
A Life Course Approach to the Prevention of Iron Deficiency Anemia in Indonesia

 , ,
, , 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Expert Selection
2.2. Expert Meeting
3. Results
4. Discussion
4.1. Indonesian Government’s Programs to Overcome Anemia
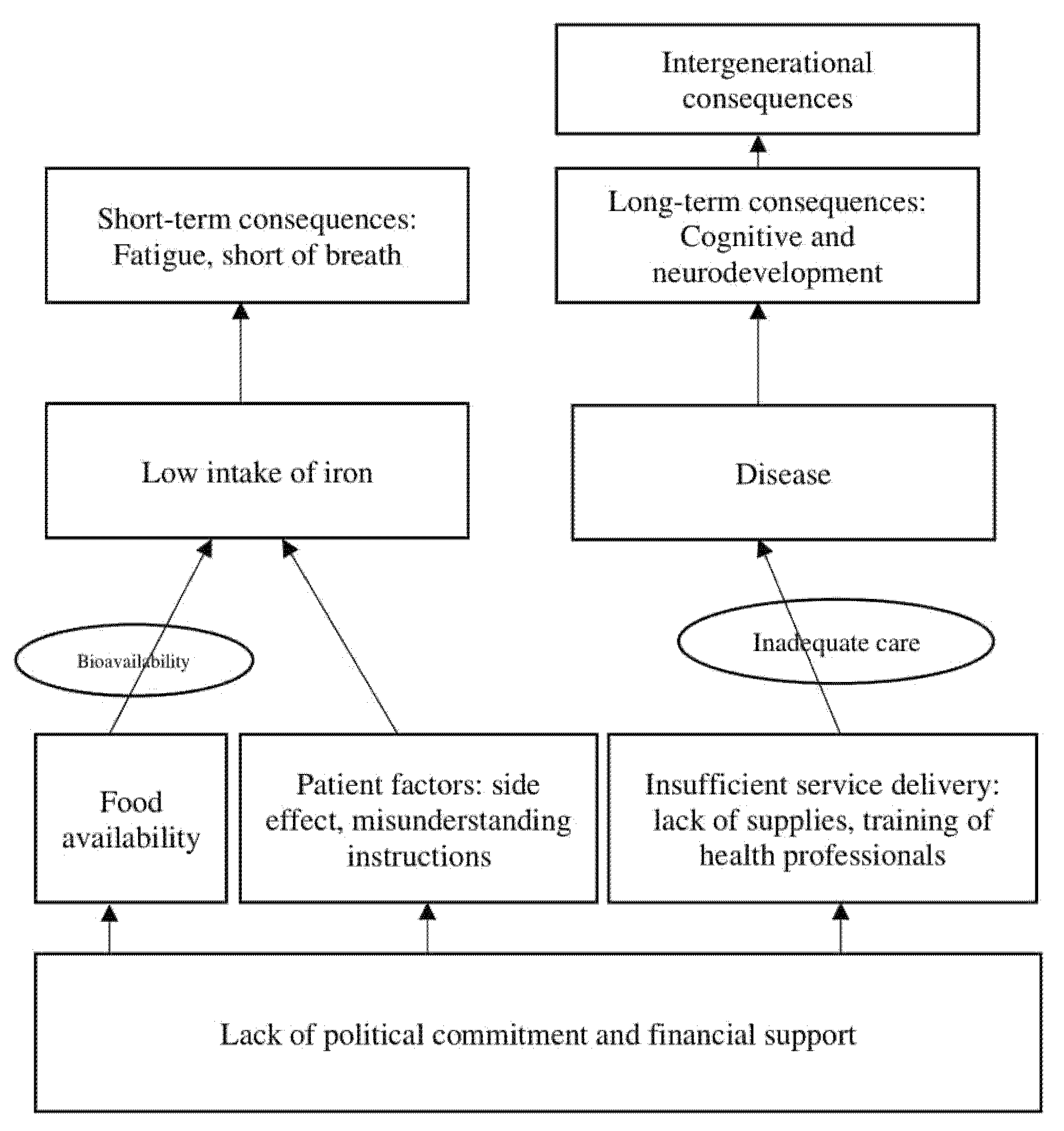
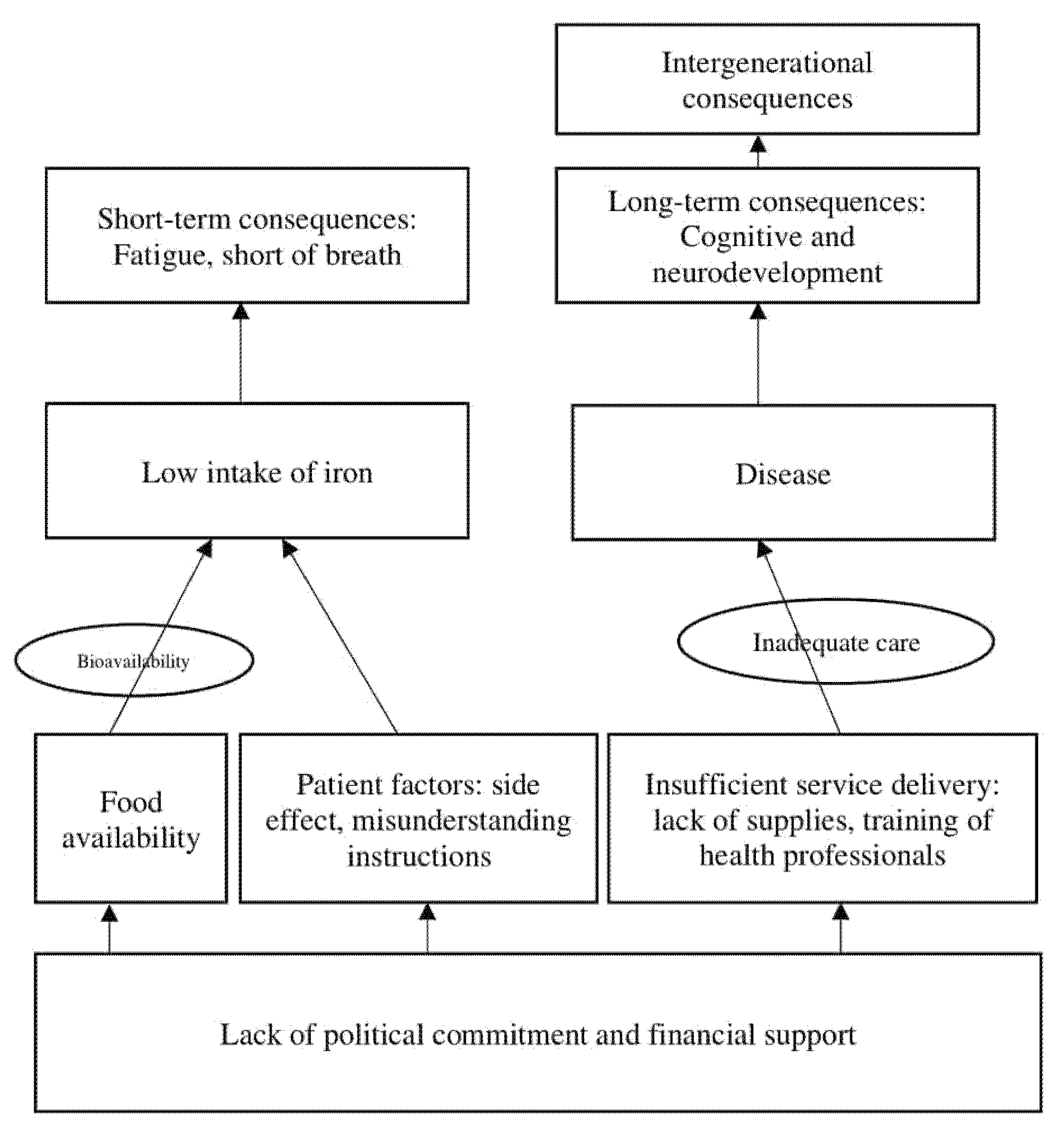
4.2. Factors Affecting the Anemia Control Program
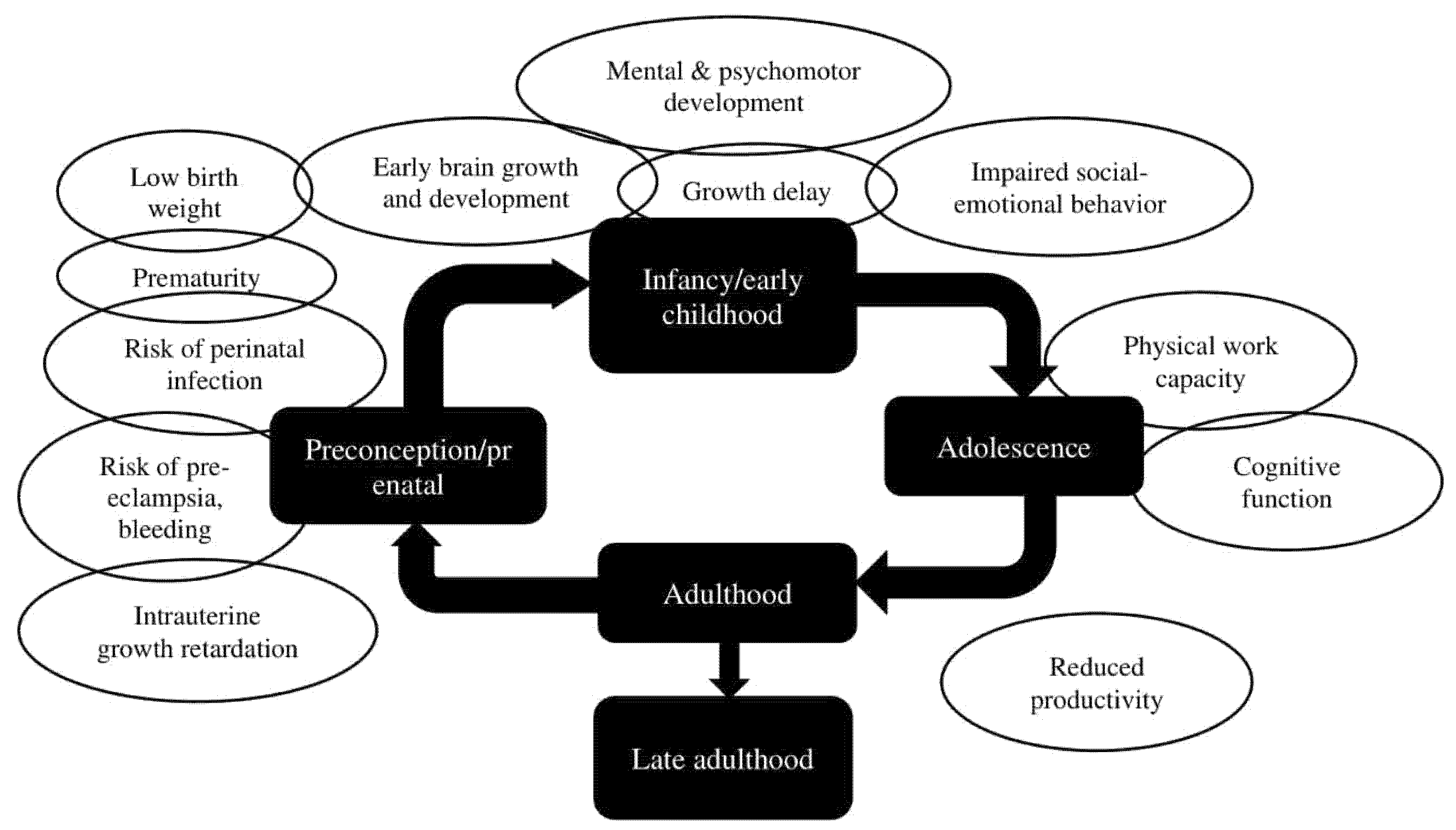
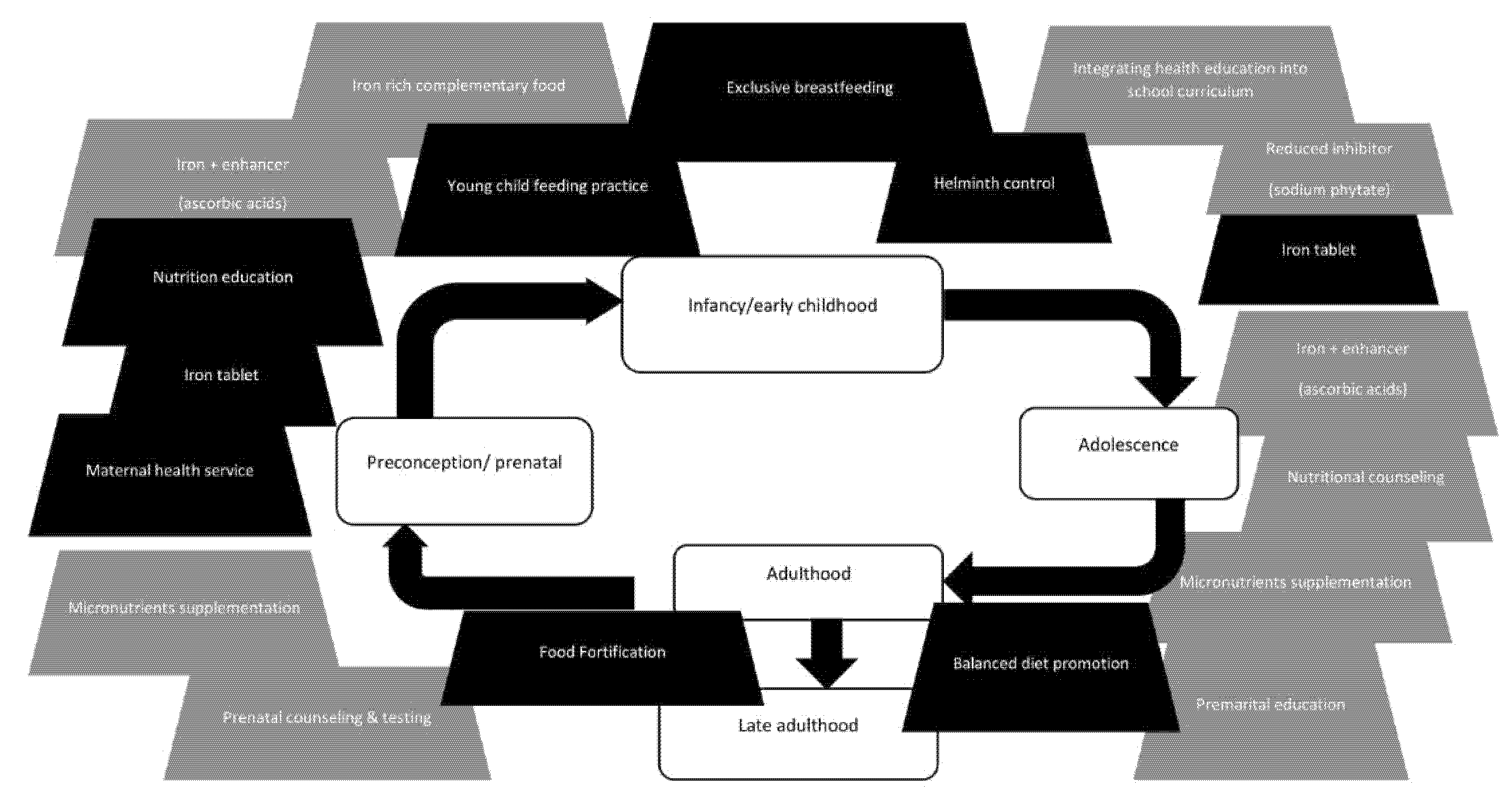
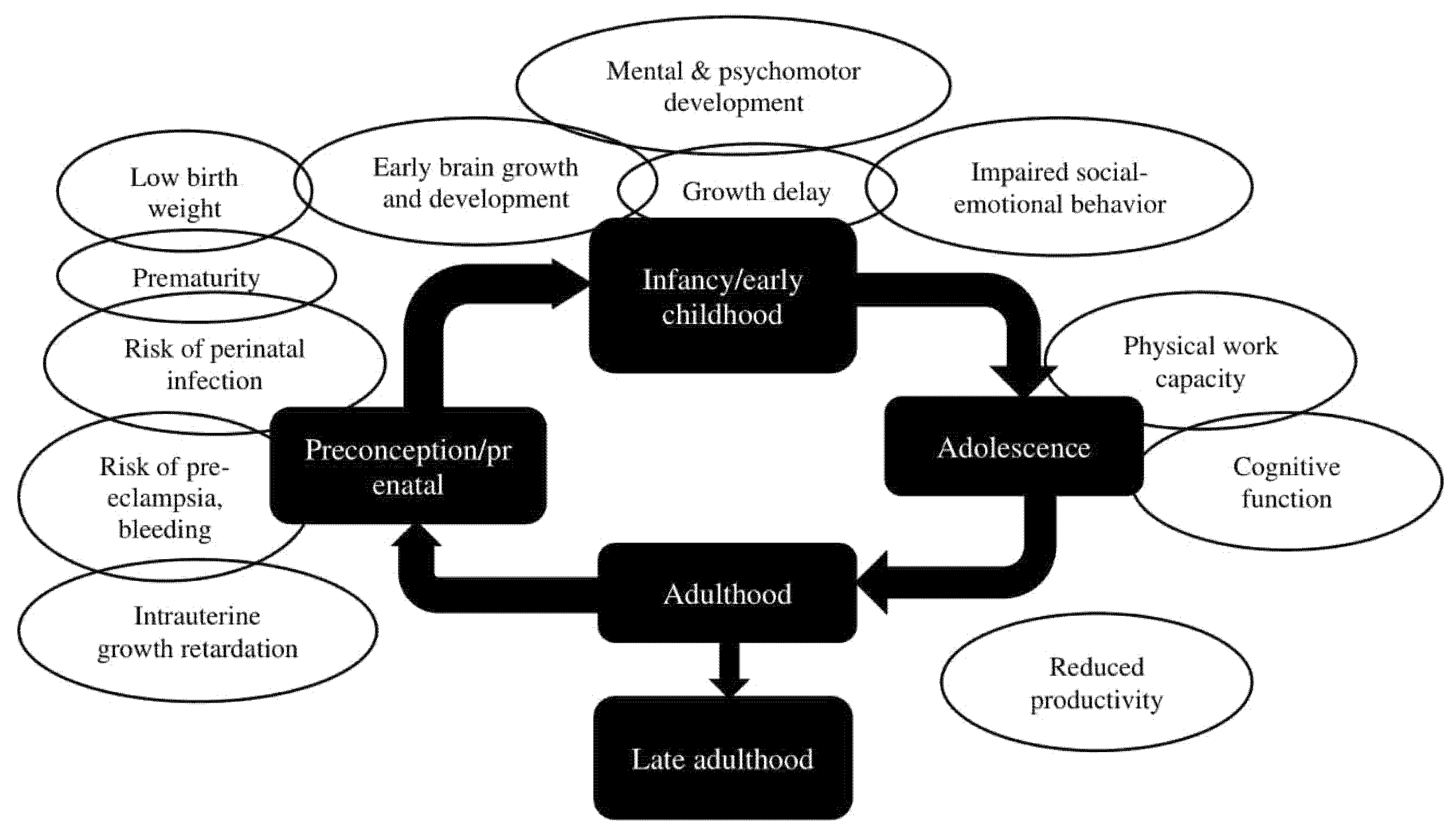
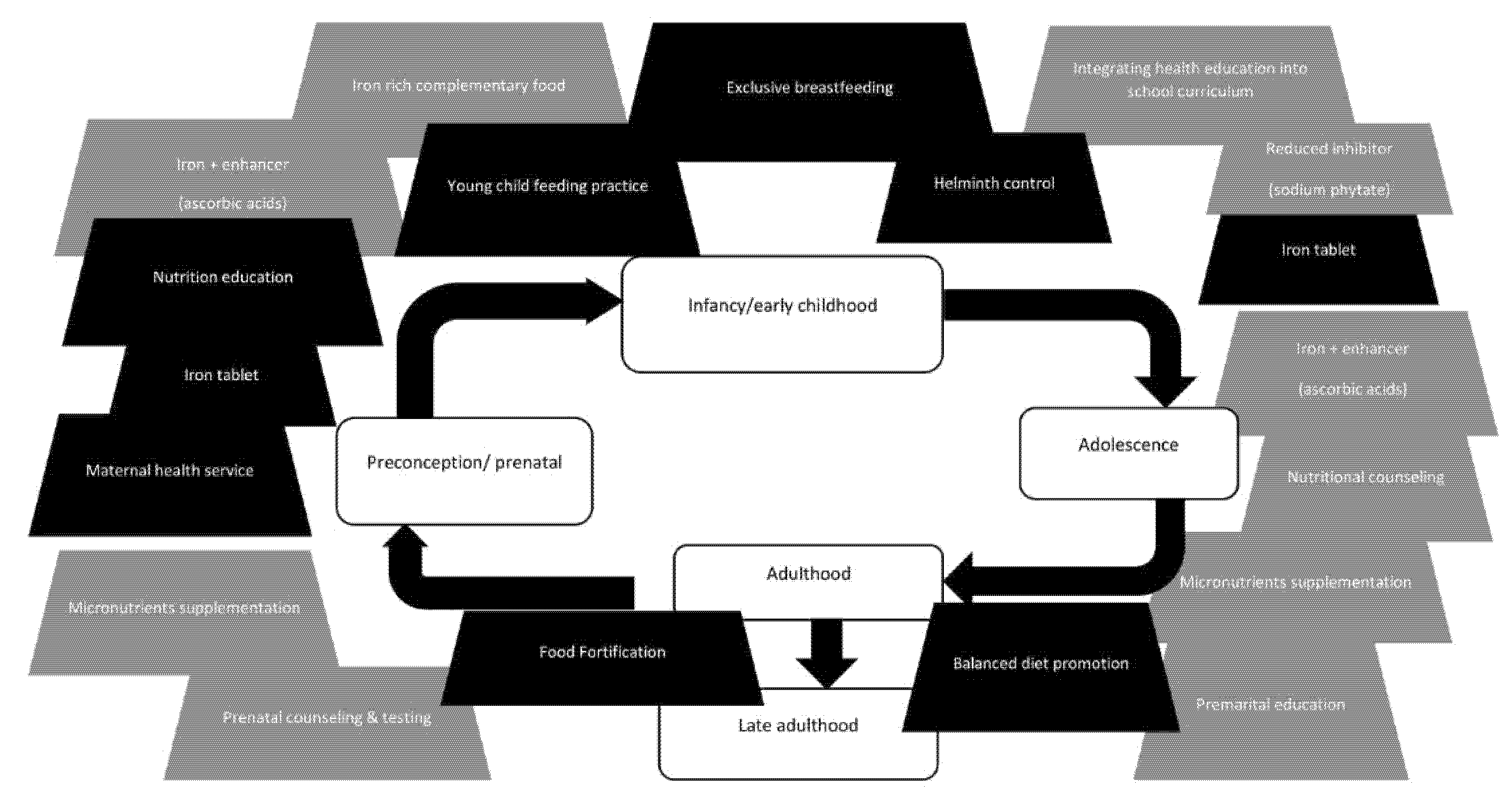
4.3. Effects and Possible Interventions in Each Life Stage
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Anaemia in Children < 5 Years—Estimates by WHO Region. Available online: https://apps.who.int/gho/data/view.main.ANEMIACHILDRENREGv (accessed on 23 April 2021).
- World Health Organization. Prevalence of Anaemia in Pregnant Women—Estimates by WHO Region. Available online: https://apps.who.int/gho/data/view.main.ANAEMIAWOMENPWREG (accessed on 23 April 2021).
- World Health Organization. Prevalence of Anaemia in Women of Reproductive Age Estimates by WHO Region. Available online: https://apps.who.int/gho/data/view.main.ANAEMIAWOMENPREVANEMIAREG? (accessed on 23 April 2021).
- Riset Kesehatan Dasar (Riskesdas). Badan Penelitian dan Pengembangan Kesehatan Kementerian Kesehatan Republik Indonesia; Badan Penelitian & Pengembangan Kesehatan Kemenkes RI: Jakarta, Indonesia, 2013. [Google Scholar]
- Riset Kesehatan Dasar (Riskesdas). Badan Penelitian dan Pengembangan Kesehatan Kementerian Kesehatan Republik Indonesia; Badan Penelitian & Pengembangan Kesehatan Kemenkes RI: Jakarta, Indonesia, 2018. [Google Scholar]
- Sandjaja, S.; Budiman, B.; Harahap, H.; Ernawati, F.; Soekatri, M.; Widodo, Y. Food consumption and nutritional and biochemical status of 0·5–12-year-old Indonesian children: The SEANUTS study. Br. J. Nutr. 2013, 110 (Suppl. S3), S11–S20. [Google Scholar] [CrossRef] [Green Version]
- McCann, S.; Perapoch Amadó, M.; Moore, S.E. The role of iron in brain development: A systematic review. Nutrients. 2020, 12, 2001. [Google Scholar] [CrossRef]
- Haas, J.D.; Brownlie, T. Iron deficiency and reduced work capacity: A critical review of the research to determine a causal relationship. J. Nutr. 2001, 131, 676S–690S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haider, B.A.; Olofin, I.; Wang, M.; Spiegelman, D.; Ezzati, M.; Fawzi, W.W. Anaemia, prenatal iron use, and risk of adverse pregnancy outcomes: Systematic review and meta-analysis. BMJ 2013, 346, f3443. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, S.; Ekmekcioglu, C. Maternal and neonatal outcomes related to iron supplementation or iron status: A summary of meta-analyses. J. Matern. Fetal Neonatal. Med. 2019, 32, 1528–1540. [Google Scholar] [CrossRef] [PubMed]
- Brabin, B.J.; Hakimi, M.; Pelletier, D. An analysis of anemia and pregnancy-related maternal mortality. J. Nutr. 2001, 131, 604S–615S. [Google Scholar] [CrossRef] [Green Version]
- Pasricha, S.R.; Black, J.; Muthayya, S.; Shet, A.; Bhat, V.; Nagaraj, S. Determinants of anemia among young children in rural India. Pediatrics 2010, 126, e140–e149. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The Global Prevalence of Anaemia in 2011. [Cited 23 April 2021]. 2015. Available online: https://apps.who.int/iris/handle/10665/177094 (accessed on 23 April 2021).
- Di Renzo, G.C.; Spano, F.; Giardina, I.; Brillo, E.; Clerici, G.; Roura, L.C. Iron deficiency anemia in pregnancy. Womens Health 2015, 11, 891–900. [Google Scholar] [CrossRef]
- Winardi, B.; Andani, E.C.G. Knowledge of pregnant women about anemia is related with adherence to iron tablets. Maj. Obstet. Ginekol. 2018, 26, 26–28. [Google Scholar] [CrossRef] [Green Version]
- Widiasih, R.; Utari, A.D.; Jayanti, T.N.; Ardiyanti, A.; Sari, R.I.; Siska, G.A. Factors associated with anaemia among pregnant women in indonesia: A systematic review. J. Keperawatan Soedirman 2019, 14, 1–14. [Google Scholar] [CrossRef]
- Unit Kerja Koordinasi Nutrisi dan Penyakit Metabolik PP IDAI. Rekomendasi Praktik Pemberian Makanan Berbasis Bukti pada Bayi dan Batita di Indonesia untuk Mencegah Malnutrisi. 2015. Available online: https://www.idai.or.id/professional-resources/pedoman-konsensus/rekomendasi-praktik-pemberian-makan-berbasis-bukti-pada-bayi-dan-batita-di-indonesia-untuk-mencegah-malnutrisi (accessed on 23 April 2021).
- Kemenkes RI. Pedoman Gizi Seimbang. Peraturan Menteri Kesehatan RI No. 41/2014. Available online: https://peraturan.bpk.go.id/Home/Details/119080/permenkes-no-41-tahun-2014 (accessed on 23 April 2021).
- UNICEF. Strategy for Improved Nutrition of Children and Women in Developing Countries; UNICEF: New York, NY, USA, 1990. [Google Scholar]
- Galloway, R.; McGuire, J. Determinants of compliance with iron supplementation: Supplies, side effects, or psychology? Soc. Sci. Med. 1994, 9, 381–390. [Google Scholar] [CrossRef]
- Chourasia, A.; Pandey, C.M.; Awasthi, A. Factors influencing the consumption of iron and folic acid supplementations in high focus states of India. Clin. Epidemiol. Glob. Health 2017, 5, 180–184. [Google Scholar] [CrossRef] [Green Version]
- Dairo, M.D.; Lawoyin, T.O. Demographic factors determining compliance to iron supplementation in pregnancy in Oyo State, Nigeria. Niger. J. Med. 2006, 15, 241–244. [Google Scholar] [CrossRef]
- Juanda, S.F.E. Factors that influence the adherence of pregnant women in consuming iron supplements: Systematical lirerature review. In Proceeding of the International Conference; Universitas Respati Yogyakarta: Yogyakarta, Indonesia, 2020. [Google Scholar]
- Dainty, J.R.; Berry, R.; Lynch, S.R.; Harvey, L.J.; Fairweather-Tait, S.J. Estimation of dietary iron bioavailability from food iron intake and iron status. PLoS ONE 2014, 9, e111824. [Google Scholar] [CrossRef] [Green Version]
- Abu-Ouf, N.M.; Jan, M.M. The impact of maternal iron deficiency and iron deficiency anemia on child’s health. Saudi Med. J. 2015, 36, 146–149. [Google Scholar] [CrossRef]
- Soliman, A.; Kalra, S.; Sanctis, V. Anemia and growth. Indian J. Endocrinol. Metab. 2014, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Sen, A.; Kanani, S.J. Deleterious functional impact of anemia on young adolescent school girls. Indian Pediatr. 2006, 43, 19–226. [Google Scholar]
- Salam, R.A.; Hooda, M.; Das, J.K.; Arshad, A.; Lassi, Z.S.; Middleton, P. Interventions to improve adolescent nutrition: A systematic review and meta-analysis. J. Adolesc. Health 2016, 59, S29–S39. [Google Scholar] [CrossRef] [Green Version]
- Black, M.M. Integrated strategies needed to prevent iron deficiency and to promote early child development. J. Trace Elem. Med. Biol. 2012, 26, 120–123. [Google Scholar] [CrossRef] [Green Version]
- Black, M.M.; Quigg, A.M.; Hurley, K.M.; Pepper, M.R. Iron deficiency and iron-deficiency anemia in the first two years of life: Strategies to prevent loss of developmental potential. Nutr. Rev. 2011, 69, S64–S70. [Google Scholar] [CrossRef]
- Juffrie, M.; Helmyati, S.; Hakimi, M. Nutritional anemia in Indonesia children and adolescents: Diagnostic reliability for appropriate management. Asian Pac. J. Clin. Nutr. 2020, 29 (Suppl. S1), S18–S31. [Google Scholar]
- Sunardi, D.; Bardosono, S.; Basrowi, R.W.; Wasito, E.; Vandenplas, Y. Dietary Determinants of Anemia in Children Aged 6–36 Months: A Cross-Sectional Study in Indonesia. Nutrients 2021, 13, 2397. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Frequency | Percentage |
|---|---|---|---|
| Gender | Male | 2 | 18.1 |
| Female | 9 | 81.8 | |
| Age | 40–50 years old | 4 | 36.3 |
| 50–60 years old | 5 | 45.4 | |
| >60 years old | 2 | 18.1 | |
| Expertise | Obstetrics and Gynecology | 2 | 18.1 |
| Pediatrician specialized in Nutrition and Metabolic | |||
| Pediatrician specialized in Growth and Development | 1 | 9.0 | |
| Specialist in Clinical Nutrition | |||
| Community Nutrition | 2 | 18.1 | |
| Clinical Psychology | 2 | 18.1 | |
| Midwife | 1 | 9.0 | |
| Education | 1 | 9.0 | |
| Experience | 10–20 years | 4 | 36.3 |
| 20–30 years | 5 | 45.4 | |
| >30 years | 2 | 18.1 |
| No | Interventions | Population Target |
|---|---|---|
| 1 | Providing iron tablets and folic acid | Female adolescents, pregnant mothers |
| 2 | Early breastfeeding initiation and promotion of exclusive breastfeeding up to 6 months of age [17] | Lactating mothers, infants |
| 3 | Providing information on infant and young child feeding practices | Infant and young child |
| 4 | Helminth prevention and control | Under-five and school-age children |
| 5 | Improving maternal healthcare services | Pregnant mothers |
| 6 | Nutrition education for pregnant mothers | Pregnant mothers |
| 7 | Balanced diet promotion (including recommending legumes consumption) [18] | General population |
| 8 | Food fortification (including the possibility of genetically modified plants) | General population |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sungkar, A.; Bardosono, S.; Irwinda, R.; Manikam, N.R.M.; Sekartini, R.; Medise, B.E.; Nasar, S.S.; Helmyati, S.; Ariani, A.S.; Nurihsan, J.; et al. A Life Course Approach to the Prevention of Iron Deficiency Anemia in Indonesia. Nutrients 2022, 14, 277. https://doi.org/10.3390/nu14020277
Sungkar A, Bardosono S, Irwinda R, Manikam NRM, Sekartini R, Medise BE, Nasar SS, Helmyati S, Ariani AS, Nurihsan J, et al. A Life Course Approach to the Prevention of Iron Deficiency Anemia in Indonesia. Nutrients. 2022; 14(2):277. https://doi.org/10.3390/nu14020277
Chicago/Turabian StyleSungkar, Ali, Saptawati Bardosono, Rima Irwinda, Nurul R. M. Manikam, Rini Sekartini, Bernie E. Medise, Sri S. Nasar, Siti Helmyati, Anna Surti Ariani, Juntika Nurihsan, and et al. 2022. "A Life Course Approach to the Prevention of Iron Deficiency Anemia in Indonesia" Nutrients 14, no. 2: 277. https://doi.org/10.3390/nu14020277
APA StyleSungkar, A., Bardosono, S., Irwinda, R., Manikam, N. R. M., Sekartini, R., Medise, B. E., Nasar, S. S., Helmyati, S., Ariani, A. S., Nurihsan, J., Nurjasmi, E., Khoe, L. C., Dilantika, C., Basrowi, R. W., & Vandenplas, Y. (2022). A Life Course Approach to the Prevention of Iron Deficiency Anemia in Indonesia. Nutrients, 14(2), 277. https://doi.org/10.3390/nu14020277