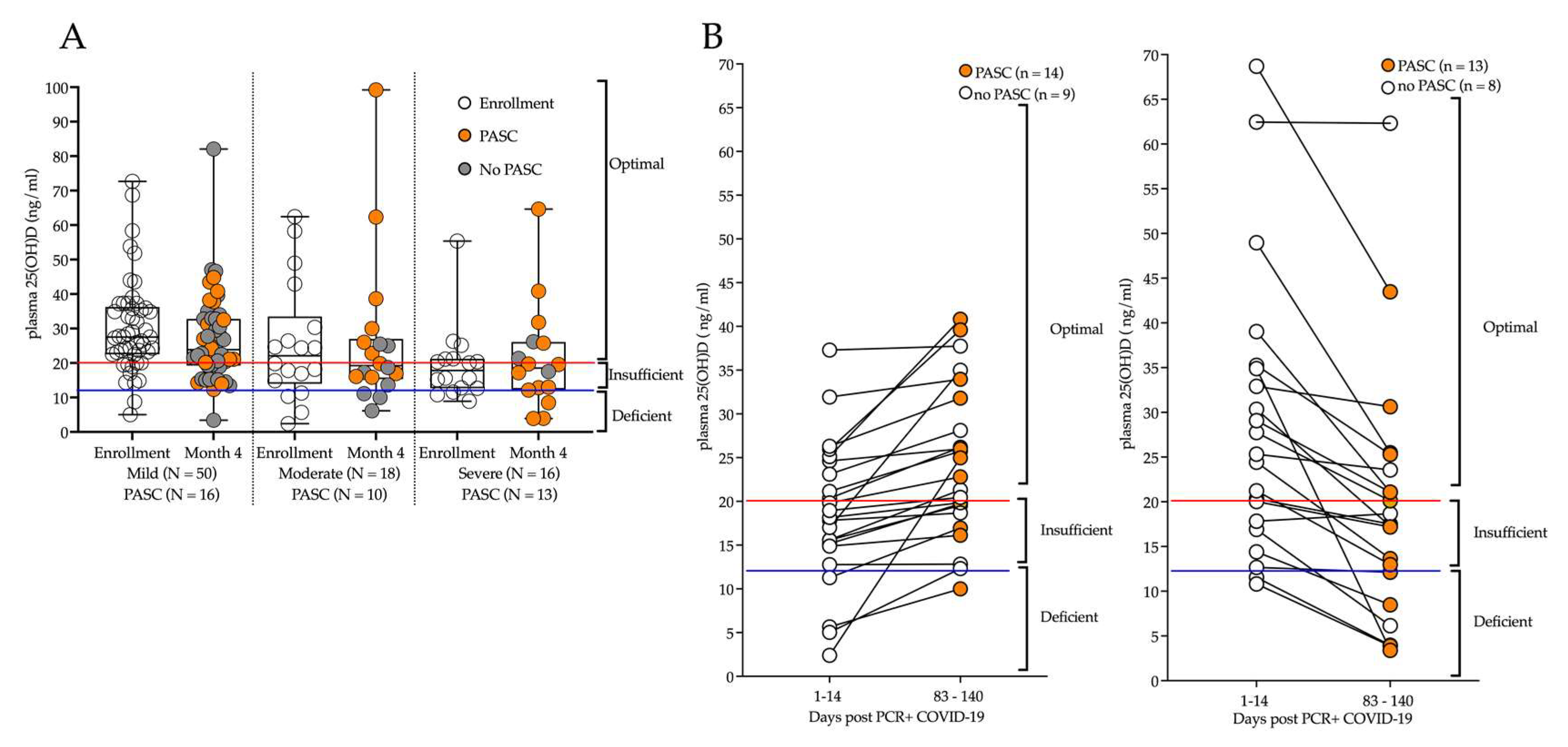
3.3. 25-hydroxyvitamin D and D3 by Disease Severity and PASC
3.4. 25-hydroxyvitamin D and D3 Differences by Body Mass Index
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; The National Academies Collection: Reports funded by National Institutes of Health; National Academies Press: Washington, DC, USA, 2011. Available online: http://www.ncbi.nlm.nih.gov/books/NBK56070/ (accessed on 23 June 2022).
- Edward, J.; Macdonald, I.; Zeisel, S. Present Knowledge in Nutrition, 10th ed.; Wiley: Washington, DC, USA, 2012. [Google Scholar]
- Prietl, B.; Treiber, G.; Pieber, T.R.; Amrein, K. Vitamin D and immune function. Nutrients 2013, 5, 2502–2521. [Google Scholar] [CrossRef]
- Park, J.E.; Pichiah, P.B.T.; Cha, Y.-S. Vitamin D and Metabolic Diseases: Growing Roles of Vitamin D. J. Obes. Metab. Syndr. 2018, 27, 223–232. [Google Scholar] [CrossRef]
- Bishop, E.L.; Ismailova, A.; Dimeloe, S.; Hewison, M.; White, J.H. Vitamin D and Immune Regulation: Antibacterial, Antiviral, Anti-Inflammatory. JBMR Plus 2021, 5, e10405. [Google Scholar] [CrossRef]
- Looker, A.C.; Schleicher, R.L. Vitamin D Status: United States, 2001–2006. NCHS Data Brief 2011, 59, 1–8. [Google Scholar]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.; Bianchi, M.L.; Stepan, J.; El-Hajj Fuleihan, G.; Bouillon, R. Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency: A position statement of the European Calcified Tissue Society. Eur. J. Endocrinol. 2019, 180, P23–P54. [Google Scholar] [CrossRef]
- Zdrenghea, M.T.; Makrinioti, H.; Bagacean, C.; Bush, A.; Johnston, S.L.; Stanciu, L.A. Vitamin D modulation of innate immune responses to respiratory viral infections. Rev. Med. Virol. 2017, 27, e1909. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, J.; Ge, X.; Du, J.; Deb, D.K.; Li, Y.C. Vitamin D receptor inhibits nuclear factor κB activation by interacting with IκB kinase β protein. J. Biol. Chem. 2013, 288, 19450–19458. [Google Scholar] [CrossRef]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef]
- Rybchyn, M.S.; Abboud, M.; Puglisi, D.A.; Gordon-Thomson, C.; Brennan-Speranza, T.C.; Mason, R.S.; Fraser, D.R. Skeletal Muscle and the Maintenance of Vitamin D Status. Nutrients 2020, 12, 3270. [Google Scholar] [CrossRef]
- Scherer, P.E.; Kirwan, J.P.; Rosen, C.J. Post-acute sequelae of COVID-19: A metabolic perspective. eLife 2022, 11, e78200. [Google Scholar] [CrossRef]
- Hars, M.; Mendes, A.; Serratrice, C.; Herrmann, F.R.; Gold, G.; Graf, C.; Zekry, D.; Trombetti, A. Sex-specific association between vitamin D deficiency and COVID-19 mortality in older patients. Osteoporos. Int. 2020, 31, 2495–2496. [Google Scholar] [CrossRef]
- Laires, P.A.; Nunes, C. Population-based Estimates for High Risk of Severe COVID-19 Disease due to Age and Underlying Health Conditions. Acta Med. Port. 2020, 33, 720–725. [Google Scholar] [CrossRef]
- LaVergne, S.M.; Stromberg, S.; Baxter, B.A.; Webb, T.L.; Dutt, T.S.; Berry, K.; Tipton, M.; Haberman, J.; Massey, B.R.; McFann, K.; et al. A longitudinal SARS-CoV-2 biorepository for COVID-19 survivors with and without post-acute sequelae. BMC Infect. Dis. 2021, 21, 677. [Google Scholar] [CrossRef]
- Lucas, C.; Wong, P.; Klein, J.; Castro, T.B.R.; Silva, J.; Sundaram, M.; Ellingson, M.K.; Mao, T.; Oh, J.E.; Israelow, B.; et al. Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature 2020, 584, 463–469. [Google Scholar] [CrossRef]
- McFann, K.; Baxter, B.A.; LaVergne, S.M.; Stromberg, S.; Berry, K.; Tipton, M.; Haberman, J.; Ladd, J.; Webb, T.L.; Dunn, J.A.; et al. Quality of Life (QoL) Is Reduced in Those with Severe COVID-19 Disease, Post-Acute Sequelae of COVID-19, and Hospitalization in United States Adults from Northern Colorado. Int. J. Environ. Res. Public Health 2021, 18, 11048. [Google Scholar] [CrossRef]
- A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus. 6 October 2021. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 9 May 2022).
- Quraishi, S.A.; Camargo, C.A. Vitamin D in acute stress and critical illness. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 625–634. [Google Scholar] [CrossRef]
- Murdoch, D.R.; Slow, S.; Chambers, S.T.; Jennings, L.C.; Stewart, A.W.; Priest, P.C.; Florkowski, C.M.; Livesey, J.H.; Camargo, C.A.; Scragg, R. Effect of vitamin D3 supplementation on upper respiratory tract infections in healthy adults: The VIDARIS randomized controlled trial. JAMA 2012, 308, 1333–1339. [Google Scholar] [CrossRef]
- Forrest, K.Y.Z.; Stuhldreher, W.L. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef]
- Sabetta, J.R.; DePetrillo, P.; Cipriani, R.J.; Smardin, J.; Burns, L.A.; Landry, M.L. Serum 25-hydroxyvitamin d and the incidence of acute viral respiratory tract infections in healthy adults. PLoS ONE 2010, 5, e11088. [Google Scholar] [CrossRef]
- Hayashi, H.; Okamatsu, M.; Ogasawara, H.; Tsugawa, N.; Isoda, N.; Matsuno, K.; Sakoda, Y. Oral Supplementation of the Vitamin D Metabolite 25(OH)D3 Against Influenza Virus Infection in Mice. Nutrients 2020, 12, E2000. [Google Scholar] [CrossRef]
- Molloy, E.J.; Murphy, N. Vitamin D, COVID-19 and Children. Ir. Med. J. 2020, 113, 64. [Google Scholar]
- Wang, H.; Chen, W.; Li, D.; Yin, X.; Zhang, X.; Olsen, N.; Zheng, S.G. Vitamin D and Chronic Diseases. Aging Dis. 2017, 8, 346–353. [Google Scholar] [CrossRef]
- Armas, L.A.G.; Heaney, R.P. Vitamin D: The Iceberg Nutrient. J. Ren. Nutr. 2011, 21, 134–139. [Google Scholar] [CrossRef]
- Pike, J.W.; Christakos, S. Biology and Mechanisms of Action of the Vitamin D Hormone. Endocrinol. Metab. Clin. N. Am. 2017, 46, 815–843. [Google Scholar] [CrossRef]
- Braun, A.B.; Gibbons, F.K.; Litonjua, A.A.; Giovannucci, E.; Christopher, K.B. Low serum 25-hydroxyvitamin D at critical care initiation is associated with increased mortality. Crit. Care Med. 2012, 40, 63–72. [Google Scholar] [CrossRef]
- Biesalski, H.K. Vitamin D deficiency and co-morbidities in COVID-19 patients—A fatal relationship? Nfs J. 2020, 20, 10–21. [Google Scholar] [CrossRef]
- Oristrell, J.; Oliva, J.C.; Casado, E.; Subirana, I.; Domínguez, D.; Toloba, A.; Balado, A.; Grau, M. Vitamin D supplementation and COVID-19 risk: A population-based, cohort study. J. Endocrinol. Investig. 2022, 45, 167–179. [Google Scholar] [CrossRef]
- Aloia, J.F.; Patel, M.; Dimaano, R.; Li-Ng, M.; Talwar, S.A.; Mikhail, M.; Pollack, S.; Yeh, J.K. Vitamin D intake to attain a desired serum 25-hydroxyvitamin D concentration. Am. J. Clin. Nutr. 2008, 87, 1952–1958. [Google Scholar] [CrossRef]
- Judd, S.E.; Tangpricha, V. Vitamin D Deficiency and Risk for Cardiovascular Disease. Am. J. Med. Sci. 2009, 338, 40–44. [Google Scholar] [CrossRef]
- Baz-Hecht, M.; Goldfine, A.B. The impact of vitamin D deficiency on diabetes and cardiovascular risk. Curr. Opin. Endocrinol. Diabetes Obes. 2010, 17, 113–119. [Google Scholar] [CrossRef]
- Latic, N.; Erben, R.G. Vitamin D and Cardiovascular Disease, with Emphasis on Hypertension, Atherosclerosis, and Heart Failure. Int. J. Mol. Sci. 2020, 21, E6483. [Google Scholar] [CrossRef]
- McMullan, C.J.; Borgi, L.; Curhan, G.C.; Fisher, N.; Forman, J.P. The effect of vitamin D on renin-angiotensin system activation and blood pressure: A randomized control trial. J. Hypertens. 2017, 35, 822–829. [Google Scholar] [CrossRef]
- Khan, D.M.; Ullah, A.; Randhawa, F.A.; Iqtadar, S.; Butt, N.F.; Waheed, K. Role of Vitamin D in reducing number of acute exacerbations in Chronic Obstructive Pulmonary Disease (COPD) patients. Pak. J. Med. Sci. 2017, 33, 610–614. [Google Scholar] [CrossRef]
- Berridge, M.J. Vitamin D deficiency and diabetes. Biochem. J. 2017, 474, 1321–1332. [Google Scholar] [CrossRef]
- Lima, R.S.; Rocha, L.P.C.; Moreira, P.R. Genetic and epigenetic control of ACE2 expression and its possible role in COVID-19. Cell Biochem. Funct. 2021, 39, 713–726. [Google Scholar] [CrossRef]
- Shirvaliloo, M. Epigenomics in COVID-19; the link between DNA methylation, histone modifications and SARS-CoV-2 infection. Epigenomics 2021, 13, 745–750. [Google Scholar] [CrossRef]
- Thacher, T.D. Evaluating the Evidence in Clinical Studies of Vitamin D in COVID-19. Nutrients 2022, 14, 464. [Google Scholar] [CrossRef]
- Sanghera, D.K.; Sapkota, B.R.; Aston, C.E.; Blackett, P.R. Vitamin D Status, Gender Differences and Cardiometabolic Health Disparities. Ann. Nutr. Metab. 2017, 70, 79–87. [Google Scholar] [CrossRef]
- AlQuaiz, A.M.; Kazi, A.; Fouda, M.; Alyousefi, N. Age and gender differences in the prevalence and correlates of vitamin D deficiency. Arch. Osteoporos. 2018, 13, 49. [Google Scholar] [CrossRef]
- Connors, M.H.; Sheikholislam, B.M.; Irias, J.J. Vitamin D toxicity after dieting in hypoparathyroidism. Pediatrics 1976, 57, 794–796. [Google Scholar] [CrossRef]
- Ziaie, H.; Razmjou, S.; Jomhouri, R.; Jenabi, A. Vitamin D Toxicity; Stored and Released from Adipose Tissue? Arch. Iran. Med. 2016, 19, 597–600. [Google Scholar] [CrossRef]
- Perticone, M.; Maio, R.; Sciacqua, A.; Suraci, E.; Pinto, A.; Pujia, R.; Zito, R.; Gigliotti, S.; Sesti, G.; Perticone, F. Ketogenic Diet-Induced Weight Loss is Associated with an Increase in Vitamin D Levels in Obese Adults. Molecules 2019, 24, E2499. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Days 1–15 Post PCR+ | Days 21–208 Post PCR+ | Adults without COVID-19 | |
|---|---|---|---|
| n = 90 | n = 41 | n = 18 | |
| Age, years ± SD | 56.5 ± 17.4 | 47.0 ± 18.0 | 47.8 ± 10.1 |
| BMI, mean ± SD | 31.8 ± 9.9 | 28.0 ± 6.0 | 25.0 ± 5.3 |
| Sex, no. (%) | |||
| Female | 45 (50) | 27 (66) | 14 (88) |
| Male | 45 (50) | 14 (34) | 4 (22) |
| Ethnicity, (%) | |||
| Hispanic/Latinx | 19 (21) | 6 (15) | 1 (6) |
| Non-Hispanic/Latinx | 71 (79) | 35 (85) | 17 (94) |
| Hospitalized | 71 (79) | 7 (17) | - |
| Non-hospitalized | 19 (21) | 35 (83) | - |
| Received Convalescent Plasma | 33 (37) | 2 (5) | - |
| Vitamin D supplementation | 6 (7) | 2 (5) | 2 (11) |
| Post-acute sequelae of COVID-19 (PASC) | 26 | 12 | - |
| Disease severity, no. (%) | |||
| Mild | 21 (23) | 34 (83) | - |
| Moderate | 35 (39) | 5 (12) | - |
| Severe | 34 (38) | 2 (5) | - |
| Without pre-existing conditions, (%) | 35 (39) | 27 (66) | |
| With pre-existing conditions, (%) | 55 (61) | 14 (34) | |
| DM | 29 (32) | 3 (7) | - |
| COPD | 8 (9) | 1 (2) | - |
| HTN | 31 (34) | 6 (15) | - |
| Asthma | 16 (18) | 5 (12) | - |
| Vitamin | Males (N = 59) | Females (N = 72) | p-Value |
|---|---|---|---|
| 25(OH)D | 23.2 ± 12.6 | 28.2 ± 13.9 | 0.037 |
| 25(OH)D3 | 22.8 ± 12.8 | 27.4 ± 14.4 | 0.057 |
| Vitamin | Normal/Underweight (N = 30) | Overweight (N = 37) | Obese (N = 64) | Omnibus ANOVA p-Value |
|---|---|---|---|---|
| 25(OH)D | 29.5 ± 13.9 | 29.4 ± 15.2 | 21.4 ± 11.6 *,a | 0.016 |
| 25(OH)D3 | 29.5 ± 13.9 | 29.4 ± 15.2 | 22.5 ± 11.6 * | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baxter, B.A.; Ryan, M.G.; LaVergne, S.M.; Stromberg, S.; Berry, K.; Tipton, M.; Natter, N.; Nudell, N.; McFann, K.; Dunn, J.; et al. Correlation between 25-hydroxyvitamin D/D3 Deficiency and COVID-19 Disease Severity in Adults from Northern Colorado. Nutrients 2022, 14, 5204. https://doi.org/10.3390/nu14245204
Baxter BA, Ryan MG, LaVergne SM, Stromberg S, Berry K, Tipton M, Natter N, Nudell N, McFann K, Dunn J, et al. Correlation between 25-hydroxyvitamin D/D3 Deficiency and COVID-19 Disease Severity in Adults from Northern Colorado. Nutrients. 2022; 14(24):5204. https://doi.org/10.3390/nu14245204
Chicago/Turabian StyleBaxter, Bridget A., Michaela G. Ryan, Stephanie M. LaVergne, Sophia Stromberg, Kailey Berry, Madison Tipton, Nicole Natter, Nikiah Nudell, Kim McFann, Julie Dunn, and et al. 2022. "Correlation between 25-hydroxyvitamin D/D3 Deficiency and COVID-19 Disease Severity in Adults from Northern Colorado" Nutrients 14, no. 24: 5204. https://doi.org/10.3390/nu14245204
APA StyleBaxter, B. A., Ryan, M. G., LaVergne, S. M., Stromberg, S., Berry, K., Tipton, M., Natter, N., Nudell, N., McFann, K., Dunn, J., Webb, T. L., Armstrong, M., Reisdorph, N., & Ryan, E. P. (2022). Correlation between 25-hydroxyvitamin D/D3 Deficiency and COVID-19 Disease Severity in Adults from Northern Colorado. Nutrients, 14(24), 5204. https://doi.org/10.3390/nu14245204