
Prevalence of Malnutrition Assessed by the GLIM Criteria and Association with Activities of Daily Living in Older Residents in an Integrated Facility for Medical and Long-Term Care



Abstract
1. Introduction
2. Materials and Methods
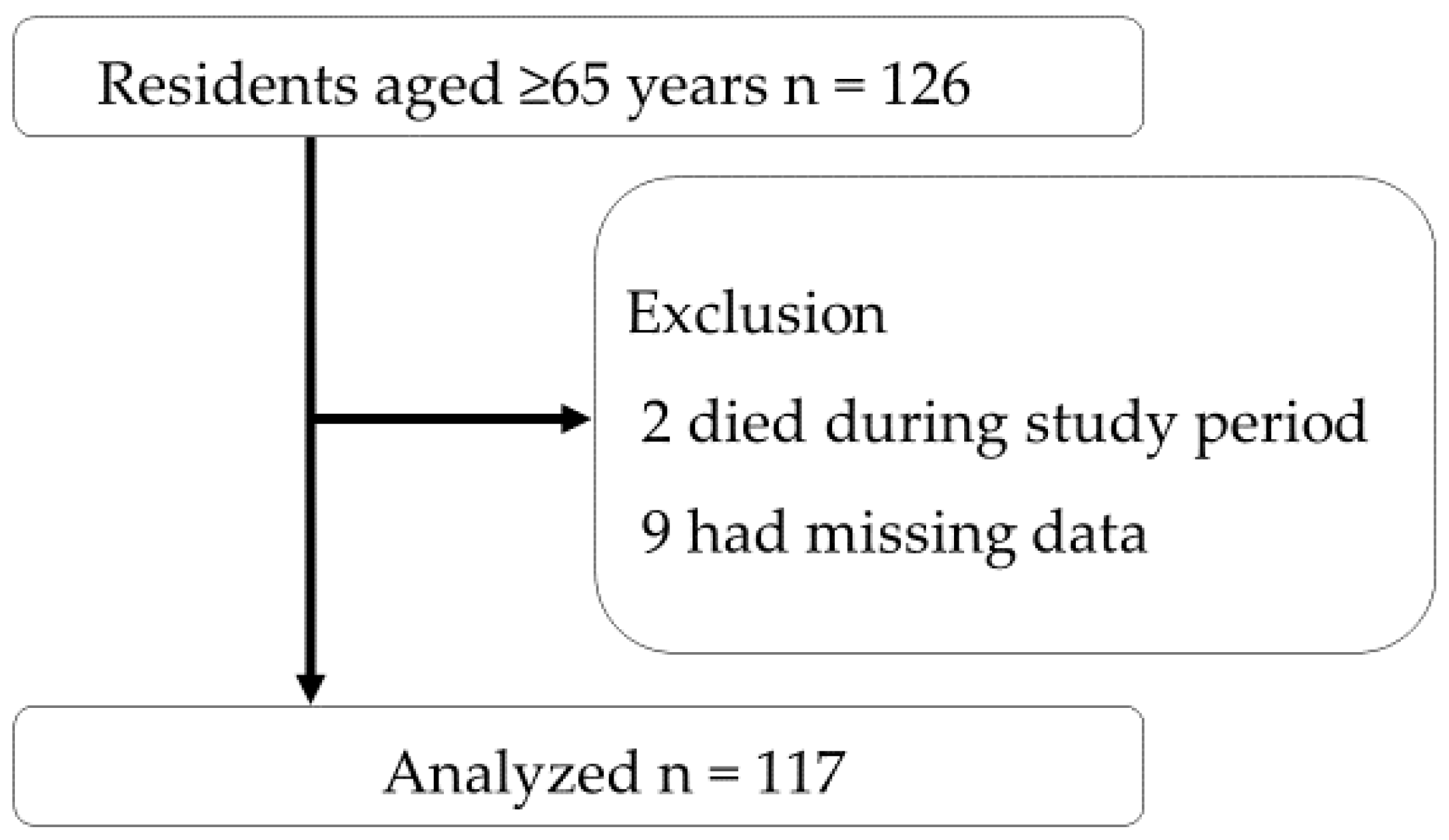
2.1. Study Design and Participants
2.2. IFMLC
2.3. Data Collection
2.4. Malnutrition Assessment
2.5. Outcome Measurement
2.6. Sample Size Calculation
2.7. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Namasivayam, A.M.; Steele, C.M. Malnutrition and dysphagia in long-term care: A systematic review. J. Nutr. Gerontol. Geriatr. 2015, 34, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Bell, C.L.; Lee, A.S.W.; Tamura, B.K. Malnutrition in the nursing home. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. Annual Report on the Ageing Society [Summary] FY2021. Cabinet Office Japan. 2021. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2021/pdf/2021.pdf (accessed on 25 July 2022).
- Ministry of Health, Labor and Welfare. Overview of Integrated Facility for Medical and Long-Term Care. 2018. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000196478.html (accessed on 25 July 2022).
- Social Security Council, Subcommittee on Long-Term Care Benefit Expenses. Integrated Facility for Medical and Long-Term Care. 2020. Available online: https://www.mhlw.go.jp/content/12300000/000672495.pdf (accessed on 25 July 2022).
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Ishida, Y.; Nonogaki, T.; Mori, N. Reference body mass index values and the prevalence of malnutrition according to the Global Leadership Initiative on Malnutrition criteria. Clin. Nutr. 2020, 39, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, A.; Maeda, K.; Wakabayashi, H.; Nishioka, S.; Nagano, A.; Kayashita, J.; Fujishima, I.; Momosaki, R. Predictive validity of body mass index cutoff values used in the global leadership initiative on malnutrition criteria for discriminating severe and moderate malnutrition based on in-patients with pneumonia in Asians. JPEN J. Parenter. Enter. Nutr. 2021, 45, 941–950. [Google Scholar] [CrossRef]
- Sugiyama, M.; Miyamotom, K. Nutrition care management cycle. Surg. Front. 2009, 16, 230–233. [Google Scholar]
- Ministry of Health, Labor and Welfare. Overview of Nutrition Care Management. No 0907002. 2005. Available online: https://www.mhlw.go.jp/topics/kaigo/housyu/dl/c23.pdf (accessed on 25 July 2022).
- Tsutsui, T.; Muramatsu, N. Care-needs certification in the long-term care insurance system of Japan. J. Am. Geriatr. Soc. 2005, 53, 522–527. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kunieda, K.; Ohno, T.; Fujishima, I.; Hojo, K.; Morita, T. Reliability and validity of a tool to measure the severity of dysphagia: The Food Intake LEVEL Scale. J. Pain Symptom Manag. 2013, 46, 201–206. [Google Scholar] [CrossRef]
- Malnutrition Action Group (MAG). The “MUST” Explanatory Booklet. Available online: http://www.bapen.org.uk/pdfs/must/must_explan.pdf (accessed on 25 July 2022).
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, Y.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for sarcopenia: 2019 Consensus Update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. Overview of the Dietary Reference Intakes for Japanese (2020). 2020. Available online: https://www.mhlw.go.jp/content/10900000/000862500.pdf (accessed on 25 July 2022).
- Kawasaki, Y.; Sakai, M.; Nishimura, K.; Fujiwara, K.; Fujisaki, K.; Shimpo, M.; Akamatsu, R. Criterion validity of the visual estimation method for determining patients’ meal intake in a community hospital. Clin. Nutr. 2016, 35, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, H.; Kobayashi, M.; Kajii, Y.; Satonaka, A.; Suzuki, N. Calf circumference positively correlates with calf muscle thickness and negatively correlates with calf subcutaneous fat thickness and percent body fat in non-obese healthy young adults. J. Sports Med. Phys. Fit. 2022, 62, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Tanimoto, Y.; Watanabe, M.; Sun, W.; Hirota, C.; Sugiura, Y.; Kono, R.; Saito, M.; Kono, K. Association between muscle mass and disability in performing Instrumental Activities of Daily Living (IADL) in community-dwelling elderly in Japan. Arch. Gerontol. Geriatr. 2012, 54, e230–e233. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, S.; Matsushita, T.; Yamanouchi, A.; Okazaki, Y.; Oishi, K.; Nishioka, E.; Mori, N.; Tokunaga, Y.; Onizuka, S. Prevalence and associated factors of coexistence of malnutrition and sarcopenia in geriatric rehabilitation. Nutrients 2021, 23, 3745. [Google Scholar] [CrossRef] [PubMed]
- Collin, C.; Wade, D.T.; Davies, S.; Horne, V. The Barthel ADL Index: A reliability study. Int. Disabil. Stud. 1988, 10, 61–63. [Google Scholar] [CrossRef]
- Mikami, Y.; Watanabe, Y.; Edahiro, A.; Motokawa, K.; Shirobe, M.; Yasuda, J.; Murakami, M.; Murakami, K.; Taniguchi, Y.; Furuya, J.; et al. Relationship between mortality and Council of Nutrition Appetite Questionnaire scores in Japanese nursing home residents. Nutrition 2019, 57, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Yeom, H.A.; Fleury, J.; Keller, C. Risk factors for mobility limitation in community-dwelling older adults: A social ecological perspective. Geriatr. Nurs. 2008, 29, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Kelly-Hayes, M.; Beiser, A.; Kase, C.S.; Scaramucci, A.; D’Agostino, R.B.; Wolf, P.A. The influence of gender and age on disability following ischemic stroke: The Framingham study. J. Stroke Cerebrovasc. Dis. 2003, 12, 119–126. [Google Scholar] [CrossRef]
- Taylor, M.E.; Close, J.C.T. Dementia. Handb. Clin. Neurol. 2018, 159, 303–321. [Google Scholar]
- Fuentes-Abolafio, I.J.; Stubbs, B.; Pérez-Belmonte, L.M.; Bernal-López, M.R.; Gómez-Huelgas, R.; Cuesta-Vargas, A.I. Physical functional performance and prognosis in patients with heart failure: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2020, 9, 512. [Google Scholar] [CrossRef] [PubMed]
- Karssemeijer, E.G.A.; Aaronson, J.A.; Bossers, B.J.; Smits, T.; Rikkert, M.G.M.O.; Kessels, R.P.C. Positive effects of combined cognitive and physical exercise training on cognitive function in older adults with mild cognitive impairment or dementia: A meta-analysis. Ageing Res. Rev. 2017, 40, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Sanz-París, A.; Martín-Palmero, A.; Gomez-Candela, C.; García-Almeida, J.M.; Burgos-Pelaez, R.; Sanz-Arque, A.; Espina, S.; Arbones-Mainar, J.M.; Study VIDA group. GLIM Criteria at hospital admission predict 8-year all-cause mortality in elderly patients with type 2 diabetes mellitus: Results from VIDA Study. JPEN J. Parenter. Enter. Nutr. 2020, 44, 1492–1500. [Google Scholar] [CrossRef]
- Bellanti, F.; Buglio, A.L.; Quiete, S.; Pellegrino, G.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Vendemiale, G. Comparison of three nutritional screening tools with the new glim criteria for malnutrition and association with sarcopenia in hospitalized older patients. J. Clin. Med. 2020, 17, 1898. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.B.; Reijnierse, E.M.; Lim, W.K.; Maier, A.B. Prevalence of malnutrition comparing the GLIM criteria, ESPEN definition and MST malnutrition risk in geriatric rehabilitation patients: RESORT. Clin. Nutr. 2020, 39, 3504–3511. [Google Scholar] [CrossRef]
- Shimizu, A.; Maeda, K.; Honda, T.; Ishida, Y.; Ueshima, J.; Nagami, S.; Nagano, A.; Inoue, T.; Murotani, K.; Kayashita, J.; et al. Comparison between the Global Leadership Initiative on Malnutrition and the European Society for Clinical Nutrition and Metabolism definitions for the prevalence of malnutrition in geriatric rehabilitation care. Geriatr. Gerontol. Int. 2020, 20, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- Faxén-Irving, G.; Luiking, Y.; Grönstedt, H.; Franzén, E.; Seiger, Å.; Vikström, S.; Wimo, A.; Boström, A.M.; Cederholm, T. Do malnutrition, sarcopenia and frailty overlap in nursing-home residents? J. Frailty Aging 2021, 10, 17–21. [Google Scholar] [CrossRef]
- Sanz-Paris, A.; Fernández, M.G.; Perez-Noguera, J.; Serrano-Oliver, A.; Torres-Anoro, E.; Sanz-Arque, A.; Arbones-Mainar, J.M. Prevalence of malnutrition and 1-year all-cause mortality in institutionalized elderly patients comparing different combinations of the GLIM criteria. JPEN J. Parenter. Enter. Nutr. 2021, 45, 1164–1171. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Mañas, L.; Rodríguez-Sánchez, B.; Carnicero, J.A.; Rueda, R.; García-Garcia, F.J.; Pereira, S.L.; Sulo, S. Impact of nutritional status according to GLIM criteria on the risk of incident frailty and mortality in community-dwelling older adults. Clin. Nutr. 2021, 40, 1192–1198. [Google Scholar] [CrossRef]
- Sanchez-Rodriguez, D.; Locquet, M.; Bruyère, O.; Lengelé, L.; Cavalier, E.; Reginster, J.Y.; Beaudart, C. Prediction of 5-year mortality risk by malnutrition according to the GLIM format using seven pragmatic approaches to define the criterion of loss of muscle mass. Clin. Nutr. 2021, 40, 2188–2199. [Google Scholar] [CrossRef] [PubMed]
- Sura, L.; Madhavan, A.; Carnaby, G.; Crary, M.A. Dysphagia in the elderly: Management and nutritional considerations. Clin. Interv. Aging 2012, 7, 287–298. [Google Scholar] [PubMed]
- Lan, S.H.; Lu, L.C.; Yen, Y.Y.; Hsieh, Y.P.; Chen, J.C.; Wu, W.J.; Lan, S.J.; Lin, L.Y. Tube feeding among elder in long-term care facilities: A systematic review and meta-analysis. J. Nutr. Health Aging 2017, 21, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Jafry, S.; Jeejeebhoy, K.; Nagpal, A.D.; Pisani, B.; Agarwala, R. Malnutrition and cachexia in heart failure. JPEN J. Parenter. Enter. Nutr. 2016, 40, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Wojzischke, J.; Van Wijngaarden, J.; Van den Berg, C.; Cetinyurek-Yavuz, A.; Diekmann, R.; Luiking, Y.; Bauer, J. Nutritional status and functionality in geriatric rehabilitation patients: A systematic review and meta-analysis. Eur. Geriatr. Med. 2020, 11, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Kootaka, Y.; Kamiya, K.; Hamazaki, N.; Nozaki, K.; Ichikawa, T.; Nakamura, T.; Yamashita, M.; Maekawa, E.; Reed, J.L.; Yamaoka-Tojo, M.; et al. The GLIM criteria for defining malnutrition can predict physical function and prognosis in patients with cardiovascular disease. Clin. Nutr. 2021, 40, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Borda, M.G.; Copete, A.M.A.; Tovar-Rios, D.A.; Jaramillo-Jimenez, A.; Giil, L.M.; Soennesyn, H.; Gómez-Arteaga, C.; Venegas-Sanabria, L.C.; Kristiansen, I.; Chavarro-Carvajal, D.A.; et al. Association of malnutrition with functional and cognitive trajectories in people living with dementia: A five-year follow-up study. J. Alzheimer’s Dis. 2021, 79, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Nozoe, M.; Yamamoto, M.; Masuya, R.; Inoue, T.; Kubo, H.; Shimada, S. Prevalence of malnutrition diagnosed with GLIM criteria and association with activities of daily living in patients with acute stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105989. [Google Scholar] [CrossRef]
- Wang, D.X.M.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 3–25. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.J.; Hwang, S.J.; Liu, C.Y.; Lin, H.R. The relationship between nutritional status and physical function, admission frequency, length of hospital stay, and mortality in old people living in long-term care facilities. J. Nurs. Res. 2012, 20, 110–121. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wakabayashi, H. Rehabilitation nutrition in general and family medicine. J. Gen. Fam. Med. 2017, 18, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, S.; Aragane, H.; Suzuki, N.; Yoshimura, Y.; Fujiwara, D.; Mori, T.; Kanehisa, Y.; Iida, Y.; Higashi, K.; Yoshimura-Yokoi, Y.; et al. Clinical practice guidelines for rehabilitation nutrition in cerebrovascular disease, hip fracture, cancer, and acute illness: 2020 update. Clin. Nutr. ESPEN 2021, 43, 90–103. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | All (117) | Mild and Severe Malnutrition (34) | Nonmild and Nonsevere Malnutrition (83) | p-Value | Severe Malnutrition (21) | Nonsevere Malnutrition (96) | p-Value |
|---|---|---|---|---|---|---|---|
| Age (year), median (IQR) | 88 (84–92) | 89 (86–93) | 87 (81–92) | 0.120 (a) | 88 (86–93) | 88 (82–92) | 0.495 (a) |
| Sex (female), n (%) | 84 (72) | 23 (68) | 61 (74) | 0.651 (b) | 15 (71) | 69 (72) | 1.000 (b) |
| Affiliation before IFMLC admission, n (%) | 0.709 (b) | 0.445 (b) | |||||
| Hospital | 86 (74) | 24 (70) | 62 (74) | 14 (67) | 72 (75) | ||
| Nursing home | 13 (11) | 5 (15) | 8 (10) | 4 (19) | 9 (9) | ||
| Home | 18 (15) | 5 (15) | 13 (16) | 3 (14) | 15 (16) | ||
| Spent at IFMLC, (days), median (IQR) | 483 (207–1175) | 416 (166–1004) | 558 (211–1255) | 0.189 (a) | 611 (230–1146) | 479 (205–1179) | 0.966 (a) |
| Primary diseases for IFMLC admission, n (%) | 0.001 (b) | 0.022 (b) | |||||
| Cerebrovascular disease | 55 (47) | 9 (26) | 46 (56) | 8 (27) | 47 (54) | ||
| Dementia | 32 (27) | 12 (35) | 20 (24) | 11 (37) | 21 (24) | ||
| Orthopedic diseases | 9 (8) | 4 (12) | 5 (6) | 4 (13) | 5 (6) | ||
| Heart failure | 9 (8) | 7 (21) | 2 (2) | 5 (17) | 4 (5) | ||
| Other diseases | 12 (10) | 2 (6) | 10 (12) | 2 (6) | 10 (11) | ||
| Nursing care level, n (%) | 0.483 (b) | 0.467 (b) | |||||
| 1 | 10 (8) | 1 (3) | 9 (11) | 0 (0) | 10 (10) | ||
| 2 | 19 (16) | 5 (15) | 14 (17) | 2 (10) | 17 (18) | ||
| 3 | 18 (15) | 6 (18) | 12 (14) | 4 (19) | 14 (15) | ||
| 4 | 34 (30) | 13 (38) | 21 (25) | 8 (38) | 26 (27) | ||
| 5 | 36 (31) | 9 (26) | 27 (33) | 7 (33) | 29 (30) | ||
| CCI, (points), median (IQR) | 2 (1–3) | 2 (2–3) | 2 (1–3) | 0.130 (a) | 2 (2–3) | 2 (1–3) | 0.411 (a) |
| BMI, (kg/m2), median (IQR) | 19 (17–21) | 17 (16–21) | 19 (17–21) | 0.148 (a) | 17 (16–17) | 19 (17–22) | <0.001 (a) |
| MUST, n (%) | 0.103 (b) | <0.001 (b) | |||||
| Low risk | 22 (19) | 5 (15) | 17 (20) | 0 (0) | 22 (23) | ||
| Medium risk | 22 (19) | 3 (9) | 19 (23) | 0 (0) | 22 (23) | ||
| High risk | 73 (62) | 26 (76) | 47 (57) | 21 (100) | 52 (54) | ||
| Dysphagia severity, n (%) | 0.016 (b) | <0.001 (b) | |||||
| Complete EN 1 | 20 (17) | 5 (14) | 15 (18) | 4 (19) | 16 (17) | ||
| Oral intake with EN 2 | 6 (5) | 5 (15) | 1 (1) | 5 (24) | 1 (1) | ||
| Oral intake without EN 3 | 91 (78) | 24 (71) | 67 (81) | 12 (57) | 79 (82) | ||
| Estimated time of rehabilitation dose (minute/day), median (IQR) | 9 (9–11) | 9 (9–11) | 11 (9–11) | 0.678 (a) | 11 (9–11) | 9 (9–11) | 0.997 (a) |
| Characteristics | Mild and Severe Malnutrition (34) | Nonmild and Nonsevere Malnutrition (83) | p-Value | Severe Malnutrition (21) | Nonsevere Malnutrition (96) | p-Value |
|---|---|---|---|---|---|---|
| Phenotypic criteria, presence, n (%) | ||||||
| Weight loss | 9 (26) | 21 (25) | 1.000 (a) | 3 (14) | 6 (6) | 0.203 (a) |
| Low BMI by GLIM | 24 (71) | 55 (66) | 0.650 (b) | 19 (90) | 31 (32) | <0.001 (a) |
| Reduced muscle mass | 34 (100) | 80 (96) | 0.555 (a) | 8 (38) | 7 (7) | <0.001 (a) |
| Etiologic criteria, presence, n (%) | ||||||
| Reduced food intake or assimilation | 5 (15) | 0 (0) | 0.002 (a) | 3 (14) | 2 (2) | 0.040 (a) |
| Disease burden/inflammation | 32 (94) | 1 (1) | <0.001 (a) | 19 (90) | 14 (15) | <0.001 (a) |
| Barthel Index (points), median (IQR) | 13 (0–51) | 15 (0–55) | 0.672 (c) | 10 (0–38) | 15 (0–55) | 0.159 (c) |
| Characteristics | Barthel Index, Median (IQR) | p-Value |
|---|---|---|
| Sex | ||
| Male | 20 (5–58) | 0.122 (a) |
| Female | 10 (0–50) | |
| Primary diseases for facility admission | ||
| Cerebrovascular disease | 10 (0–25) | 0.06 (b) |
| Dementia | 15 (5–55) | |
| Orthopedic diseases | 50 (13–70) | |
| Heart failure | 55 (10–75) | |
| Other diseases | 10 (0–35) |
| Factor | p-Value | Β | 95% CI | p-Value | Β | 95% CI |
|---|---|---|---|---|---|---|
| Age | 0.301 | 0.339 | −0.307 to 0.986 | 0.403 | 0.270 | −0.367 to 0.907 |
| Sex, female | 0.064 | −5.620 | −11.577 to 0.337 | 0.070 | −5.430 | −11.309 to 0.447 |
| Primary diseases for facility admission | ||||||
| Cerebrovascular disease | Reference | Reference | ||||
| Dementia | 0.555 | −2.998 | −13.045 to 7.049 | 0.797 | −1.306 | −11.363 to 8.751 |
| Orthopedic diseases | 0.060 | 14.592 | −0.949 to 30.133 | 0.044 | 15.935 | 0.472 to 31.399 |
| Heart failure | 0.060 | 15.415 | −0.666 to 31.496 | 0.166 | 10.773 | −4.549 to 26.095 |
| Other diseases | 0.040 | −14.262 | −28.131 to −0.393 | 0.069 | −12.552 | −26.074 to 0.970 |
| Estimated time of rehabilitation dose (minute/day) | 0.338 | 0.952 | −1.008 to 2.912 | 0.314 | 0.988 | −0.948 to 2.923 |
| Mild and severe malnutrition | 0.046 | −6.113 | −12.129 to −0.098 | — | — | — |
| Severe malnutrition | — | — | — | 0.015 | −8.411 | −15.137 to −1.684 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kokura, Y.; Momosaki, R. Prevalence of Malnutrition Assessed by the GLIM Criteria and Association with Activities of Daily Living in Older Residents in an Integrated Facility for Medical and Long-Term Care. Nutrients 2022, 14, 3656. https://doi.org/10.3390/nu14173656
Kokura Y, Momosaki R. Prevalence of Malnutrition Assessed by the GLIM Criteria and Association with Activities of Daily Living in Older Residents in an Integrated Facility for Medical and Long-Term Care. Nutrients. 2022; 14(17):3656. https://doi.org/10.3390/nu14173656
Chicago/Turabian StyleKokura, Yoji, and Ryo Momosaki. 2022. "Prevalence of Malnutrition Assessed by the GLIM Criteria and Association with Activities of Daily Living in Older Residents in an Integrated Facility for Medical and Long-Term Care" Nutrients 14, no. 17: 3656. https://doi.org/10.3390/nu14173656
APA StyleKokura, Y., & Momosaki, R. (2022). Prevalence of Malnutrition Assessed by the GLIM Criteria and Association with Activities of Daily Living in Older Residents in an Integrated Facility for Medical and Long-Term Care. Nutrients, 14(17), 3656. https://doi.org/10.3390/nu14173656