
Effects of Irvingia gabonensis Extract on Metabolism, Antioxidants, Adipocytokines, Telomere Length, and Aerobic Capacity in Overweight/Obese Individuals

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
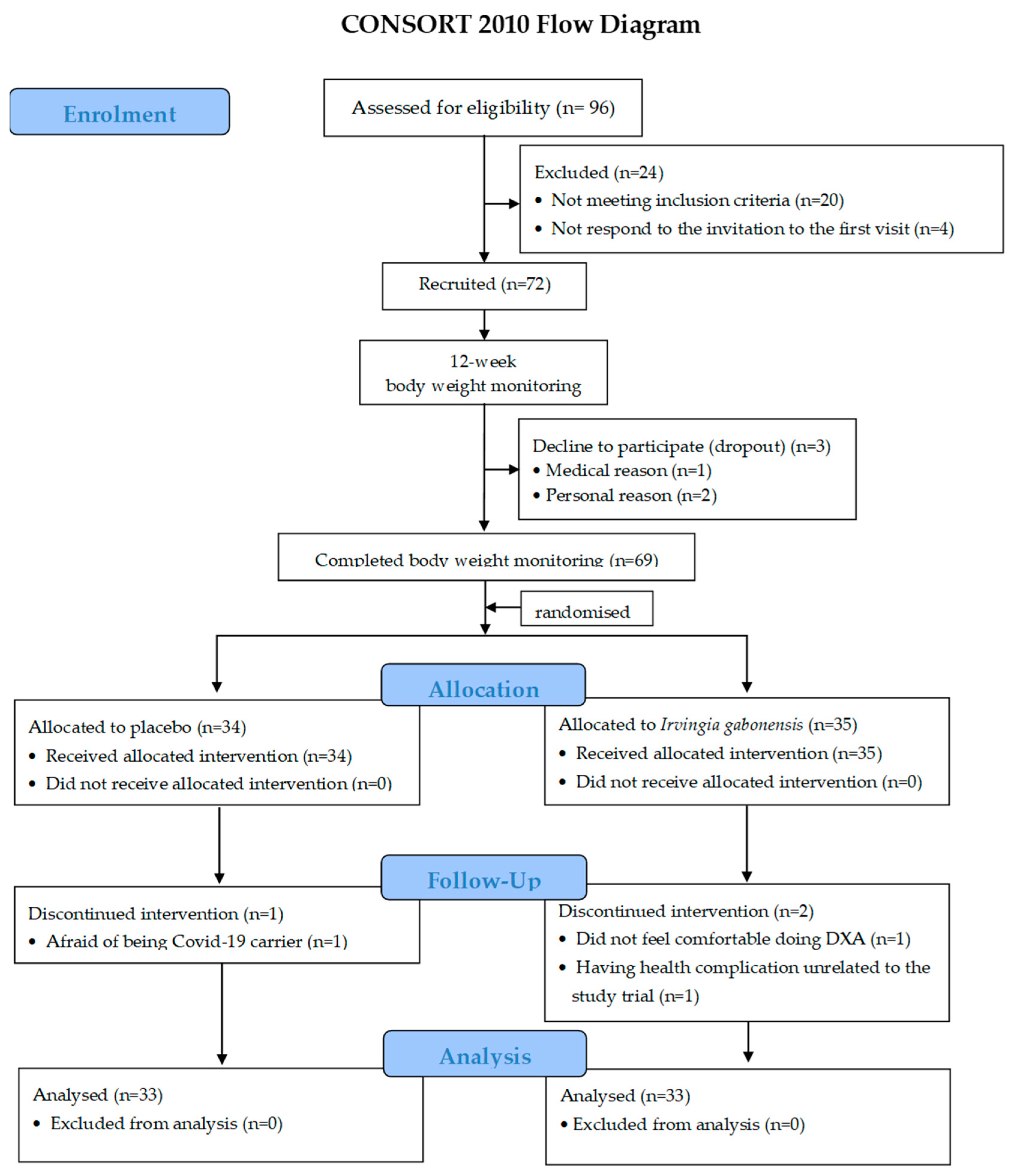
2.1. Participants
2.2. Research Design, Randomised Allocation, and Blinding
2.2.1. Power Calculation
2.2.2. IG and PLA Preparation
2.2.3. Supplementation Intake and Adverse Event Monitoring
2.3. Study Protocol
Blood Collection
2.4. Outcome Measurements
2.4.1. Adiposity Outcomes
2.4.2. Dietary Intake and Energy Expenditure Record
2.4.3. Metabolic Markers
Fat Oxidation Measurement
Blood Chemistry
Serum Leptin and Adiponectin Measurements
2.4.4. Redox Status Measurement
2.4.5. Inflammation Measurement
2.4.6. RTL Measurement
2.4.7. Aerobic Capacity Test
2.5. Statistical Analysis
3. Results
3.1. Adiposity Indices
3.2. Metabolic Markers
3.2.1. Fat Oxidation
3.2.2. Blood Chemistry
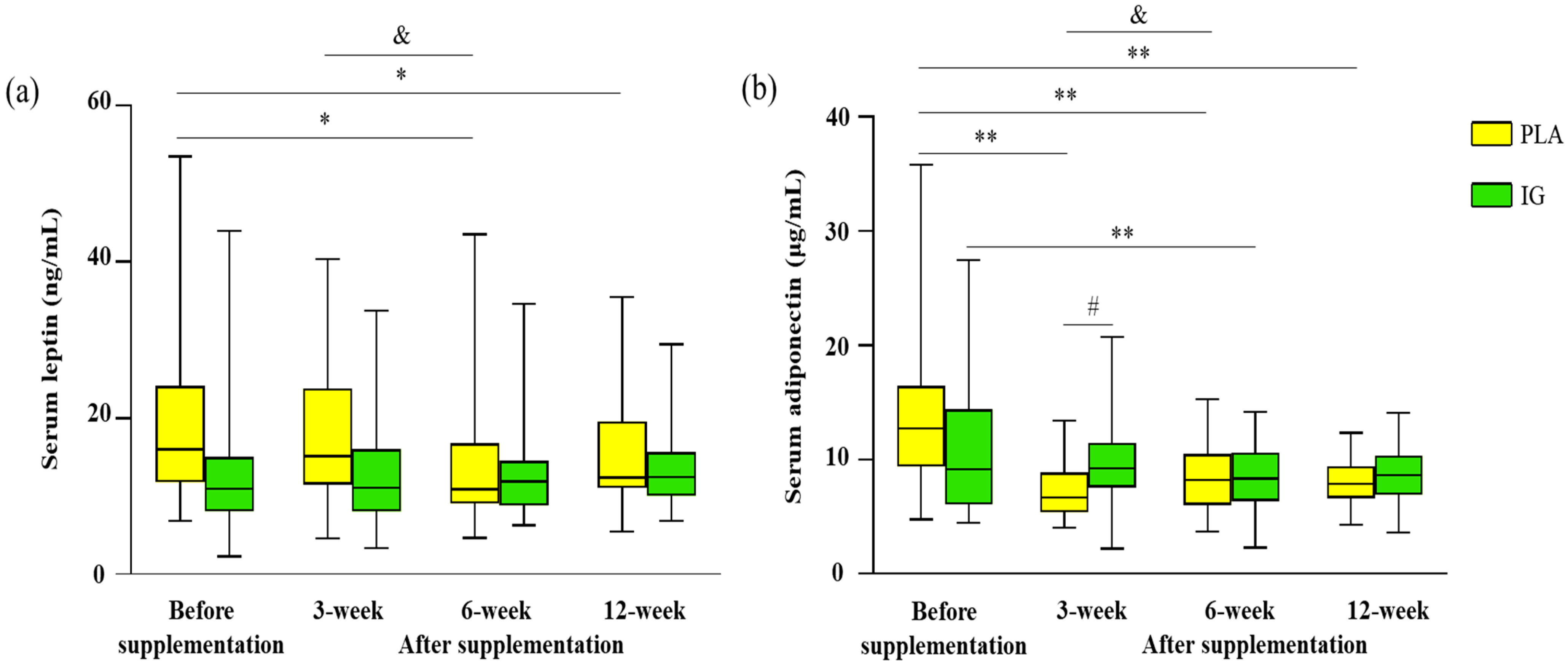
3.2.3. Serum Leptin and Adiponectin
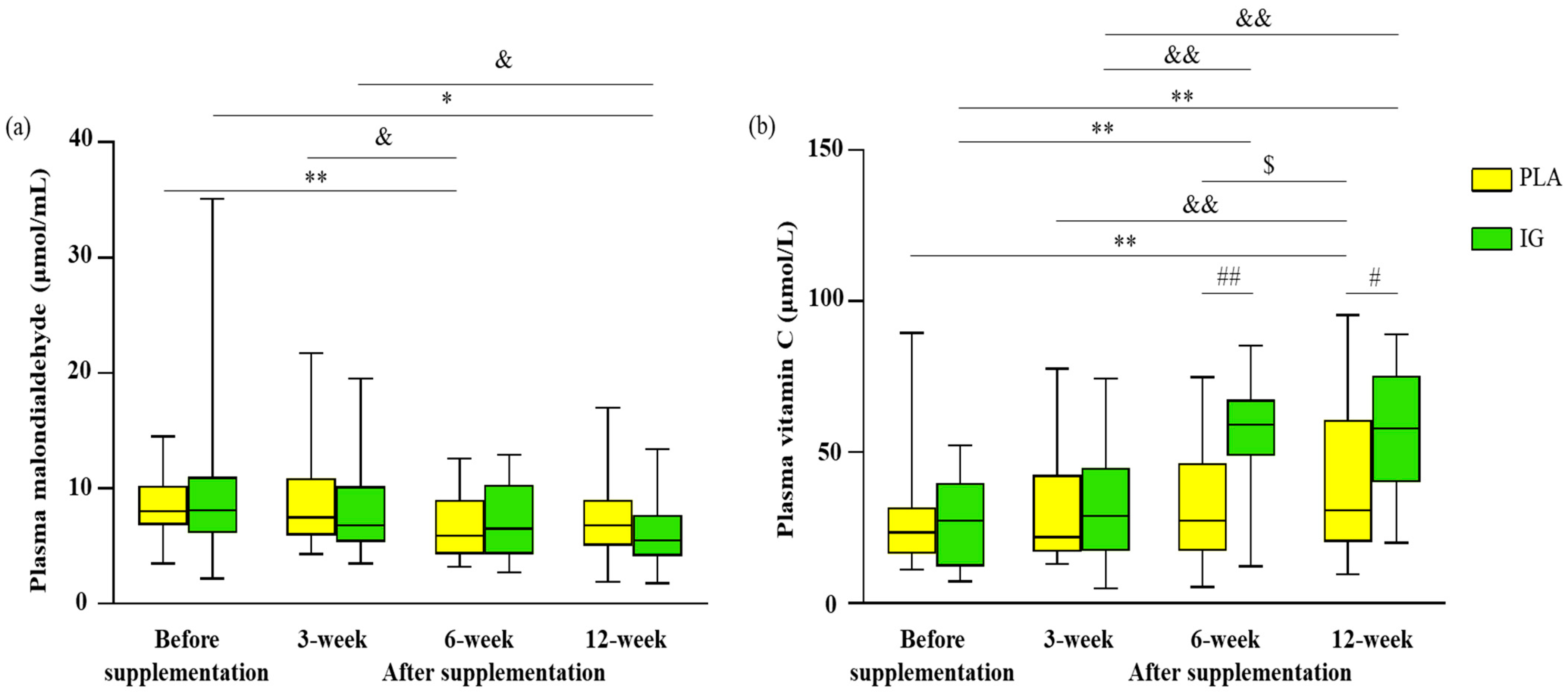
3.3. Redox Status and Inflammation
3.4. Blood Leukocyte Relative Telomere Length (RTL)
3.5. Aerobic Capacity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization; Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000; ISBN 978-0-9577082-1-1. [Google Scholar]
- Morgen, C.S.; Sørensen, T.I.A. Obesity: Global Trends in the Prevalence of Overweight and Obesity. Nat. Rev. Endocrinol. 2014, 10, 513–514. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, Pathophysiology, and Management of Obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Artemniak-Wojtowicz, D.; Kucharska, A.M.; Pyrżak, B. Obesity and Chronic Inflammation Crosslinking. Cent. Eur. J. Immunol. 2020, 45, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Forrester, S.J.; Kikuchi, D.S.; Hernandes, M.S.; Xu, Q.; Griendling, K.K. Reactive Oxygen Species in Metabolic and Inflammatory Signaling. Circ. Res. 2018, 122, 877–902. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Kukreti, R.; Saso, L.; Kukreti, S. Oxidative Stress: Role and Response of Short Guanine Tracts at Genomic Locations. Int. J. Mol. Sci. 2019, 20, 4258. [Google Scholar] [CrossRef]
- Picó, C.; Palou, M.; Pomar, C.A.; Rodríguez, A.M.; Palou, A. Leptin as a Key Regulator of the Adipose Organ. Rev. Endocr. Metab. Disord. 2022, 23, 13–30. [Google Scholar] [CrossRef]
- Blaak, E.E.; Saris, W.H.M. Substrate Oxidation, Obesity and Exercise Training. Best Pract. Res. Clin. Endocrinol. Metab. 2002, 16, 667–678. [Google Scholar] [CrossRef][Green Version]
- Hulens, M.; Vansant, G.; Lysens, R.; Claessens, A.L.; Muls, E. Exercise Capacity in Lean versus Obese Women. Scand. J. Med. Sci. Sport. 2001, 11, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Ranneries, C.; Bülow, J.; Buemann, B.; Christensen, N.J.; Madsen, J.; Astrup, A. Fat Metabolism in Formerly Obese Women. Am. J. Physiol. 1998, 274, E155–E161. [Google Scholar] [CrossRef]
- Fassina, P.; Scherer Adami, F.; Terezinha Zani, V.; Kasper Machado, I.C.; Garavaglia, J.; Quevedo Grave, M.T.; Ramos, R.; Morelo Dal Bosco, S. The effect of Garcinia cambogia as coadjuvant in the weight loss process. Nutr. Hosp. 2015, 32, 2400–2408. [Google Scholar] [CrossRef]
- Liu, J.; Lee, J.; Salazar Hernandez, M.A.; Mazitschek, R.; Ozcan, U. Treatment of Obesity with Celastrol. Cell 2015, 161, 999–1011. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Yun, P.; Hu, Y.; Yang, J.; Khadka, R.B.; Peng, X. Effects of Grape Seed Proanthocyanidin Extract on Obesity. Obes. Facts 2020, 13, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Unuofin, J.O.; Otunola, G.A.; Afolayan, A.J. Polyphenolic Content, Antioxidant and Antimicrobial Activities of Vernonia mespilifolia Less. Used in Folk Medicine in the Eastern Cape Province, South Africa. J. Evid. Based Integr. Med. 2018, 23, 2515690X18773990. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Chen, P. UHPLC/HRMS Analysis of African Mango (Irvingia gabonensis) Seeds, Extract and Related Dietary Supplements. J. Agric Food Chem. 2012, 60, 8703–8709. [Google Scholar] [CrossRef]
- Lee, J.; Chung, M.; Fu, Z.; Choi, J.; Lee, H.-J. The Effects of Irvingia gabonensis Seed Extract Supplementation on Anthropometric and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis. J. Am. Coll. Nutr. 2020, 39, 388–396. [Google Scholar] [CrossRef]
- Ross, S.M. African Mango (IGOB131): A Proprietary Seed Extract of Irvingia gabonensis Is Found to Be Effective in Reducing Body Weight and Improving Metabolic Parameters in Overweight Humans. Holist. Nurs. Pract. 2011, 25, 215–217. [Google Scholar] [CrossRef]
- Onakpoya, I.; Davies, L.; Posadzki, P.; Ernst, E. The Efficacy of Irvingia gabonensis Supplementation in the Management of Overweight and Obesity: A Systematic Review of Randomized Controlled Trials. J. Diet. Suppl. 2013, 10, 29–38. [Google Scholar] [CrossRef]
- Ngondi, J.L.; Oben, J.E.; Minka, S.R. The Effect of Irvingia gabonensis Seeds on Body Weight and Blood Lipids of Obese Subjects in Cameroon. Lipids Health Dis. 2005, 4, 12. [Google Scholar] [CrossRef]
- Ngondi, J.L.; Etoundi, B.C.; Nyangono, C.B.; Mbofung, C.M.; Oben, J.E. IGOB131, a Novel Seed Extract of the West African Plant Irvingia gabonensis, Significantly Reduces Body Weight and Improves Metabolic Parameters in Overweight Humans in a Randomized Double-Blind Placebo Controlled Investigation. Lipids Health Dis. 2009, 8, 7. [Google Scholar] [CrossRef]
- Mateus-Reguengo, L.; Barbosa-Pereira, L.; Rembangouet, W.; Bertolino, M.; Giordano, M.; Rojo-Poveda, O.; Zeppa, G. Food Applications of Irvingia gabonensis (Aubry-Lecomte Ex. O’Rorke) Baill., the “Bush Mango”: A Review. Crit. Rev. Food Sci. Nutr. 2020, 60, 2446–2459. [Google Scholar] [CrossRef]
- Olorundare, O.; Adeneye, A.; Akinsola, A.; Soyemi, S.; Mgbehoma, A.; Okoye, I.; Ntambi, J.M.; Mukhtar, H. African Vegetables (Clerodendrum volubile Leaf and Irvingia gabonensis Seed Extracts) Effectively Mitigate Trastuzumab-Induced Cardiotoxicity in Wistar Rats. Oxid. Med. Cell. Longev. 2020, 2020, 9535426. [Google Scholar] [CrossRef] [PubMed]
- Awah, F.; Uzoegwu, P.; Ifeonu, P.; Oyugi, J.; Rutherford, J.; Yao, X.; Fehrmann, F.; Fowke, K.; Eze, M. Free Radical Scavenging Activity, Phenolic Contents and Cytotoxicity of Selected Nigerian Medicinal Plants. Food Chem. 2012, 131, 1279–1286. [Google Scholar] [CrossRef]
- Oben, J.E.; Ngondi, J.L.; Blum, K. Inhibition of Irvingia gabonensis Seed Extract (OB131) on Adipogenesis as Mediated via down Regulation of the PPARgamma and Leptin Genes and up-Regulation of the Adiponectin Gene. Lipids Health Dis. 2008, 7, 44. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.D.; Roberts, M.G.; Tarpey, M.D.; Weekes, J.C.; Thomas, C.H. The Effect of a Decaffeinated Green Tea Extract Formula on Fat Oxidation, Body Composition and Exercise Performance. J. Int. Soc. Sport Nutr. 2015, 12, 1. [Google Scholar] [CrossRef] [PubMed]
- Rosner, B. Fundamentals of Biostatistics; Cengage Learning: Boston, MA, USA, 2015; ISBN 978-1-305-46551-0. [Google Scholar]
- Kothari, S.C.; Shivarudraiah, P.; Venkataramaiah, S.B.; Gavara, S.; Soni, M.G. Subchronic Toxicity and Mutagenicity/Genotoxicity Studies of Irvingia gabonensis Extract (IGOB131). Food Chem. Toxicol. 2012, 50, 1468–1479. [Google Scholar] [CrossRef]
- Online Thai Food Composition Database (THAI FCD). Available online: https://inmu2.mahidol.ac.th/thaifcd/home.php (accessed on 26 June 2022).
- Péronnet, F.; Massicotte, D. Table of Nonprotein Respiratory Quotient: An Update. Can. J. Sport Sci. 1991, 16, 23–29. [Google Scholar] [PubMed]
- Draper, H.H.; Squires, E.J.; Mahmoodi, H.; Wu, J.; Agarwal, S.; Hadley, M. A Comparative Evaluation of Thiobarbituric Acid Methods for the Determination of Malondialdehyde in Biological Materials. Free Radic. Biol. Med. 1993, 15, 353–363. [Google Scholar] [CrossRef]
- Zhang, H.; Li, J.; Wang, K.; Du, X.; Li, Q. A Simple and Sensitive Assay for Ascorbate Using Potassium Ferricyanide as Spectroscopic Probe Reagent. Anal. Biochem. 2009, 388, 40–46. [Google Scholar] [CrossRef]
- Cawthon, R.M. Telomere Measurement by Quantitative PCR. Nucleic Acids Res. 2002, 30, e47. [Google Scholar] [CrossRef]
- Udomsinprasert, W.; Poovorawan, Y.; Chongsrisawat, V.; Vejchapipat, P.; Jittikoon, J.; Honsawek, S. Leukocyte Mitochondrial DNA Copy Number as a Potential Biomarker Indicating Poor Outcome in Biliary Atresia and Its Association with Oxidative DNA Damage and Telomere Length. Mitochondrion 2019, 47, 1–9. [Google Scholar] [CrossRef]
- Boonthongkaew, C.; Tong-Un, T.; Kanpetta, Y.; Chaungchot, N.; Leelayuwat, C.; Leelayuwat, N. Vitamin C Supplementation Improves Blood Pressure and Oxidative Stress after Acute Exercise in Patients with Poorly Controlled Type 2 Diabetes Mellitus: A Randomized, Placebo-Controlled, Cross-over Study. Chin. J. Physiol. 2021, 64, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-Predicted Maximal Heart Rate Revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Marrocco, I.; Altieri, F.; Peluso, I. Measurement and Clinical Significance of Biomarkers of Oxidative Stress in Humans. Oxid. Med. Cell. Longev. 2017, 2017, 6501046. [Google Scholar] [CrossRef] [PubMed]
- Achari, A.E.; Jain, S.K. Adiponectin, a Therapeutic Target for Obesity, Diabetes, and Endothelial Dysfunction. Int. J. Mol. Sci. 2017, 18, 1321. [Google Scholar] [CrossRef]
- Obradovic, M.; Sudar-Milovanovic, E.; Soskic, S.; Essack, M.; Arya, S.; Stewart, A.J.; Gojobori, T.; Isenovic, E.R. Leptin and Obesity: Role and Clinical Implication. Front. Endocrinol. 2021, 12, 585887. [Google Scholar] [CrossRef]
- Kwon, H.; Pessin, J.E. Adipokines Mediate Inflammation and Insulin Resistance. Front. Endocrinol. 2013, 4, 71. [Google Scholar] [CrossRef]
- Ryo, M.; Nakamura, T.; Kihara, S.; Kumada, M.; Shibazaki, S.; Takahashi, M.; Nagai, M.; Matsuzawa, Y.; Funahashi, T. Adiponectin as a Biomarker of the Metabolic Syndrome. Circ. J. 2004, 68, 975–981. [Google Scholar] [CrossRef]
- Singh, R.B.; Beegom, R.; Rastogi, S.S.; Gaoli, Z.; Shoumin, Z. Association of Low Plasma Concentrations of Antioxidant Vitamins, Magnesium and Zinc with High Body Fat per Cent Measured by Bioelectrical Impedance Analysis in Indian Men. Magnes. Res. 1998, 11, 3–10. [Google Scholar]
- Lee, H.; Ahn, J.; Shin, S.S.; Yoon, M. Ascorbic Acid Inhibits Visceral Obesity and Nonalcoholic Fatty Liver Disease by Activating Peroxisome Proliferator-Activated Receptor α in High-Fat-Diet-Fed C57BL/6J Mice. Int. J. Obes. 2019, 43, 1620–1630. [Google Scholar] [CrossRef]
- Wilson, R.; Willis, J.; Gearry, R.; Skidmore, P.; Fleming, E.; Frampton, C.; Carr, A. Inadequate Vitamin C Status in Prediabetes and Type 2 Diabetes Mellitus: Associations with Glycaemic Control, Obesity, and Smoking. Nutrients 2017, 9, 997. [Google Scholar] [CrossRef]
- Howard, P.A.; Meyers, D.G. Effect of Vitamin C on Plasma Lipids. Ann. Pharm. 1995, 29, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Pancorbo, D.; Vazquez, C.; Fletcher, M.A. Vitamin C-Lipid Metabolites: Uptake and Retention and Effect on Plasma C-Reactive Protein and Oxidized LDL Levels in Healthy Volunteers. Med. Sci. Monit. 2008, 14, CR547–CR551. [Google Scholar]
- Sen, A.; Marsche, G.; Freudenberger, P.; Schallert, M.; Toeglhofer, A.M.; Nagl, C.; Schmidt, R.; Launer, L.J.; Schmidt, H. Association between Higher Plasma Lutein, Zeaxanthin, and Vitamin C Concentrations and Longer Telomere Length: Results of the Austrian Stroke Prevention Study. J. Am. Geriatr. Soc. 2014, 62, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.D.; Maughan, R.J.; Duthie, G.G.; Morrice, P.C. Increased Blood Antioxidant Systems of Runners in Response to Training Load. Clin. Sci. 1991, 80, 611–618. [Google Scholar] [CrossRef]
- Apostolova, N.; Victor, V.M. Molecular Strategies for Targeting Antioxidants to Mitochondria: Therapeutic Implications. ARS 2015, 22, 686–729. [Google Scholar] [CrossRef]
- Englard, S.; Seifter, S. The Biochemical Functions of Ascorbic Acid. Annu. Rev. Nutr. 1986, 6, 365–406. [Google Scholar] [CrossRef]
- Albrecht, E.; Sillanpaa, E.; Karrasch, S.; Alves, A.C.; Codd, V.; Hovatta, I.; Buxton, J.L.; Nelson, C.P.; Broer, L.; Hagg, S.; et al. Telomere Length in Circulating Leukocytes Is Associated with Lung Function and Disease. Eur. Respir. J. 2014, 43, 983–992. [Google Scholar] [CrossRef] [PubMed]
- Lendeckel, F.; Zylla, S.; Markus, M.R.P.; Ewert, R.; Gläser, S.; Völzke, H.; Albrecht, D.; Friedrich, N.; Nauck, M.; Felix, S.B.; et al. Association of Cardiopulmonary Exercise Capacity and Adipokines in the General Population. Int. J. Sport Med. 2022, 43, 616–624. [Google Scholar] [CrossRef] [PubMed]
- de Lima Vieira-Brock, P.; Vaughan, B.M.; Vollmer, D.L. Thermogenic Blend Alone or in Combination with Whey Protein Supplement Stimulates Fat Metabolism and Improves Body Composition in Mice. Pharmacogn. Res. 2018, 10, 37–43. [Google Scholar] [CrossRef]
- Uti, D.E.; Atangwho, I.J.; Eyong, E.U.; Umoru, G.U.; Egbung, G.E.; Nna, V.U.; Udeozor, P.A. African Walnuts Attenuate Ectopic Fat Accumulation and Associated Peroxidation and Oxidative Stress in Monosodium Glutamate-Obese Wistar Rats. Biomed. Pharm. 2020, 124, 109879. [Google Scholar] [CrossRef]
- Arika, W.; Kibiti, C.M.; Njagi, J.M.; Ngugi, M.P. In Vitro Antioxidant Properties of Dichloromethanolic Leaf Extract of Gnidia Glauca (Fresen) as a Promising Antiobesity Drug. J. Evid. Based Integr. Med. 2019, 24, 2515690X19883258. [Google Scholar] [CrossRef] [PubMed]
- Lundholm, L.; Zang, H.; Hirschberg, A.L.; Gustafsson, J.-A.; Arner, P.; Dahlman-Wright, K. Key Lipogenic Gene Expression Can Be Decreased by Estrogen in Human Adipose Tissue. Fertil. Steril. 2008, 90, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Cho, H.T.; Kim, Y.J. The Role of Estrogen in Adipose Tissue Metabolism: Insights into Glucose Homeostasis Regulation. Endocr. J. 2014, 61, 1055–1067. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, J. Effects of gender on vitamin C pharmacokinetics in man. J. Am. Coll. Nutr. 1991, 10, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Song, H.J.; Oh, S.; Quan, S.; Ryu, O.H.; Jeong, J.Y.; Hong, K.S.; Kim, D.H. Gender differences in adiponectin levels and body composition in older adults: Hallym aging study. BMC Geriatr. 2014, 14, 8. [Google Scholar] [CrossRef]
- Zhang, Y.B.; Chen, W.H.; Guo, J.J.; Fu, Z.H.; Yi, C.; Zhang, M.; Na, X.L. Soy isoflavone supplementation could reduce body weight and improve glucose metabolism in non-Asian postmenopausal women—A meta-analysis. Nutrition 2013, 29, 8–14. [Google Scholar] [CrossRef]
- Greenlee, H.; Hershman, D.L.; Jacobson, J.S. Use of antioxidant supplements during breast cancer treatment: A comprehensive review. Breast Cancer Res. Treat. 2009, 115, 437–452. [Google Scholar] [CrossRef]
- Tsoukalas, D.; Fragkiadaki, P.; Docea, A.O.; Alegakis, A.K.; Sarandi, E.; Vakonaki, E.; Salataj, E.; Kouvidi, E.; Nikitovic, D.; Kovatsi, L.; et al. Association of nutraceutical supplements with longer telomere length. Int. J. Mol. Med. 2019, 44, 218–226. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Body Weight Monitoring Phase | ||
|---|---|---|
| Before (Visit 1) (n = 66) | After (Visit 2) (n = 66) | |
| Age (years) | 44.7 ± 6.7 | 44.7 ± 6.7 |
| Gender (women/men) | 66/0 | 66/0 |
| BW (kg) | 61.1 ± 5.4 | 61.2 ± 5.5 |
| Ht (m) | 1. 6 ± 0.1 | 1. 6 ± 0.1 |
| BMI (kg/m2) | 24.7 (24.1–26.4) | 25.1 (24.1–26.5) |
| W (cm) | 86.4 ± 6.1 | 88.0 ± 6.3 |
| H (cm) | 99.2 ± 4.9 | 99.8 ± 4.6 |
| W/H | 0.86 (0.84–0.91) | 0.88 (0.84–0.92) |
| RHR (/min) | 68.1 ± 8.5 | 65.5 ± 7.9 |
| SBP (mmHg) | 119.3 ± 12.9 | 119.6 ± 14.2 |
| DBP (mmHg) | 75.0 ± 9.8 | 75.9 ± 9.1 |
| MAP (mmHg) | 85.5 (78.5–91.5) | 85.0 (79.0–90.0) |
| FBG (mg/dL) | 92.9 (84.0–104.0) | 87.0 (84.0–93.0) |
| TC (mg/dL) | 186.7 ± 33.5 | 189.7 ± 37.1 |
| HDL-c (mg/dL) | 50.4 ± 14.2 | 52.7 ± 11.6 |
| LDL-c (mg/dL) | 110.4 ± 32.3 | 114.0 ± 34.0 |
| HDL-c/LDL-c ratio | 0.43 (0.33–0.60) | 0.47 (0.39–0.57) |
| TC/HDL-c ratio | 3.78 (3.15–4.55) | 3.50 (3.06–3.97) |
| TG (mg/dL) | 105.5 (85.1–137.0) | 100.9 (71.0–140.0) |
| Cr (mg/dL) | 0.7 ± 0.1 | 0. 8 ± 0.1 |
| SGPT (IU/L) | 14.7 (11.7–18.1) | 14.0 (11.6–18.1) |
| PLA (n = 33) | IG (n = 33) | |
|---|---|---|
| CHO intake (g) | ||
| Before | 257.5 ± 61.8 | 253.5 ± 63.8 |
| After 3 weeks | 249.4 ± 78.19 | 264.5 ± 61.7 |
| After 6 weeks | 243.1 ± 68.2 | 253.7 ± 58.4 |
| After 12 weeks | 267.8 ± 72.0 | 239.2 ± 59.0 |
| Fat intake (g) | ||
| Before | 49.8 ± 21.3 | 37.9 ± 14.5 # |
| After 3 weeks | 51.9 ± 22.7 | 36.2 ± 11.5 ## |
| After 6 weeks | 44.8 ± 15.6 | 36.8 ± 14.0 |
| After 12 weeks | 48.5 ± 17.1 | 37.4 ± 11.1 |
| Protein intake (g) | ||
| Before | 79.5 ± 19.3 | 66.8 ± 15.4 # |
| After 3 weeks | 82.4 ± 27.9 | 63.5 ± 13.3 ## |
| After 6 weeks | 79.3 ± 20.6 | 65.4 ± 13.3 ## |
| After 12 weeks | 82.3 ± 22.9 | 61.3 ± 12.9 ## |
| Vitamin C intake (mg/day) | ||
| Before | 49.6 (32.5–95.6) | 48.5 (34.8–74.9) |
| After 3 weeks | 71.6 (32.2–87.7) | 43.0 (26.4–59.3) |
| After 6 weeks | 66.2 (33.5–84.8) | 48.4 (39.0–90.1) |
| After 12 weeks | 49.8 (26.8–68.7) | 48.5 (26.9–75.0) |
| Energy intake (kcal/day) | ||
| Before | 1796.4 ±440.7 | 1622.2 ± 329.5 |
| After 3 weeks | 1794.2 ± 488.4 | 1637.8 ± 299.4 |
| After 6 weeks | 1692.9 ± 381.5 | 1607.5 ± 296.2 |
| After 12 weeks | 2122.5 ± 1734.0 | 1538.6 ± 294.7 |
| Energy expenditure (kcal/day) | ||
| Before | 1376.8 ± 260.3 | 1461.2 ± 218.1 |
| After 3 weeks | 1444.7 ± 296.6 | 1462.0 ± 274.1 |
| After 6 weeks | 1404.3 ± 370.1 | 1470.0 ± 278.9 |
| After 12 weeks | 1435.5 ± 332.3 | 1487.9 ± 284.0 |
| PLA (n = 33) | IG (n = 33) | |
|---|---|---|
| BW (kg) | ||
| Before | 59.7 (56.8–64.8) | 61.1 (57.3–63.6) |
| After 3 weeks | 60.5 (56.9–65.1) | 62.0 (57.3–64.1) |
| After 6 weeks | 60.2 (56.9–65.3) | 62.0 (57.5–63.5) |
| After 12 weeks | 60.0 (56.6–65.6) | 62.4 (57.3–64.0) |
| BMI (kg/m2) | ||
| Before | 25.3 (24.1–27.0) | 24.7 (24.1–25.6) |
| After 3 weeks | 25.8 (23.9–27.0) | 24.8 (24.1–26.0) |
| After 6 weeks | 25.7 (24.0–26.2) | 24.9 (24.2–26.0) |
| After 12 weeks | 25.3 (24.0–27.3) | 24.7 (24.2–26.0) |
| W (cm) | ||
| Before | 88.6 ± 6.8 | 87.3 ± 5.8 |
| After 3 weeks | 88.4 ± 7.0 | 86.9 ± 5.7 |
| After 6 weeks | 88.2 ± 6.9 | 86.3 ± 5.4 |
| After 12 weeks | 87.6 ± 7.0 | 86.6 ± 6.1 |
| FM (%) | ||
| Before | 36.4 ± 2.8 | 35.5 ± 3.1 |
| After 3 weeks | 36.7 ± 2.7 | 35.8 ± 3.1 |
| After 6 weeks | 36.7 ± 2.9 | 35.9 ± 3.1 |
| After 12 weeks | 36.8 ± 2.8 | 35.9 ± 3.1 |
| FM (kg) | ||
| Before | 23.1 ± 3.6 | 21.9 ± 3.9 |
| After 3 weeks | 23.3 ± 3.5 | 22.2 ± 2.9 |
| After 6 weeks | 23.3 ± 3.6 | 22.2 ± 2.8 |
| After 12 weeks | 23.2 ± 3.6 | 22.1 ± 2.6 |
| PLA (n = 33) | IG (n = 33) | Mean Difference (95% CI) | |
|---|---|---|---|
| Fat oxidation rate (mg/min) | |||
| Before | 45.7 ± 22.2 | 43.6 ± 20.2 | 2.08 mg/min; 95%CI, −8.34, 12.51 |
| After 3 weeks | 43.0 ± 22.8 | 43.6 ± 25.0 | −0.58 mg/min; 95%CI, −12.34, 11.18 |
| After 6 weeks | 44.5 ± 24.0 | 37.7 ± 15.3 | 6.83 mg/min; 95%CI, −3.07, 16.72 |
| After 12 weeks | 48.3 ± 19.9 | 40.5 ± 25.8 | 7.81 mg/min; 95%CI, −3.52, 19.14 |
| PLA (n = 33) | IG (n = 33) | |
|---|---|---|
| FBG (mg/dL) | ||
| Before | 87.0 (82.0–92.0) | 87.0 (85.0–93.0) |
| After 3 weeks | 85.0 (82.0–92.0) | 86.0 (82.0–94.0) |
| After 6 weeks | 86.0 (83.0–90.0) | 89.0 (82.0–94.0) |
| After 12 weeks | 88.0 (82.0–91.0) | 89.0 (86.0–91.0) |
| TC (mg/dL) | ||
| Before | 182.0 (166.0–209.0) | 191.0 (166.0–191.0) |
| After 3 weeks | 186.0 (170.0–217.0) | 187.0 (170.0–212.0) |
| After 6 weeks | 192.0 (176.0–206.0) | 190.0 (167.0–207.0) |
| After 12 weeks | 177.5 (166.0–207.0) | 192.0 (169.0–220.0) |
| HDL-c (mg/dL) | ||
| Before | 51.7 (42.6–58.4) | 54.2 (48.2–62.8) |
| After 3 weeks | 47.1 (40.5–54.6) | 52.8 (44.5–57.5) |
| After 6 weeks | 47.7 (41.9–55.5) | 52.5 (44.7–60.9) |
| After 12 weeks | 53.6 (43.1–58.6) | 47.0 (41.0–57.2) |
| LDL-c (mg/dL) | ||
| Before | 111.6 (91.9–133.6) | 108.6 (98.9–139.0) |
| After 3 weeks | 112.1 (101.7–140.2) | 106.4 (94.7–137.4) |
| After 6 weeks | 116.7 (105.0–142.9) | 115.8 (93.7–132.7) |
| After 12 weeks | 112.1 (83.5–137.5) | 112.3 (94.4–142.4) |
| HDL-c/LDL-c ratio | ||
| Before | 0.5 (0.4–0.6) | 0.6 (0.4–0.6) |
| After 3 weeks | 0.5 (0.3–0.5) | 0.5 (0.3–0.6) |
| After 6 weeks | 0.4 (0.3–0.5) | 0.4 (0.4–0.6) |
| After 12 weeks | 0.5 (0.3–0.6) | 0.4 (0.3–0.6) |
| TC/HDL-c ratio | ||
| Before | 3.5 (3.1–4.0) | 3.5 (2.8–3.9) |
| After 3 weeks | 3.6 (3.3–5.3) | 3.7 (3.1–4.4) |
| After 6 weeks | 3.9 (3.4–4.5) | 3.8 (3.2–4.2) |
| After 12 weeks | 3.4 (3.1–4.4) | 3.8 (3.3–4.8) |
| TG (mg/dL) | ||
| Before | 97.7 (82.5–140.0) | 106.0 (69.0–134.0) |
| After 3 weeks | 95.0 (69.0–141.0) | 112.0 (88.9–153.0) |
| After 6 weeks | 111.0 (84.2–145.0) | 105.0 (81.0–170.0) |
| After 12 weeks | 89.2 (73.4–126.0) | 119.0 (91.9–178.0) * |
| hsCRP (mg/dL) | ||
| Before | 1.6 (0.8–2.6) | 1.3 (0.8–1.8) |
| After 3 weeks | 1.3 (0.8–2.2) | 1.2 (0.8–1.9) |
| After 6 weeks | 1.9 (1.1–2.8) | 1.2 (0.9–2.2) |
| After 12 weeks | 1.5 (0.8–2.2) | 1.2 (0.7–1.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nonsa-ard, R.; Aneknan, P.; Tong-un, T.; Honsawek, S.; Leelayuwat, N. Effects of Irvingia gabonensis Extract on Metabolism, Antioxidants, Adipocytokines, Telomere Length, and Aerobic Capacity in Overweight/Obese Individuals. Nutrients 2022, 14, 4646. https://doi.org/10.3390/nu14214646
Nonsa-ard R, Aneknan P, Tong-un T, Honsawek S, Leelayuwat N. Effects of Irvingia gabonensis Extract on Metabolism, Antioxidants, Adipocytokines, Telomere Length, and Aerobic Capacity in Overweight/Obese Individuals. Nutrients. 2022; 14(21):4646. https://doi.org/10.3390/nu14214646
Chicago/Turabian StyleNonsa-ard, Rujira, Ploypailin Aneknan, Terdthai Tong-un, Sittisak Honsawek, and Naruemon Leelayuwat. 2022. "Effects of Irvingia gabonensis Extract on Metabolism, Antioxidants, Adipocytokines, Telomere Length, and Aerobic Capacity in Overweight/Obese Individuals" Nutrients 14, no. 21: 4646. https://doi.org/10.3390/nu14214646
APA StyleNonsa-ard, R., Aneknan, P., Tong-un, T., Honsawek, S., & Leelayuwat, N. (2022). Effects of Irvingia gabonensis Extract on Metabolism, Antioxidants, Adipocytokines, Telomere Length, and Aerobic Capacity in Overweight/Obese Individuals. Nutrients, 14(21), 4646. https://doi.org/10.3390/nu14214646