
Effect of a Multicomponent mHealth Intervention on the Composition of Diet in a Population with Overweight and Obesity—Randomized Clinical Trial EVIDENT 3

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
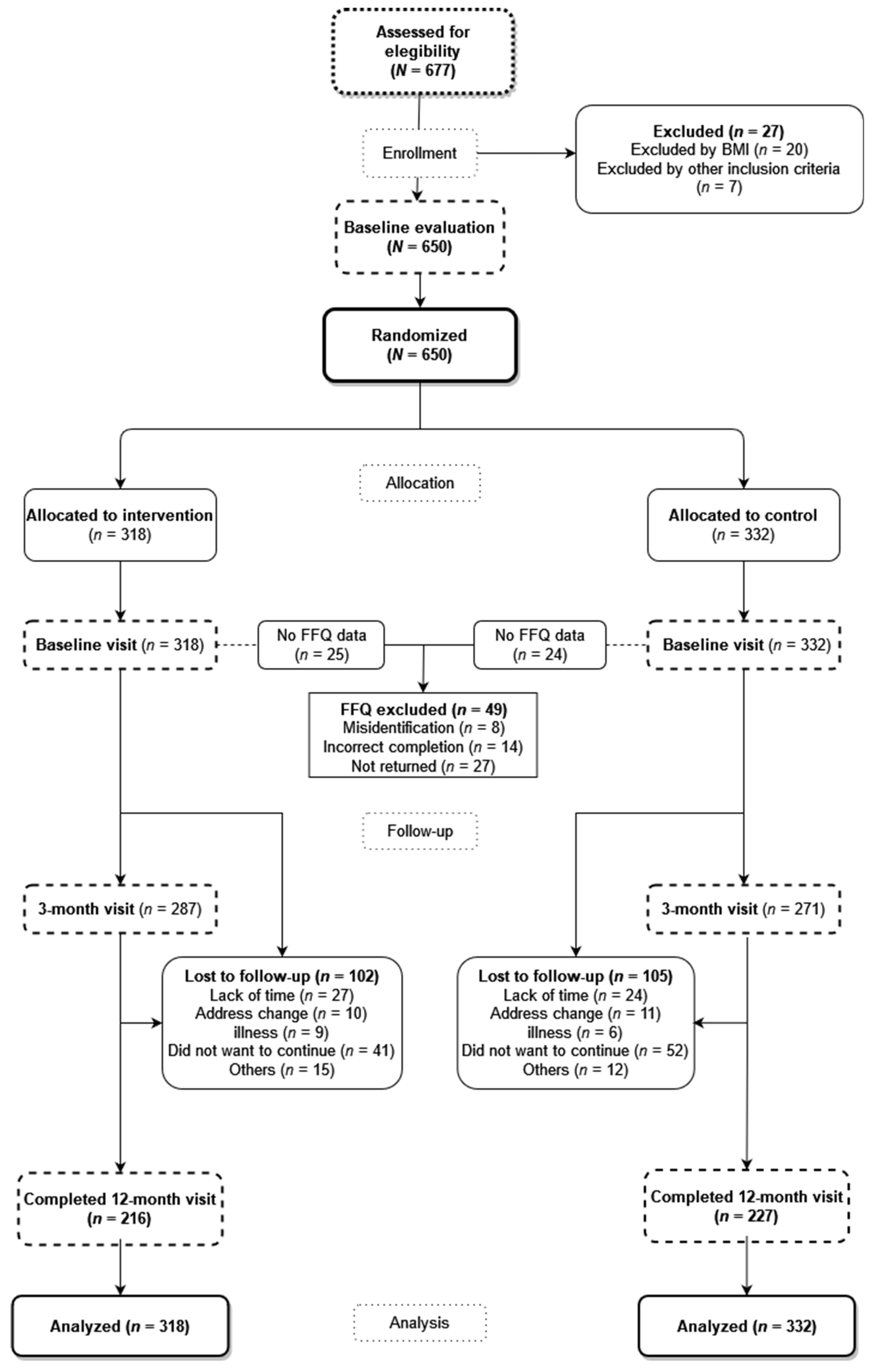
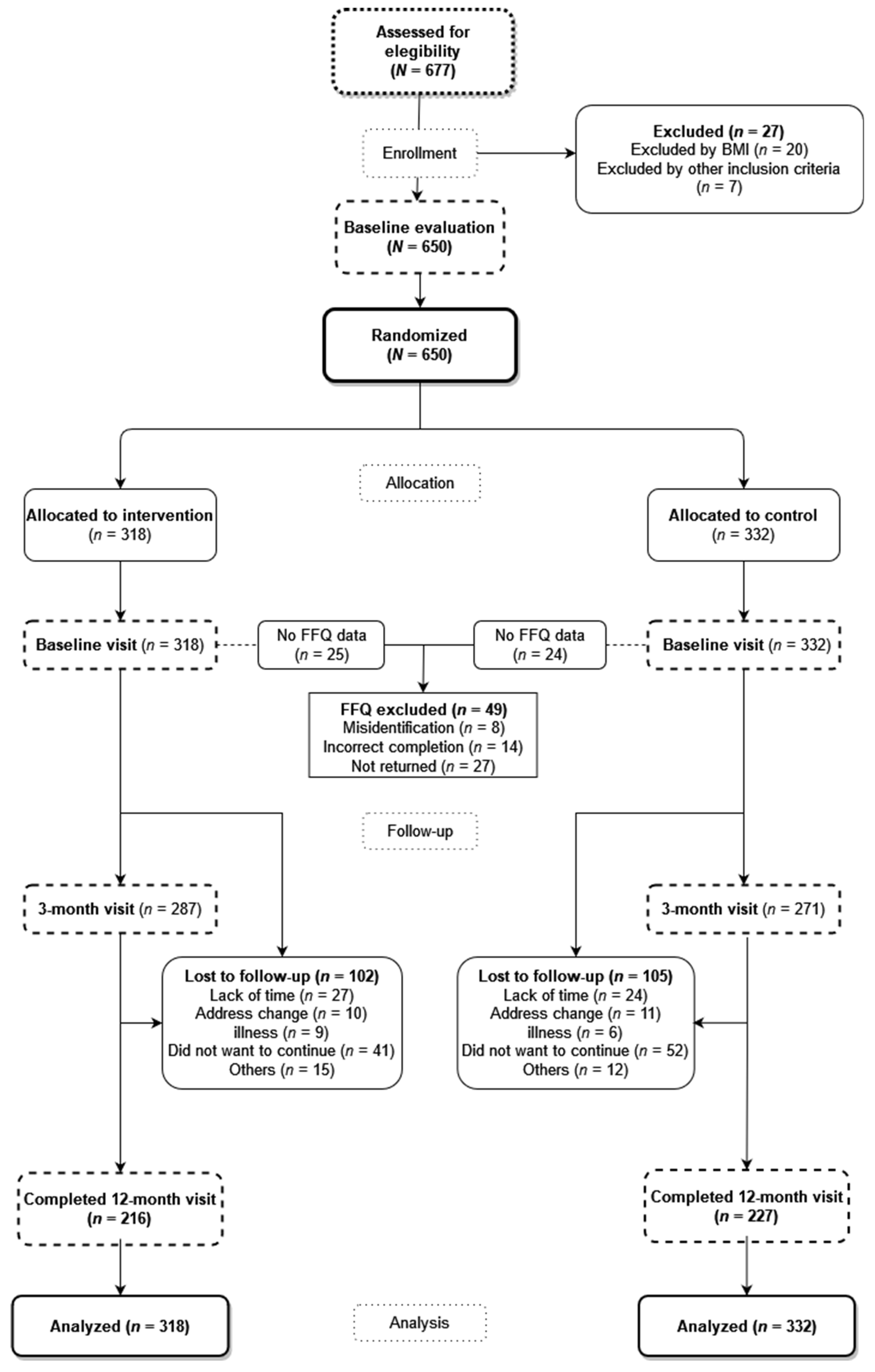
2.2. Participants
2.3. Screening and Randomization
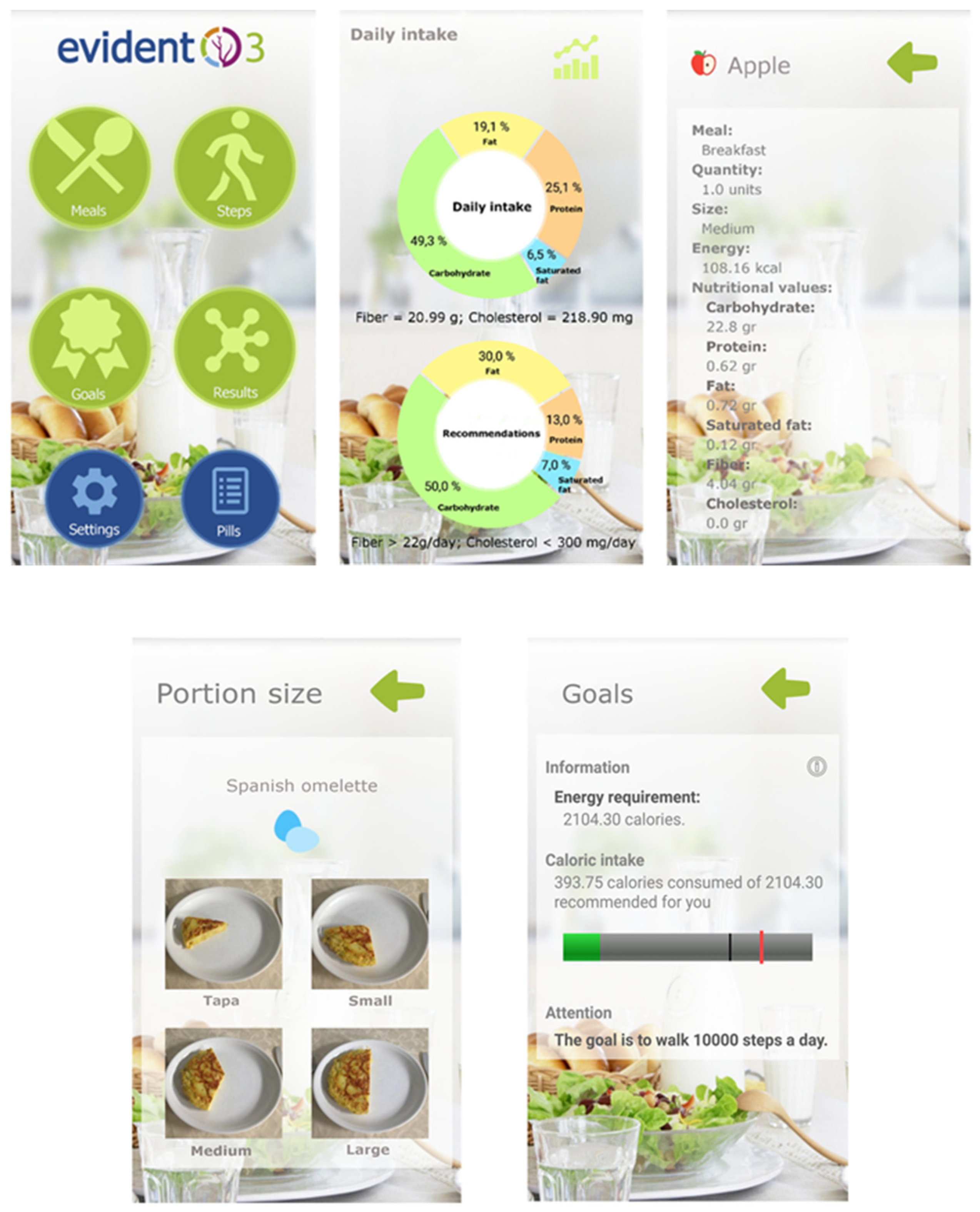
2.4. Intervention
2.4.1. Intervention Common for Both Groups
2.4.2. Specific Intervention
2.5. Measurements
2.5.1. Dietary Intake
2.5.2. Other Measurements
2.6. Ethics Approval and Consent to Participate
2.7. Stadistical Analysis
3. Results
3.1. Baseline Characteristics
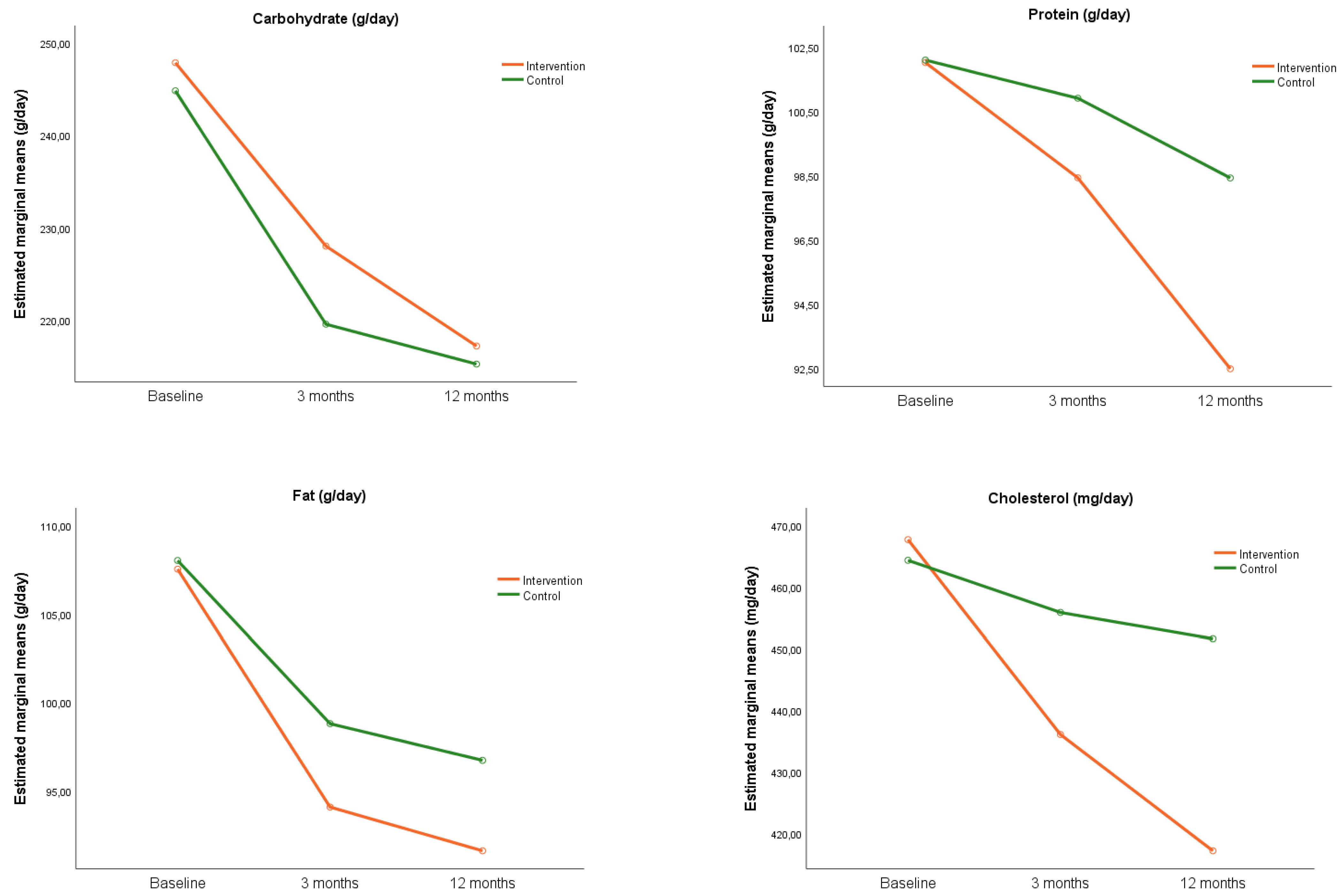
3.2. Changes in Macronutrients Intake
3.3. Changes in Daily Intake of Food Groups
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Complete (n = 443) | Loss of Follow-Up (n = 207) | p Value | ||
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Age, years (SD) | 49.2 ± 9.4 | 46.3 ± 9.9 | <0.001 | |
| Sex, n (%) | Men | 140 (31.6) | 65 (31.4) | 0.959 |
| Women | 303 (68.4) | 142 (68.6) | ||
| Smoker status, n (%) | Non-smoker | 181 (40.9) | 82 (39.6) | 0.403 |
| Current smoker | 91 (20.5) | 52 (25.1) | ||
| Former smoker | 171 (38.6) | 73 (35.3) | ||
| Civil status, n (%) | Single | 94 (21.2) | 40 (19.3) | 0.111 |
| Married | 299 (67.5) | 145 (70.1) | ||
| Separated | 39 (8.8) | 22 (10.6) | ||
| Widower | 11 (2.5) | 0 (0.0) | ||
| BMI (kg/m2) | 32.7 ± 3.4 | 33.6 ± 3.6 | 0.003 | |
| SBP (mmHg) | 119.6 ± 15.9 | 119.9 ± 14.7 | 0.851 | |
| DBP (mmHg) | 80.4 ± 9.8 | 79.5 ± 9.7 | 0.265 | |
| Total Cholesterol (mg/dL) | 200.0 ± 39.1 | 199.4 ± 34.7 | 0.835 | |
| HDL Cholesterol (mg/dL) | 51.6 ± 12.6 | 51.3 ± 12.0 | 0.732 | |
| Hypertension, n (%) | 144 (32.5) | 60 (29.1) | 0.414 | |
| Dyslipidaemia, n (%) | 122 (27.5) | 38 (19.3) | 0.029 | |
| Diabetes Mellitus, n (%) | 5 (1.2) | 4 (2.2) | 0.465 |
References
- De Deus Mendonça, R.; Pimenta, A.M.; Gea, A.; de la Fuente-Arrillaga, C.; Martinez-Gonzalez, M.A.; Lopes, A.C.S.; Bes-Rastrollo, M. Ultraprocessed Food Consumption and Risk of Overweight and Obesity: The University of Navarra Follow-Up (SUN) Cohort Study. Am. J. Clin. Nutr. 2016, 104, 1433–1440. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Moubarac, J.-C.; Levy, R.B.; Canella, D.S.; da Costa Louzada, M.L.; Cannon, G. Household Availability of Ultra-Processed Foods and Obesity in Nineteen European Countries. Public Health Nutr. 2018, 21, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Aljuraiban, G.S.; Gibson, R.; Oude Griep, L.M.; Okuda, N.; Steffen, L.M.; Van Horn, L.; Chan, Q. Perspective: The Application of A Priori Diet Quality Scores to Cardiovascular Disease Risk—A Critical Evaluation of Current Scoring Systems. Adv. Nutr. 2020, 11, 10–24. [Google Scholar] [CrossRef]
- Asghari, G.; Mirmiran, P.; Yuzbashian, E.; Azizi, F. A Systematic Review of Diet Quality Indices in Relation to Obesity. Br. J. Nutr. 2017, 117, 1055–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicklas, T.A.; O’Neil, C.E.; Fulgoni, V.L., III. Diet Quality Is Inversely Related to Cardiovascular Risk Factors in Adults. J. Nutr. 2012, 142, 2112–2118. [Google Scholar] [CrossRef]
- Morze, J.; Danielewicz, A.; Hoffmann, G.; Schwingshackl, L. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: A Second Update of a Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2020, 120, 1998–2031.e15. [Google Scholar] [CrossRef]
- Nouri, F.; Sadeghi, M.; Mohammadifard, N.; Roohafza, H.; Feizi, A.; Sarrafzadegan, N. Longitudinal Association between an Overall Diet Quality Index and Latent Profiles of Cardiovascular Risk Factors: Results from a Population Based 13-Year Follow up Cohort Study. Nutr. Metab. 2021, 18, 28. [Google Scholar] [CrossRef] [PubMed]
- Jannasch, F.; Kröger, J.; Schulze, M.B. Dietary Patterns and Type 2 Diabetes: A Systematic Literature Review and Meta-Analysis of Prospective Studies. J. Nutr. 2017, 147, 1174–1182. [Google Scholar] [CrossRef] [Green Version]
- George, S.M.; Ballard-Barbash, R.; Manson, J.E.; Reedy, J.; Shikany, J.M.; Subar, A.F.; Tinker, L.F.; Vitolins, M.; Neuhouser, M.L. Comparing Indices of Diet Quality With Chronic Disease Mortality Risk in Postmenopausal Women in the Women’s Health Initiative Observational Study: Evidence to Inform National Dietary Guidance. Am. J. Epidemiol. 2014, 180, 616–625. [Google Scholar] [CrossRef] [Green Version]
- Reedy, J.; Krebs-Smith, S.M.; Miller, P.E.; Liese, A.D.; Kahle, L.L.; Park, Y.; Subar, A.F. Higher Diet Quality Is Associated with Decreased Risk of All-Cause, Cardiovascular Disease, and Cancer Mortality among Older Adults. J. Nutr. 2014, 144, 881–889. [Google Scholar] [CrossRef] [Green Version]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health Effects of Dietary Risks in 195 Countries, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, A.C.; Rieger, D.K.; Proença, R.P.C. Perspective: Public Health Nutrition Policies Should Focus on Healthy Eating, Not on Calorie Counting, Even to Decrease Obesity. Adv. Nutr. 2019, 10, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Chawla, S.; Tessarolo Silva, F.; Amaral Medeiros, S.; Mekary, R.A.; Radenkovic, D. The Effect of Low-Fat and Low-Carbohydrate Diets on Weight Loss and Lipid Levels: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 3774. [Google Scholar] [CrossRef]
- Mehrabani, H.H.; Salehpour, S.; Amiri, Z.; Farahani, S.J.; Meyer, B.J.; Tahbaz, F. Beneficial Effects of a High-Protein, Low-Glycemic-Load Hypocaloric Diet in Overweight and Obese Women with Polycystic Ovary Syndrome: A Randomized Controlled Intervention Study. J. Am. Coll. Nutr. 2012, 31, 117–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stern, L.; Iqbal, N.; Seshadri, P.; Chicano, K.L.; Daily, D.A.; McGrory, J.; Williams, M.; Gracely, E.J.; Samaha, F.F. The Effects of Low-Carbohydrate versus Conventional Weight Loss Diets in Severely Obese Adults: One-Year Follow-up of a Randomized Trial. Ann. Intern. Med. 2004, 140, 778–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saslow, L.R.; Daubenmier, J.J.; Moskowitz, J.T.; Kim, S.; Murphy, E.J.; Phinney, S.D.; Ploutz-Snyder, R.; Goldman, V.; Cox, R.M.; Mason, A.E.; et al. Twelve-Month Outcomes of a Randomized Trial of a Moderate-Carbohydrate versus Very Low-Carbohydrate Diet in Overweight Adults with Type 2 Diabetes Mellitus or Prediabetes. Nutr. Diabetes 2017, 7, 304. [Google Scholar] [CrossRef]
- Shai, I.; Schwarzfuchs, D.; Henkin, Y.; Shahar, D.R.; Witkow, S.; Greenberg, I.; Golan, R.; Fraser, D.; Bolotin, A.; Vardi, H.; et al. Weight Loss with a Low-Carbohydrate, Mediterranean, or Low-Fat Diet. N. Engl. J. Med. 2008, 359, 229–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouns, F. Overweight and Diabetes Prevention: Is a Low-Carbohydrate–High-Fat Diet Recommendable? Eur. J. Nutr. 2018, 57, 1301–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rumbo-Rodríguez, L.; Sánchez-SanSegundo, M.; Ruiz-Robledillo, N.; Albaladejo-Blázquez, N.; Ferrer-Cascales, R.; Zaragoza-Martí, A. Use of Technology-Based Interventions in the Treatment of Patients with Overweight and Obesity: A Systematic Review. Nutrients 2020, 12, 3634. [Google Scholar] [CrossRef]
- Phillips, N.E.; Mareschal, J.; Schwab, N.; Manoogian, E.N.C.; Borloz, S.; Ostinelli, G.; Gauthier-Jaques, A.; Umwali, S.; Gonzalez Rodriguez, E.; Aeberli, D.; et al. The Effects of Time-Restricted Eating versus Standard Dietary Advice on Weight, Metabolic Health and the Consumption of Processed Food: A Pragmatic Randomised Controlled Trial in Community-Based Adults. Nutrients 2021, 13, 1042. [Google Scholar] [CrossRef]
- Hu, E.A.; Nguyen, V.; Langheier, J.; Shurney, D. Weight Reduction Through a Digital Nutrition and Food Purchasing Platform Among Users With Obesity: Longitudinal Study. J. Med. Internet Res. 2020, 22, e19634. [Google Scholar] [CrossRef] [PubMed]
- Dunford, E.; Trevena, H.; Goodsell, C.; Ng, K.H.; Webster, J.; Millis, A.; Goldstein, S.; Hugueniot, O.; Neal, B. FoodSwitch: A Mobile Phone App to Enable Consumers to Make Healthier Food Choices and Crowdsourcing of National Food Composition Data. JMIR mHealth uHealth 2014, 2, e3230. [Google Scholar] [CrossRef]
- Block, G.; Azar, K.M.; Romanelli, R.J.; Block, T.J.; Hopkins, D.; Carpenter, H.A.; Dolginsky, M.S.; Hudes, M.L.; Palaniappan, L.P.; Block, C.H. Diabetes Prevention and Weight Loss with a Fully Automated Behavioral Intervention by Email, Web, and Mobile Phone: A Randomized Controlled Trial Among Persons with Prediabetes. J. Med. Internet Res. 2015, 17, e4897. [Google Scholar] [CrossRef]
- Haas, K.; Hayoz, S.; Maurer-Wiesner, S. Effectiveness and Feasibility of a Remote Lifestyle Intervention by Dietitians for Overweight and Obese Adults: Pilot Study. JMIR mHealth uHealth 2019, 7, e12289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarroll, R.; Eyles, H.; Ni Mhurchu, C. Effectiveness of Mobile Health (MHealth) Interventions for Promoting Healthy Eating in Adults: A Systematic Review. Prev. Med. 2017, 105, 156–168. [Google Scholar] [CrossRef]
- Wallace, T.C.; Bailey, R.L.; Blumberg, J.B.; Burton-Freeman, B.; Chen, C.O.; Crowe-White, K.M.; Drewnowski, A.; Hooshmand, S.; Johnson, E.; Lewis, R.; et al. Fruits, Vegetables, and Health: A Comprehensive Narrative, Umbrella Review of the Science and Recommendations for Enhanced Public Policy to Improve Intake. Crit. Rev. Food Sci. Nutr. 2020, 60, 2174–2211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puig-Ribera, A.; Martín-Cantera, C.; Puigdomenech, E.; Real, J.; Romaguera, M.; Magdalena-Belio, J.F.; Recio-Rodríguez, J.I.; Rodriguez-Martin, B.; Arietaleanizbeaskoa, M.S.; Repiso–Gento, I.; et al. Screening Physical Activity in Family Practice: Validity of the Spanish Version of a Brief Physical Activity Questionnaire. PLoS ONE 2015, 10, e0136870. [Google Scholar] [CrossRef]
- Recio-Rodriguez, J.I.; Gómez-Marcos, M.A.; Agudo-Conde, C.; Ramirez, I.; Gonzalez-Viejo, N.; Gomez-Arranz, A.; Salcedo-Aguilar, F.; Rodriguez-Sanchez, E.; Alonso-Domínguez, R.; Sánchez-Aguadero, N.; et al. EVIDENT 3 Study: A Randomized, Controlled Clinical Trial to Reduce Inactivity and Caloric Intake in Sedentary and Overweight or Obese People Using a Smartphone Application: Study Protocol. Medicine 2018, 97, e9633. [Google Scholar] [CrossRef]
- Raidl, M.; Spain, K.; Hartman-Cunningham, M.; Lanting, R.; Lockard, M.; Johnson, S.; Spencer, M.; Sant, L.; Welch, J.; Liddil, A. The Healthy Diabetes Plate. Prev. Chronic Dis. 2006, 4, A12. [Google Scholar]
- RedBedca; AESAN BEDCA. Base de Datos Española de Composición De Alimentos. Available online: https://bedca.net/ (accessed on 2 October 2021).
- Burke, L.E.; Wang, J.; Sevick, M.A. Self-Monitoring in Weight Loss: A Systematic Review of the Literature. J. Am. Diet. Assoc. 2011, 111, 92–102. [Google Scholar] [CrossRef] [Green Version]
- Schmidt-Kraepelin, M.; Toussaint, P.A.; Thiebes, S.; Hamari, J.; Sunyaev, A. Archetypes of Gamification: Analysis of MHealth Apps. JMIR mHealth uHealth 2020, 8, e19280. [Google Scholar] [CrossRef]
- de la Fuente-Arrillaga, C.; Ruiz, Z.V.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ Validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- Prochaska, J.; Velicer, W.F. The Transtheoretical Model of Health Behavior Change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Andrés, A.; Saldaña, C.; Gómez-Benito, J. The Transtheoretical Model in Weight Management: Validation of the Processes of Change Questionnaire. OFA 2011, 4, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redán, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 Practice Guidelines for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 2013, 31, 1925–1938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO MONICA Project Principal Investigators The World Health Organization Monica Project (Monitoring Trends and Determinants in Cardiovascular Disease): A Major International Collaboration. J. Clin. Epidemiol. 1988, 41, 105–114. [CrossRef]
- World Medical Association World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [Green Version]
- Recio-Rodriguez, J.I.; Agudo Conde, C.; Calvo-Aponte, M.J.; Gonzalez-Viejo, N.; Fernandez-Alonso, C.; Mendizabal-Gallastegui, N.; Rodriguez-Martin, B.; Maderuelo-Fernandez, J.A.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; et al. The Effectiveness of a Smartphone Application on Modifying the Intakes of Macro and Micronutrients in Primary Care: A Randomized Controlled Trial. EVIDENT II Study. Nutr. 2018, 10, 1473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.K. Intention-to-Treat Concept: A Review. Perspect. Clin. Res. 2011, 2, 109. [Google Scholar] [CrossRef] [PubMed]
- Burke, L.E.; Styn, M.A.; Sereika, S.M.; Conroy, M.B.; Ye, L.; Glanz, K.; Sevick, M.A.; Ewing, L.J. Using MHealth Technology to Enhance Self-Monitoring for Weight Loss: A Randomized Trial. Am. J. Prev. Med. 2012, 43, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Mandracchia, F.; Llauradó, E.; Tarro, L.; del Bas, J.M.; Valls, R.M.; Pedret, A.; Radeva, P.; Arola, L.; Solà, R.; Boqué, N. Potential Use of Mobile Phone Applications for Self-Monitoring and Increasing Daily Fruit and Vegetable Consumption: A Systematized Review. Nutrients 2019, 11, 686. [Google Scholar] [CrossRef] [Green Version]
- Burke, L.E.; Conroy, M.B.; Sereika, S.M.; Elci, O.U.; Styn, M.A.; Acharya, S.D.; Sevick, M.A.; Ewing, L.J.; Glanz, K. The Effect of Electronic Self-Monitoring on Weight Loss and Dietary Intake: A Randomized Behavioral Weight Loss Trial. Obesity 2011, 19, 338–344. [Google Scholar] [CrossRef]
- Hendrie, G.A.; Hussain, M.S.; Brindal, E.; James-Martin, G.; Williams, G.; Crook, A. Impact of a Mobile Phone App to Increase Vegetable Consumption and Variety in Adults: Large-Scale Community Cohort Study. JMIR mHealth uHealth 2020, 8, e14726. [Google Scholar] [CrossRef]
- Mummah, S.; Robinson, T.N.; Mathur, M.; Farzinkhou, S.; Sutton, S.; Gardner, C.D. Effect of a Mobile App Intervention on Vegetable Consumption in Overweight Adults: A Randomized Controlled Trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacios, C.; Torres, M.; López, D.; Trak-Fellermeier, M.A.; Coccia, C.; Pérez, C.M. Effectiveness of the Nutritional App “MyNutriCart” on Food Choices Related to Purchase and Dietary Behavior: A Pilot Randomized Controlled Trial. Nutrients 2018, 10, 1967. [Google Scholar] [CrossRef] [Green Version]
- Maki, K.C.; Beiseigel, J.M.; Jonnalagadda, S.S.; Gugger, C.K.; Reeves, M.S.; Farmer, M.V.; Kaden, V.N.; Rains, T.M. Whole-Grain Ready-to-Eat Oat Cereal, as Part of a Dietary Program for Weight Loss, Reduces Low-Density Lipoprotein Cholesterol in Adults with Overweight and Obesity More than a Dietary Program Including Low-Fiber Control Foods. J. Am. Diet. Assoc. 2010, 110, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Berger, S.; Raman, G.; Vishwanathan, R.; Jacques, P.F.; Johnson, E.J. Dietary Cholesterol and Cardiovascular Disease: A Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2015, 102, 276–294. [Google Scholar] [CrossRef] [Green Version]
- Diabetes Prevention Program Research Group A High-Carbohydrate, High-Fiber, Low-Fat Diet Results in Weight Loss among Adults at High Risk of Type 2 Diabetes. J. Nutr. 2017, 147, 2060–2066. [CrossRef] [Green Version]
- Meyer, K.A.; Kushi, L.H.; Jacobs, D.R., Jr.; Slavin, J.; Sellers, T.A.; Folsom, A.R. Carbohydrates, Dietary Fiber, and Incident Type 2 Diabetes in Older Women. Am. J. Clin. Nutr. 2000, 71, 921–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Călinoiu, L.F.; Vodnar, D.C. Whole Grains and Phenolic Acids: A Review on Bioactivity, Functionality, Health Benefits and Bioavailability. Nutrients 2018, 10, 1615. [Google Scholar] [CrossRef] [Green Version]
- Ambeba, E.J.; Ye, L.; Sereika, S.M.; Styn, M.A.; Acharya, S.D.; Sevick, M.A.; Ewing, L.J.; Conroy, M.B.; Glanz, K.; Zheng, Y.; et al. The Use of MHealth to Deliver Tailored Messages Reduces Reported Energy and Fat Intake. J. Cardiovasc. Nurs. 2015, 30, 35–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carson, J.A.S.; Lichtenstein, A.H.; Anderson, C.A.M.; Appel, L.J.; Kris-Etherton, P.M.; Meyer, K.A.; Petersen, K.; Polonsky, T.; Van Horn, L. Dietary Cholesterol and Cardiovascular Risk: A Science Advisory From the American Heart Association. Circulation 2020, 141, e39–e53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recio-Rodriguez, J.I.; Agudo-Conde, C.; Martin-Cantera, C.; González-Viejo, M.N.; Fernandez-Alonso, M.C.; Arietaleanizbeaskoa, M.S.; Schmolling-Guinovart, Y.; Maderuelo-Fernandez, J.-A.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; et al. Short-Term Effectiveness of a Mobile Phone App for Increasing Physical Activity and Adherence to the Mediterranean Diet in Primary Care: A Randomized Controlled Trial (EVIDENT II Study). J. Med. Internet Res. 2016, 18, e6814. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Erdt, M.; Lee, J.; Cao, Y.; Naharudin, N.B.; Theng, Y.-L. Effectiveness of EHealth Nutritional Interventions for Middle-Aged and Older Adults: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2021, 23, e15649. [Google Scholar] [CrossRef]
- Miller, T.M.; Abdel-Maksoud, M.F.; Crane, L.A.; Marcus, A.C.; Byers, T.E. Effects of Social Approval Bias on Self-Reported Fruit and Vegetable Consumption: A Randomized Controlled Trial. Nutr. J. 2008, 7, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumville, J.C.; Torgerson, D.J.; Hewitt, C.E. Reporting Attrition in Randomised Controlled Trials. BMJ 2006, 332, 969–971. [Google Scholar] [CrossRef] [Green Version]



| Intervention (n = 318) | Control (n = 332) | p-Value | ||
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Age, years | 47.7 ± 10.1 | 48.9 ± 9.2 | 0.130 | |
| Sex, n (%) | Men | 104 (32.7) | 101(30.4) | 0.555 |
| Women | 214 (67.3) | 231 (69.6) | ||
| Smoking status, n (%) | Non smoker | 124 (39.0) | 139 (41.9) | 0.560 |
| Smoker | 68 (21.4) | 75 (22.6) | ||
| Former smoker | 126 (39.6) | 118 (35.5) | ||
| Marital status, n (%) | Single | 60 (18.9) | 74 (22.3) | 0.736 |
| Married | 222 (69.8) | 222 (66.9) | ||
| Divorced | 31 (9.7) | 30 (9.0) | ||
| Widowed | 5 (1.6) | 6 (1.8) | ||
| BMI (kg/m2) | 33.1 ± 3.4 | 33.0 ± 3.6 | 0.607 | |
| SBP (mmHg) | 119 ± 15 | 120 ± 16 | 0.402 | |
| DBP (mmHg) | 79 ± 9 | 81 ± 10 | 0.091 | |
| Heart rate (lpm) | 72 ± 12 | 74 ± 12 | 0.061 | |
| Total Cholesterol (mg/dL) | 198 ± 36 | 202 ± 40 | 0.230 | |
| HDL Cholesterol (mg/dL) | 51 ± 13 | 52 ± 12 | 0.557 | |
| LDL Cholesterol (mg/dL) | 122 ± 31 | 125 ± 36 | 0.247 | |
| Triglycerides (mg/dL) | 131 ± 73 | 127 ± 63 | 0.513 | |
| Glycaemia (mg/dL) | 93 ± 14 | 95 ± 21 | 0.190 | |
| HbA1c (%) | 5.4 ± 0.4 | 5.5 ± 0.5 | 0.058 | |
| Hypertension, n (%) | 88 (27.7) | 116 (35.0) | 0.052 | |
| Dyslipidemia, n (%) | 73 (23.4) | 87 (26.5) | 0.411 | |
| Diabetes Mellitus n (%) | 5 (1.7) | 4 (1.3) | 0.748 | |
| Motivation, state to change, n (%) | Not ready | 15 (4.7) | 12 (3.6) | 0.754 |
| Ready | 167 (52.5) | 173 (52.1) | ||
| Right moment | 136 (42.8) | 147 (44.3) |
| Intervention Group (n = 293) | Control Group (n = 308) | |||||
|---|---|---|---|---|---|---|
| Baseline Mean (SD) | 3 Months Mean Diff. (95 CI%) | 12 Months Mean Diff. (95 CI%) | Baseline Mean (SD) | 3 Months Mean Diff. (95 CI%) | 12 Months Mean Diff. (95 CI%) | |
| Carbohydrates (g/day) | 242.0 (81.9) | −18.3 (−29.4 to −7.3) ** | −31.4 (−43.6 to −19.2) ** | 235.8 (86.9) | −22.1 (−32.2 to −12.0) ** | −27.2 (−38.5 to −15.9) ** |
| Proteins (g/day) | 102.4 (26.2) | −3.3 (−6.3 to −0.3) * | −8.8 (−12.4 to −5.1) ** | 102.0 (24.8) | −2.6 (−5.9 to 0.7) | −3.9 (−7.4 to −0.5) * |
| Total fat (g/day) | 107.6 (35.9) | −13.4 (−17.4 to −9.4) ** | −15.2 (−20.3 to −10.0) ** | 106.8 (35.3) | −9.4 (−13.6 to −5.3) ** | −10.4 (−15.2 to −5.7) ** |
| Monounsaturated fatty acids (g/day) | 48.5 (18.2) | −6.6 (−8.7 to −4.5) ** | −7.0 (−9.7 to −4.2) ** | 47.6 (17.4) | −3.9 (−6.0 to −1.8) ** | −5.0 (−7.3 to −2.7) ** |
| Polyunsaturated fatty acids (g/day) | 16.8 (6.8) | −1.2 (−2.0 to −0.4) ** | −1.3 (−2.4 to −0.2) * | 16.8 (7.4) | −1.7 (−2.6 to −0.8) ** | −1.0 (−2.1 to 0.2) |
| Saturated fatty acids (g/day) | 30.7 (10.6) | −4.5 (−5.6 to −3.3) ** | −5.6 (−7.0 to −4.2) ** | 30.7 (10.7) | −3.3 (−4.5 to −2.0) ** | −3.7 (−5.1 to −2.3) ** |
| Trans fatty acids (g/day) | 0.8 (0.4) | −0.2 (−0.2 to −0.1) ** | −0.2 (−0.3 to −0.2) ** | 0.9 (0.5) | −0.2 (−0.2 to −0.1) ** | −0.2 (−0.2 to −0.1) ** |
| Cholesterol (mg/day) | 475.2 (144.4) | −30.7 (−48.5 to −12.8) ** | −46.1 (−66.7 to −25.5) ** | 462.2 (139.0) | −14.6 (−33.0 to 3.8) | −15.3 (−36.0 to 5.4) |
| Dietary fiber (g/day) | 23.8 (8.3) | 1.1 (0.1 to 2.0) * | 0.5 (−0.6 to 1.6) | 23.0 (8.5) | 0.4 (−0.5 to 1.3) | 0.8 (−0.3 to 1.8) |
| Alcohol (g/day) | 6.8 (9.0) | 0.4 (−0.5 to 1.4) | 0.3 (−0.8 to 1.4) | 6.9 (10.2) | −0.9 (−1.8 to 0.1) | −0.6 (−1.6 to 0.3) |
| Energy (kcal/day) | 2394.1 (676.4) | −204.2 (−285.5 to −122.9) ** | −295.3 (−391.6 to −198.9) ** | 2360.0 (681.1) | −189.8 (−268.9 to −110.7) ** | −222.9 (−310.6 to −135.1) ** |
| Mean Difference (IG–CG) 3 Months (95% CI) | Mean Difference (IG–CG) 12 Months (95% CI) | p for Trend | |
|---|---|---|---|
| Carbohydrates (g/day) | 3.8 (−11.1 to 18.7) | −4.2 (−20.8 to 12.4) | 0.696 |
| Proteins (g/day) | −0.7 (−5.1 to 3.7) | −4.8 (−9.8 to 0.2) | 0.071 |
| Total fat (g/day) | −4.0 (−9.7 to 1.8) | −4.7 (−11.7 to 2.2) | 0.316 |
| Monounsaturated fatty acids (g/day) | −2.7 (−5.7 to 0.2) | −1.9 (−5.6 to 1.7) | 0.208 |
| Polyunsaturated fatty acids (g/day) | 0.5 (−0.7 to 1.8) | −0.3 (−1.9 to 1.3) | 0.396 |
| Saturated fatty acids (g/day) | −1.2 (−2.9 to 0.5) | −1.9 (−3.9 to 0.1) | 0.073 |
| Trans fatty acids (g/day) | 0.0 (−0.1 to 0.0) | 0.0 (−0.1 to 0.0) | 0.253 |
| Cholesterol (mg/day) | −16.1 (−41.7 to 9.5) | −30.8 (−59.9 to −1.7) * | 0.043 |
| Dietary fiber (g/day) | 0.6 (−0.7 to 2.0) | −0.2 (−1.8 to 1.3) | 0.431 |
| Alcohol (g/day) | 1.3 (−0.1 to 2.7) | 0.9 (−0.5 to 2.4) | 0.328 |
| Energy (kcal/day) | −14.3 (−127.5 to 98.8) | −72.4 (−202.1 to 57.3) | 0.470 |
| Intervention Group (n = 293) | Control Group (n =308) | |||||
|---|---|---|---|---|---|---|
| Baseline | 3 Months Mean Diff. (95 CI%) | 12 Months Mean Diff. (95 CI%) | Baseline | 3 Months Mean Diff. (95 CI%) | 12 Months Mean Diff. (95 CI%) | |
| Vegetables (g/day) | 259.8 ± 129.7 | 6.9 (−7.5 to 21.4) | 24.8 (7.9 to 41.7) * | 255.4 ± 119.7 | 16.4 (3.6 to 29.3) * | 25.4 (8.7 to 42.1) ** |
| Fresh fruits (g/day) | 253.4 ± 133.7 | 13.9 (−2.5 to 30.3) | 34.3 (12.4 to 56.1) * | 249.0 ± 142.3 | 25.3 (8.5 to 42.2) ** | 37.9 (16.0 to 59.8) ** |
| Legumes (g/day) | 21.2 ± 10.8 | 0.3 (−1.2 to 1.9) | −0.4 (−2.0 to 1.1) | 20.7 ± 9.9 | 2.2 (0.5 to 3.9) ** | 0.0 (−1.9 to 1.9) |
| White meat (g/day) | 68.4 ± 34.7 | 2.0 (−3.4 to 7.3) | 2.2 (−3.6 to 8.0) | 69.5 ± 35.8 | 5.9 (0.3 to 11.5) * | 6.1 (−0.3 to 12.6) |
| Red meat (g/day) | 67.0 ± 38.9 | −3.6 (−8.4 to 1.1) | −9.4 (−15.9 to −2.9) ** | 70.6 ± 38.3 | −3.1 ( −7.9 to 1.7) | −8.2 (−14.1 to −2.4) ** |
| Fish (g/day) | 107.4 ± 58.3 | 2.8 (−3.5 to 9.1) | −3.2 (−10.7 to 4.2) | 104.8 ± 51.3 | 3.7 (3.7 to 11.1) | 5.4 (−1.8 to 12.6) |
| Nuts (g/day) | 12.7 ± 15.6 | 1.4 (−0.3 to 3.1) | 2.4 (0.0 to 4.8) * | 12.7 ± 16.6 | −0.8 (−2.7 to 1.1) | 2.4 (0.0 to 4.8) |
| Olive oil (g/day) | 27.3 ± 18.6 | −3.6 (−6.0 to −1.2) ** | −2.0 (−5.0 to 1.0) | 25.7 ± 17.1 | −0.9 (−3.2 to 1.4) | −2.7 (−5.3 to −0.1) * |
| Dairy (g/day) | 344.0 ± 188.5 | −9.1 (−32.7 to 14.5) | −58.6 (−85.5 to −31.7) ** | 346.9 ± 200.3 | −17.3 (−38.2 to 3.6) | −43.0 (−67.5 to −18.5) ** |
| Full-fat dairy (g/day) | 102.2 ± 107.8 | −20.8 (−34.8 to −6.8) ** | −26.6 (−39.8 to −13.3) | 106.6 ± 119.9 | −9.3 (−19.3 to 0.7) | −3.3 (−17.7 to 11.1) |
| Wholemeal bread (g/day) | 23.4 ± 38.0 | 16.3 (9.7 to 22.8) ** | 7.2 (0.3 to 14.0) * | 19.9 ± 39.3 | 1.5 (−3.6 to 6.7) | 3.9 (−3.4 to 11.1) |
| Whole-grain cereals (g/day) | 26.6 ± 39.5 | 17.4 (10.7 to 24.0) ** | 7.2 (−0.1 to 14.5) | 22.9 ± 40.4 | 1.7 (−3.4 to 6.8) | 3.8 (−3.4 to 11.0) |
| Confectionery (g/day) | 48.4 ± 40.3 | −21.7 (−26.8 to −16.7) ** | −22.8 (−28.3 to −17.4) ** | 46.6 ± 40.1 | −16.0 (−20.6 to −11.4) ** | −17.0 (−22.5 to −11.4) ** |
| Industrial pastries (g/day) | 30.5 ± 29.5 | −10.2 (−14.0 to −6.4) ** | −10.2 (−14.3 to −6.2) ** | 31.4 ± 32.4 | −8.2 (−11.6 to −4.7) ** | −9.3 (−13.6 to −5.0) ** |
| Sweetened beverages (g/day) | 34.4 ± 73.0 | −10.0(−19.8 to −0.1) | −12.1 (−20.6 to −3.6) ** | 38.2 ± 76.3 | −10.2 (−21.1 to 0.7) | −15.4 (−26.5 to −4.3) ** |
| Sodium (mg/ day) | 2638.2 ± 893.0 | −229.7 (−338.1 to −121.3) ** | −382.6 (−503.4 to −261.8) ** | 2574.4 ± 894.9 | −240.5 (−351.2 to −129.8) ** | −268.6 (−389.2 to −147.9) ** |
| Sugar (g/day) | 8.1 ± 13.0 | −1.9 (−3.5 to −0.3) * | −2.6 (−4.3 to −0.8) ** | 8.7 ± 14.7 | −2.5 (−4.0 to −1.0) ** | −2.2 (−3.8 to −0.6) ** |
| Mean Difference (IG–CG) 3 Months (95% CI) | Mean Difference (IG–CG) 12 Months (95% CI) | p for Trend | |
|---|---|---|---|
| Vegetables (g/day) | −9.5 (−28.8 to 9.8) | −0.6 (−24.3 to 23.1) | 0.716 |
| Fresh fruits (g/day) | −11.5 (−34.9 to 12.0) | −3.6 (−34.5 to 27.3) | 0.603 |
| Legumes (g/day) | −1.9 (−4.2 to 0.4) | −0.4 (−2.9 to 2.0) | 0.373 |
| White meat (g/day) | −4.0 (−11.7 to 3.7) | −3.9 (−12.6 to 4.7) | 0.508 |
| Red meat (g/day) | −0.5 (−7.2 to 6.2) | −1.2 (−9.9 to 7.5) | 0.528 |
| Fish (g/day) | −0.9 (−10.6 to 8.8) | −8.6 (−18.9 to 1.7) | 0.195 |
| Nuts (g/day) | 2.3 (−0.3 to 4.8) | 0.1 (−3.3 to 3.4) | 0.263 |
| Dairy (g/day) | 8.3 (−23.2 to 39.7) | −15.6 (−51.8 to 20.6) | 0.428 |
| Full-fat dairy (g/day) | −11.5 (−28.7 to 5.7) | −23.3 (−42.8 to −3.8) * | 0.043 |
| Olive oil (g/day) | −2.7 (−6.0 to 0.6) | 0.7 (−3.3 to 4.7) | 0.218 |
| Wholemeal bread (g/day) | 14.7 (6.4 to 23.0) * | 3.3 (−6.7 to 13.3) | 0.005 |
| Whole-grain cereals (g/day) | 15.7 (7.3 to 24.1) * | 3.4 (−6.8 to 13.7) | 0.004 |
| Confectionery (g/day) | −5.7 (−12.6 to 1.1) | −5.9 (−13.7 to 1.9) | 0.112 |
| Industrial pastries (g/day) | −2.1 (−7.2 to 3.1) | −1.0 (−6.8 to 4.9) | 0.304 |
| Sweetened beverages (g/day) | 0.2 (−14.4 to 14.9) | 3.3 (−10.7 to 17.3) | 0.860 |
| Sodium (mg/ day) | 10.8 (−143.7 to 165.3) | −114.0 (−284.3 to 56.2) | 0.463 |
| Sugar (g/day) | 0.6 (−1.6 to 2.7) | −0.4 (−2.8 to 2.0) | 0.293 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lugones-Sánchez, C.; Recio-Rodríguez, J.I.; Menéndez-Suárez, M.; Saz-Lara, A.; Ramirez-Manent, J.I.; Sánchez-Calavera, M.A.; Gómez-Sánchez, L.; Rodríguez-Sánchez, E.; García-Ortiz, L.; Evident 3 Investigators Group. Effect of a Multicomponent mHealth Intervention on the Composition of Diet in a Population with Overweight and Obesity—Randomized Clinical Trial EVIDENT 3. Nutrients 2022, 14, 270. https://doi.org/10.3390/nu14020270
Lugones-Sánchez C, Recio-Rodríguez JI, Menéndez-Suárez M, Saz-Lara A, Ramirez-Manent JI, Sánchez-Calavera MA, Gómez-Sánchez L, Rodríguez-Sánchez E, García-Ortiz L, Evident 3 Investigators Group. Effect of a Multicomponent mHealth Intervention on the Composition of Diet in a Population with Overweight and Obesity—Randomized Clinical Trial EVIDENT 3. Nutrients. 2022; 14(2):270. https://doi.org/10.3390/nu14020270
Chicago/Turabian StyleLugones-Sánchez, Cristina, José I. Recio-Rodríguez, Marta Menéndez-Suárez, Alicia Saz-Lara, José I. Ramirez-Manent, María A. Sánchez-Calavera, Leticia Gómez-Sánchez, Emiliano Rodríguez-Sánchez, Luis García-Ortiz, and Evident 3 Investigators Group. 2022. "Effect of a Multicomponent mHealth Intervention on the Composition of Diet in a Population with Overweight and Obesity—Randomized Clinical Trial EVIDENT 3" Nutrients 14, no. 2: 270. https://doi.org/10.3390/nu14020270
APA StyleLugones-Sánchez, C., Recio-Rodríguez, J. I., Menéndez-Suárez, M., Saz-Lara, A., Ramirez-Manent, J. I., Sánchez-Calavera, M. A., Gómez-Sánchez, L., Rodríguez-Sánchez, E., García-Ortiz, L., & Evident 3 Investigators Group. (2022). Effect of a Multicomponent mHealth Intervention on the Composition of Diet in a Population with Overweight and Obesity—Randomized Clinical Trial EVIDENT 3. Nutrients, 14(2), 270. https://doi.org/10.3390/nu14020270