
Unhealthy Food Choices among Healthcare Shift Workers: A Cross-Sectional Study


 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Design and Sample Characteristics
2.3. Dietary Patterns Identification
2.4. Polish-Adapted Mediterranean Diet Score
2.5. Dietary Fat Intake Assessment
2.6. Confounders
2.7. Statistical Analysis
3. Results
3.1. Baseline Sample Characteristics
3.2. Dietary Patterns
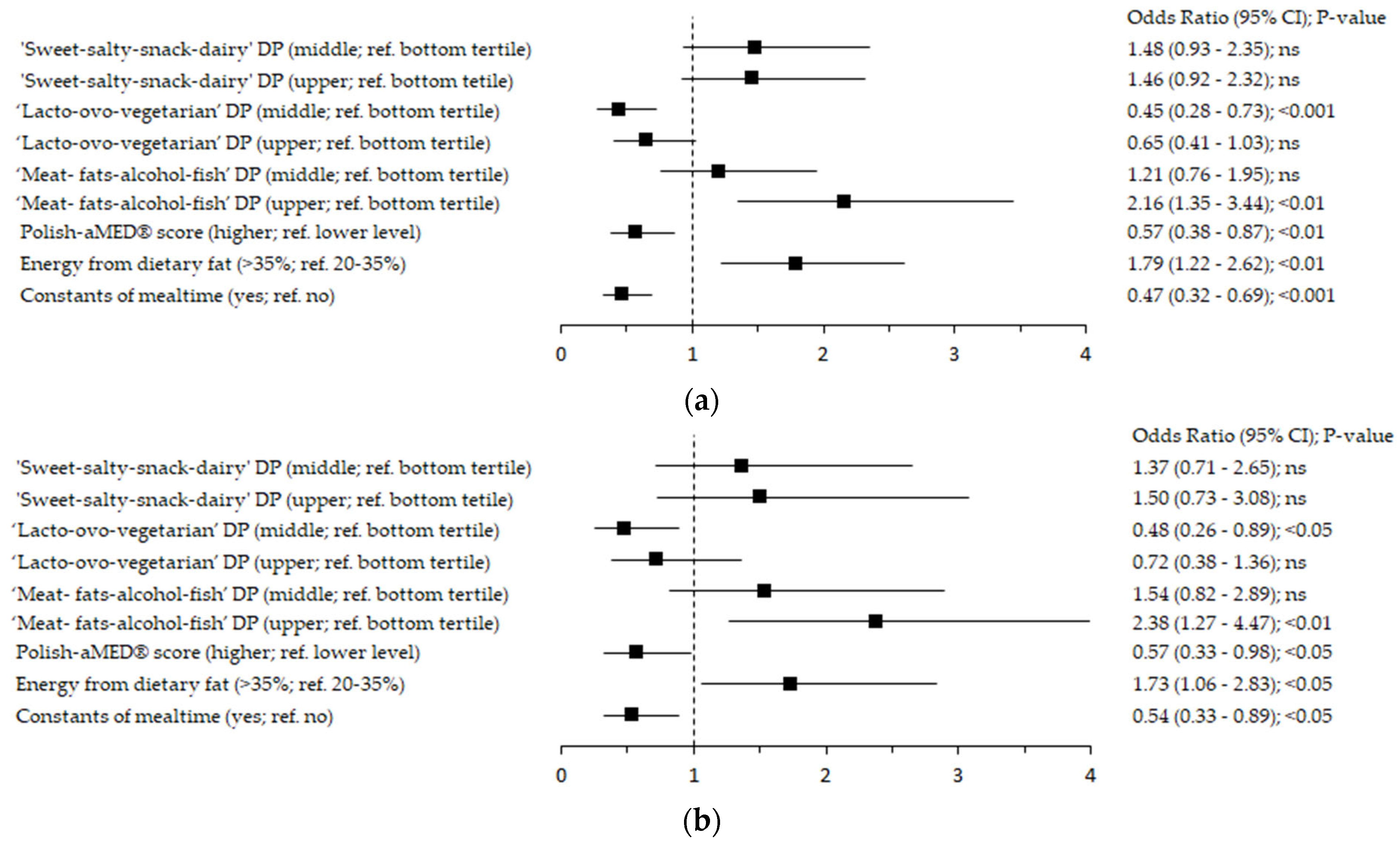
3.3. Food Choices and Fat Intake: Associations with Shift Work
4. Discussion
4.1. Mealtime among Healthcare Workers
4.2. Unhealthy Food Choices and Fat Intake among Shift Healthcare Workers
4.3. Pro-Healthy Dietary Patterns among Shift Healthcare Workers
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gacek, M. Selected Aspects of Life Style of Women with Secondaryand Higher Education Employed as Shift Workers. Med. Ogólna Nauk. O Zdrowiu 2018, 24, 25–30. [Google Scholar] [CrossRef]
- Kuleta, A. Wpływ pracy zmianowej na wystąpienie zmian patofizjologicznych—Przegląd literatury. Forum Zaburzeń Metab. 2016, 7, 93–98. [Google Scholar]
- Costa, G. Shift Work and Occupational Medicine: An Overview. Occup. Med. 2003, 53, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Leka, S.; Jain, A.; Orlak, K. Zdrowa Praca Zagrozenia Psychospoleczne w Srodowisku Pracy i ich Wplyw na Zdrowie; Stowarzyszenie Zdrowa Praca: Warszawa, Poland, 2013; ISBN 978-83-936081-0-2. [Google Scholar]
- Lewandowski, J. Epidemiologia Nadciśnienia Tętniczego Oraz Badanie Chorego Na Nadciśnienie Tętnicze. Przew Lek 2010, 4, 30–35. [Google Scholar]
- Dzierżewicz, Z.; Balwierz, R.; Marciniak, D.; Sarecka-Hujar, B.; Delijewski, M.; Dolińska, B. Plejotropowe Działanie Melatoniny. Med. Rodz. 2018, 21. [Google Scholar] [CrossRef]
- Pawlak, J.; Pawlak, B.; Zalewski, P.; Bitner, A. Praca Zmianowa a Powstawanie Chorób Układu Sercowonaczyniowego w Kontekście Regulacji Normatywnej. Hygeia Public Health 2013, 48, 6–9. [Google Scholar]
- Liu, W.; Zhou, Z.; Dong, D.; Sun, L.; Zhang, G. Sex Differences in the Association between Night Shift Work and the Risk of Cancers: A Meta-Analysis of 57 Articles. Dis. Markers 2018, 2018, 7925219. [Google Scholar] [CrossRef]
- Roenneberg, T.; Merrow, M. The Network of Time: Understanding the Molecular Circadian System. Curr. Biol. 2003, 13, R198–R207. [Google Scholar] [CrossRef]
- Waterhouse, J.; Minors, D.; Atkinson, G.; Benton, D. Chronobiology and Meal Times: Internal and External Factors. Br. J. Nutr. 1997, 77, S29–S38. [Google Scholar] [CrossRef]
- Keogh, K. Shift Work and Vending Machines to Blame for Poor Workplace Diet: Nurses Are Struggling with Their Weight as the Pressures of the Job Leave Little Time for Healthy Eating, a Nursing Standard Survey Reveals. Kat Keogh Reports. Nurs. Stand. 2014, 29, 14–15. [Google Scholar] [CrossRef]
- Hulsegge, G.; Boer, J.M.; van der Beek, A.J.; Verschuren, W.M.; Sluijs, I.; Vermeulen, R.; Proper, K.I. Shift Workers Have a Similar Diet Quality but Higher Energy Intake than Day Workers. Scand. J. Work. Environ. Health 2016, 42, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, J.d.C.; Portela, L.F.; Rotenberg, L.; Griep, R.H. Working Hours and Health Behaviour among Nurses at Public Hospitals. Rev. Lat. Am. Enferm. 2013, 21, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Tucker, K.L. Empirically Derived Eating Patterns Using Factor or Cluster Analysis: A Review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Canuto, R.; Garcez, A.; Spritzer, P.M.; Olinto, M.T.A. Associations of Perceived Stress and Salivary Cortisol with the Snack and Fast-Food Dietary Pattern in Women Shift Workers. Stress 2021, 24, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Khorasaniha, R.; Siassi, F.; Khajehnasiri, F.; Qorbani, M.; Sotoudeh, G. Dietary Patterns in Relation to Inflammation in Shift Workers. BMJ Mil Health 2020, 166, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Mota, M.C.; Waterhouse, J.; De-Souza, D.A.; Rossato, L.T.; Silva, C.M.; Araújo, M.B.J.; Tufik, S.; de Mello, M.T.; Crispim, C.A. Sleep Pattern Is Associated with Adipokine Levels and Nutritional Markers in Resident Physicians. Chronobiol. Int. 2014, 31, 1130–1138. [Google Scholar] [CrossRef]
- Mortaş, H.; Bilici, S.; Öztürk, H.; Karakan, T. Changes in Intestinal Parameters and Their Association with Dietary Patterns in Rotational Shift Workers. Chronobiol. Int. 2022, 39, 872–885. [Google Scholar] [CrossRef]
- Niedzwiedzka, E.; Wadolowska, L.; Kowalkowska, J. Reproducibility of A Non-Quantitative Food Frequency Questionnaire (62-Item FFQ-6) and PCA-Driven Dietary Pattern Identification in 13–21-Year-Old Females. Nutrients 2019, 11, 2183. [Google Scholar] [CrossRef]
- Krusinska, B.; Hawrysz, I.; Wadolowska, L.; Slowinska, M.; Biernacki, M.; Czerwinska, A.; Golota, J. Associations of Mediterranean Diet and a Posteriori Derived Dietary Patterns with Breast and Lung Cancer Risk: A Case-Control Study. Nutrients 2018, 10, 470. [Google Scholar] [CrossRef]
- Stachowska, E.; Ryterska, K.; Maciejewska, D.; Banaszczak, M.; Milkiewicz, P.; Milkiewicz, M.; Gutowska, I.; Ossowski, P.; Kaczorowska, M.; Jamioł-Milc, D.; et al. Nutritional Strategies for the Individualized Treatment of Non-Alcoholic Fatty Liver Disease (NAFLD) Based on the Nutrient-Induced Insulin Output Ratio (NIOR). Int. J. Mol. Sci. 2016, 17, 1192. [Google Scholar] [CrossRef]
- Armitage, C.J.; Conner, M. Efficacy of the Theory of Planned Behaviour: A Meta-Analytic Review. Br. J. Soc. Psychol. 2001, 40, 471–499. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute, Division of Cancer Control and Population Sciences—Percentage En-Ergy from Fat Screener: Scoring Procedures. Available online: https://Epi.Grants.Cancer.Gov/Diet/Screeners/Fat/Scoring.Html (accessed on 22 July 2022).
- Katherine, S.T.; Linda, E. Cleveland Results from USDA’s 1994-96 Diet and Health Knowledge Survey; US Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2001. [Google Scholar]
- Stasiewicz, B.; Wadolowska, L.; Biernacki, M.; Slowinska, M.A.; Stachowska, E. Dietary Fat Intake: Associations with Dietary Patterns and Postmenopausal Breast Cancer-A Case-Control Study. Cancers 2022, 14, 1724. [Google Scholar] [CrossRef] [PubMed]
- Gaston Godin The Godin Shephard Leisure Time Physical Activity Questionnaire. Health Fit. J. Can. 2011, 4, 18–22.
- Krupa-Kozak, U.; Drabińska, N.; Jarocka-Cyrta, E. The Effect of Oligofructose-Enriched Inulin Supplementation on Gut Microbiota, Nutritional Status and Gastrointestinal Symptoms in Paediatric Coeliac Disease Patients on a Gluten-Free Diet: Study Protocol for a Pilot Randomized Controlled Trial. Nutr. J. 2017, 16, 47. [Google Scholar] [CrossRef]
- Ahmed, S.; Rahman, T.; Ripon, M.S.H.; Rashid, H.-U.; Kashem, T.; Md Ali, M.S.; Khor, B.-H.; Khosla, P.; Karupaiah, T.; Daud, Z.A.M. A Food Frequency Questionnaire for Hemodialysis Patients in Bangladesh (BDHD-FFQ): Development and Validation. Nutrients 2021, 13, 4521. [Google Scholar] [CrossRef]
- Filipczuk, A.; Wrońska, I. Promocja Zdrowia Wśród Pracowników Ochrony Zdrowia. Ann. UMCS 2003, 58. [Google Scholar]
- Sokołowska, B.; Samoszuk, T.; Piaszczyk, D. Styl Życia a Odżywianie Pielęgniarek Jako Jeden z Wyznaczników Programu Promocji Zdrowia. Ann. UMCS 2003, 58, 152. [Google Scholar]
- Gawęcki, J.; Mossor-Pietraszewska, T. Kompendium Wiedzy o Żywności, Żywieniu i Zdrowiu; PWN: Warszawa, Poland, 2014. [Google Scholar]
- Jarosz, M.; Respondek, W.; Wolnicka, W. Zalecenia Dotyczące Żywienia i Aktywności Fizycznej; Jarosz, M., Ed.; Normy Żywienia Dla Populacji Polskiej—Nowelizacja; Instytut Żywności i Żywienia: Warszawa, Poland, 2012. [Google Scholar]
- Jeżewska-Zychowicz, M. Zachowania Żywieniowe i Ich Uwarunkowania; Wydawnictwo Szkoły Głównej Gospodarstwa Wiejskiego: Warszawa, Poland, 2007. [Google Scholar]
- Łokieć, K.; Górska-Ciebiada, M. Nutritional Behaviours of Shift Workers. Med. Ogólna Nauk. O Zdrowiu 2020, 26, 213–220. [Google Scholar] [CrossRef]
- Sińska, B.; Kucharska, A.; Dykowska, G. Zakład Ekonomiki i Prawa, Warszawski Uniwersytet Medyczny, Warszawa, Polska Wpływ Systemu Zmianowego Pracy Pielęgniarek Na Ich Sposób Odżywiania i Aktywność Fizyczną. Zdr. Publiczne Zarządzanie 2018, 16, 105–111. [Google Scholar] [CrossRef]
- Siedlecka, J. Selected work-related health problems in drivers of public transport vehicles. Med. Pr. 2006, 57, 47–52. (In Polish) [Google Scholar]
- Kochan, Z.; Karbowska, J.; Babicz-Zielińska, E. Dietary trans-fatty acids and metabolic syndrome. Postep. Hig. Med. Dosw. Online 2010, 64, 650–658. [Google Scholar]
- Beunza, J.-J.; Toledo, E.; Hu, F.B.; Bes-Rastrollo, M.; Serrano-Martínez, M.; Sánchez-Villegas, A.; Martínez, J.A.; Martínez-González, M.A. Adherence to the Mediterranean Diet, Long-Term Weight Change, and Incident Overweight or Obesity: The Seguimiento Universidad de Navarra (SUN) Cohort. Am. J. Clin. Nutr. 2010, 92, 1484–1493. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Barrajón-Catalán, E.; Herranz-López, M.; Joven, J.; Segura-Carretero, A.; Alonso-Villaverde, C.; Menéndez, J.A.; Micol, V. Molecular Promiscuity of Plant Polyphenols in the Management of Age-Related Diseases: Far Beyond Their Antioxidant Properties. In Oxidative Stress and Inflammation in Non-Communicable Diseases—Molecular Mechanisms and Perspectives in Therapeutics; Camps, J., Ed.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Switzerland, 2014; Volume 824, pp. 141–159. ISBN 978-3-319-07319-4. [Google Scholar]
- Joven, J.; Micol, V.; Segura-Carretero, A.; Alonso-Villaverde, C.; Menéndez, J.A.; for the Bioactive Food Components Platform. Polyphenols and the Modulation of Gene Expression Pathways: Can We Eat Our Way Out of the Danger of Chronic Disease? Crit. Rev. Food Sci. Nutr. 2014, 54, 985–1001. [Google Scholar] [CrossRef]
- Bouvard, V.; Loomis, D.; Guyton, K.Z.; Grosse, Y.; Ghissassi, F.E.; Benbrahim-Tallaa, L.; Guha, N.; Mattock, H.; Straif, K. Carcinogenicity of Consumption of Red and Processed Meat. Lancet Oncol. 2015, 16, 1599–1600. [Google Scholar] [CrossRef]
- Zeraatkar, D.; Han, M.A.; Guyatt, G.H.; Vernooij, R.W.M.; El Dib, R.; Cheung, K.; Milio, K.; Zworth, M.; Bartoszko, J.J.; Valli, C.; et al. Red and Processed Meat Consumption and Risk for All-Cause Mortality and Cardiometabolic Outcomes: A Systematic Review and Meta-Analysis of Cohort Studies. Ann. Intern. Med. 2019, 171, 703. [Google Scholar] [CrossRef]
- Han, M.A.; Zeraatkar, D.; Guyatt, G.H.; Vernooij, R.W.M.; El Dib, R.; Zhang, Y.; Algarni, A.; Leung, G.; Storman, D.; Valli, C.; et al. Reduction of Red and Processed Meat Intake and Cancer Mortality and Incidence: A Systematic Review and Meta-Analysis of Cohort Studies. Ann. Intern. Med. 2019, 171, 711. [Google Scholar] [CrossRef]
- Vernooij, R.W.M.; Zeraatkar, D.; Han, M.A.; El Dib, R.; Zworth, M.; Milio, K.; Sit, D.; Lee, Y.; Gomaa, H.; Valli, C.; et al. Patterns of Red and Processed Meat Consumption and Risk for Cardiometabolic and Cancer Outcomes: A Systematic Review and Meta-Analysis of Cohort Studies. Ann. Intern. Med. 2019, 171, 732. [Google Scholar] [CrossRef]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Aboyans, V.; et al. Global, Regional, and National Comparative Risk Assessment of 84 Behavioural, Environmental and Occupational, and Metabolic Risks or Clusters of Risks, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Di Bella, G.; Veronese, N.; Barbagallo, M. Impact of Mediterranean Diet on Chronic Non-Communicable Diseases and Longevity. Nutrients 2021, 13, 2028. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-López, M.; Bes-Rastrollo, M.; Toledo, E.; Martínez-Lapiscina, E.H.; Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J.J. Mediterranean Diet and the Incidence of Cardiovascular Disease: A Spanish Cohort. Nutr. Metab. Cardiovasc. Dis. 2010, 21, 237–244. [Google Scholar] [CrossRef]
- Ma, W.; Nguyen, L.H.; Song, M.; Wang, D.D.; Franzosa, E.A.; Cao, Y.; Joshi, A.; Drew, D.A.; Mehta, R.; Ivey, K.L.; et al. Dietary Fiber Intake, the Gut Microbiome, and Chronic Systemic Inflammation in a Cohort of Adult Men. Genome Med. 2021, 13, 102. [Google Scholar] [CrossRef]


{kind=link}
| Socioeconomic Factors | Categories | Scoring |
|---|---|---|
| Place of residence | Village | 1 |
| Town <50,000 inhabitants | 2 | |
| City 50,000–200,000 inhabitants | 3 | |
| City >200,000 inhabitants | 4 | |
| Educational level | Primary | 1 |
| Secondary | 2 | |
| Higher | 3 | |
| Situation of household (self-declared) | We live very poorly—we do not have enough resources even for basic needs (food/clothing/housing fees) | 1 |
| We live poorly—we only have enough resources for the cheapest food and clothing, but not for housing fees | 2 | |
| We live poorly—after paying the housing fees, we only have enough resources for the cheapest food and clothing | 3 | |
| We live very thriftily—we only have enough resources for basic needs (food/clothing/housing fees) | 4 | |
| We live thriftily—we have enough resources for everything | 5 | |
| We live well—we have enough resources for everything, without any special restrictions | 6 |
| Variables | Total Sample | Mode of the Work | p-Value | |
|---|---|---|---|---|
| Shift | Daily | |||
| Sample Size (n) | 445 | 193 | 252 | |
| Gender | ||||
| Men | 20.0 | 16.6 | 22.6 | 0.1145 |
| Women | 80.0 | 83.4 | 77.4 | |
| Age (years #) | 35.4 ± 10.9 | 34.0 ± 11.0 | 36.4 ±10.7 | 0.0188 |
| <30.0 | 42.2 | 50.3 | 36.1 | |
| 30.0–39.9 | 27.4 | 22.8 | 31.0 | 0.0164 |
| 40.0–49.9 | 17.5 | 14.0 | 20.2 | |
| ≥50.0 | 12.8 | 13.0 | 12.7 | |
| Place of residence | ||||
| Village | 14.8 | 14.5 | 15.1 | |
| Town <50,000 inhabitants | 14.6 | 17.6 | 12.3 | 0.0872 |
| City (50,000–200,000 inhabitants) | 18.4 | 21.8 | 15.9 | |
| City (>200,000 inhabitants) | 52.1 | 46.1 | 56.7 | |
| Educational level | ||||
| Primary | 0.5 | 0.5 | 0.4 | |
| Secondary | 6.8 | 7.8 | 6.0 | 0.7256 |
| Higher | 92.8 | 91.7 | 93.7 | |
| Situation of household | ||||
| We live poorly—after paying the housing fees, we have enough resources only for the cheapest food and clothing | 1.6 | 1.6 | 1.6 | |
| We live very thriftily—we have enough resources only for basic needs (food/clothing/housing fees) | 9.7 | 13.0 | 7.2 | 0.0495 |
| We live thriftily—so we have enough resources for everything | 33.5 | 37.0 | 30.8 | |
| We live well—we have enough resources for everything, without any special restrictions | 55.2 | 48.4 | 60.4 | |
| Socioeconomic status (SES Index, points #) | 11.4 ± 1.5 | 11.2 ± 1.4 | 11.6 ± 1.5 | 0.0045 |
| Low (3–6) | 0.5 | 0.0 | 0.8 | |
| Average (7–10) | 26.5 | 29.8 | 24.0 | 0.1922 |
| High (11–13) | 73.0 | 70.2 | 75.2 | |
| BMI (kg/m2 #) | 24.2 ± 3.0 | 24.2 ± 3.2 | 24.3 ± 2.9 | 0.7891 |
| Underweight (<18.5) | 1.4 | 2.6 | 0.4 | |
| Normal weight (18.5–24.9) | 55.0 | 54.4 | 55.4 | |
| Overweight (25.0–29.9) | 40.3 | 38.9 | 41.4 | 0.1974 |
| Obesity (≥30) | 3.4 | 4.1 | 2.8 | |
| Chronic diseases | 38.2 | 33.5 | 41.8 | 0.0772 |
| Taking medication >1 year | 31.5 | 25.9 | 35.7 | 0.0272 |
| Physical activity 1 | ||||
| GLTEQ (summary points #) | 36.3 ± 28.4 | 36.4 ± 29.5 | 36.3 ± 27.2 | 0.8274 |
| GLTEQ (strenuous and moderate points #) | 27.8 ± 24.4 | 28.1 ± 25.1 | 27.4 ± 23.6 | 0.9711 |
| Insufficiently active (<14 points) | 30.3 | 30.7 | 29.9 | |
| Moderately active (14–23 points) | 20.3 | 20.5 | 20.1 | 0.9780 |
| Active (≥24 points) | 49.3 | 48.8 | 50.0 | |
| Alcohol drinking | ||||
| Within the 12 last months | 35.4 | 33.9 | 36.5 | 0.5623 |
| Within the last 10 years | 75.2 | 74.9 | 75.4 | 0.8987 |
| Smoking status (smoker 2) | 54.7 | 55.4 | 54.2 | 0.7919 |
| Current smoker | ||||
| No | 83.5 | 83.8 | 83.3 | |
| Yes, up to 5 cigarettes/day | 6.3 | 6.3 | 6.3 | |
| Yes, up to 10 cigarettes/day | 6.5 | 7.3 | 6.0 | 0.7356 |
| Yes, up to 20 cigarettes/day | 2.7 | 1.6 | 3.6 | |
| Yes, up >20 cigarettes/day | 0.9 | 1.0 | 0.8 | |
| Vitamin/mineral supplements use 3 | 70.8 | 65.3 | 75.0 | 0.0255 |
| Food Groups | PCA-Derived Dietary Patterns | Polish-aMED® Score | ||
|---|---|---|---|---|
| ‘Sweet-Salty-Snack-Dairy’ | ‘Lacto-Ovo-Vegetarian’ | ‘Meat- Fats-Alcohol-Fish’ | ||
| Sweetened milk drinks and flavored cheese | 0.72 | 0.06 | 0.07 | −0.03 |
| Salty snacks | 0.66 | −0.07 | 0.19 | −0.06 |
| Sugar, honey, and sweets | 0.62 | −0.08 | 0.23 | −0.15 * |
| Refined grains | 0.52 | 0.03 | 0.21 | −0.08 |
| Breakfast cereals | 0.52 | 0.01 | −0.14 | 0.00 |
| Milk, fermented milk drinks, and cheese curd | 0.49 | 0.43 | −0.19 | 0.27 * |
| Cheese | 0.45 | 0.22 | 0.19 | 0.11 * |
| Sweetened beverages | 0.40 | −0.28 | 0.28 | −0.22 * |
| Animal fats | 0.34 | 0.14 | 0.55 | −0.16 * |
| Potatoes | 0.31 | 0.23 | 0.29 | 0.08 |
| Vegetables | 0.00 | 0.77 | −0.04 | 0.69 * |
| Fruits | 0.07 | 0.65 | −0.06 | 0.51 * |
| Whole grains | −0.02 | 0.65 | −0.05 | 0.58 * |
| Legumes | −0.11 | 0.62 | 0.12 | 0.49 * |
| Nuts and seeds | −0.05 | 0.62 | 0.16 | 0.45 * |
| Vegetable oils (including olive oil) | 0.15 | 0.44 | 0.31 | 0.30 * |
| Eggs | 0.23 | 0.41 | 0.20 | 0.20 * |
| Processed meats | 0.22 | −0.14 | 0.69 | −0.31 * |
| Other fats (margarine, mayonnaise, dressings) | 0.26 | −0.04 | 0.61 | −0.13 * |
| White meat | 0.09 | 0.13 | 0.60 | 0.02 |
| Alcoholic drinks | 0.03 | 0.03 | 0.60 | −0.03 |
| Fish | −0.12 | 0.28 | 0.54 | 0.28 * |
| Fruit, vegetable or vegetable-fruit juices | 0.24 | −0.02 | 0.20 | −0.09 |
| Ratio of vegetable oils to animal fats | NA | NA | NA | 0.18 * |
| Share in explaining the variance (%) | 18.6 | 12.5 | 7.3 | NA |
| Variables | Total Sample | Mode of the Work | p-Value | |
|---|---|---|---|---|
| Shift | Daily | |||
| Sample Size | 445 | 193 | 252 | |
| PCA-derived dietary patterns (tertiles) | ||||
| ‘Sweet-salty-snack-dairy’ | ||||
| Bottom | 33.3 | 28.5 | 36.9 | |
| Middle | 33.3 | 35.8 | 31.3 | 0.1752 |
| Upper | 33.5 | 35.8 | 31.7 | |
| ‘Lacto-ovo-vegetarian’ | ||||
| Bottom | 33.3 | 40.9 | 27.4 | |
| Middle | 33.5 | 26.4 | 38.9 | 0.0038 |
| Upper | 33.3 | 32.6 | 33.7 | |
| ‘Meat- fats-alcohol-fish’ | ||||
| Bottom | 33.5 | 27.5 | 38.1 | |
| Middle | 33.0 | 30.6 | 34.9 | 0.0030 |
| Upper | 33.5 | 42.0 | 27.0 | |
| Polish-amed® score (points) # | 3.9 ± 1.7 | 3.5 ± 1.8 | 4.1 ± 1.6 | 0.0001 |
| Levels (points) | ||||
| Lower (0–4) | 66.7 | 73.6 | 61.5 | |
| Higher (5–8) | 33.3 | 26.4 | 38.5 | 0.0074 |
| Total fat intake (g) # | 3.4 ± 4.8 | 4.1 ± 5.4 | 2.9 ± 4.2 | 0.0395 |
| Regular fat intake (g) # | 3.1 ± 4.5 | 3.7 ± 5.0 | 2.7 ± 4.0 | 0.1546 |
| Percentage energy from dietary fat # | 35.4 ± 5.9 | 36.4 ± 6.4 | 34.6 ± 5.4 | 0.0013 |
| 20–35% | 57.8 | 49.7 | 63.9 | |
| >35% | 42.2 | 50.3 | 36.1 | 0.0028 |
| Number of meals | ||||
| 1–2 | 8.3 | 9.3 | 7.5 | |
| 3 | 27.9 | 29.0 | 27.0 | 0.7367 |
| 4 | 44.3 | 41.5 | 46.4 | |
| ≥5 | 19.6 | 20.2 | 19.0 | |
| Constants of mealtime (yes) | 54.6 | 44.0 | 62.7 | <0.0001 |
| Special diet or intake restrictions | 40.8 | 34.2 | 45.8 | 0.0135 |
| Overall decrease in food consumption | 74.6 | 72.5 | 76.2 | 0.3805 |
| Restriction in consumption of: | ||||
| Dairy | 29.1 | 21.8 | 34.7 | 0.0030 |
| Fish | 16.9 | 14.5 | 18.8 | 0.2323 |
| Fruits | 9.7 | 5.7 | 12.7 | 0.0128 |
| Raw vegetables | 5.2 | 4.2 | 6.0 | 0.4003 |
| Fats | 54.2 | 50.3 | 57.2 | 0.1460 |
| Foods in high fat content | 64.3 | 60.1 | 67.5 | 0.1085 |
| Sugar and sweets | 70.7 | 66.1 | 74.1 | 0.0683 |
| Potatoes and cereals | 29.9 | 21.8 | 36.1 | 0.0011 |
| Meat and meat products | 42.9 | 33.2 | 50.4 | 0.0003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolska, A.; Stasiewicz, B.; Kaźmierczak-Siedlecka, K.; Ziętek, M.; Solek-Pastuszka, J.; Drozd, A.; Palma, J.; Stachowska, E. Unhealthy Food Choices among Healthcare Shift Workers: A Cross-Sectional Study. Nutrients 2022, 14, 4327. https://doi.org/10.3390/nu14204327
Wolska A, Stasiewicz B, Kaźmierczak-Siedlecka K, Ziętek M, Solek-Pastuszka J, Drozd A, Palma J, Stachowska E. Unhealthy Food Choices among Healthcare Shift Workers: A Cross-Sectional Study. Nutrients. 2022; 14(20):4327. https://doi.org/10.3390/nu14204327
Chicago/Turabian StyleWolska, Anna, Beata Stasiewicz, Karolina Kaźmierczak-Siedlecka, Maciej Ziętek, Joanna Solek-Pastuszka, Arleta Drozd, Joanna Palma, and Ewa Stachowska. 2022. "Unhealthy Food Choices among Healthcare Shift Workers: A Cross-Sectional Study" Nutrients 14, no. 20: 4327. https://doi.org/10.3390/nu14204327
APA StyleWolska, A., Stasiewicz, B., Kaźmierczak-Siedlecka, K., Ziętek, M., Solek-Pastuszka, J., Drozd, A., Palma, J., & Stachowska, E. (2022). Unhealthy Food Choices among Healthcare Shift Workers: A Cross-Sectional Study. Nutrients, 14(20), 4327. https://doi.org/10.3390/nu14204327