
Longitudinal Analysis of Quadriceps Muscle Strength in Patients with Previous COVID-19 Hospitalization and in Patients with Post-Acute Sequelae following Mild COVID-19

Abstract
1. Introduction
2. Materials and Methods
2.1. Quadriceps Muscle Strength Assessment
2.2. Acute COVID-19 Severity Markers
2.3. Data Collection and Measurements at Visit 1
2.4. Muscle Ultrasound
2.5. Statistical Analysis
3. Results
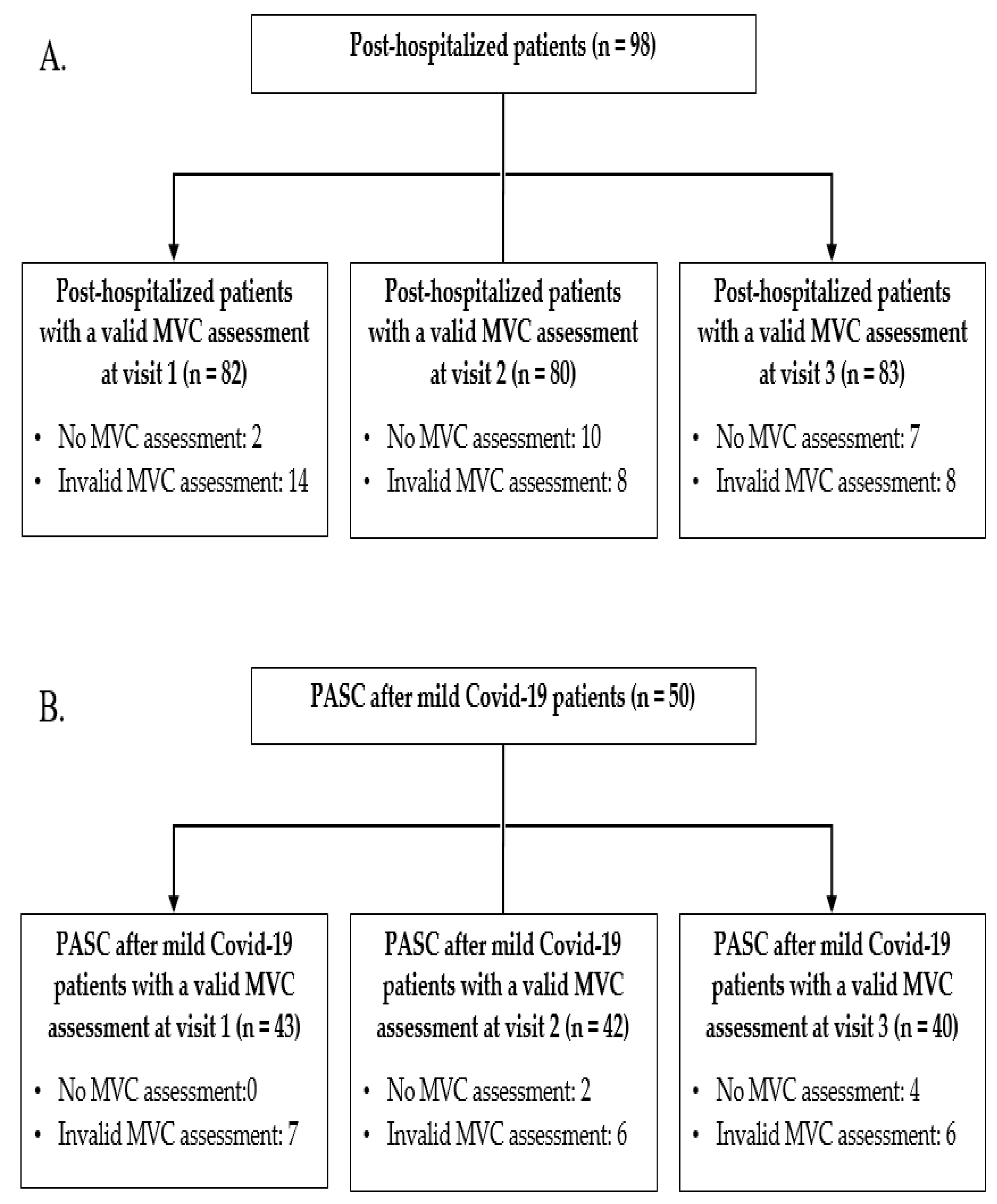
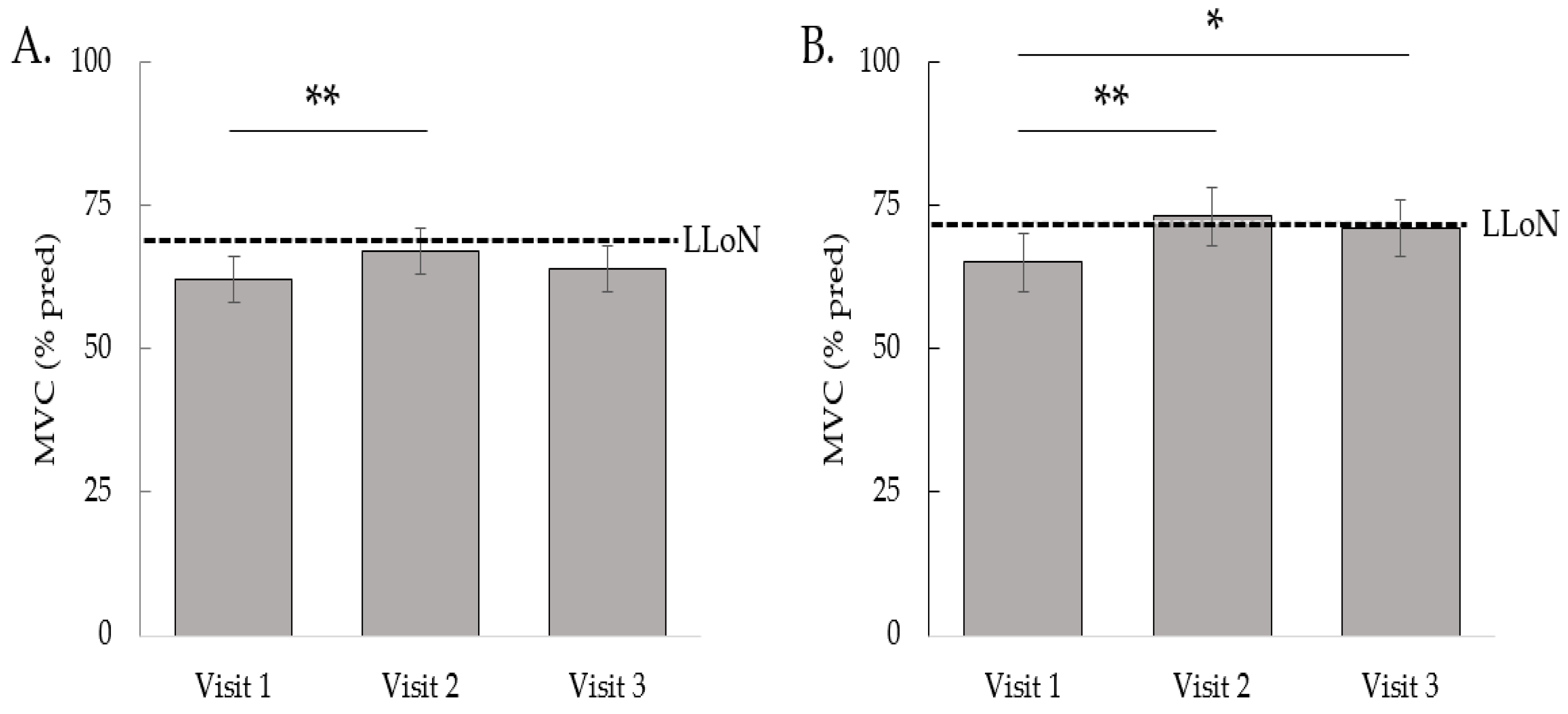
3.1. Post-Hospitalized Patients
3.2. Patients with PASC after Mild COVID-19
3.3. Muscle Ultrasound
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Medicine, J.H.U. COVID-19 Dashboard. Available online: https://coronavirus.jhu.edu/map.html (accessed on 7 June 2022).
- World Health Organization. Living Guidance for Clinical Management of COVID-19. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-2 (accessed on 7 July 2022).
- Liu, B. Whole of population-based study of recovery time from COVID-19 in New South Wales Australia. Lancet Reg. Health West. Pac. 2021, 12, 100193. [Google Scholar] [CrossRef]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.N.; Eggelbusch, M.; Naddaf, E.; Gerrits, K.H.L.; van der Schaaf, M.; van den Borst, B.; Wiersinga, W.J.; van Vugt, M.; Weijs, P.J.M.; Murray, A.J. Skeletal muscle alterations in patients with acute Covid-19 and post-acute sequelae of Covid-19. J. Cachexia Sarcopenia Muscle 2022, 13, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Lorent, N.; Weygaerde, Y.V.; Claeys, E.; Fajardo, I.G.C.; De Vos, N.; De Wever, W.; Salhi, B.; Gyselinck, I.; Bosteels, C.; Lambrecht, B.N.; et al. Prospective longitudinal evaluation of hospitalised COVID-19 survivors 3 and 12 months after discharge. ERJ Open Res. 2022, 8, 00004-2022. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Hartley, P.; Costello, P.; Fenner, R.; Gibbins, N.; Quinn, É.; Kuhn, I.; Keevil, V.L.; Romero-Ortuno, R. Change in skeletal muscle associated with unplanned hospital admissions in adult patients: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0210186. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, S.; Batra, A.; Lerner, D.P. Review of Critical Illness Myopathy and Neuropathy. Neurohospitalist 2017, 7, 41–48. [Google Scholar] [CrossRef]
- Stevens, R.D.; Dowdy, D.W.; Michaels, R.K.; Mendez-Tellez, P.A.; Pronovost, P.J.; Needham, D.M. Neuromuscular dysfunction acquired in critical illness: A systematic review. Intensive Care Med. 2007, 33, 1876–1891. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, A.I.V.; Spiliopoulos, L.; Bager, P.; Nielsen, N.M.; Hansen, J.V.; Koch, A.; Meder, I.K.; Ethelberg, S.; Hviid, A. A nationwide questionnaire study of post-acute symptoms and health problems after SARS-CoV-2 infection in Denmark. Nat. Commun. 2022, 13, 4213. [Google Scholar] [CrossRef]
- Frykholm, E.; Géphine, S.; Saey, D.; Van Hees, H.; Lemson, A.; Klijn, P.; Maltais, F.; Nyberg, A. Inter-day test-retest reliability and feasibility of isokinetic, isometric, and isotonic measurements to assess quadriceps endurance in people with chronic obstructive pulmonary disease: A multicenter study. Chron. Respir. Dis. 2019, 16, 1479973118816497. [Google Scholar] [CrossRef]
- Harbo, T.; Brincks, J.; Andersen, H. Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body mass, height, and sex in 178 healthy subjects. Eur. J. Appl. Physiol. 2012, 112, 267–275. [Google Scholar] [CrossRef]
- Revel, M.P.; Parkar, A.P.; Prosch, H.; Silva, M.; Sverzellati, N.; Gleeson, F.; Brady, A.; European Society of Radiology (ESR) and the European Society of Thoracic Imaging (ESTI). COVID-19 patients and the radiology department—Advice from the European Society of Radiology (ESR) and the European Society of Thoracic Imaging (ESTI). Eur. Radiol. 2020, 30, 4903–4909. [Google Scholar] [CrossRef]
- Graham, B.L.; Brusasco, V.; Burgos, F.; Cooper, B.G.; Jensen, R.; Kendrick, A.; MacIntyre, N.R.; Thompson, B.R.; Wanger, J. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur. Respir. J. 2017, 49, 1600016. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef] [PubMed]
- Wanger, J.; Clausen, J.L.; Coates, A.; Pedersen, O.F.; Brusasco, V.; Burgos, F.; Casaburi, R.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.M.; et al. Standardisation of the measurement of lung volumes. Eur. Respir. J. 2005, 26, 511–522. [Google Scholar] [CrossRef]
- Franssen, F.M.; Rutten, E.P.; Groenen, M.T.; Vanfleteren, L.E.; Wouters, E.F.; Spruit, M.A. New reference values for body composition by bioelectrical impedance analysis in the general population: Results from the UK Biobank. J. Am. Med. Dir. Assoc. 2014, 15, 448.e1–448.e6. [Google Scholar] [CrossRef] [PubMed]
- Abbott, J.; Teleni, L.; McKavanagh, D.; Watson, J.; McCarthy, A.L.; Isenring, E. Patient-Generated Subjective Global Assessment Short Form (PG-SGA SF) is a valid screening tool in chemotherapy outpatients. Support Care Cancer 2016, 24, 3883–3887. [Google Scholar] [CrossRef]
- Mahler, D.A.; Wells, C.K. Evaluation of clinical methods for rating dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Muller, M.; Cohen, P.D.; Essink-Bot, M.-L.; Fekkes, M.; Sanderman, R.; Sprangers, M.A.; Velde, A.T.; Verrips, E. Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J. Clin. Epidemiol. 1998, 51, 1055–1068. [Google Scholar] [CrossRef]
- Vercoulen, J.H.; Swanink, C.M.A.; Fennis, J.F.M.; Galama, J.M.D.; van der Meer, J.W.M.; Bleijenberg, G. Dimensional assessment of chronic fatigue syndrome. J. Psychosom. Res. 1994, 38, 383–392. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef] [PubMed]
- van Alfen, N.; Mah, J.K. Neuromuscular Ultrasound: A New Tool in Your Toolbox. Can. J. Neurol. Sci. 2018, 45, 504–515. [Google Scholar] [CrossRef]
- van Doorn, J.L.M.; Wijntjes, J.; Saris, C.G.J.; Ottenheijm, C.A.C.; van Alfen, N.; Doorduin, J. Association of diaphragm thickness and echogenicity with age, sex, and body mass index in healthy subjects. Muscle Nerve. 2022, 66, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Cawthon, P.M.; Fox, K.M.; Gandra, S.R.; Delmonico, M.J.; Chiou, C.F.C.; Anthony, M.S.; Sewall, A.; Goodpaster, B.; Satterfield, S.; Cummings, S.R. Do Muscle Mass, Muscle Density, Strength, and Physical Function Similarly Influence Risk of Hospitalization in Older Adults? J. Am. Geriatr. Soc. 2009, 57, 1411–1419. [Google Scholar] [CrossRef] [PubMed]
- Cheval, B.; Sieber, S.; Maltagliati, S.; Millet, G.P.; Formánek, T.; Chalabaev, A.; Cullati, S.; Boisgontier, M.P. Muscle strength is associated with COVID-19 hospitalization in adults 50 years of age or older. J. Cachexia Sarcopenia Muscle 2021, 12, 1136–1143. [Google Scholar] [CrossRef]
- Perez-Valera, M.; Martinez-Canton, M.; Gallego-Selles, A.; Galván-Alvarez, V.; Gelabert-Rebato, M.; Morales-Alamo, D.; Santana, A.; Martin-Rodriguez, S.; Ponce-Gonzalez, J.G.; Larsen, S.; et al. Angiotensin-Converting Enzyme 2 (SARS-CoV-2 receptor) expression in human skeletal muscle. Scand. J. Med. Sci. Sport. 2021, 31, 2249–2258. [Google Scholar] [CrossRef]
- Hurst, C.; Murray, J.C.; Granic, A.; Hillman, S.J.; Cooper, R.; Sayer, A.A.; Robinson, S.M.; Dodds, R.M. Long-term conditions, multimorbidity, lifestyle factors and change in grip strength over 9 years of follow-up: Findings from 44,315 UK biobank participants. Age Ageing 2021, 50, 2222–2229. [Google Scholar] [CrossRef]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.S.; de Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; Newman, A.B. Decreased muscle strength and quality in older adults with type 2 diabetes: The health, aging, and body composition study. Diabetes 2006, 55, 1813–1818. [Google Scholar] [CrossRef]
- Fogelholm, M.; Van Marken Lichtenbelt, W. Comparison of body composition methods: A literature analysis. Eur. J. Clin. Nutr. 1997, 51, 495–503. [Google Scholar] [CrossRef]
- Goselink, R.J.M.; Schreuder, T.H.; Mul, K.; Voermans, N.C.; Erasmus, C.E.; van Engelen, B.G.; van Alfen, N. Muscle ultrasound is a responsive biomarker in facioscapulohumeral dystrophy. Neurology 2020, 94, e1488–e1494. [Google Scholar] [CrossRef] [PubMed]
- Kroon, R.; Kalf, J.G.; Meijers, R.L.; de Swart, B.J.M.; Cameron, I.G.M.; Doorduin, J.; van Alfen, N.; van Engelen, B.G.; Horlings, C.G. Muscle ultrasound is a sensitive biomarker in oculopharyngeal muscular dystrophy. Muscle Nerve. 2022, 66, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Leeuwenberg, K.E.; Van Alfen, N.; Christopher-Stine, L.; Paik, J.J.; Tiniakou, E.; Mecoli, C.; Doorduin, J.; Saris, C.G.; Albayda, J. Ultrasound can differentiate inclusion body myositis from disease mimics. Muscle Nerve. 2020, 61, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Wijntjes, J.; van Alfen, N. Muscle ultrasound: Present state and future opportunities. Muscle Nerve. 2021, 63, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Zaidman, C.M.; Wu, J.S.; Kapur, K.; Pasternak, A.; Madabusi, L.; Yim, S.; Pacheck, A.; Szelag, H.; Harrington, T.; Darras, B.T.; et al. Quantitative muscle ultrasound detects disease progression in Duchenne muscular dystrophy. Ann. Neurol. 2017, 81, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Hejbol, E.K.; Harbo, T.; Agergaard, J.; Madsen, L.B.; Pedersen, T.H.; Østergaard, L.J.; Andersen, H.; Schrøder, H.D.; Tankisi, H. Myopathy as a cause of fatigue in long-term post-COVID-19 symptoms: Evidence of skeletal muscle histopathology. Eur. J. Neurol. 2022, 29, 2832–2841. [Google Scholar] [CrossRef] [PubMed]
- World Physiotherapy (Ed.) World Physiotherapy Response to COVID-19 Briefing Paper 9. In Safe Rehabilitation Approaches for People Living with Long COVID: Physical Activity and Exercise; World Physiotherapy: London, UK, 2021; Available online: https://world.physio/covid-19-information-hub/long-covid (accessed on 6 July 2022).
- Group, R.C. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- Schakman, O.; Gilson, H.; Thissen, J.P. Mechanisms of glucocorticoid-induced myopathy. J. Endocrinol. 2008, 197, 1–10. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Post-Hospitalized (n = 82) | PASC after Mild COVID-19 (n = 43) | ||||
|---|---|---|---|---|---|
| Patients with Missing Data, n | Normal Muscle Strength (n = 34) | Muscle Weakness (n = 48) | Normal Muscle Strength (n = 15) | Muscle Weakness (n = 28) | |
| Demographics | |||||
| Age, years | 0 | 61 ± 10 | 60 ± 10 | 53 ± 17 | 50 ± 15 |
| Male gender, No. (%) | 0 | 21 (62) | 34 (71) | 7 (47) | 9 (32) |
| Active smokers, No. (%) | 6 | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Acute COVID-19 characteristics | |||||
| Length of stay, days | 0 | 10 (4–19) | 13 (6–33) | NA | NA |
| ICU admission, No. (%) | 0 | 11 (32) | 19 (40) | NA | NA |
| CT severity score | 15 | 13 ± 5 | 14 ± 5 | NA | NA |
| Peak D-Dimer, µg/L | 13 | 1420 (1025–5025) | 3580 (810–12,005) | NA | NA |
| Peak CRP, mg/L | 7 | 115 (50–174) | 167 (67–254) | NA | NA |
| Peak Ferritin, µg/L | 10 | 1184 (618–2550) | 1929 (820–3526) | NA | NA |
| Chloroquine, No. (%) | 0 | 26 (77) | 35 (73) | NA | NA |
| Corticosteroids, No. (%) | 0 | 2 (6) | 7 (15) | NA | NA |
| Anakinra, No. (%) | 0 | 3 (9) | 8 (17) | NA | NA |
| Comorbidities, No. (%) | |||||
| Cardiovascular | 0 | 8 (24) | 11 (23) | 1 (7) | 5 (18) |
| Oncological | 0 | 6 (18) | 9 (19) | 0 (0) | 1 (4) |
| Immunocompromised | 0 | 4 (12) | 11 (23) | 1 (7) | 0 (0) |
| Chronic lung disease | 0 | 12 (35) | 11 (23) | 3 (20) | 4 (14) |
| COPD | 0 | 4 (12) | 2 (4) | 1 (7) | 0 (0) |
| Asthma | 0 | 8 (24) | 3 (6) * | 2 (13) | 4 (14) |
| Other lung disease | 0 | 4 (12) | 7 (15) | 0 (0) | 0 (0) |
| Hypertension | 0 | 9 (27) | 18 (38) | 3 (20) | 5 (18) |
| Diabetes mellitus | 0 | 1 (3) | 15 (31) ** | 0 (0) | 3 (11) |
| Chronic kidney failure | 0 | 0 (0) | 5 (10) | 0 (0) | 0 (0) |
| Number of comorbidities, No. | 0 | 1 (0–2) | 1 (1–3) | 0 (0-1) | 0 (0–1) |
| Full Model | Final Model | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables in the Equation | β | SE | OR | 95% CI | p | β | SE | OR | 95% CI | p |
| Age (years) | −0.05 | 0.03 | 0.95 | 0.90–1.01 | 0.10 | |||||
| Gender | 0.11 | 0.54 | 1.12 | 0.39–3.21 | 0.84 | |||||
| Length of stay (days) | 0.03 | 0.02 | 1.03 | 1.00–1.06 | 0.07 | 0.03 | 0.02 | 1.03 | 1.00–1.06 | 0.05 |
| Asthma | −1.57 | 0.85 | 0.21 | 0.04–1.11 | 0.07 | |||||
| Diabetes mellitus | 2.19 | 1.12 | 8.95 | 1.00–80.16 | 0.05 | 2.75 | 1.07 | 15.62 | 1.92–127.08 | 0.01 |
| Number of comorbidities | 0.32 | 0.24 | 1.38 | 0.86–2.23 | 0.18 | |||||
| Nagelkerke pseudo R2 | 0.33 | 0.26 | ||||||||
| Post-Hospitalized (n = 82) | PASC after Mild COVID-19 (n = 43) | ||||
|---|---|---|---|---|---|
| Patients with Missing Data, n | Normal Muscle Strength (n = 34) | Muscle Weakness (n = 48) | Normal Muscle Strength (n = 15) | Muscle Weakness (n = 28) | |
| Time since symptom onset, weeks | 1 | 12 (11–13) | 13 (11–18) | 22 (19–25) | 18 (15–24) |
| Time since discharge, weeks | 0 | 10 (8–10) | 10 (8–12) | NA | NA |
| BMI, kg/m2 | 0 | 27.2 ± 4.3 | 28.8 ± 3.7 | 26.4 ± 4.6 | 28.9 ± 5.2 |
| FFMi, kg/m2 | 2 | 19.3 ± 2.9 | 19.9 ± 2.6 | 18.0 ± 2.1 | 18.9 ± 2.7 |
| Abnormal FFMi, No. (%) | 2 | 3 (9) | 10 (22) | 3 (20) | 1 (4) |
| PS-SGA SF score | 3 | 1 (1–2) | 1 (1–3) | 2 (1–3) | 3 (1–6) |
| mMRC score | 1 | 1 (0–1) | 1 (0–2) | 1 (1–2) | 1 (1–2) |
| CIS—fatigue score | 1 | 36 (26–43) | 41 (32–51) | 44 (38–48) | 51 (46–55) ## |
| SF-36 physical functioning score | 5 | 70 (53–85) | 58 (31–74) * | 70 (55–80) | 60 (41–75) |
| FEV1, % of predicted | 0 | 99 ± 20 | 93 ± 18 | 90 ± 18 | 100 ± 13 |
| VC, % of predicted | 0 | 103 ± 18 | 92 ± 19 * | 98 ± 9 | 100 ± 11 |
| DLco, % of predicted | 3 | 80 ± 19 | 72 ± 18 | 89 ± 18 | 91 ± 12 |
| 6MWD, m | 7 | 549 ± 119 | 454 ± 111 ** | 575 ± 84 | 516 ± 64 # |
| 6MWD, % of predicted | 7 | 100 ± 19 | 81 ± 17 ** | 103 ± 20 | 89 ± 11 # |
| CRP > 5 mg/L, No. (%) | 1 | 4 (12) | 8 (17) | 1 (7) | 5 (18) |
| Muscle Thickness | Echo Intensity | |||||
|---|---|---|---|---|---|---|
| Thickness (cm) | z-Score | Abnormal (n) | Intensity (Grey Level) | z-Score | Abnormal (n) | |
| m. biceps brachii | 2.6 (2.2, 3.2) | 0.5 (−0.3, 1.7) | 0 | 61 (54,69) | −1.1 (−1.5, −0.5) | 0 |
| m. deltoideus | 2.0 (1.8, 2.2) | 0.3 (−0.3, 0.6) | 0 | 59 (55, 69) | 0.3 (−0.4, 0.8) | 0 |
| m. flexor carpi radialis | 1.3 (1.2, 1.6) | 0.3 (−0.4, 1.6) | 0 | 50 (45, 54) | −0.4 (−0.8, 0.1) | 0 |
| m. gastrocnemius (medial head) | 1.8 (1.6, 1.9) | 0.8 (0.1, 1.0) | 0 | 64 (55, 70) | −0.7 (−1.3, −0.1) | 0 |
| m. interosseus dorsalis I | 1.2 (1.0, 1.3) | 0.2 (−0.3, 0.9) | 0 | 44 (39, 48) | −1.3 (−1.7, −0.6) | 0 |
| m. peroneus tertius | 1.6 (1.5, 1.9) | 0.9 (0.6, 2.1) | 0 | 74 (68, 77) | −0.1 (−0.7, 0.2) | 0 |
| m. rectus femoris * | 4.1 (3.6, 4.7) | −0.2 (−1.4, 0.1) | 0 | 63 (51, 69) | −0.2 (−1.3, 0.6) | 0 |
| m. tibialis anterior | 2.6 (2.3, 2.9) | 0.1 (−0.8, 0.6) | 0 | 82 (74, 85) | 0.5 (−0.4, 1.0) | 0 |
| m. vastus lateralis | 3.5 (2.8, 3.8) | −1.0 (−1.3, −0.2) | 0 | 70 (63, 75) | 0.0 (−0.2, 1.1) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoffels, A.A.F.; van Voorthuizen, E.L.; van Hees, H.W.H.; Peters, J.B.; van Helvoort, H.A.C.; Voermans, N.C.; Doorduin, J.; van den Borst, B. Longitudinal Analysis of Quadriceps Muscle Strength in Patients with Previous COVID-19 Hospitalization and in Patients with Post-Acute Sequelae following Mild COVID-19. Nutrients 2022, 14, 4319. https://doi.org/10.3390/nu14204319
Stoffels AAF, van Voorthuizen EL, van Hees HWH, Peters JB, van Helvoort HAC, Voermans NC, Doorduin J, van den Borst B. Longitudinal Analysis of Quadriceps Muscle Strength in Patients with Previous COVID-19 Hospitalization and in Patients with Post-Acute Sequelae following Mild COVID-19. Nutrients. 2022; 14(20):4319. https://doi.org/10.3390/nu14204319
Chicago/Turabian StyleStoffels, Anouk A. F., Esther L. van Voorthuizen, Hieronymus W. H. van Hees, Jeannette B. Peters, Hanneke A. C. van Helvoort, Nicol C. Voermans, Jonne Doorduin, and Bram van den Borst. 2022. "Longitudinal Analysis of Quadriceps Muscle Strength in Patients with Previous COVID-19 Hospitalization and in Patients with Post-Acute Sequelae following Mild COVID-19" Nutrients 14, no. 20: 4319. https://doi.org/10.3390/nu14204319
APA StyleStoffels, A. A. F., van Voorthuizen, E. L., van Hees, H. W. H., Peters, J. B., van Helvoort, H. A. C., Voermans, N. C., Doorduin, J., & van den Borst, B. (2022). Longitudinal Analysis of Quadriceps Muscle Strength in Patients with Previous COVID-19 Hospitalization and in Patients with Post-Acute Sequelae following Mild COVID-19. Nutrients, 14(20), 4319. https://doi.org/10.3390/nu14204319