
Dietary Vitamin D Intake, Pain Incidence, and Pain Changes in Older Adults: The Seniors-ENRICA-1 Cohort

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
Objectives
2. Methods
2.1. Study Design and Participants
2.2. Study Variables
2.2.1. Vitamin D Intake
2.2.2. Pain
2.2.3. Potential Confounders
2.3. Statistical Methods
2.3.1. Study Size
2.3.2. Statistical Methods
2.3.3. Interactions and Sensitivity Analyses
3. Results
3.1. Descriptive Data
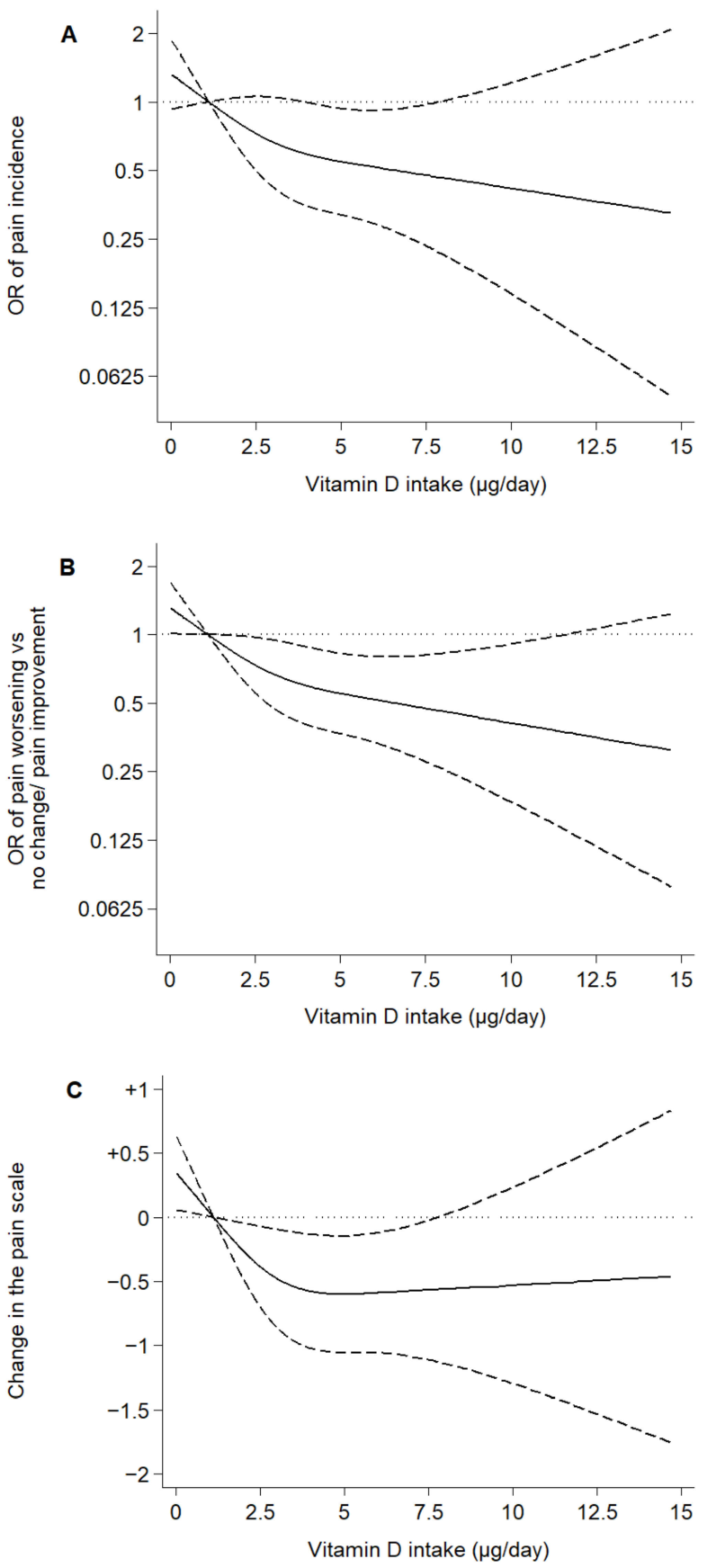
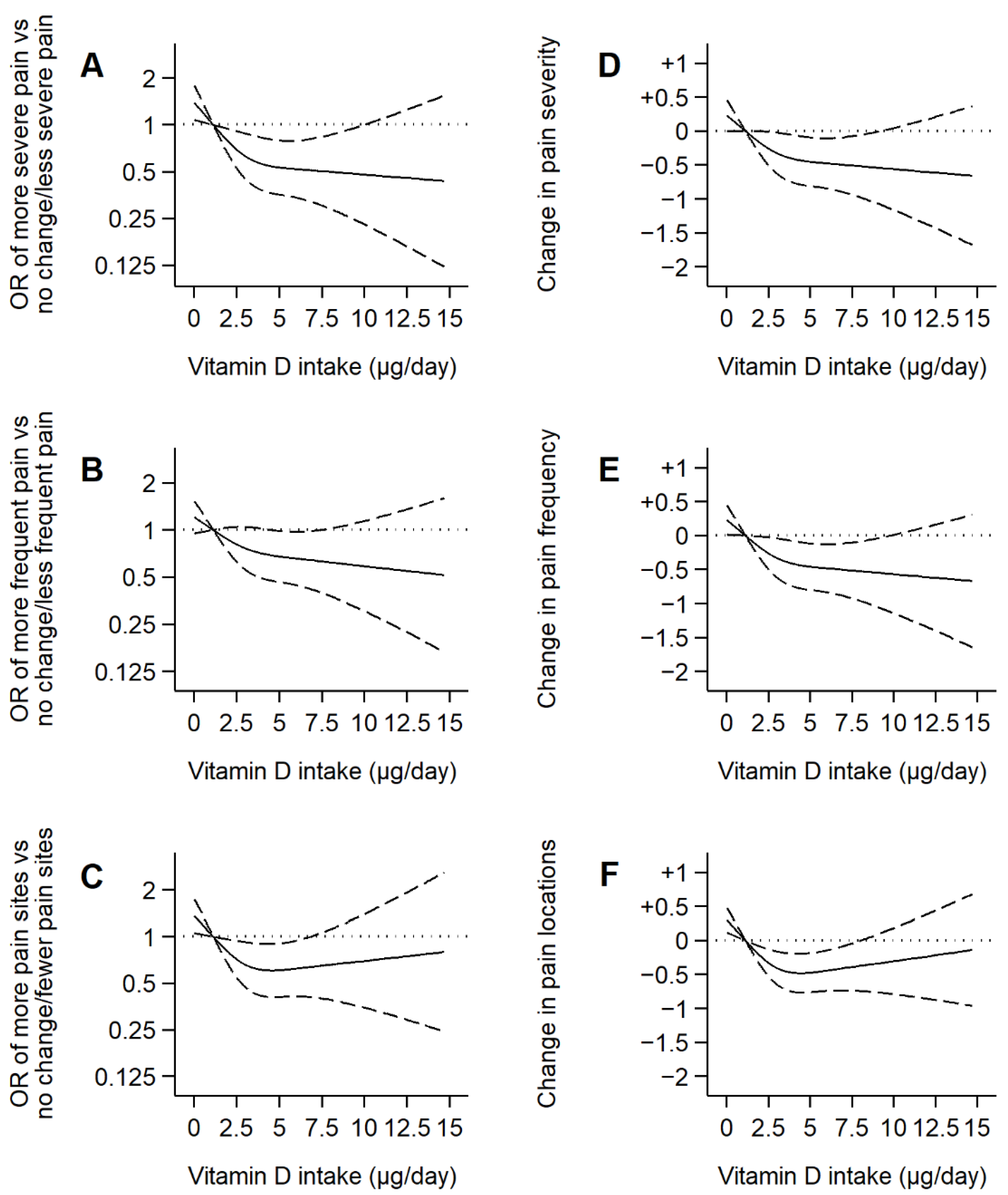
3.2. Main Results
3.3. Interactions and Sensitivity Analyses
4. Discussion
4.1. Interpretation
4.1.1. Relevant Findings from Other Published Studies
4.1.2. Possible Mechanisms and Explanations
4.2. Limitations
4.3. Generalizability
4.4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Marley, J.; Tully, M.A.; Porter-Armstrong, A.; Bunting, B.; O’Hanlon, J.; Atkins, L.; Howes, S.; McDonough, S.M. The effectiveness of interventions aimed at increasing physical activity in adults with persistent musculoskeletal pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2017, 18, 482. [Google Scholar] [CrossRef]
- Borisovskaya, A.; Chmelik, E.; Karnik, A. Exercise and Chronic Pain. Adv. Exp. Med. Biol. 2020, 1228, 233–253. [Google Scholar] [CrossRef]
- Tsang, A.; Von Korff, M.; Lee, S.; Alonso, J.; Karam, E.; Angermeyer, M.C.; Borges, G.L.G.; Bromet, E.J.; de Girolamo, G.; de Graaf, R.; et al. Common Chronic Pain Conditions in Developed and Developing Countries: Gender and Age Differences and Comorbidity With Depression-Anxiety Disorders. J. Pain 2008, 9, 883–891. [Google Scholar] [CrossRef]
- Gaskin, D.J.; Richard, P. The Economic Costs of Pain in the United States. J. Pain 2012, 13, 715–724. [Google Scholar] [CrossRef]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- Fayaz, A.; Croft, P.; Langford, R.M.; Donaldson, L.J.; Jones, G.T. Prevalence of chronic pain in the UK: A systematic review and meta-analysis of population studies. BMJ Open 2016, 6, e010364. [Google Scholar] [CrossRef]
- Miró, J.; Paredes, S.; Rull, M.; Queral, R.; Miralles, R.; Nieto, R.; Huguet, A.; Baos, J. Pain in older adults: A prevalence study in the Mediterranean region of Catalonia. Eur. J. Pain 2007, 11, 83–92. [Google Scholar] [CrossRef]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; Ferreira, P.H.; Fritz, J.M.; Koes, B.W.; Peul, W.; et al. Prevention and treatment of low back pain: Evidence, challenges, and promising directions. Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horgas, A.L. Pain Management in Older Adults. Nurs. Clin. N. Am. 2017, 52, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Field, R.; Pourkazemi, F.; Turton, J.; Rooney, K. Dietary Interventions Are Beneficial for Patients with Chronic Pain: A Systematic Review with Meta-Analysis. Pain Med. 2021, 22, 694–714. [Google Scholar] [CrossRef] [PubMed]
- Totsch, S.K.; Waite, M.E.; Sorge, R.E. Dietary Influence on Pain via the Immune System. Prog. Mol. Biol. Transl. Sci. 2015, 131, 435–469. [Google Scholar] [CrossRef] [PubMed]
- Goltzman, D. Functions of vitamin D in bone. Histochem. Cell Biol. 2018, 149, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Habib, A.M.; Nagi, K.; Thillaiappan, N.B.; Sukumaran, V.; Akhtar, S. Vitamin D and Its Potential Interplay With Pain Signaling Pathways. Front. Immunol. 2020, 11, 820. [Google Scholar] [CrossRef]
- Helde-Frankling, M.; Björkhem-Bergman, L. Vitamin D in Pain Management. Int. J. Mol. Sci. 2017, 18, 2170. [Google Scholar] [CrossRef]
- De Oliveira, D.L.; Hirotsu, C.; Tufik, S.; Andersen, M.L. The interfaces between vitamin D, sleep and pain. J. Endocrinol. 2017, 234, R23–R36. [Google Scholar] [CrossRef]
- Pereda, C.A.; Nishishinya, M.B.; Roldan, E.J. 25-Hydroxyvitamin D serum levels in rheumatic female patients in southeast Spain: The paradigm of daily optimal sunshine levels and inadequate vitamin D status. Endocrinol. Diabetes Y Nutr. 2019, 66, 181–187. [Google Scholar] [CrossRef]
- Wu, Z.; Malihi, Z.; Stewart, A.W.; Lawes, C.M.; Scragg, R. The association between vitamin D concentration and pain: A systematic review and meta-analysis. Vic. Lit. Cult. 2018, 21, 2022–2037. [Google Scholar] [CrossRef]
- Zadro, J.; Shirley, D.; Ferreira, M.; Carvalho-Silva, A.P.; Lamb, S.E.; Cooper, C.; Ferreira, P.H. Mapping the Association between Vitamin D and Low Back Pain: A Systematic Review and Meta-Analysis of Observational Studies. Pain Physician 2017, 20, 611–640. [Google Scholar] [CrossRef]
- van der Wielen, R.P.J.; de Groot, L.C.P.G.M.; van Staveren, W.A.; Löwik, M.R.H.; van den Berg, H.; Haller, J.; Moreiras, O. Serum vitamin D concentrations among elderly people in Europe. Lancet 1995, 346, 207–210. [Google Scholar] [CrossRef]
- Kechichian, E.; Ezzedine, K. Vitamin D and the Skin: An Update for Dermatologists. Am. J. Clin. Dermatol. 2018, 19, 223–235. [Google Scholar] [CrossRef] [PubMed]
- Pattanaungkul, S.; Riggs, B.L.; Yergey, A.L.; Vieira, N.E.; O’Fallon, W.M.; Khosla, S. Relationship of Intestinal Calcium Absorption to 1,25-Dihydroxyvitamin D [1,25(OH) 2 D] Levels in Young Versus Elderly Women: Evidence for Age-Related Intestinal Resistance to 1,25(OH) 2 D Action 1. J. Clin. Endocrinol. Metab. 2000, 85, 4023–4027. [Google Scholar] [CrossRef] [PubMed]
- Bresson, J.L.; Burlingame, B.; Dean, T.; Fairweather-Tait, S.; Heinonen, M.; Hirsch-Ernst, K.I.; Mangelsdorf, I.; McArdle, H.; Naska, A.; Neuhäuser-Berthold, M.; et al. Dietary reference values for vitamin D. EFSA J. 2016, 14, 4547. [Google Scholar]
- Wu, Z.; Stewart, A.; Lawes, C.; Scragg, R.; Malihi, Z. Effect of Vitamin D Supplementation on Pain: A Systematic Review and Meta-analysis. Pain Physician 2016, 19, 415–427. [Google Scholar] [PubMed]
- Zadro, J.R.; Shirley, D.; Ferreira, M.; Silva, A.P.C.; Lamb, S.E.; Cooper, C.; Ferreira, P.H. Is Vitamin D Supplementation Effective for Low Back Pain? A Systematic Review and Meta-Analysis. Pain Physician 2018, 21, 121–145. [Google Scholar] [CrossRef]
- von Mutius, E.; Martinez, F.D. Inconclusive Results of Randomized Trials of Prenatal Vitamin D for Asthma Prevention in Offspring: Curbing the Enthusiasm. JAMA 2016, 315, 347–348. [Google Scholar] [CrossRef]
- Rodríguez-Sánchez, I.; García-Esquinas, E.; Mesas, A.; Martín-Moreno, J.M.; Rodríguez-Mañas, L.; Rodríguez-Artalejo, F. Frequency, intensity and localization of pain as risk factors for frailty in older adults. Age Ageing 2019, 48, 74–80. [Google Scholar] [CrossRef]
- Ortolá, R.; Struijk, E.A.; García-Esquinas, E.; Rodríguez-Artalejo, F.; Lopez-Garcia, E. Changes in Dietary Intake of Animal and Vegetable Protein and Unhealthy Aging. Am. J. Med. 2020, 133, 231–239.e7. [Google Scholar] [CrossRef]
- Rodríguez-Artalejo, F.; Graciani, A.; Guallar-Castillón, P.; León-Muñoz, L.M.; Zuluaga, M.C.; López-García, E.; Gutiérrez-Fisac, J.L.; Taboada, J.M.; Aguilera, M.T.; Regidor, E.; et al. Rationale and Methods of the Study on Nutrition and Cardiovascular Risk in Spain (ENRICA). Rev. Española Cardiol. 2011, 64, 876–882. [Google Scholar] [CrossRef]
- Guallar-Castillón, P.; Sagardui-Villamor, J.; Balboa-Castillo, T.; Sala-Vila, A.; Astolfi, M.J.A.; Pelous, M.D.S.; León-Muñoz, L.M.; Graciani, A.; Laclaustra, M.; Benito, C.; et al. Validity and Reproducibility of a Spanish Dietary History. PLoS ONE 2014, 9, e86074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pols, M.A.; Peeters, P.H.; Ocké, M.C.; Slimani, N.; Bueno-De-Mesquita, H.B.; Collette, H.J. Estimation of reproducibility and relative validity of the questions included in the EPIC Physical Activity Questionnaire. Int. J. Epidemiol. 1997, 26, S181–S189. [Google Scholar] [CrossRef] [PubMed]
- García-Esquinas, E.; Andrade, E.; Martínez-Gómez, D.; Caballero, F.F.; López-García, E.; Rodríguez-Artalejo, F. Television viewing time as a risk factor for frailty and functional limitations in older adults: Results from 2 European prospective cohorts. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 54. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; López-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef]
- Gutiérrez-Fisac, J.L.; Guallar-Castillon, P.; León-Muñoz, L.M.; Graciani, A.; Banegas, J.R.; Rodríguez-Artalejo, F. Prevalence of general and abdominal obesity in the adult population of Spain, 2008–2010: The ENRICA study. Obes. Rev. 2011, 13, 388–392. [Google Scholar] [CrossRef]
- Harrell, F.E. Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer: New York, NY, USA, 2001. [Google Scholar]
- Buchbinder, R.; van Tulder, M.; Öberg, B.; Costa, L.M.; Woolf, A.; Schoene, M.; Croft, P. Lancet Low Back Pain Series Working Group. Low back pain: A call for action. Lancet 2018, 391, 2384–2388. [Google Scholar] [CrossRef]
- Monthly Statistical Bulletin. Climatology. Average Temperatures, Sunshine Hours, and Rainfall, by Autonomous Communities and Meteorological Observatories. 2016. Available online: https://www.ine.es/daco/daco42/bme/c19.pdf (accessed on 11 September 2022).
- Schleicher, R.L.; Sternberg, M.R.; Lacher, D.A.; Sempos, C.T.; Looker, A.C.; Durazo-Arvizu, R.A.; Yetley, E.A.; Chaudhary-Webb, M.; Maw, K.L.; Pfeiffer, C.M.; et al. The vitamin D status of the US population from 1988 to 2010 using standardized serum concentrations of 25-hydroxyvitamin D shows recent modest increases. Am. J. Clin. Nutr. 2016, 104, 454–461. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- Yong, W.C.; Sanguankeo, A.; Upala, S. Effect of vitamin D supplementation in chronic widespread pain: A systematic review and meta-analysis. Clin. Rheumatol. 2017, 36, 2825–2833. [Google Scholar] [CrossRef]
- Riccardi, C.; Perrone, L.; Napolitano, F.; Sampaolo, S.; Melone, M.A.B. Understanding the Biological Activities of Vitamin D in Type 1 Neurofibromatosis: New Insights into Disease Pathogenesis and Therapeutic Design. Cancers 2020, 12, 2965. [Google Scholar] [CrossRef]
- Song, G.G.; Bae, S.-C.; Lee, Y.H. Association between vitamin D intake and the risk of rheumatoid arthritis: A meta-analysis. Clin. Rheumatol. 2012, 31, 1733–1739. [Google Scholar] [CrossRef] [PubMed]
- Harris, H.R.; Chavarro, J.E.; Malspeis, S.; Willett, W.C.; Missmer, S.A. Dairy-Food, Calcium, Magnesium, and Vitamin D Intake and Endometriosis: A Prospective Cohort Study. Am. J. Epidemiol. 2013, 177, 420–430. [Google Scholar] [CrossRef] [PubMed]
- Arnson, Y.; Shoenfeld, Y.; Amital, H. Effects of tobacco smoke on immunity, inflammation and autoimmunity. J. Autoimmun. 2010, 34, J258–J265. [Google Scholar] [CrossRef] [PubMed]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthr. Care Res. 2011, 63, S240–S252. [Google Scholar] [CrossRef]
- Iberian Climate Atlas. Air Temperature and Precipitation (1971–2000); Spanish Meteorological Agency and Portuguese Meteorology Institute: Madrid, Spain, 2011. [Google Scholar] [CrossRef]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144, 138–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Vitamin D Intake (Subjects without Pain) a | Vitamin D Intake (Subjects with and without Pain) a | |||||
|---|---|---|---|---|---|---|
| Tertile 1 (Lowest) | Tertile 2 | Tertile 3 (Highest) | Tertile 1 (Lowest) | Tertile 2 | Tertile 3 (Highest) | |
| n | 156 | 188 | 180 | 278 | 345 | 327 |
| Vitamin D (µg/day) | 1.16 (0.46) | 2.56 (0.48) | 5.60 (2.60) | 1.15 (0.43) | 2.59 (0.48) | 5.69 (2.67) |
| Sex-Men, n (%) | 69 (44.2) | 110 (58.5) | 119 (66.1) * | 108 (38.9) | 164 (47.5) | 188 (57.5) * |
| Age (years) | 71.9 (5.81) | 70.8 (5.37) | 70.1 (5.13) * | 71.3 (5.64) | 70.7 (5.22) | 70.1 (4.98) * |
| Educational level, n (%) | ||||||
| Primary or less | 70 (44.9) | 85 (45.2) | 68 (37.8) | 147 (52.9) | 165 (47.8) | 147 (45.0) |
| Secondary | 47 (30.1) | 44 (23.4) | 58 (32.2) | 71 (25.5) | 89 (25.8) | 97 (29.7) |
| University | 39 (25.0) | 59 (31.4) | 54 (30.0) | 60 (21.6) | 91 (26.4) | 83 (25.4) |
| Tobacco smoking, n (%) | ||||||
| Never | 96 (61.5) | 107 (56.9) | 86 (47.8) | 182 (65.5) | 206 (59.7) | 171 (52.3) * |
| Former | 47 (30.1) | 69 (36.7) | 77 (42.8) | 75 (27.0) | 109 (31.6) | 130 (39.8) |
| Current | 13 (8.33) | 12 (6.38) | 17 (9.44) | 21 (7.55) | 30 (8.70) | 26 (7.95) |
| Alcohol consumption, n (%) | ||||||
| Never | 33 (21.2) | 35 (18.6) | 16 (8.9) * | 61 (21.9) | 71 (20.6) | 43 (13.2) |
| Former | 75 (48.1) | 79 (42.0) | 81 (45.0) | 115 (41.4) | 145 (42.0) | 138 (42.2) |
| Moderate b | 29(18.6) | 53 (28.2) | 55 (30.6) | 60 (21.6) | 81 (23.5) | 91 (27.8) |
| Heavy | 19 (12.2) | 21 (11.2) | 28 (15.6) | 42 (15.1) | 48 (13.9) | 55 (16.8) |
| Physical activity, MET-hours/week | 20.6 (14.4) | 24.2(14.7) | 26.0 (16.2) * | 20.4 (14.3) | 22.3 (14.7) | 24.9 (15.8) * |
| Sedentary behavior, TV hours/day | 2.59 (1.24) | 2.44 (1.40) | 2.48 (1.36) | 2.80 (1.54) | 2.59 (1.36) | 2.66 (1.49) |
| Energy intake, kcal/day | 1907 (400) | 2000 (404) | 2173 (510) * | 1898 (381) | 2018 (432) | 2188 (508) * |
| Body mass index, kg/m2 | 27.9 (4.28) | 27.9 (3.91) | 27.8 (3.85) | 28.2 (4.46) | 28.4 (4.30) | 28.3 (4.28) |
| Number of chronic diseases c | 0.99 (0.49) | 0.98 (0.88) | 0.81 (0.87) | 1.24 (0.99) | 1.17 (0.93) | 1.06 (0.98) |
| Fiber intake, g/day | 23.5 (6.54) | 23.9 (7.14) | 26.4 (8.82) * | 23.9 (7.00) | 24.4 (7.44) | 27.6 (9.80) * |
| Carbohydrate intake, g/day | 202 (43.8) | 203 (44.3) | 216 (57.5) * | 203 (42.8) | 209 (48.4) | 220 (59.8) * |
| Unsaturated fat intake, g/day | 47.7 (14.3) | 50.7 (15.1) | 57.0(17.3) * | 46.6 (14.1) | 50.6 (15.8) | 56.9 (16.8) * |
| Sodium intake, mg/day d | 2437 (810) | 2650 (915) | 2817 (1062) * | 2438 (792) | 2693 (1004) | 2921 (1064) * |
| Vitamin D Intake a | ||||
|---|---|---|---|---|
| Tertile 1 (Lowest) | Tertile 2 | Tertile 3 (Highest) | Per 1-µg/day Increment | |
| Pain incidence | ||||
| Cases/n | 48/156 | 46/188 | 31/180 | 125/524 |
| Model 1: OR (95% CI) b | Ref. | 0.80 (0.49,1.30) | 0.54 (0.32,0.92) * | 0.89 (0.81,0.99) * |
| Model 2: OR (95% CI) c | Ref. | 0.78 (0.47,1.30) | 0.52 (0.29,0.92) * | 0.89 (0.80,1.00) * |
| Model 3: OR (95% CI) d | Ref. | 0.78 (0.47,1.32) | 0.49 (0.28,0.88) * | 0.88 (0.79,0.99) * |
| Changes in the pain scale | ||||
| Pain worsening vs. no change/pain improvement | ||||
| Cases/n | 69/278 | 66/345 | 49/327 | 184/950 |
| Model 1: OR (95% CI) b | Ref. | 0.75 (0.51,1.10) | 0.59 (0.39,0.89) * | 0.89 (0.82,0.97) ** |
| Model 2: OR (95% CI) c | Ref. | 0.74 (0.50,1.09) | 0.57 (0.37,0.88) * | 0.88 (0.81,0.96) ** |
| Model 3: OR (95% CI) d | Ref. | 0.73 (0.49,1.08) | 0.55 (0.36,0.86) ** | 0.88 (0.81,0.96) ** |
| Change in the pain scale | ||||
| n | 278 | 345 | 327 | 950 |
| Model 4: β (95% CI) e | Ref. | −0.56 (−1.00,−0.11) * | −0.57 (−1.03,−0.12) * | −0.07 (−0.15,−0.00) * |
| Model 5: β (95% CI) f | Ref. | −0.54 (−0.99,−0.10) * | −0.53 (−1.00,−0.06) * | −0.07 (−0.14,0.01) |
| Model 6: β (95% CI) g | Ref. | −0.56 (−1.01,−0.12) * | −0.56 (−1.03,−0.09) * | −0.07 (−0.15,0.00) |
| Vitamin D Intake a | ||||
|---|---|---|---|---|
| Tertile 1 (Lowest) | Tertile 2 | Tertile 3 (Highest) | Per 1-µg/day Increment | |
| Pain severity | ||||
| More severe pain vs. no change/less severe pain | ||||
| Cases/n | 74/278 | 67/345 | 53/327 | 194/950 |
| Model 1: OR (95% CI) b | Ref. | 0.68 (0.47,1.00) * | 0.57 (0.38,0.85) ** | 0.92 (0.85,1.00) * |
| Model 2: OR (95% CI) c | Ref. | 0.69 (0.47,1.02) | 0.55 (0.36,0.84) ** | 0.91 (0.84,0.99) * |
| Model 3: OR (95% CI) d | Ref. | 0.68 (0.46,1.00) | 0.53 (0.35,0.81) ** | 0.91 (0.84,0.98) * |
| Change in pain severity | ||||
| n | 278 | 345 | 327 | 950 |
| Model 4: β (95% CI) e | Ref. | −0.39 (−0.74,−0.04) * | −0.47 (−0.83,−0.11) * | −0.07 (−0.12,−0.01) * |
| Model 5: β (95% CI) f | Ref. | −0.36 (−0.72,−0.01) * | −0.41 (−0.78,−0.04) * | −0.06 (−0.12,0.00) |
| Model 6: β (95% CI) g | Ref. | −0.37 (−0.73,−0.02) * | −0.42 (−0.79,−0.05) * | −0.06 (−0.12,−0.00) * |
| Pain frequency | ||||
| More frequent pain vs. no change/less frequent pain | ||||
| Cases/n | 103/278 | 100/345 | 85/327 | 288/950 |
| Model 1: OR (95% CI) b | Ref. | 0.76 (0.53,1.07) | 0.72 (0.50,1.03) | 0.96 (0.90,1.02) |
| Model 2: OR (95% CI) c | Ref. | 0.75 (0.52,1.08) | 0.72 (0.49,1.05) | 0.96 (0.90,1.03) |
| Model 3: OR (95% CI) d | Ref. | 0.75 (0.52,1.08) | 0.69 (0.47,1.03) | 0.95 (0.89,1.02) |
| Change in pain frequency | ||||
| n | 278 | 345 | 327 | 950 |
| Model 4: β (95% CI) e | Ref. | −0.41 (−0.75,−0.08) * | −0.50 (−0.84,−0.15) ** | −0.07 (−0.12,−0.01) * |
| Model 5: β (95% CI) f | Ref. | −0.39 (−0.73,−0.05) * | −0.47 (−0.82,−0.12) ** | −0.06 (−0.12,−0.00) * |
| Model 6: β (95% CI) g | Ref. | −0.40 (−0.73,−0.06) * | −0.45 (−0.81,−0.09) * | −0.06 (−0.12,−0.00) * |
| Pain locations | ||||
| More pain sites vs. no change/fewer pain sites | ||||
| Cases/n | 73/278 | 72/345 | 54/327 | 199/950 |
| Model 1: OR (95% CI) b | Ref. | 0.79 (0.54,1.15) | 0.63 (0.42,0.94) * | 0.94 (0.87,1.01) |
| Model 2: OR (95% CI) c | Ref. | 0.78 (0.53,1.15) | 0.60 (0.40,0.92) * | 0.93 (0.86,1.00) |
| Model 3: OR (95% CI) d | Ref. | 0.78 (0.53,1.14) | 0.60 (0.39,0.92) * | 0.93 (0.86,1.01) |
| Change in the number of pain locations | ||||
| n | 278 | 345 | 327 | 950 |
| Model 4: β (95% CI) e | Ref. | −0.39 (−0.67,−0.11) ** | −0.37 (−0.66,−0.08) * | −0.04 (−0.09,0.00) |
| Model 5: β (95% CI) f | Ref. | −0.39 (−0.68,−0.11) ** | −0.39 (−0.68,−0.09) * | −0.05 (−0.09,0.00) |
| Model 6: β (95% CI) g | Ref. | −0.41 (−0.69,−0.12) ** | −0.41 (−0.71,−0.11) ** | −0.05 (−0.10,−0.00) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carballo-Casla, A.; de Paz-Cantos, S.; Ortolá, R.; García-Esquinas, E.; Sotos-Prieto, M.; Banegas, J.R.; Rodríguez-Artalejo, F. Dietary Vitamin D Intake, Pain Incidence, and Pain Changes in Older Adults: The Seniors-ENRICA-1 Cohort. Nutrients 2022, 14, 3776. https://doi.org/10.3390/nu14183776
Carballo-Casla A, de Paz-Cantos S, Ortolá R, García-Esquinas E, Sotos-Prieto M, Banegas JR, Rodríguez-Artalejo F. Dietary Vitamin D Intake, Pain Incidence, and Pain Changes in Older Adults: The Seniors-ENRICA-1 Cohort. Nutrients. 2022; 14(18):3776. https://doi.org/10.3390/nu14183776
Chicago/Turabian StyleCarballo-Casla, Adrián, Sonia de Paz-Cantos, Rosario Ortolá, Esther García-Esquinas, Mercedes Sotos-Prieto, José R. Banegas, and Fernando Rodríguez-Artalejo. 2022. "Dietary Vitamin D Intake, Pain Incidence, and Pain Changes in Older Adults: The Seniors-ENRICA-1 Cohort" Nutrients 14, no. 18: 3776. https://doi.org/10.3390/nu14183776
APA StyleCarballo-Casla, A., de Paz-Cantos, S., Ortolá, R., García-Esquinas, E., Sotos-Prieto, M., Banegas, J. R., & Rodríguez-Artalejo, F. (2022). Dietary Vitamin D Intake, Pain Incidence, and Pain Changes in Older Adults: The Seniors-ENRICA-1 Cohort. Nutrients, 14(18), 3776. https://doi.org/10.3390/nu14183776