
Fetuin-A and Its Association with Anthropometric, Atherogenic, and Biochemical Parameters and Indices among Women with Polycystic Ovary Syndrome


 , and
, and
Abstract
1. Introduction
2. Methods
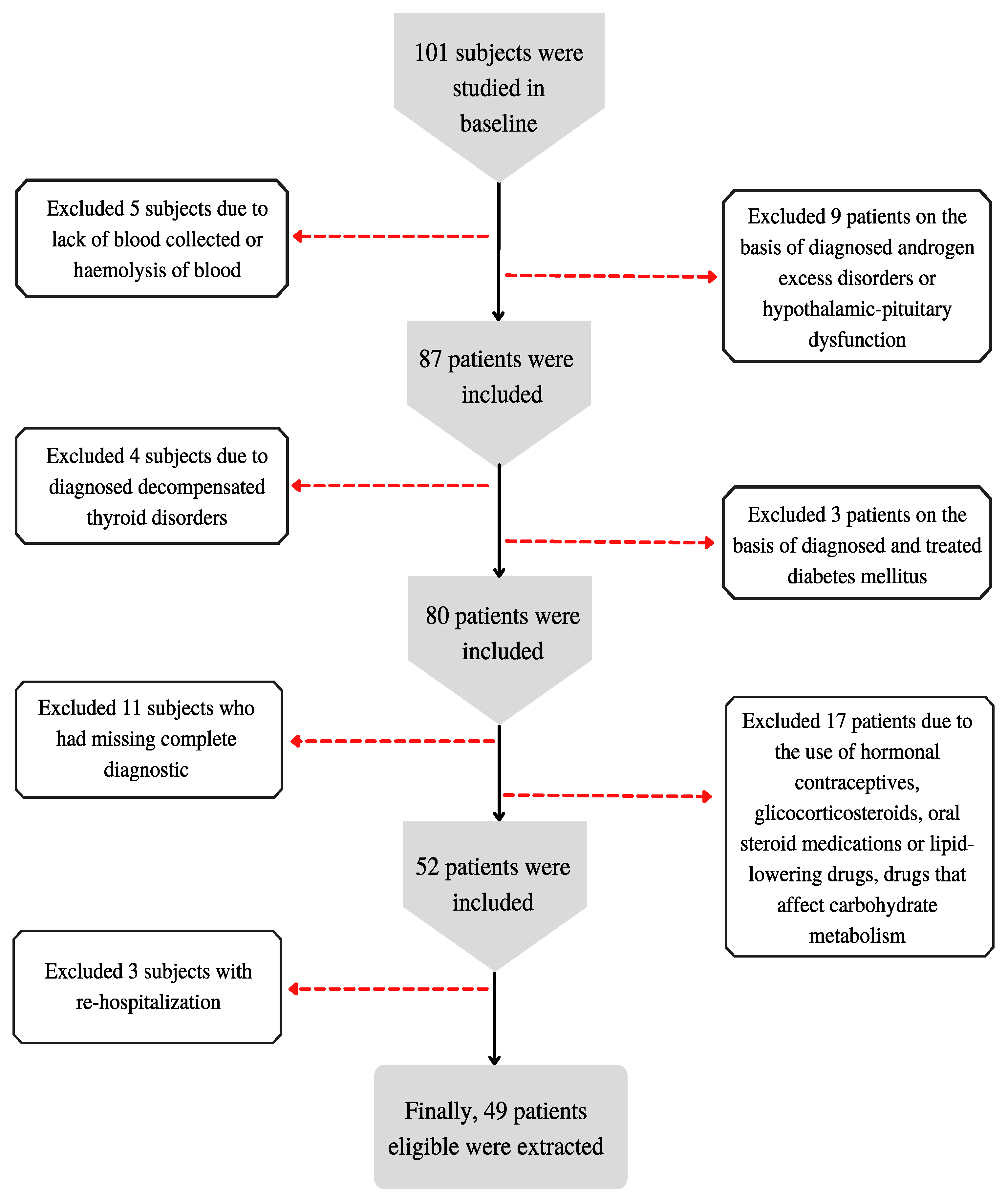
2.1. Study Population
2.2. Methods
2.3. Laboratory Measurements
2.4. Statistical Analysis
3. Results
Characteristics of the Study Group
4. Discussion
5. Study Strength and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, F.; Yao, L.; Wu, H.; Cao, S. Analysis on endocrine and metabolic features of different phenotypes of polycystic ovary syndrome patients. Pak. J. Pharm. Sci. 2016, 29, 1735–1738. [Google Scholar] [PubMed]
- Yoo, H.J.; Choi, K.M. Hepatokines as a link between obesity and cardiovascular diseases. Diabetes Metab. J. 2015, 39, 10–15. [Google Scholar] [CrossRef] [PubMed]
- El-Deeb, T.S.; Bakkar, S.M.; Eltoony, L.; Zakhary, M.M.; Kamel, A.A.; Nafee, A.M.; Hetta, H.F. The adipokine Chemerin and Fetuin-a serum levels in type 2 diabetes mellitus: Relation to obesity and inflammatory markers. Egypt J. Immunol. 2018, 25, 191–202. [Google Scholar] [PubMed]
- Díaz, M.; Gallego-Escuredo, J.M.; López-Bermejo, A.; de Zegher, F.; Villarroya, F.; Ibáñez, L. Low-dose spironolactone-pioglitazone-metformin normalizes circulating Fetuin-a concentrations in adolescent girls with polycystic ovary syndrome. Int. J. Endocrinol. 2018, 2018, 4192940. [Google Scholar] [CrossRef] [PubMed]
- Khadir, A.; Kavalakatt, S.; Madhu, D.; Hammad, M.; Devarajan, S.; Tuomilehto, J.; Tiss, A. Fetuin-A levels are increased in the adipose tissue of diabetic obese humans but not in circulation. Lipids Health Dis. 2018, 17, 291. [Google Scholar] [CrossRef]
- Bayramoğlu, E.; Çetinkaya, S.; Özalkak, S.; Kurnaz, E.; Demirci, G.; Öztürk, H.S.; Savaş-Erdeve, Ş.; Aycan, Z. Evaluation of the pathophysiological role of Fetuin A levels in adolescents with polycystic ovary syndrome. J. Pediatr. Endocrinol. Metab. 2021, 34, 911–916. [Google Scholar] [CrossRef]
- Ramanjaneya, M.; Bensila, M.; Bettahi, I.; Jerobin, J. Dynamic Changes in Circulating Endocrine FGF19 Subfamily and Fetuin-A in Response to Intralipid and Insulin Infusions in Healthy and PCOS Woman. Front. Endocrinol. 2020, 11, 1568500. [Google Scholar] [CrossRef]
- Gupta, V.; Mishra, S.; Mishra, S.; Gupta, V. A ratio, Insulin resistance and metabolic risk in women with polycystic ovarian syndrome. Diabetes Metab. Syndr. 2017, 11 (Suppl. S2), S697–S701. [Google Scholar] [CrossRef]
- Gunning, M.N.; Fauser, B.C.J.M. Are women with polycystic ovary syndrome at increased cardiovascular disease risk later in life? Climacteric 2017, 20, 222–227. [Google Scholar] [CrossRef]
- Panico, A.; Messina, G.; Lupoli, G.A.; Lupoli, R.; Cacciapuoti, M.; Moscatelli, F.; Esposito, T.; Villano, I.; Valenzano, A.; Monda, V.; et al. Quality of life in overweight (obese) and normal-weight women with polycystic ovary syndrome. Patient Prefer. Adherence 2017, 11, 423–429. [Google Scholar] [CrossRef]
- Cosar, E.; Üçok, K.; Akgün, L.; Koken, G.; Sahin, F.K.; Arioz, D.T.; Baş, O. Body fat composition and distribution in women with polycystic ovary syndrome. Gynecol. Endocrinol. 2008, 24, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Yin, Q.; Cao, J.; Zhang, B. Obesity contributes more to increasing ApoB/ApoA1 ratio than hyperandrogenism in PCOS women aged 20–38 years in China. Exp. Ther. Med. 2017, 13, 1337–1342. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Naito, C.; Hashimoto, M.; Watanabe, K.; Shirai, R.; Takahashi, Y.; Kojima, M.; Watanabe, R.; Sato, K.; Iso, Y.; Matsuyama, T.-A.; et al. Facilitatory effects of fetuin-A on atherosclerosis. Atherosclerosis 2016, 246, 344–351. [Google Scholar] [CrossRef]
- Bourebaba, L.; Marycz, K. Pathophysiological Implication of Fetuin-A Glycoprotein in the Development of Metabolic Disorders: A Concise Review. J. Clin. Med. 2019, 8, 2033. [Google Scholar] [CrossRef]
- Sangouni, A.A.; Sasanfar, B.; Ghadiri-Anari, A.; Hosseinzadeh, M. Effect of l-carnitine supplementation on liver fat content and cardiometabolic indices in overweight/obese women with polycystic ovary syndrome: A randomized controlled trial. Clin. Nutr. ESPEN 2021, 46, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, E.; Spiga, R.; Rubino, M.; Averta, C.; Rotundo, S.; Segura-Garcìa, C.; Mannino, G.C.; Sesti, G.; Andreozzi, F. Effects of Alpha-2-HS-glycoprotein on cognitive and emotional assessment in prediabetic and diabetic subjects. J. Affect. Disord. 2021, 282, 700–706. [Google Scholar] [CrossRef]
- Westenfeld, R.; Schäfer, C.; Krüger, T.; Haarmann, C.; Schurgers, L.J.; Reutelingsperger, C.; Ivanovski, O.; Drueke, T.; Massy, Z.A.; Ketteler, M.; et al. Fetuin-A protects against atherosclerotic calcification in CKD. J. Am. Soc. Nephrol. 2009, 20, 1264–1274. [Google Scholar] [CrossRef]
- Gurbuz, T.; Alanya Tosun, S.; Cebi, A.; Gokmen, O.; Usta, M. Investigating Fetuin-A and Paraoxonase-1 Activity as Markers in Polycystic Ovary Syndrome Based on Body Mass Index: A Prospective Case-Control Study. Cureus 2021, 13, e18553. [Google Scholar] [CrossRef]
- bin Ali, A.; Zhang, Q.; Lim, Y.K.; Fang, D.; Retnam, L.; Lim, S.K. Expression of major HDL-associated antioxidant PON-1 is gender dependent and regulated during inflammation. Free Radic. Biol. Med. 2003, 34, 824–829. [Google Scholar] [CrossRef]
- Icer, M.A.; Yıldıran, H. Effects of fetuin-A with diverse functions and multiple mechanisms on human health. Clin. Biochem. 2021, 88, 1–10. [Google Scholar] [CrossRef]
- Pérez-Sotelo, D.; Roca-Rivada, A.; Larrosa-García, M.; Castelao, C.; Baamonde, I.; Baltar, J.; Crujeiras, A.B.; Seoane, L.M.; Casanueva, F.F.; Pardo, M. Visceral and subcutaneous adipose tissue express and secrete functional alpha2hsglycoprotein (fetuin a) especially in obesity. Endocrine 2017, 55, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Sartori, C.; Lazzeroni, P.; Merli, S.; Patianna, V.D.; Viaroli, F.; Cirillo, F.; Amarri, S.; Street, M.E. From Placenta to Polycystic Ovarian Syndrome: The Role of Adipokines. Mediat. Inflamm. 2016, 2016, 4981916. [Google Scholar] [CrossRef] [PubMed]
- Enli, Y.; Fenkci, S.M.; Fenkci, V.; Oztekin, O. Serum Fetuin-A levels, insulin resistance and oxidative stress in women with polycystic ovary syndrome. Gynecol. Endocrinol. 2013, 29, 1036–1039. [Google Scholar] [CrossRef] [PubMed]
- Abali, R.; Celik, C.; Tasdemir, N.; Guzel, S.; Alpsoy, S.; Yuksel, A.; Celik, E. The serum protein α2-Heremans-Schmid glycoprotein/fetuin-a concentration and carotid intima-media thickness in women with polycystic ovary syndrome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 169, 45–49. [Google Scholar] [CrossRef]
- Gulhan, I.; Bozkaya, G.; Oztekin, D.; Uyar, I.; Kebapcilar, A.G.; Pamuk, B. Serum Fetuin-A levels in women with polycystic ovary syndrome. Arch. Gynecol. Obstet. 2012, 286, 1473–1476. [Google Scholar] [CrossRef]
- Głuszek, S.; Cieśla, E.; Głuszek-Osuch, M.; Kozieł, D.; Kiebzak, W.; Wypchło, Ł.; Suliga, E. Anthropometric indices and cut-off points in the diagnosis of metabolic disorders. PLoS ONE 2020, 15, e0235121. [Google Scholar] [CrossRef]
- Brończyk-Puzoń, A.; Jagielski, P.; Kulik-Kupka, K.; Koszowska, A.; Nowak, J.; Zubelewicz-Szkodzińska, B. Usefulness of a new anthropometric indicator—VAI (Visceral Adiposity Index) in the evaluation of metabolic and hormonal disorders in women with polycystic ovary syndrome. Adv. Clin. Exp. Med. 2017, 26, 825–828. [Google Scholar] [CrossRef]
- Li, Y.-W.; Kao, T.-W.; Chang, P.-K.; Chen, W.-L.; Wu, L.-W. Atherogenic index of plasma as predictors for metabolic syndrome, hypertension and diabetes mellitus in Taiwan citizens: A 9-year longitudinal study. Sci. Rep. 2021, 11, 9900. [Google Scholar] [CrossRef]
- Walczyk, T. Anthropometric indicators of obesity. Are the new indicators a better predictor of body fat content than BMI? J. Educ. Health Sport 2021, 11, 11–23. [Google Scholar] [CrossRef]
- Wilczyński, M.; Domańska-Senderowska, D.; Kassassir-Ćwiklak, S.A.; Janas, Ł.; Malinowski, J.; Wilczyński, R. A body shape index (ABSI) and endometrial pathology. Women Health 2021, 61, 313–321. [Google Scholar] [CrossRef]
- Bawadi, H.; Abouwatfa, M.; Alsaeed, S.; Kerkadi, A.; Shi, Z. Body Shape Index Is a Stronger Predictor of Diabetes. Nutrients 2019, 11, 1018. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Waist Circumference and Waist-Hip Ratio; Report of a WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut Off Points. [Updated 2021 Jun 29]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK541070/ (accessed on 12 July 2022).
- Lizak, D.; Budzowski, A.; Seń, M.; Czarny, W. Anthropometric measures of body composition used in obesity diagnosis—An overview. Hyg. Pub. Health 2016, 51, 124–280. [Google Scholar]
- Ahn, N.; Baumeister, S.E.; Amann, U.; Rathmann, W.; Peters, A.; Huth, C.; Thorand, B.; Meisinger, C. Visceral adiposity index (VAI), lipid accumulation product (LAP), and product of triglycerides and glucose (TyG) to discriminate prediabetes and diabetes. Sci. Rep. 2019, 9, 9693. [Google Scholar] [CrossRef]
- Gumprecht, J. Zalecenia kliniczne u chorych na cukrzycę 2016. Stanowisko Polskiego Towarzystwa Diabetologicznego. Diabetol. Klin. 2016, 5, A1–A76. [Google Scholar]
- Kośmicki, M. Zaburzenia lipidowe u pacjentów z chorobami układu sercowo- naczyniowego. Część I: Leczenie statynami. Przew. Lek. 2000, 3, 35–46. [Google Scholar]
- Barber, T.M.; McCarthy, M.I.; Wass, J.A.H.; Franks, S. Obesity and polycystic ovary syndrome. Clin. Endocrinol. 2006, 65, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Wassel, C.L.; Chertow, G.M.; Koster, A.; Johnson, K.C.; Tylavsky, F.A.; Cauley, J.A.; Cummings, S.R.; Harris, T.B.; Shlipak, M.G.; et al. Health Aging and Body Composition Study: Fetuin-A and change in body composition in older persons. J. Clin. Endocrinol. Metab. 2009, 94, 4492–4498. [Google Scholar] [CrossRef]
- Brix, J.M.; Stingl, H.; Höllerl, F.; Schernthaner, G.H.; Kopp, H.P.; Schernthaner, G. Elevated Fetuin-A concentrations in morbid obesity decrease after dramatic weight loss. J. Clin. Endocrinol. Metab. 2010, 95, 4877–4881. [Google Scholar] [CrossRef]
- Kozakowski, J.; Jeske, W.; Zgliczyński, W. Fetuin-A levels in lean and obese women with polycystic ovary syndrome. Endokrynol. Pol. 2014, 65, 371–376. [Google Scholar] [CrossRef][Green Version]
- Nawrocka-Rutkowska, J.; Szydłowska, I.; Jakubowska, K.; Olszewska, M.; Chlubek, S.; Szczuko, M.; Starczewski, A. The role of Oxidative Stress in the Risk of Cardiovascular Disease and Identification of Risk Factors Using AIP and Castelli Atherogenicity Indicators in Patients with PCOS. Biomedicines 2022, 10, 1700. [Google Scholar] [CrossRef]
- Kheirollahi, A.; Teimouri, M.; Karimi, M.; Vatannejad, A.; Moradi, N.; Borumandnia, N.; Sadeghi, A. Evalutation of lipid ratios and triglyceride-glucose index as risk markers of insulin resistance in Iranian polycystic ovary syndrome women. Lipids Health Dis. 2020, 19, 235. [Google Scholar] [CrossRef] [PubMed]
- Galluzzo, A.; Amato, M.C.; Giordano, C. Insulin resistance and polycystic ovary syndrome. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Aroner, S.A.; Mukamal, K.J.; St-Jules, D.E.; Budoff, M.J.; Katz, R.; Criqui, M.H.; Allison, M.A.; de Boer, I.H.; Siscovick, D.S.; Ix, J.H.; et al. Fetuin-A and Risk of Diabetes Independent of Liver Fat Content: The Multi-Ethnic Study of Atherosclerosis. Am. J. Epidemiol. 2017, 185, 54–64. [Google Scholar] [CrossRef]
- Iyidir, O.T.; Degertekin, C.K.; Yilmaz, B.A.; Altinova, A.E.; Toruner, F.B.; Bozkurt, N.; Ayvaz, G.; Akturk, M. Serum levels of fetuin A are increased in women with gestational diabetes mellitus. Arch. Gynecol. Obstet. 2015, 291, 933–937. [Google Scholar] [CrossRef]
- Ehrmann, D.A.; Liljenquist, D.R.; Kasza, K.; Azziz, R.; Legro, R.S.; Ghazzi, M.N. Prevalence and predictors of the metabolic syndrome in women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2006, 91, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Shlipak, M.G.; Brandenburg, V.M.; Ali, S.; Ketteler, M.; Whooley, M.A. Association Between Human Fetuin-A and the Metabolic Syndrome. Circulation 2006, 113, 1760–1767. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Tested Measurements and Anthropometric Indicators | Standards | Interpretation of Standards | References |
|---|---|---|---|
| WC (cm) | >88 cm | significantly increased risk of metabolic complications | [32] |
| BMI Index (kg/m2) | <18.5 kg/m2 | underweight | [33] |
| 18.5–24.9 kg/m2 | normal body weight | ||
| 25.0–29.9 kg/m2 | overweight | ||
| 30.0–34.9 kg/m2 | I obesity | ||
| 35.0–39.9 kg/m2 | II obesity | ||
| ≥40.0 kg/m2 | III obesity | ||
| WHR | ≥0.85 | increasing the risk of metabolic complications | [32] |
| WHtR | ≥0.5 | abdominal obesity | [32] |
| increased risk | |||
| cardiovascular diseases | |||
| and diabetes | |||
| BAI [%] | <21% | underweight | [34] |
| 21–33% | standard | ||
| >33% | overweight | ||
| >39% | obesity | ||
| VAI | >1.675 | risk of metabolic diseases | [27] |
| LAP | <41.30 | discrimination of prediabetes/diabetes | [35] |
| BRI | <4.910 | risk of metabolic diseases | [26] |
| ABSI | <0.076 | risk of diabetes and CVD | [26,29] |
| ABSI z-score | <−0.868 | mortality risk—very low | [29,30,31] |
| −0.868 and −0.272 | mortality risk—low | ||
| −0.272 and +0.229 | mortality risk—average | ||
| 0.229 and 0.798 | mortality risk—high | ||
| >0.798 | mortality risk—very high |
| Parameter | Total Group (N) |
|---|---|
| Age (years) | 26.29 ± 5.97 (49) |
| Biochemical parameters | |
| Fetuin (µg/mL) | 226.75 (201.16–289.71) (49) |
| TSH (uIU/mL) | 2.19 ± 1.07 (49) |
| Fasting insulin (pmol/L) | 77.13 (48.07–106.91) (49) |
| Fasting glucose (mmol/L) | 5.04 ± 0.68 (49) |
| Glucose after 120 min (glucose tolerance test) (mmol/L) | 6.47 (5.36–7.77) (40) |
| Glucose after 60 min (glucose tolerance test) (mmol/L) | 8.01 ± 2.42 (39) |
| Insulin after 60 min (glucose tolerance test) (pmol/L) | 703.15 (325.03–835.17) (36) |
| HbA1c (%) | 5.16 ± 0.91 (25) |
| HOMA-IR index | 2.65 (1.40–4.08) (49) |
| Total cholesterol (mmol/L) | 4.94 ± 1.05 (49) |
| HDL cholesterol (mmol/L) | 1.67 ± 0.49 (49) |
| LDL cholesterol (mmol/L) | 2.41 (2.06–3.29) (49) |
| Triglycerides (mmol/L) | 0.93 (0.67–1.63) (49) |
| CRP (mg/L) | 14.29 (3.81–49.52) (47) |
| Atherogenic indices | |
| Castelli’s risk index-I | 2.92 (2.23–3.87) (49) |
| Castelli’s risk index-II | 1.65 (1.06–2.33) (49) |
| Atherogenic Index of plasma | −0.19 ± 0.33 (49) |
| Atherogenic coefficient | 1.92 (1.23–2.87) (49) |
| Parameter | Total Group (N) |
|---|---|
| Body weight (kg) | 77.42 ± 21.03 (49) |
| Height (cm) | 164.91 ± 5.84 (49) |
| Waist circumference (cm) | 91.11 ± 18.87 (49) |
| Hip circumference (cm) | 108.12 ± 13.30 (49) |
| BMI index (kg/m2) | 28.34 ± 7.13 (49) |
| WHR | 0.84 ± 0.10 (49) |
| WHtR | 0.55 ± 0.11 (49) |
| BAI (%) | 33.04 ± 5.69 (49) |
| VAI | 1.22 (0.64–2.29) (49) |
| LAP | 36.16 (9.83–67.80) (49) |
| BRI | 4.63 ± 2.38 (49) |
| ABSI | 0.08 ± 0.01 (49) |
| Body composition | |
| Body fat mass (kg) | 48.37 ± 6.13 (49) |
| Percent of body fat (%) | 37.73 ± 10.26 (49) |
| Lean body mass (kg) | 48.37 ± 6.13 (49) |
| Muscle mass (kg) | 46.11 ± 6.15 (49) |
| Water content (kg) | 34.76 ± 5.38 (49) |
| Water content (%) | 46.45 ± 6.34 (49) |
| Weight status by BMI: | |
| Underweight, n (%) | 1 (2.0) |
| Normal weight, n (%) | 17 (34.7) |
| Overweight, n (%) | 13 (26.5) |
| Obesity, n (%) | 18 (36.7) |
| Weight status by BAI: | |
| Underweight, n (%) | 0 (0.0) |
| Normal weight, n (%) | 24 (49.0) |
| Overweight, n (%) | 18 (36.7) |
| Obesity, n (%) | 7 (14.3) |
| Waist circumference (WC): | |
| Significantly increased risk of metabolic complications, n (%) | 26 (53.1) |
| WHR: | |
| Increasing the risk of metabolic complications, n (%) | 22 (44.9) |
| WHtR: | |
| Abdominal obesity increased risk of cardiovascular diseases and diabetes, n (%) | 30 (61.2) |
| VAI: | |
| Risk of metabolic diseases, n (%) | 17 (34.7) |
| LAP: | |
| Discrimination of prediabetes/diabetes, n (%) | 27 (55.10) |
| BRI: | |
| Discrimination of prediabetes/diabetes, n (%) | 28 (57.14) |
| ABSI: | |
| Risk of diabetes and cardiovascular disease, n (%) | 21 (42.9) |
| ABSI z-score: | |
| Mortality risk—very low, n (%) | 14 (28.6) |
| Mortality risk—low, n (%) | 7 (14.3) |
| Mortality risk—average, n (%) | 12 (24.5) |
| Mortality risk—high, n (%) | 6 (12.2) |
| Mortality risk—very high, n (%) | 10 (20.4) |
| Hypertension, n (%) | 4 (8.2) |
| Dyslipidemia: | |
| Hypercholesterolemia, n (%) | 10 (20.4) |
| Hypertriglyceridemia, n (%) | 2 (4.1) |
| Mixed hyperlipidemia, n (%) | 2 (4.1) |
| Impaired fasting glucose, n (%) | 5 (10.2) |
| Impaired glucose tolerance, n (%) | 9 (18.4) |
| Diabetes mellitus, n (%) | 3 (6.1) |
| Hypothyroidism, n (%) | 23 (46.9) |
| Insulin resistance, n (%) | 29 (59.2) |
| N | R | p-Value | |
|---|---|---|---|
| Body weight (kg) | 49 | −0.10 | 0.48 |
| Waist circumference (cm) | 49 | −0.06 | 0.66 |
| Hip circumference (cm) | 49 | −0.07 | 0.61 |
| BMI index (kg/m2) | 49 | −0.06 | 0.65 |
| WHR | 49 | 0.01 | 0.93 |
| WHtR | 49 | −0.04 | 0.78 |
| Percent of body fat (%) | 49 | −0.20 | 0.17 |
| BAI (%) | 49 | −0.01 | 0.90 |
| VAI | 49 | 0.08 | 0.57 |
| LAP | 49 | 0.08 | 0.58 |
| BRI | 49 | −0.04 | 0.78 |
| ABSI | 49 | 0.03 | 0.83 |
| Castelli’s risk index-I | 49 | 0.04 | 0.75 |
| Castelli’s risk index-II | 49 | 0.03 | 0.82 |
| Atherogenic Index of plasma | 49 | 0.07 | 0.62 |
| Atherogenic coefficient | 49 | 0.04 | 0.75 |
| Fasting insulin (pmol/L) | 49 | −0.08 | 0.56 |
| Fasting glucose (mmol/L) | 49 | −0.11 | 0.42 |
| Glucose after 120 min (mmol/L) (glucose tolerance test) | 40 | 0.04 | 0.80 |
| Glucose after 60 min (mmol/L) (glucose tolerance test) | 39 | 0.08 | 0.62 |
| Insulin after 60 min (pmol/L) (glucose tolerance test) | 36 | −0.06 | 0.70 |
| HbA1c (%) | 25 | −0.13 | 0.52 |
| HOMA-IR index | 49 | 0.09 | 0.50 |
| Total cholesterol (mmol/L) | 49 | 0.30 | 0.03 |
| HDL cholesterol (mmol/L) | 49 | 0.09 | 0.53 |
| LDL cholesterol (mmol/L) | 49 | 0.14 | 0.30 |
| Triglycerides (mmol/L) | 49 | 0.15 | 0.29 |
| Concentration of Fetuin-A [µg/mL] | ||||
|---|---|---|---|---|
| N | Mean ± SD | p-Value | ||
| BMI | Normal weight | 17 | 249.24 ± 55.87 | 0.58 |
| Excess weight (overweight + obesity) | 31 | 246.73 ± 63.28 | ||
| BAI | Normal weight | 24 | 238.03 ± 53.09 | 0.36 |
| Excess weight (overweight + obesity) | 25 | 259.82 ± 66.14 | ||
| WC | ≤88 cm | 23 | 246.47 ± 61.57 | 0.81 |
| >88 cm | 26 | 251.51 ± 60.63 | ||
| WHR | WHR < 0.85 | 27 | 250.36 ± 60.18 | 0.75 |
| WHR ≥ 0.85 | 22 | 247.66 ± 62.24 | ||
| WHtR | WHtR < 0.5 | 19 | 239.52 ± 58.23 | 0.37 |
| WHtR ≥ 0.5 | 30 | 255.24 ± 62.06 | ||
| VAI | VAI ≤ 1.675 | 32 | 244.16 ± 58.60 | 0.51 |
| VAI > 1.675 | 17 | 258.54 ± 64.65 | ||
| LAP | LAP < 41.30 | 27 | 238.99 ± 56.73 | 0.24 |
| LAP ≥ 41.30 | 22 | 261.62 ± 63.89 | ||
| BRI | BRI < 4.910 | 28 | 251.97 ± 60.12 | 0.63 |
| BRI ≥ 4.910 | 21 | 245.39 ± 62.25 | ||
| ABSI | ABSI < 0.076 | 21 | 257.6 ± 68.8 | 0.50 |
| ABSI ≥ 0.076 | 28 | 242.8 ± 53.9 | ||
| ABSI z-score | ABSI <−0.868 | 14 | 251.82 ± 66.34 | 0.89 |
| ABSI −0.868 and −0.272 | 7 | 269.11 ± 77.39 | ||
| ABSI −0.272 and +0.229 | 12 | 236.84 ± 46.87 | ||
| ABSI 0.229 and 0.798 | 6 | 237.30 ± 62.74 | ||
| ABSI > 0.798 | 10 | 253.32 ± 60.46 | ||
| HOMA-IR | Lack of insulin resistance | 20 | 252.48 ± 52.70 | 0.51 |
| Insulin resistance (EGIR—The European Group for the Study of Insulin Resistance) | 29 | 246.85 ± 66.67 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kulik-Kupka, K.; Jabczyk, M.; Nowak, J.; Jagielski, P.; Hudzik, B.; Zubelewicz-Szkodzińska, B. Fetuin-A and Its Association with Anthropometric, Atherogenic, and Biochemical Parameters and Indices among Women with Polycystic Ovary Syndrome. Nutrients 2022, 14, 4034. https://doi.org/10.3390/nu14194034
Kulik-Kupka K, Jabczyk M, Nowak J, Jagielski P, Hudzik B, Zubelewicz-Szkodzińska B. Fetuin-A and Its Association with Anthropometric, Atherogenic, and Biochemical Parameters and Indices among Women with Polycystic Ovary Syndrome. Nutrients. 2022; 14(19):4034. https://doi.org/10.3390/nu14194034
Chicago/Turabian StyleKulik-Kupka, Karolina, Marzena Jabczyk, Justyna Nowak, Paweł Jagielski, Bartosz Hudzik, and Barbara Zubelewicz-Szkodzińska. 2022. "Fetuin-A and Its Association with Anthropometric, Atherogenic, and Biochemical Parameters and Indices among Women with Polycystic Ovary Syndrome" Nutrients 14, no. 19: 4034. https://doi.org/10.3390/nu14194034
APA StyleKulik-Kupka, K., Jabczyk, M., Nowak, J., Jagielski, P., Hudzik, B., & Zubelewicz-Szkodzińska, B. (2022). Fetuin-A and Its Association with Anthropometric, Atherogenic, and Biochemical Parameters and Indices among Women with Polycystic Ovary Syndrome. Nutrients, 14(19), 4034. https://doi.org/10.3390/nu14194034