
Adherence to High Dietary Diversity and Incident Cognitive Impairment for the Oldest-Old: A Community-Based, Nationwide Cohort Study
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Measurement of DDS
2.3. Measurement of DDS Change Patterns
2.4. Assessment of Cognitive Function
2.5. Covariates
2.6. Statistical Analysis
3. Result
3.1. Participant Characteristics
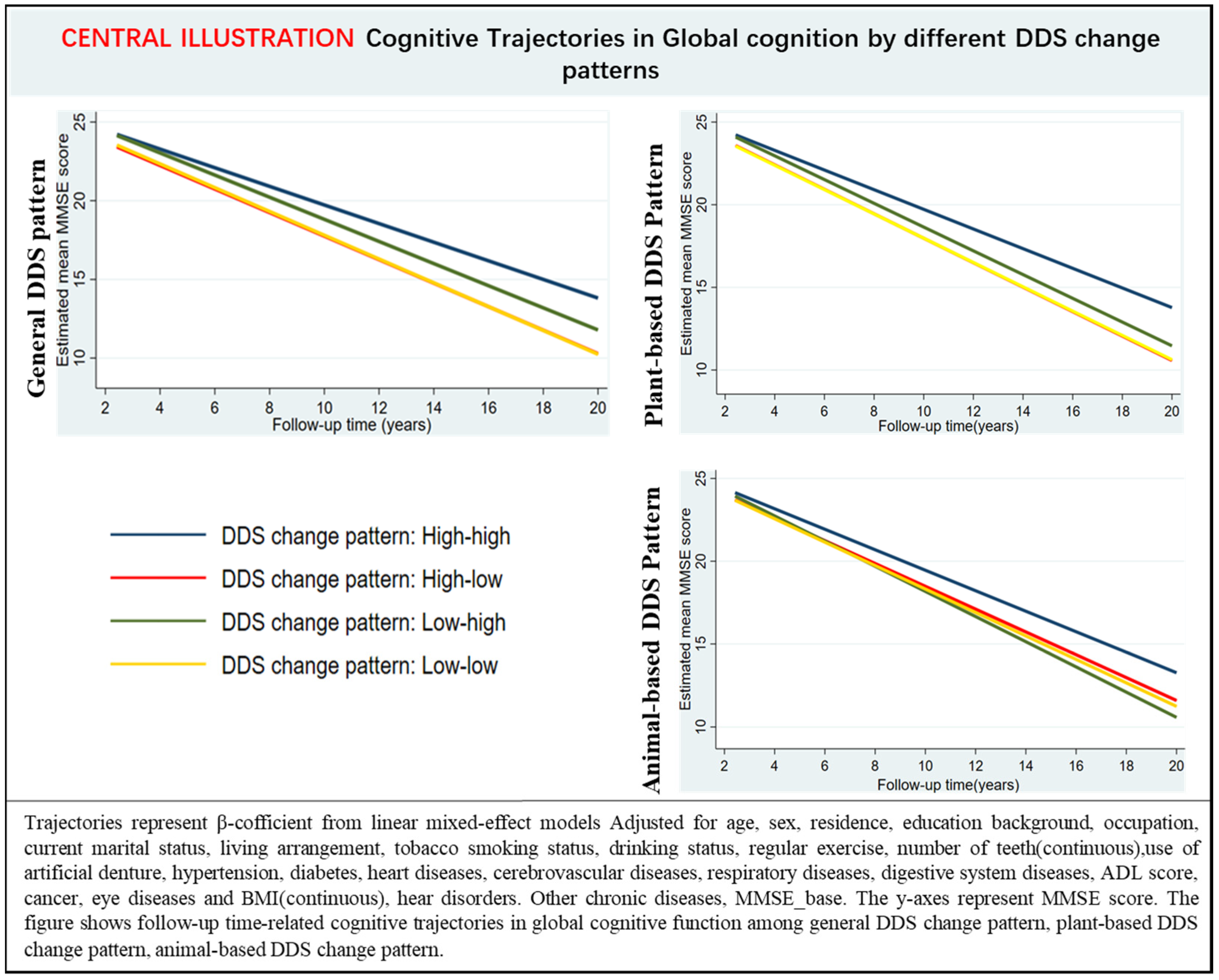
3.2. Association of DDS Change Patterns with Cognitive Impairment
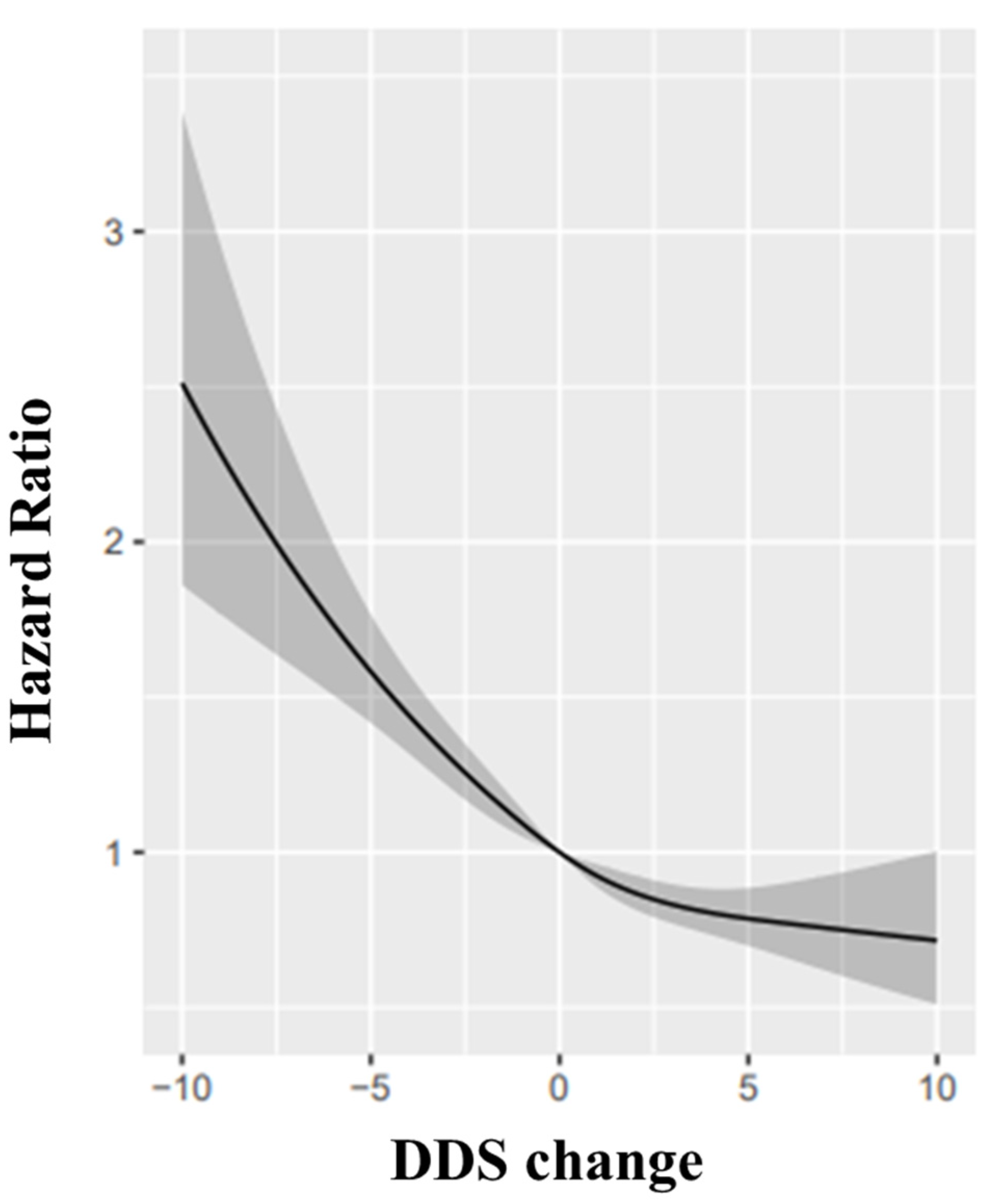
3.3. DDS Change Score and Cognitive Impairment
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015—The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International (ADI): London, UK, 2015. [Google Scholar]
- Jia, L.F.; Du, Y.F.; Chu, L.; Zhang, Z.J.; Li, F.Y.; Lyu, D.Y.; Li, Y.; Li, Y.; Zhu, M.; Jiao, H.S.; et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: A cross-sectional study. Lancet Public Health 2020, 5, E661–E671. [Google Scholar] [CrossRef]
- Lourida, I.; Soni, M.; Thompson-Coon, J.; Purandare, N.; Lang, I.A.; Ukoumunne, O.C.; Llewellyn, D.J. Mediterranean diet, cognitive function, and dementia: A systematic review. Epidemiology 2013, 24, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Veronese, N.; Vernuccio, L.; Catanese, G.; Inzerillo, F.; Salemi, G.; Barbagallo, M. Nutrition, Physical Activity, and Other Lifestyle Factors in the Prevention of Cognitive Decline and Dementia. Nutrients 2021, 13, 4080. [Google Scholar] [CrossRef]
- Liu, D.; Zhang, X.R.; Li, Z.H.; Zhang, Y.J.; Lv, Y.B.; Wang, Z.H.; Shen, D.; Chen, P.L.; Zhong, W.F.; Huang, Q.M.; et al. Association of dietary diversity changes and mortality among older people: A prospective cohort study. Clin. Nutr. 2021, 40, 2620–2629. [Google Scholar] [CrossRef] [PubMed]
- Qin, B.; Adair, L.S.; Plassman, B.L.; Batis, C.; Edwards, L.J.; Popkin, B.M.; Mendez, M.A.J.E. Dietary patterns and cognitive decline among Chinese older adults. Epidemiology 2015, 26, 758. [Google Scholar] [CrossRef]
- Titova, O.E.; Ax, E.; Brooks, S.J.; Sjogren, P.; Cederholm, T.; Kilander, L.; Kullberg, J.; Larsson, E.M.; Johansson, L.; Ahlstrom, H.; et al. Mediterranean diet habits in older individuals: Associations with cognitive functioning and brain volumes. Exp. Gerontol. 2013, 48, 1443–1448. [Google Scholar] [CrossRef]
- Roberts, R.O.; Geda, Y.E.; Cerhan, J.R.; Knopman, D.S.; Cha, R.H.; Christianson, T.J.H.; Pankratz, V.S.; Ivnik, R.J.; Boeve, B.F.; O’Connor, H.M.; et al. Vegetables, Unsaturated Fats, Moderate Alcohol Intake, and Mild Cognitive Impairment. Dement. Geriatr. Cogn. 2010, 29, 413–423. [Google Scholar] [CrossRef]
- Cherbuin, N.; Anstey, K.J. The Mediterranean diet is not related to cognitive change in a large prospective investigation: The PATH Through Life study. Am. J. Geriatr. Psychiatry 2012, 20, 635–639. [Google Scholar] [CrossRef]
- Gallucci, M.; Mazzuco, S.; Ongaro, F.; Di Giorgi, E.; Mecocci, P.; Cesari, M.; Albani, D.; Forloni, G.L.; Durante, E.; Gajo, G.B.; et al. Body mass index, lifestyles, physical performance and cognitive decline: The “Treviso Longeva (Trelong)” study. J. Nutr. Health Aging 2013, 17, 378–384. [Google Scholar] [CrossRef]
- Hosking, D.E.; Eramudugolla, R.; Cherbuin, N.; Anstey, K.J. MIND not Mediterranean diet related to 12-year incidence of cognitive impairment in an Australian longitudinal cohort study. Alzheimers Dement. 2019, 15, 581–589. [Google Scholar] [CrossRef]
- De Oliveira Otto, M.C.; Anderson, C.A.M.; Dearborn, J.L.; Ferranti, E.P.; Mozaffarian, D.; Rao, G.; Wylie-Rosett, J.; Lichtenstein, A.H.; American Heart Association Behavioral Change for Improving Health Factors Committee of the Council on Lifestyle and Cardiometabolic Health and Council on Epidemiology and Prevention; Council on Cardiovascular and Stroke Nursing; et al. Dietary Diversity: Implications for Obesity Prevention in Adult Populations: A Science Advisory From the American Heart Association. Circulation 2018, 138, e160–e168. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Smiciklas-Wright, H.; Guthrie, H.A.; Krebs-Smith, J. The effects of variety in food choices on dietary quality. J. Am. Diet. Assoc. 1987, 87, 897–903. [Google Scholar] [CrossRef]
- Milte, C.M.; McNaughton, S.A. Dietary patterns and successful ageing: A systematic review. Eur. J. Nutr. 2016, 55, 423–450. [Google Scholar] [CrossRef]
- Ruel, M.T. Operationalizing dietary diversity: A review of measurement issues and research priorities. J. Nutr. 2003, 133, 3911S–3926S. [Google Scholar] [CrossRef]
- Yin, Z.; Fei, Z.; Qiu, C.; Brasher, M.S.; Kraus, V.B.; Zhao, W.; Shi, X.; Zeng, Y. Dietary Diversity and Cognitive Function among Elderly People: A Population-Based Study. J. Nutr. Health Aging 2017, 21, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Record Owner, N.L.M. Dietary diversity decreases the risk of cognitive decline among Japanese older adults. Geriatr. Gerontol. Int. 2017, 17, 937–944. [Google Scholar] [CrossRef]
- Zheng, J.; Zhou, R.; Li, F.; Chen, L.; Wu, K.; Huang, J.; Liu, H.; Huang, Z.; Xu, L.; Yuan, Z.L.; et al. Association between dietary diversity and cognitive impairment among the oldest-old: Findings from a nationwide cohort study. Clin. Nutr. 2021, 40, 1452–1462. [Google Scholar] [CrossRef]
- Liu, D.; Zhang, W.T.; Wang, J.H.; Shen, D.; Zhang, P.D.; Li, Z.H.; Chen, P.L.; Zhang, X.R.; Huang, Q.M.; Zhong, W.F.; et al. Association between Dietary Diversity Changes and Cognitive Impairment among Older People: Findings from a Nationwide Cohort Study. Nutrients 2022, 14, 1251. [Google Scholar] [CrossRef]
- Zeng, Y.; Feng, Q.; Hesketh, T.; Christensen, K.; Vaupel, J.W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: A cohort study. Lancet 2017, 389, 1619–1629. [Google Scholar] [CrossRef]
- Lv, Y.-B.; Gao, X.; Yin, Z.-X.; Chen, H.-S.; Luo, J.-S.; Brasher, M.S.; Kraus, V.B.; Li, T.-T.; Zeng, Y.; Shi, X.-M. Revisiting the association of blood pressure with mortality in oldest old people in China: Community based, longitudinal prospective study. BMJ 2018, 361, k2158. [Google Scholar] [CrossRef]
- Goodkind, D.; Poston, D.L. Healthy Longevity in China: Demographic, Socioeconomic, and Psychological Dimensions. Pop. Stud-J. Demog. 2009, 63, 312–313. [Google Scholar]
- Zhao, W.H.; Huang, Z.P.; Zhang, X.; He, L.; Willett, W.; Wang, J.L.; Hasegawa, K.; Chen, J.S. Reproducibility and Validity of a Chinese Food Frequency Questionnaire. Biomed. Environ. Sci. 2010, 23, 1–38. [Google Scholar] [CrossRef]
- Zhao, W.H.; Hasegawa, K.; Chen, J.S. The use of food-frequency questionnaires for various purposes in China. Public Health Nutr. 2002, 5, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.B.; Kraus, V.B.; Gao, X.; Yin, Z.X.; Zhou, J.H.; Mao, C.; Duan, J.; Zeng, Y.; Brasher, M.S.; Shi, W.Y.; et al. Higher dietary diversity scores and protein-rich food consumption were associated with lower risk of all-cause mortality in the oldest old. Clin. Nutr. 2020, 39, 2246–2254. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Bhupathiraju, S.N.; Mattei, J.; Fung, T.T.; Li, Y.P.; Pan, A.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Association of Changes in Diet Quality with Total and Cause-Specific Mortality. N. Engl. J. Med. 2017, 377, 143–153. [Google Scholar] [CrossRef]
- An, R.; Liu, G.G. Cognitive impairment and mortality among the oldest-old Chinese. Int. J. Geriatr. Psychiatry 2016, 31, 1345–1353. [Google Scholar] [CrossRef]
- Wu, S.S.; Lv, X.Z.; Shen, J.; Chen, H.; Ma, Y.; Jin, X.R.; Yang, J.X.; Cao, Y.Y.; Zong, G.; Wang, H.L.; et al. Association between body mass index, its change and cognitive impairment among Chinese older adults: A community-based, 9-year prospective cohort study. Eur. J. Epidemiol. 2021, 36, 1043–1054. [Google Scholar] [CrossRef]
- Wang, J.N.; Li, T.T.; Lv, Y.B.; Kraus, V.B.; Zhang, Y.; Mao, C.; Yin, Z.X.; Shi, W.Y.; Zhou, J.H.; Zheng, T.Z.; et al. Fine Particulate Matter and Poor Cognitive Function among Chinese Older Adults: Evidence from a Community-Based, 12-Year Prospective Cohort Study. Environ. Health Persp. 2020, 128, 067013. [Google Scholar] [CrossRef]
- Liu, M.; He, P.; Zhou, C.; Zhang, Z.; Zhang, Y.; Li, H.; Ye, Z.; Wu, Q.; Yang, S.; Zhang, Y.; et al. Association of waist-calf circumference ratio with incident cognitive impairment in older adults. Am. J. Clin. Nutr. 2022, 115, 1005–1012. [Google Scholar] [CrossRef]
- Deng, Y.; Yang, T.; Gao, Q.; Yang, D.; Liu, R.; Wu, B.; Hu, L.; Liu, Y.; He, M. Cooking with biomass fuels increased the risk for cognitive impairment and cognitive decline among the oldest-old Chinese adults (2011–2018): A prospective cohort study. Environ. Int. 2021, 155, 106593. [Google Scholar] [CrossRef]
- Gopinath, B.; Schneider, J.; McMahon, C.M.; Teber, E.; Leeder, S.R.; Mitchell, P. Severity of age-related hearing loss is associated with impaired activities of daily living. Age Ageing 2012, 41, 195–200. [Google Scholar] [CrossRef]
- Romaniuk, H.; Patton, G.C.; Carlin, J.B. Multiple Imputation in a Longitudinal Cohort Study: A Case Study of Sensitivity to Imputation Methods. Am. J. Epidemiol. 2014, 180, 920–932. [Google Scholar] [CrossRef]
- Malloy, E.J.; Spiegelman, D.; Eisen, E.A. Comparing measures of model selection for penalized splines in Cox models. Comput. Stat. Data Anal. 2009, 53, 2605–2616. [Google Scholar] [CrossRef] [PubMed]
- Herring, A.H. Applied Longitudinal Analysis, 2nd Edition, by Garrett M. Fitzmaurice, Nan M. Laird, and James H. Ware, John Wiley & Sons, 2011. J. Biopharm. Stat. 2013, 23, 940–941. [Google Scholar] [CrossRef]
- van den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; van de Rest, O. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease—A Review. Adv. Nutr. 2019, 10, 1040–1065. [Google Scholar] [CrossRef] [PubMed]
- Malek Rivan, N.F.; Shahar, S.; Fakhruddin, N.; You, Y.X.; Che Din, N.; Rajikan, R. The effect of dietary patterns on mild cognitive impairment and dementia incidence among community-dwelling older adults. Front. Nutr. 2022, 9, 901750. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Bhupathiraju, S.N.; Mattei, J.; Fung, T.T.; Li, Y.; Pan, A.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Changes in Diet Quality Scores and Risk of Cardiovascular Disease Among US Men and Women. Circulation 2015, 132, 2212–2219. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Li, Y.; Satija, A.; Pan, A.; Sotos-Prieto, M.; Rimm, E.; Willett, W.C.; Hu, F.B. Association of changes in red meat consumption with total and cause specific mortality among US women and men: Two prospective cohort studies. BMJ 2019, 365, l2110. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Kyrozis, A.; Rossi, M.; Katsoulis, M.; Trichopoulos, D.; La Vecchia, C.; Lagiou, P. Mediterranean diet and cognitive decline over time in an elderly Mediterranean population. Eur. J. Nutr. 2015, 54, 1311–1321. [Google Scholar] [CrossRef]
- Feart, C.; Samieri, C.; Rondeau, V.; Amieva, H.; Portet, F.; Dartigues, J.F.; Scarmeas, N.; Barberger-Gateau, P. Adherence to a Mediterranean Diet, Cognitive Decline, and Risk of Dementia. JAMA-J. Am. Med. Assoc. 2009, 302, 638–648. [Google Scholar] [CrossRef]
- Martinez-Lapiscina, E.H.; Clavero, P.; Toledo, E.; Estruch, R.; Salas-Salvado, J.; San Julian, B.; Sanchez-Tainta, A.; Ros, E.; Valls-Pedret, C.; Martinez-Gonzalez, M.A. Mediterranean diet improves cognition: The PREDIMED-NAVARRA randomised trial. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1318–1325. [Google Scholar] [CrossRef] [PubMed]
- Aridi, Y.S.; Walker, J.L.; Wright, O.R.L. The Association between the Mediterranean Dietary Pattern and Cognitive Health: A Systematic Review. Nutrients 2017, 9, 674. [Google Scholar] [CrossRef] [PubMed]
- Kumawat, M.; Sharma, T.K.; Singh, I.; Singh, N.; Singh, S.K.; Ghalaut, V.S.; Shankar, V.; Vardey, S.K. Decrease in antioxidant status of plasma and erythrocytes from geriatric population. Dis. Markers 2012, 33, 303–308. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rajaram, S.; Jones, J.; Lee, G.J. Plant-Based Dietary Patterns, Plant Foods, and Age-Related Cognitive Decline. Adv. Nutr. 2019, 10, S422–S436. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Meckling, K.A.; Marcone, M.F.; Kakuda, Y.; Tsao, R. Synergistic, additive, and antagonistic effects of food mixtures on total antioxidant capacities. J. Agric. Food Chem. 2011, 59, 960–968. [Google Scholar] [CrossRef]
- Nani, A.; Murtaza, B.; Sayed Khan, A.; Khan, N.A.; Hichami, A. Antioxidant and Anti-Inflammatory Potential of Polyphenols Contained in Mediterranean Diet in Obesity: Molecular Mechanisms. Molecules 2021, 26, 985. [Google Scholar] [CrossRef]
- Shannon, O.M.; Ashor, A.W.; Scialo, F.; Saretzki, G.; Martin-Ruiz, C.; Lara, J.; Matu, J.; Griffiths, A.; Robinson, N.; Lilla, L.; et al. Mediterranean diet and the hallmarks of ageing. Eur. J. Clin. Nutr. 2021, 75, 1176–1192. [Google Scholar] [CrossRef]
- Moreira, P.L.; Villas Boas, P.J.; Ferreira, A.L. Association between oxidative stress and nutritional status in the elderly. Rev. Assoc. Med. Bras. 2014, 60, 75–83. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Dietary patterns, Mediterranean diet, and cardiovascular disease. Curr. Opin. Lipidol. 2014, 25, 20–26. [Google Scholar] [CrossRef]
- Grosso, G. Nutritional Psychiatry: How Diet Affects Brain through Gut Microbiota. Nutrients 2021, 13, 1282. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.J.; Vangay, P.; Al-Ghalith, G.A.; Hillmann, B.M.; Ward, T.L.; Shields-Cutler, R.R.; Kim, A.D.; Shmagel, A.K.; Syed, A.N.; Personalized Microbiome Class Students; et al. Daily Sampling Reveals Personalized Diet-Microbiome Associations in Humans. Cell Host Microbe 2019, 25, 789–802.e785. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Ma, K.; Wen, J.; Wang, G.; Zhang, C.; Li, Q.; Bao, X.; Wang, H. A Review of the Brain-Gut-Microbiome Axis and the Potential Role of Microbiota in Alzheimer’s Disease. J. Alzheimers Dis. 2020, 73, 849–865. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.; Chan, D.; Woo, J. A cross sectional study to examine the association between dietary patterns and cognitive impairment in older Chinese people in Hong Kong. J. Nutr. Health Aging 2013, 17, 757–765. [Google Scholar] [CrossRef]
- Chuang, S.Y.; Lo, Y.L.; Wu, S.Y.; Wang, P.N.; Pan, W.H. Dietary Patterns and Foods Associated With Cognitive Function in Taiwanese Older Adults: The Cross-sectional and Longitudinal Studies. J. Am. Med. Dir. Assoc. 2019, 20, 544–550.e4. [Google Scholar] [CrossRef]
- D’Amico, D.; Parrott, M.D.; Greenwood, C.E.; Ferland, G.; Gaudreau, P.; Belleville, S.; Laurin, D.; Anderson, N.D.; Kergoat, M.J.; Morais, J.A.; et al. Sex differences in the relationship between dietary pattern adherence and cognitive function among older adults: Findings from the NuAge study. Nutr. J. 2020, 19, 58. [Google Scholar] [CrossRef]
- Xiu, L.L.; Wahlqvist, M.L.; Lee, M.S.; Chen, R.C.Y.; Li, D. Cognitive impairment and limited dietary diversity or physical inactivity are conjoint precursors of incident diabetes more so in elderly women than men. Asia Pac. J. Clin. Nutr. 2013, 22, 635–645. [Google Scholar] [CrossRef]
- Soldan, A.; Pettigrew, C.; Zhu, Y.; Wang, M.C.; Gottesman, R.F.; DeCarli, C.; Albert, M.; Team, B.R. Cognitive reserve and midlife vascular risk: Cognitive and clinical outcomes. Ann. Clin. Transl. Neurol. 2020, 7, 1307–1317. [Google Scholar] [CrossRef]
- Lam, B.; Middleton, L.E.; Masellis, M.; Stuss, D.T.; Harry, R.D.; Kiss, A.; Black, S.E. Criterion and Convergent Validity of the Montreal Cognitive Assessment with Screening and Standardized Neuropsychological Testing. J. Am. Geriatr. Soc. 2013, 61, 2181–2185. [Google Scholar] [CrossRef]
- Hinkle, J.T.; Perepezko, K.; Bakker, C.C.; Dawson, T.M.; Johnson, V.; Mari, Z.; Marvel, C.L.; Mills, K.A.; Pantelyat, A.; Pletnikova, O.; et al. Domain-specific cognitive impairment in non-demented Parkinson’s disease psychosis. Int. J. Geriatr. Psychiatry 2018, 33, E131–E139. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total | DDS Change Patterns from Baseline to First Follow-Up | |||||
|---|---|---|---|---|---|---|---|
| High–High | High–Low | Low–High | Low–Low | DDS Change Score | p-Value | ||
| Number of participants (%) | 6237 | 1700 (27.3) | 1092 (17.5) | 1255 (20.1) | 2190 (35.1) | 0.12 ± 3.46 | |
| Age in years, mean (SD) | 88.55 (6.93) | 87.56 (6.59) | 88.50 (6.91) | 88.32 (6.66) | 89.48 (7.22) | 0.12 ± 3.46 | |
| Age group in years | 0.027 | ||||||
| 80–89 | 3698 (59.3) | 1094 (64.4) | 642 (58.8) | 756 (60.2) | 1206 (55.1) | 0.20 ± 3.46 | |
| ≥90 | 2539 (40.7) | 606 (35.6) | 450 (41.2) | 499 (39.8) | 984 (44.9) | 0.07 ± 3.56 | |
| Sex | 0.499 | ||||||
| Female | 3344 (53.6) | 734 (43.2) | 583 (53.4) | 689 (54.9) | 1338 (61.1) | 0.15 ± 3.45 | |
| Male | 2893 (46.4) | 966 (56.8) | 509 (46.6) | 566 (45.1) | 852 (38.9) | 0.09 ± 3.46 | |
| Type of residence | 0.002 | ||||||
| Urban | 3050 (48.9) | 1059 (62.3) | 507 (46.4) | 627 (50.0) | 857 (39.1) | 0.26 ± 3.50 | |
| Rural | 3187 (51.1) | 641 (37.7) | 585 (53.6) | 628 (50.0) | 1333 (60.9) | −0.02 ± 3.41 | |
| Marital status | 0.418 | ||||||
| In marriage | 1495 (24.0) | 516 (30.4) | 261 (23.9) | 286 (22.8) | 432 (19.7) | 0.18 ± 3.50 | |
| Not in marriage | 4742 (76.0) | 1184 (69.6) | 831 (76.1) | 969 (77.2) | 1758 (80.3) | 0.10 ± 3.45 | |
| Educational background | 0.939 | ||||||
| Illiteracy | 3680 (59.0) | 780 (45.9) | 635 (58.2) | 757 (60.3) | 1508 (68.9) | 0.11 ± 3.45 | |
| Literacy | 2557 (41.0) | 920 (54.1) | 457 (41.8) | 498 (39.7) | 682 (31.1) | 0.12 ± 3.46 | |
| Living pattern | 0.253 | ||||||
| With family members | 5084 (81.5) | 1451 (85.4) | 909 (83.2) | 1018 (81.1) | 1706 (77.9) | 0.09 ± 3.46 | |
| Alone or at nursing home | 1153 (18.5) | 249 (14.6) | 183 (16.8) | 237 (18.9) | 484 (22.1) | 0.22 ± 3.43 | |
| Tobacco smoking status | 0.045 † | ||||||
| Non-smoker | 3933 (63.1) | 966 (56.8) | 688 (63.0) | 799 (63.7) | 1480 (67.6) | 0.11 ± 3.47 | |
| Current smoker | 1261 (20.2) | 364 (21.4) | 242 (22.2) | 232 (18.5) | 423 (19.3) | −0.03 ± 3.42 | |
| Former smoker | 1043 (16.7) | 370 (21.8) | 162 (14.8) | 224 (17.8) | 287 (13.1) | 0.33 ± 3.47 | |
| Alcohol drinking status | 0.001 † | ||||||
| Non-drinker | 4005 (64.2) | 998 (58.7) | 713 (65.3) | 817 (65.1) | 1477 (67.4) | 0.18 ± 3.46 | |
| Current drinker | 1549 (24.8) | 500 (29.4) | 273 (25.0) | 284 (22.6) | 492 (22.5) | −0.16 ± 3.42 | |
| Former drinker | 683 (11.0) | 202 (11.9) | 106 (9.7) | 154 (12.3) | 221 (10.1) | 0.37 ± 3.48 | |
| Regular exercise | 0.001 | ||||||
| Yes | 2370 (38.0) | 889 (52.3) | 441 (40.4) | 423 (33.7) | 617 (28.2) | −0.07 ± 3.39 | |
| No | 3867 (62.0) | 811 (47.7) | 651 (59.6) | 832 (66.3) | 1573 (71.8) | 0.23 ± 3.50 | |
| Number of teeth, mean (SD) | 7.31 (11.82) | 8.75 (13.77) | 6.68 (10.39) | 7.62 (12.38) | 6.32 (10.32) | 0.12 ± 3.46 | |
| Use of artificial denture | 1681 (26.95) | 584 (34.35) | 301 (27.56) | 348 (27.73) | 448 (20.46) | 0.12 ± 3.46 | |
| BMI, mean (SD), Kg/m2 | 19.38 (5.43) | 19.46 (6.15) | 19.39 (5.53) | 19.44 (5.12) | 19.29 (4.94) | 0.12 ± 3.46 | |
| Hypertension | 898 (14.4) | 241 (14.2) | 153 (14.0) | 176 (14.0) | 328 (15.0) | −0.03 ± 3.46 | 0.158 |
| Diabetes | 62 (1.0) | 31 (1.8) | 9 (0.8) | 12 (1.0) | 10 (0.5) | 0.76 ± 3.71 | 0.142 |
| Hear disease | 438 (7.0) | 139 (8.2) | 74 (6.8) | 76 (6.1) | 149 (6.8) | −0.17 ± 3.72 | 0.069 |
| Cerebrovascular disease | 134 (2.1) | 37 (2.2) | 25 (2.3) | 29 (2.3) | 43 (2.0) | 0.07 ± 3.78 | 0.888 |
| Digestive disease | 217 (3.5) | 58 (3.4) | 47 (4.3) | 34 (2.7) | 78 (3.6) | −0.14 ± 3.58 | 0.270 |
| Cancer | 20 (0.3) | 7 (0.4) | 4 (0.4) | 1 (0.1) | 8 (0.4) | −1.10 ± 3.63 | 0.115 |
| Respiratory disease | 722 (11.6) | 216 (12.7) | 122 (11.2) | 141 (11.2) | 243 (11.1) | 0.27 ± 3.48 | 0.195 |
| Eye diseases | 894 (14.3) | 254 (14.9) | 183 (16.8) | 142 (11.3) | 315 (14.4) | −0.25 ± 3.42 | 0.001 |
| Duration of follow-up, months | 63.13 (38.71) | 68.62 (40.33) | 60.53 (37.93) | 67.05 (39.64) | 57.93 (36.43) | 0.12 ± 3.46 | |
| Events/Participants | Unadjusted Model | Model 1 † | Model 2 ‡ | ||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| DDS change (continuous) | 1829/6237 | 0.96 (0.95, 0.98) | 0.000 | 0.97 (0.96, 0.98) | 0.000 | 0.96 (0.95, 0.98) | 0.000 |
| Plant-based DDS change (continuous) | 1829/6237 | 0.96 (0.94, 0.98) | 0.000 | 0.96 (0.95, 0.98) | 0.000 | 0.96 (0.94, 0.97) | 0.000 |
| Animal-based DDS change (continuous) | 1829/6237 | 0.95 (0.92, 0.97) | 0.000 | 0.95 (0.93, 0.98) | 0.000 | 0.95 (0.92, 0.98) | 0.000 |
| DDS change pattern | |||||||
| Total DDS | |||||||
| High–high | 355/1700 | Reference | Reference | Reference | |||
| High–low | 347/1092 | 1.71 (1.47, 1.98) | 0.000 | 1.56 (1.35, 1.81) | <0.001 | 1.44 (1.24, 1.67) | <0.001 |
| Low–high | 329/1255 | 1.29 (1.11, 1.50) | 0.001 | 1.18 (1.01, 1.38) | 0.028 | 1.03 (0.88, 1.20) | 0.722 |
| Low–low | 798/2190 | 2.04 (1.80, 2.31) | 0.000 | 1.70 (1.50, 1.93) | <0.001 | 1.43 (1.25, 1.63) | <0.001 |
| Plant-based DDS | |||||||
| High–high | 304/1496 | Reference | Reference | Reference | |||
| High–low | 353/1157 | 1.664 (1.427, 1.940) | 0.000 | 1.52 (1.30, 1.77) | <0.001 | 1.43 (1.23, 1.67) | <0.001 |
| Low–high | 325/1217 | 1.37 (1.17, 1.60) | 0.000 | 1.24 (1.06, 1.46) | <0.001 | 1.11 (0.95, 1.30) | 0.201 |
| Low–low | 847/2367 | 2.05 (1.80, 2.34) | 0.000 | 1.66 (1.46, 1.90) | <0.001 | 1.44 (1.26, 1.65) | <0.001 |
| Animal-based DDS | |||||||
| High–high | 285/1214 | Reference | Reference | Reference | |||
| High–low | 294/986 | 0.65 (0.57, 0.74) | 0.000 | 1.30 (1.10, 1.53) | <0.001 | 1.18 (1.00, 1.39) | 0.047 |
| Low–high | 329/1267 | 0.88 (0.77, 1.00) | 0.048 | 1.11 (0.95, 1.30) | 0.205 | 0.98 (0.84, 1.16) | 0.840 |
| Low–low | 921/2770 | 0.72 (0.64, 0.82) | 0.000 | 1.46 (1.28, 1.67) | <0.001 | 1.22 (1.07, 1.40) | 0.004 |
| Subgroups | Events/Participants | DDS Change Patterns | p for Interaction | ||||
|---|---|---|---|---|---|---|---|
| DDS Change Score | High–High | High–Low | Low–High | Low–Low | |||
| Age (years) | |||||||
| 80–89 | 857/3698 | 0.96 (0.94, 0.98) ‡ | Ref. | 1.66 (1.34, 2.06) ‡ | 1.01 (0.81, 1.26) | 1.48 (1.22, 1.80) ‡ | 0.662 |
| ≥90 | 972/2539 | 0.96 (0.94, 0.98) ‡ | Ref. | 1.25 (1.02, 1.55) ‡ | 1.01 (0.82, 1.25) | 1.37 (1.14, 1.63) ‡ | |
| Gender | 0.854 | ||||||
| Male | 613/2893 | 0.97 (0.95, 0.99) ‡ | Ref. | 1.40 (1.09, 1.77) ‡ | 1.02 (0.80, 1.32) | 1.37 (1.10, 1.70) ‡ | |
| Female | 1216/3344 | 0.96 (0.95, 0.98) ‡ | Ref. | 1.45 (1.20, 1.76) ‡ | 1.02 (0.84, 1.24) | 1.44 (1.22, 1.71) ‡ | |
| Education | 0.948 | ||||||
| Illiterate | 1309/3680 | 0.96 (0.94, 0.99) ‡ | Ref. | 1.51 (1.25, 1.83) ‡ | 1.16 (0.96, 1.41) | 1.60 (1.36, 1.88) ‡ | |
| Literate | 520/2557 | 0.96 (0.95, 0.98) ‡ | Ref. | 1.36 (1.05, 1.75) ‡ | 0.94 (0.72, 1.23) | 1.28 (1.02, 1.62) | |
| Residence | 0.016 | ||||||
| Urban | 738/3050 | 0.97 (0.95, 0.99) ‡ | Ref. | 1.30 (1.04, 1.63) ‡ | 0.98 (0.79, 1.23) | 1.61 (1.33, 1.95) ‡ | |
| Rural | 1091/3187 | 0.96 (0.94, 0.98) ‡ | Ref. | 1.55 (1.26, 1.91) ‡ | 1.08 (0.87, 1.33) | 1.36 (1.13, 1.64) ‡ | |
| Smoking status | 0.296 | ||||||
| Current or former smoker | 545/2304 | 0.98 (0.96, 1.00) | Ref. | 1.29 (0.99, 1.68) ‡ | 1.08 (0.82, 1.41) | 1.43 (1.13, 1.81) ‡ | |
| Non-smoker | 1284/3933 | 0.96 (0.94, 0.97) ‡ | Ref. | 1.47 (1.22, 1.76) ‡ | 0.99 (0.83, 1.20) | 1.41 (1.2, 1.66) ‡ | |
| Drinking status | 0.117 | ||||||
| Current or former drinker | 591/2232 | 0.97 (0.95, 0.99) ‡ | Ref. | 1.59 (1.22, 2.07) ‡ | 1.20 (0.92, 1.56) | 1.67 (1.32, 2.12) ‡ | |
| Non-drinker | 1238/4005 | 0.96 (0.94, 0.98) ‡ | Ref. | 1.39 (1.15, 1.65) ‡ | 0.95 (0.79, 1.15) | 1.33 (1.13, 1.56) ‡ | |
| Regular exercise | 0.468 | ||||||
| Yes | 540/2370 | 0.96 (0.93, 0.98) ‡ | Ref. | 1.42 (1.11, 1.82) ‡ | 1.03 (0.79, 1.35) | 1.50 (1.20, 1.87) ‡ | |
| No | 1289/3867 | 0.97 (0.95, 0.98) ‡ | Ref. | 1.44 (1.19, 1.74) ‡ | 1.03 (0.86, 1.25) | 1.41 (1.20, 1.67) ‡ | |
| Living pattern | 0.671 | ||||||
| Living with family | 1505/5084 | 0.96 (0.95, 0.98) ‡ | Ref. | 1.41 (1.20, 1.66) ‡ | 1.0 (0.85, 1.18) | 1.43 (1.24, 1.64) ‡ | |
| Living alone | 324/1153 | 0.98 (0.95, 1.01) | Ref. | 1.73 (1.14, 2.61) ‡ | 1.31 (0.88, 1.95) | 1.58 (1.11, 2.25) ‡ | |
| Cognitive Domain | DDS Change Patterns | ||||||
|---|---|---|---|---|---|---|---|
| High–High | High–Low | Low–High | Low–Low | ||||
| Total DDS | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Global | Ref. | 1.27 (1.15, 1.40) | 0.000 | 0.93 (0.84, 1.03) | 0.200 | 1.12 (1.03, 1.23) | 0.008 |
| Orientation | Ref. | 1.23 (1.10, 1.38) | 0.000 | 1.00 (0.89, 1.11) | 0.925 | 1.24 (1.12, 1.36) | 0.000 |
| Registration | Ref. | 1.19 (1.07, 1.33) | 0.001 | 1.04 (0.94, 1.16) | 0.459 | 1.15 (1.04, 1.26) | 0.005 |
| Attention † | Ref. | 1.29 (1.16, 1.43) | 0.000 | 1.03 (0.93, 1.15) | 0.527 | 1.22 (1.12, 1.34) | 0.000 |
| Memory | Ref. | 1.15 (1.04, 1.27) | 0.005 | 0.96 (0.87, 1.06) | 0.379 | 1.05 (0.96, 1.14) | 0.291 |
| Language ‡ | Ref. | 1.26 (1.13, 1.39) | 0.000 | 1.00 (0.90, 1.11) | 0.981 | 1.17 (1.07, 1.28) | 0.001 |
| Plant-based DDS | |||||||
| Global | Ref. | 1.27 (1.15, 1.40) | 0.000 | 1.06 (0.95, 1.17) | 0.294 | 1.17 (1.07, 1.28) | 0.000 |
| Orientation | Ref. | 1.24 (1.11, 1.39) | 0.000 | 1.02 (0.91, 1.15) | 0.715 | 1.30 (1.18, 1.44) | 0.000 |
| Registration | Ref. | 1.15 (1.03, 1.28) | 0.015 | 1.04 (0.93, 1.17) | 0.453 | 1.16 (1.05, 1.28) | 0.003 |
| Attention † | Ref. | 1.28 (1.15, 1.42) | 0.000 | 1.14 (1.03, 1.27) | 0.014 | 1.25 (1.14, 1.37) | 0.000 |
| Memory | Ref. | 1.08 (0.97, 1.19) | 0.157 | 1.02 (0.92, 1.12) | 0.742 | 1.06 (0.97, 1.16) | 0.213 |
| Language ‡ | Ref. | 1.21 (1.09, 1.34) | 0.000 | 1.03 (0.92, 1.14) | 0.633 | 1.12 (1.02, 1.23) | 0.017 |
| Animal-based DDS | |||||||
| Global | Ref. | 1.21 (1.08, 1.34) | 0.001 | 0.94 (0.85, 1.05) | 0.260 | 1.09 (0.99, 1.19) | 0.073 |
| Orientation | Ref. | 1.05 (0.93, 1.19) | 0.444 | 1.01 (0.89, 1.13) | 0.924 | 1.09 (0.99, 1.21) | 0.091 |
| Registration | Ref. | 1.12 (0.99, 1.26) | 0.077 | 1.05 (0.93, 1.17) | 0.459 | 1.15 (1.04, 1.27) | 0.007 |
| Attention † | Ref. | 1.14 (1.02, 1.28) | 0.025 | 1.11 (1.0, 1.24) | 0.054 | 1.15 (1.05, 1.27) | 0.004 |
| Memory | Ref. | 0.98 (0.87, 1.09) | 0.669 | 1.01 (0.91, 1.12) | 0.820 | 1.02 (0.93, 1.12) | 0.614 |
| Language‡ | Ref. | 1.19 (1.06, 1.33) | 0.004 | 1.08 (0.96, 1.20) | 0.191 | 1.16 (1.06, 1.28) | 0.002 |
| DDS Change Patterns | MMSE Score-β | 95% CI | p-Value |
|---|---|---|---|
| Baseline | |||
| DDS change categories | |||
| High–high | Ref. | ||
| High–low | −0.403 | −0.755, −0.051 | 0.025 |
| Low–high | −0.202 | −0.134, 0.537 | 0.239 |
| Low–low | −0.286 | −0.585, −0.130 | 0.061 |
| Longitudinal | |||
| High–high × time | Ref. | ||
| High–low × time | −0.157 | −0.264, −0.050 | 0.004 |
| Low–high × time | −0.111 | −0.209, −0.014 | 0.025 |
| Low–low × time | −0.164 | −0.252, −0.076 | 0.000 |
| Event | Participants | Model 1 † | Model 2 ‡ | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |||
| DDS change (categorical) | 1829 | 6237 | ||||
| Large decline | 216 | 589 | 1.39 (1.20, 1.63) | 0.000 | 1.70 (1.44, 2.01) | 0.000 |
| Small decline | 402 | 1280 | 1.11 (0.98, 1.26) | 0.100 | 1.23 (1.08, 1.40) | 0.002 |
| Stable status | 651 | 2268 | Ref. | Ref. | Ref. | Ref. |
| Small improvement | 397 | 1483 | 0.91 (0.80, 1.03) | 0.125 | 0.83 (0.73, 0.94) | 0.003 |
| Large improvement | 163 | 617 | 0.97 (0.82, 1.15) | 0.721 | 0.75 (0.63, 0.90) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Y.; Zeng, L.; Gao, J.; Chen, L.; Sun, C.; Yan, M.; Li, M.; Jiang, H. Adherence to High Dietary Diversity and Incident Cognitive Impairment for the Oldest-Old: A Community-Based, Nationwide Cohort Study. Nutrients 2022, 14, 4530. https://doi.org/10.3390/nu14214530
Song Y, Zeng L, Gao J, Chen L, Sun C, Yan M, Li M, Jiang H. Adherence to High Dietary Diversity and Incident Cognitive Impairment for the Oldest-Old: A Community-Based, Nationwide Cohort Study. Nutrients. 2022; 14(21):4530. https://doi.org/10.3390/nu14214530
Chicago/Turabian StyleSong, Yangyang, Lu Zeng, Julin Gao, Lei Chen, Chuanhui Sun, Mengyao Yan, Mengnan Li, and Hongli Jiang. 2022. "Adherence to High Dietary Diversity and Incident Cognitive Impairment for the Oldest-Old: A Community-Based, Nationwide Cohort Study" Nutrients 14, no. 21: 4530. https://doi.org/10.3390/nu14214530
APA StyleSong, Y., Zeng, L., Gao, J., Chen, L., Sun, C., Yan, M., Li, M., & Jiang, H. (2022). Adherence to High Dietary Diversity and Incident Cognitive Impairment for the Oldest-Old: A Community-Based, Nationwide Cohort Study. Nutrients, 14(21), 4530. https://doi.org/10.3390/nu14214530