
Processed Food as a Risk Factor for the Development and Perpetuation of Crohn’s Disease—The ENIGMA Study

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.1.1. Inclusion and Exclusion Criteria
2.1.2. Enrolment
2.1.3. Demographic and Clinical Information
2.2. Food Intake Questionnaires
2.2.1. Early Life Processed Food Intake
2.2.2. Recent (Last 12 Months) Food Additive Intake
2.2.3. Current (Last 3-Days) Food Additive and Nutrient Intake
2.2.4. Nutrient Database Harmonization
2.3. Statistical Methods
Data Analyses
3. Results
3.1. Participant Characteristics
3.2. Food Intake
3.2.1. Early Life Intake—Infancy to 18 years
Household Members
First-Degree Relatives
Regional Differences
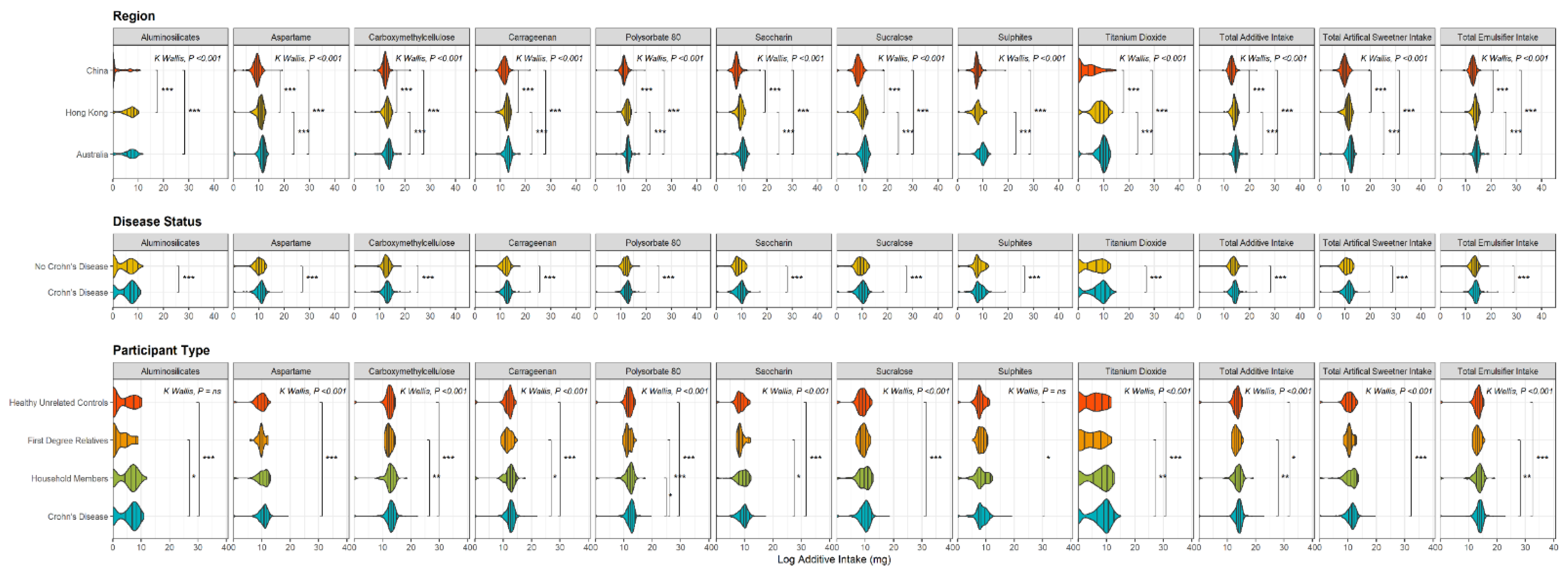
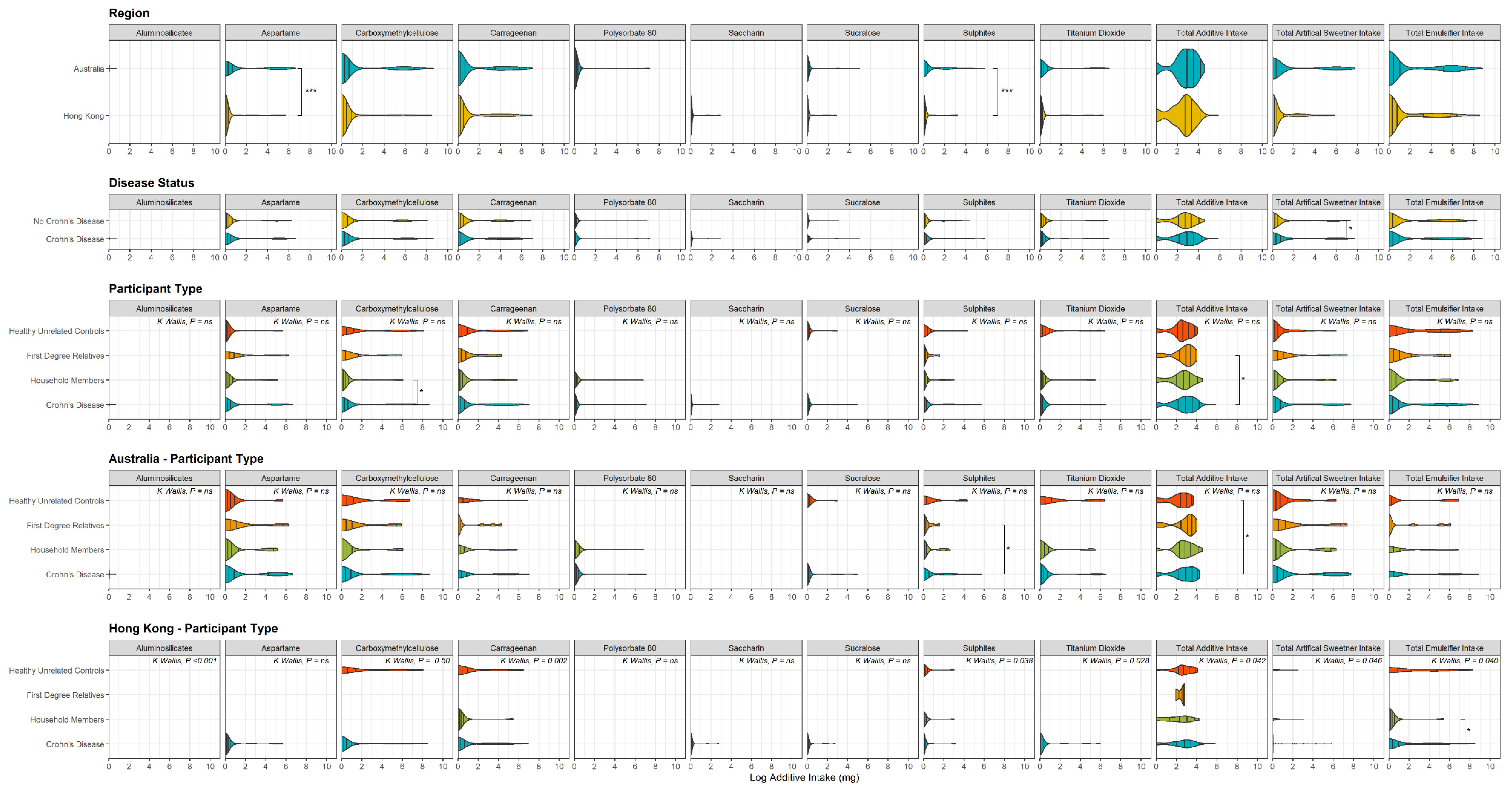
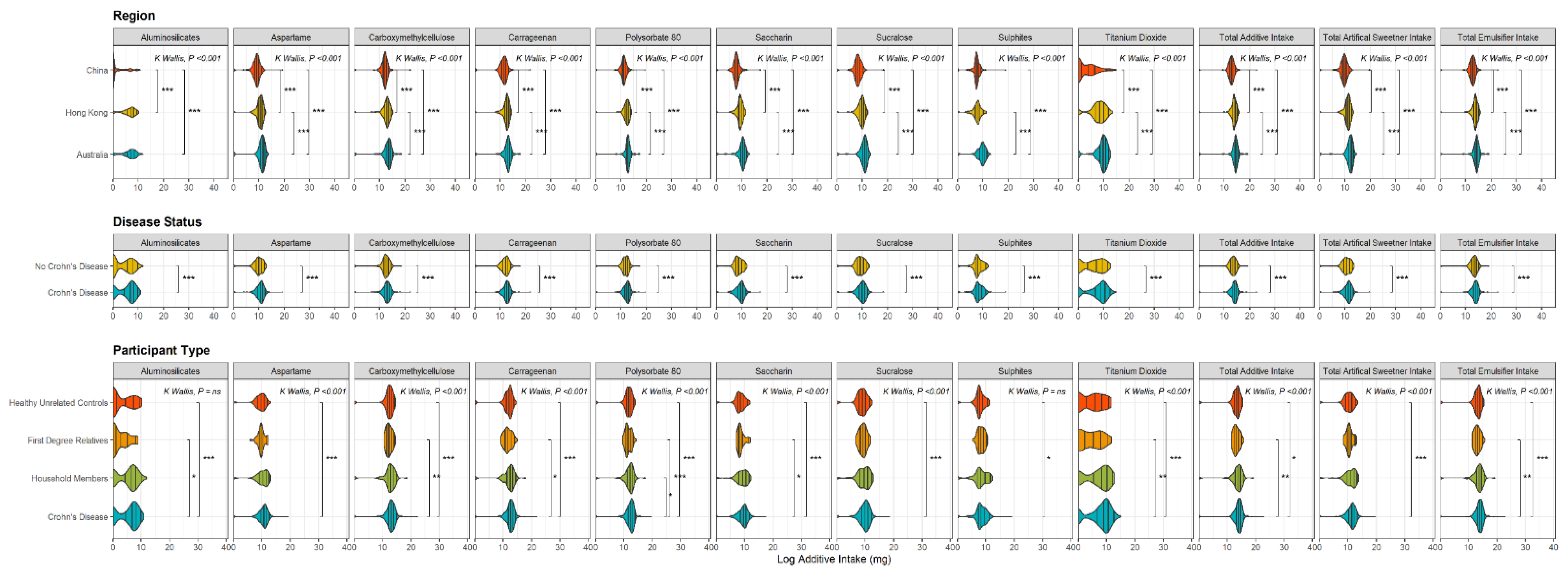
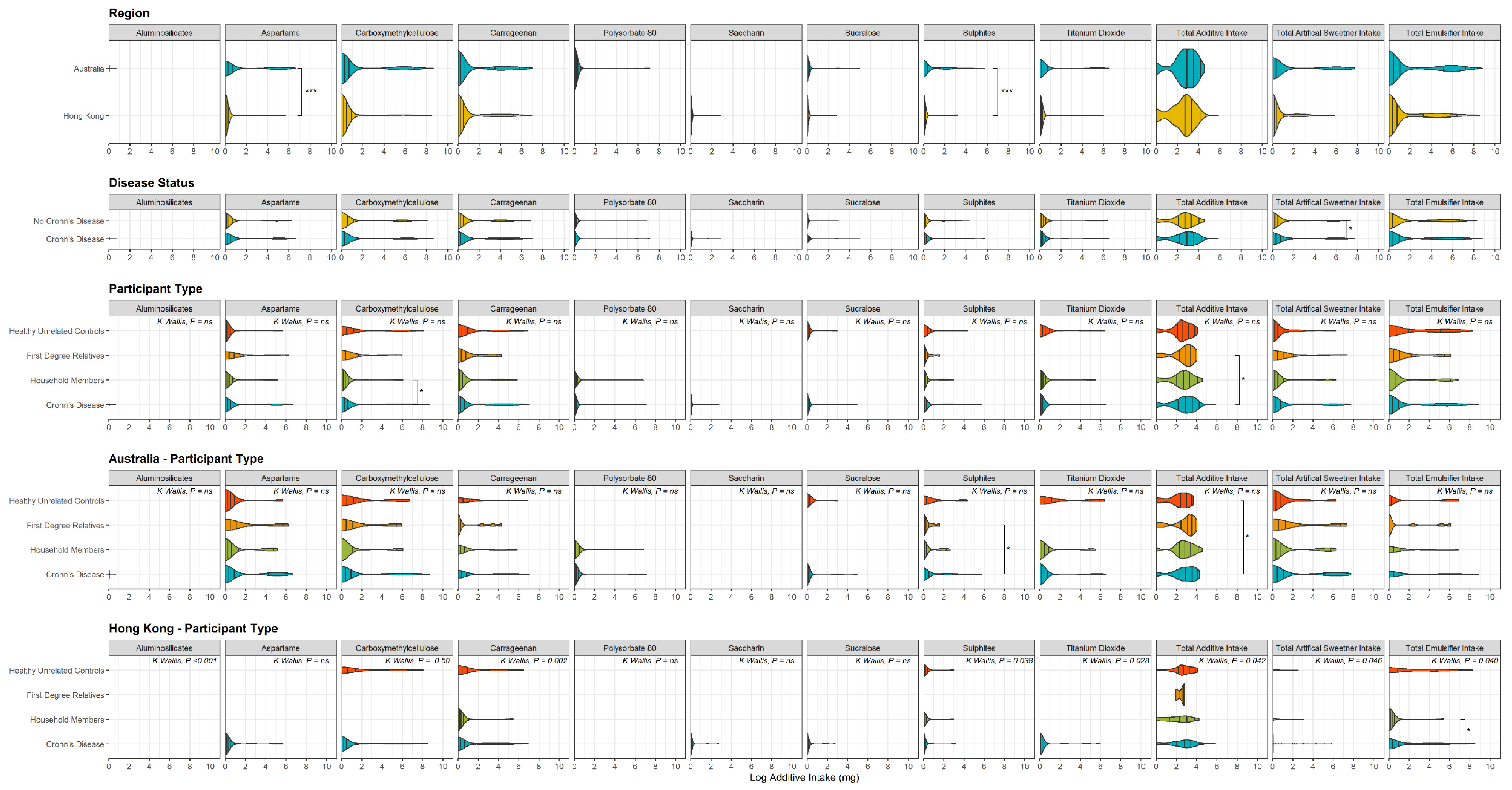
3.2.2. Recent—Past 12 Months Additive Intake
Household Members
First-Degree Relatives
Regional Differences
3.2.3. Current—3 Days Additive Intake
Crohn’s Disease Patients Compared to Controls
Regional Differences
3.3. Dietary Inflammatory Index (DII)
3.3.1. Crohn’s Disease Patients Compared to Controls
3.3.2. Regional Differences
Relationship between DII and Total Additive Intake
3.4. Disease Activity and Dietary Intake
4. Discussion
4.1. Early Life Processed Food Intake
4.2. Recent and Current Food Additive Intake
4.3. Dietary Inflammatory Index
4.4. Study Novelty and Strengths
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, J.Z.; Van Sommeren, S.; Huang, H.; Ng, S.C.; Alberts, R.; Takahashi, A.; Ripke, S.; Lee, J.C.; Jostins, L.; Shah, T.; et al. Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nat. Genet. 2015, 47, 979–986. [Google Scholar] [CrossRef]
- Ko, Y.; Kariyawasam, V.; Karnib, M.; Butcher, R.; Samuel, D.; Alrubaie, A.; Rahme, N.; McDonald, C.; Cowlishaw, J.; Katelaris, P.; et al. Inflammatory Bowel Disease Environmental Risk Factors: A Population-Based Case–Control Study of Middle Eastern Migration to Australia. Clin. Gastroenterol. Hepatol. 2015, 13, 1453–1463.e1. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Bernstein, C.N.; Vatn, M.H.; Lakatos, P.L.; Loftus, E.V., Jr.; Tysk, C.; O’Morain, C.; Moum, B.; Colombel, J.-F.; on behalf of the Epidemiology and Natural History Task Force of the International Organization of Inflammatory Bowel Disease (IOIBD). Geographical variability and environmental risk factors in inflammatory bowel disease. Gut 2013, 62, 630–649. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Tang, W.; Leong, R.W.; Chen, M.; Ko, Y.; Studd, C.; Niewiadomski, O.; Bell, S.; Kamm, M.A.; De Silva, H.J.; et al. Environmental risk factors in inflammatory bowel disease: A population-based case-control study in Asia-Pacific. Gut 2015, 64, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Ahuja, V.; Tandon, R.K. Inflammatory bowel disease in the Asia-Pacific area: A comparison with developed countries and regional differences. J. Dig. Dis. 2010, 11, 134–147. [Google Scholar] [CrossRef]
- Lewis, J.D.; Abreu, M.T. Diet as a Trigger or Therapy for Inflammatory Bowel Diseases. Gastroenterology 2017, 152, 398–414.e6. [Google Scholar] [CrossRef]
- Kaplan, G.G.; Ng, S.C. Understanding and Preventing the Global Increase of Inflammatory Bowel Disease. Gastroenterology 2017, 152, 313–321.e2. [Google Scholar] [CrossRef]
- Levine, A.; Boneh, R.S.; Wine, E. Evolving role of diet in the pathogenesis and treatment of inflammatory bowel diseases. Gut 2018, 67, 1726–1738. [Google Scholar] [CrossRef]
- Li, T.; Qiu, Y.; Yang, H.S.; Li, M.Y.; Zhuang, X.J.; Zhang, S.H.; Feng, R.; Chen, B.L.; He, Y.; Zeng, Z.R.; et al. Systematic review and meta-analysis: Association of a pre-illness Western dietary pattern with the risk of developing inflammatory bowel disease. J. Dig. Dis. 2020, 21, 362–371. [Google Scholar] [CrossRef]
- Khorshidi, M.; Djafarian, K.; Aghayei, E.; Shab-Bidar, S. A posteriori dietary patterns and risk of inflammatory bowel disease: A meta-analysis of observational studies. Int. J. Vitam. Nutr. Res. 2020, 90, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Vasseur, P.; Dugelay, E.; Benamouzig, R.; Savoye, G.; Lan, A.; Srour, B.; Hercberg, S.; Touvier, M.; Hugot, J.-P.; Julia, C.; et al. Dietary Patterns, Ultra-processed Food, and the Risk of Inflammatory Bowel Diseases in the NutriNet-Santé Cohort. Inflamm. Bowel Dis. 2021, 27, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Khalili, H.; Håkansson, N.; Chan, S.S.; Chen, Y.; Lochhead, P.; Ludvigsson, J.; Chan, A.T.; Hart, A.R.; Olén, O.; Wolk, A. Adherence to a Mediterranean diet is associated with a lower risk of later-onset Crohn’s disease: Results from two large prospective cohort studies. Gut 2020, 69, 1637–1644. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.-H.; Lochhead, P.; Khalili, H.; Song, M.; Tabung, F.K.; Burke, K.E.; Richter, J.M.; Giovannucci, E.L.; Chan, A.T.; Ananthakrishnan, A.N. Dietary Inflammatory Potential and Risk of Crohn’s Disease and Ulcerative Colitis. Gastroenterology 2020, 159, 873–883.e1. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- Shivappa, N.; Hebert, J.R.; Rashvand, S.; Rashidkhani, B.; Hekmatdoost, A. Inflammatory potential of diet and risk of ulcerative colitis in a case-control study from Iran. Nutr. Cancer 2016, 68, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Marx, W.; Veronese, N.; Kelly, J.T.; Smith, L.; Hockey, M.; Collins, S.; Trakman, G.L.; Hoare, E.; Teasdale, S.B.; Wade, A.; et al. The Dietary Inflammatory Index and Human Health: An Umbrella Review of Meta-Analyses of Observational Studies. Adv. Nutr. Int. Rev. J. 2021, 12, 1681–1690. [Google Scholar] [CrossRef]
- Yuan, F.; Deng, L.; Sun, X.; Chen, Z.; Shivappa, N.; Sheth, A.K.; Cooper, G.S.; Hebert, J.R.; Li, L. Dietary inflammatory index and risk of colorectal adenoma: Effect measure modification by race, nonsteroidal anti-inflammatory drugs, cigarette smoking and body mass index? Cancer Causes Control 2021, 32, 837–847. [Google Scholar] [CrossRef]
- da Silva, A.; Felício, M.B.; Caldas, A.P.S.; Miranda Hermsdorff, H.H.; Bersch-Ferreira Â, C.; Torreglosa, C.R.; Shivappa, N.; Hébert, J.R.; Weber, B.; Bressan, J. Pro-inflammatory diet is associated with a high number of cardiovascular events and ultra-processed foods consumption in patients in secondary care. Public Health Nutr. 2020, 24, 3331–3340. [Google Scholar] [CrossRef]
- Piovani, D.; Danese, S.; Peyrin-Biroulet, L.; Nikolopoulos, G.K.; Lytras, T.; Bonovas, S. Environmental Risk Factors for Inflammatory Bowel Diseases: An Umbrella Review of Meta-analyses. Gastroenterology 2019, 157, 647–659.e4. [Google Scholar] [CrossRef] [Green Version]
- Spooren, C.E.G.M.; Pierik, M.J.; Zeegers, M.P.; Feskens, E.J.M.; Masclee, A.A.M.; Jonkers, D.M.A.E. Review article: The association of diet with onset and relapse in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2013, 38, 1172–1187. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.K.; Abraham, B.; El-Serag, H. Dietary Intake and Risk of Developing Inflammatory Bowel Disease: A Systematic Review of the Literature. Am. J. Gastroenterol. 2011, 106, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Chassaing, B.; Koren, O.; Goodrich, J.K.; Poole, A.C.; Srinivasan, S.; Ley, R.E.; Gewirtz, A.T. Dietary emulsifiers impact the mouse gut microbiota promoting colitis and metabolic syndrome. Nature 2015, 519, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Chassaing, B.; Van De Wiele, T.; De Bodt, J.; Marzorati, M.; Gewirtz, A.T. Dietary emulsifiers directly alter human microbiota composition and gene expression ex vivo potentiating intestinal inflammation. Gut 2017, 66, 1414–1427. [Google Scholar] [CrossRef]
- Roberts, C.L.; Keita, Å.V.; Duncan, S.H.; O’Kennedy, N.; Söderholm, J.D.; Rhodes, J.M.; Campbell, B.J. Translocation of Crohn’s disease Escherichia coli across M-cells: Contrasting effects of soluble plant fibres and emulsifiers. Gut 2010, 59, 1331–1339. [Google Scholar] [CrossRef]
- Ruiz, P.A.; Morón, B.; Becker, H.M.; Lang, S.; Atrott, K.; Spalinger, M.R.; Scharl, M.; Wojtal, K.A.; Fischbeck-Terhalle, A.; Frey-Wagner, I.; et al. Titanium dioxide nanoparticles exacerbate DSS-induced colitis: Role of the NLRP3 inflammasome. Gut 2017, 66, 1216–1224. [Google Scholar] [CrossRef]
- Lomer, M.C.E.; Thompson, R.P.H.; Powell, J.J. Fine and ultrafine particles of the diet: Influence on the mucosal immune response and association with Crohn’s disease. Proc. Nutr. Soc. 2002, 61, 123–130. [Google Scholar] [CrossRef]
- Zhang, J.; Hoedt, E.C.; Liu, Q.; Berendsen, E.; Teh, J.J.; Hamilton, A.; Brien, A.W.O.; Ching, J.Y.; Wei, H.; Yang, K.; et al. Elucidation of Proteus mirabilis as a Key Bacterium in Crohn’s Disease Inflammation. Gastroenterology 2021, 160, 317–330.e11. [Google Scholar] [CrossRef]
- Pitcher, M.C.; Cummings, J.H. Hydrogen sulphide: A bacterial toxin in ulcerative colitis? Gut 1996, 39, 1–4. [Google Scholar] [CrossRef]
- Ronan, V.; Yeasin, R.; Claud, E.C. Childhood Development and the Microbiome—The Intestinal Microbiota in Maintenance of Health and Development of Disease During Childhood Development. Gastroenterology 2021, 160, 495–506. [Google Scholar] [CrossRef]
- Zhao, J.; Ng, S.C.; Lei, Y.; Yi, F.; Li, J.; Yu, L.; Zou, K.; Dan, Z.; Dai, M.; Ding, Y. First Prospective, Population-Based Inflammatory Bowel Disease Incidence Study in Mainland of China: The Emergence of “Western” Disease. Inflamm Bowel Dis. 2013, 19, 1839–1845. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Leung, W.K.; Shi, H.Y.; Li, M.K.K.; Leung, C.M.; Ng, C.K.M.; Lo, F.H.; Hui, Y.T.; Tsang, S.W.C.; Chan, Y.K.; et al. Epidemiology of Inflammatory Bowel Disease from 1981 to 2014: Results from a Territory-Wide Population-Based Registry in Hong Kong. Inflamm. Bowel Dis. 2016, 22, 1954–1960. [Google Scholar] [CrossRef] [PubMed]
- Trakman, G.L.; Lin, W.; Wilson-O’Brien, A.L.; Stanley, A.; Hamilton, A.L.; Tang, W.; Or, L.; Ching, J.; Morrison, M.; Yu, J.; et al. Development and Validation of Surveys to Estimate Food Additive Intake. Nutrients 2020, 12, 812. [Google Scholar] [CrossRef] [PubMed]
- Marion-Letellier, R.; Amamou, A.; Savoye, G.; Ghosh, S. Inflammatory bowel diseases and food additives: To add fuel on the flames! Nutrients 2019, 11, 1111. [Google Scholar] [CrossRef] [PubMed]
- Hviid, A.; Svanström, H.; Frisch, M. Antibiotic use and inflammatory bowel diseases in childhood. Gut 2011, 60, 49–54. [Google Scholar] [CrossRef]
- Narula, N.; Wong, E.C.L.; Dehghan, M.; Mente, A.; Rangarajan, S.; Lanas, F.; Lopez-Jaramillo, P.; Rohatgi, P.; Lakshmi, P.V.M.; Varma, R.P.; et al. Association of ultra-processed food intake with risk of inflammatory bowel disease: Prospective cohort study. BMJ 2021, 374, n1554. [Google Scholar] [CrossRef]
- Cint Insight Exchange. “Australia: How Often Do You Eat Fast Food (Any Quick Service Restaurant) in Any Given Week (on Average)?”. Statista, Australia. 2018. Available online: https://www.statista.com/statistics/921343/australia-average-fast-food-consumption-per-week/ (accessed on 25 July 2022).
- Prideaux, L.; Kang, S.; Wagner, J.; Buckley, M.; Mahar, J.E.; De Cruz, P.; Wen, Z.; Chen, L.; Xia, B.; van Langenberg, D.R.; et al. Impact of Ethnicity, Geography, and Disease on the Microbiota in Health and Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2013, 19, 2906–2918. [Google Scholar] [CrossRef]
- Niewiadomski, O.; Studd, C.; Wilson, J.; Williams, J.; Hair, C.; Knight, R.; Prewett, E.; Dabkowski, P.; Alexander, S.; Allen, B.; et al. Influence of food and lifestyle on the risk of developing inflammatory bowel disease. Intern. Med. J. 2016, 46, 669–676. [Google Scholar] [CrossRef]
- Persson, P.G.; Ahlbom, A.; Hellers, G. Diet and Inflammatory Bowel Disease: A Case-Control Study. Epidemiology 1992, 3, 47–52. [Google Scholar] [CrossRef]
- Jimenez Loayza, J.J.; Berendsen, E.M.; Teh, J.J.; Hoedt, E.C.; Zhang, J.; Liu, Q.; Hamilton, A.L.; Wilson-O’Brien, A.; Trakman, G.L.; Lin, W.; et al. P837 The common food additives sodium sulfite and polysorbate 80 have a profound inhibitory effect on the commensal, anti-inflammatory bacterium Faecalibacterium prausnitzii: The ENIGMA study. J. Crohn’s Colitis 2019, 13, S542–S543. [Google Scholar] [CrossRef]
- Wang, Z.; Shao, Y. Effects of microbial diversity on nitrite concentration in pao cai, a naturally fermented cabbage product from China. Food Microbiol. 2018, 72, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Lu, M.; Liu, R.; Tian, Y.; Vu, V.H.; Li, Y.; Liu, B.; Kushmaro, A.; Li, Y.; Sun, Q. Inhibition of Streptococcus mutans Biofilm Formation and Virulence by Lactobacillus plantarum K41 Isolated From Traditional Sichuan Pickles. Front. Microbiol. 2020, 11, 774. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Chen, B.; Liu, B.; Zhou, X.; Mu, J.; Wang, Q.; Zhao, X.; Yang, Z. Preventive Effect of Lactobacillus fermentum CQPC03 on Activated Carbon-Induced Constipation in ICR Mice. Medicina 2018, 54, 89. [Google Scholar] [CrossRef] [PubMed]
- Dimidi, E.; Cox, S.R.; Rossi, M.; Whelan, K. Fermented Foods: Definitions and Characteristics, Impact on the Gut Microbiota and Effects on Gastrointestinal Health and Disease. Nutrients 2019, 11, 1806. [Google Scholar] [CrossRef]
- Campbell, E.; Nagler, C.R. Fe, fi, fo, fum, I smell the diet of a healthy human. Cell 2021, 184, 4107–4109. [Google Scholar] [CrossRef]
- Wastyk, H.C.; Fragiadakis, G.K.; Perelman, D.; Dahan, D.; Merrill, B.D.; Yu, F.B.; Topf, M.; Gonzalez, C.G.; Van Treuren, W.; Han, S.; et al. Gut-microbiota-targeted diets modulate human immune status. Cell 2021, 184, 4137–4153.e14. [Google Scholar] [CrossRef]
- I Benchimol, E.; Mack, D.R.; Guttmann, A.; Nguyen, G.C.; To, T.; Mojaverian, N.; Quach, P.; Manuel, D.G. Inflammatory Bowel Disease in Immigrants to Canada And Their Children: A Population-Based Cohort Study. Am. J. Gastroenterol. 2015, 110, 553–563. [Google Scholar] [CrossRef]
- Agrawal, M.; Corn, G.; Shrestha, S.; Nielsen, N.M.; Frisch, M.; Colombel, J.-F.; Jess, T. Inflammatory bowel diseases among first-generation and second-generation immigrants in Denmark: A population-based cohort study. Gut 2020, 70, 1037–1043. [Google Scholar] [CrossRef]
- Lo, C.-H.; Khandpur, N.; Rossato, S.L.; Lochhead, P.; Lopes, E.W.; Burke, K.E.; Richter, J.M.; Song, M.; Korat, A.V.A.; Sun, Q.; et al. Ultra-processed Foods and Risk of Crohn’s Disease and Ulcerative Colitis: A Prospective Cohort Study. Clin. Gastroenterol. Hepatol. 2021, in press. [Google Scholar] [CrossRef]
- Swidsinski, A.; Ung, V.; Sydora, B.C.; Loening-Baucke, V.; Doerffel, Y.; Verstraelen, H.; Fedorak, R.N. Bacterial Overgrowth and Inflammation of Small Intestine After Carboxymethylcellulose Ingestion in Genetically Susceptible Mice. Inflamm. Bowel Dis. 2009, 15, 359–364. [Google Scholar] [CrossRef]
- Devkota, S.; Chang, E.B. Interactions between diet, bile acid metabolism, gut microbiota, and inflammatory bowel diseases. Dig. Dis. 2015, 33, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Ijssennagger, N.; van der Meer, R.; van Mil, S.W. Sulfide as a mucus barrier-breaker in inflammatory bowel disease? Trends Mol. Med. 2016, 22, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Cox, S.; Sandall, A.; Smith, L.; Rossi, M.; Whelan, K. Food additive emulsifiers: A review of their role in foods, legislation and classifications, presence in food supply, dietary exposure, and safety assessment. Nutr. Rev. 2020, 79, 726–741. [Google Scholar] [CrossRef] [PubMed]
- Chazelas, E.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Agaesse, C.; De Sa, A.; Lutchia, R.; Rebouillat, P.; Srour, B.; Debras, C.; et al. Exposure to food additive mixtures in 106,000 French adults from the NutriNet-Santé cohort. Sci. Rep. 2021, 11, 19680. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Kolanos, R.; DiNovi, M.J.; Mattia, A.; Kaneko, K.J. Dietary exposures for the safety assessment of seven emulsifiers commonly added to foods in the United States and implications for safety. Food Addit. Contam. Part A 2017, 34, 905–917. [Google Scholar] [CrossRef] [PubMed]
- Vin, K.; Connolly, A.; McCaffrey, T.; McKevitt, A.; O’Mahony, C.; Prieto, M.A.; Tennant, D.; Hearty, A.; Volatier, J.L. Estimation of the dietary intake of 13 priority additives in France, Italy, the UK and Ireland as part of the FACET project. Food Addit. Contam. Part A 2013, 30, 2050–2080. [Google Scholar] [CrossRef]
- Penttila, P.L.; Salminen, S.; Niemi, E. Estimates on the intake of food additives in Finland. Z Lebensm Unters Forsch. 1988, 186, 11–15. [Google Scholar] [CrossRef]
- Shah, Z.C.; Huffman, F.G. Current Availability and Consumption of Carrageenan-Containing Foods. Ecol. Food Nutr. 2003, 42, 357–371. [Google Scholar] [CrossRef]
- Cressey, P.; Jones, S. Levels of preservatives (sulfite, sorbate and benzoate) in New Zealand foods and estimated dietary exposure. Food Addit. Contam. Part A 2009, 26, 604–613. [Google Scholar] [CrossRef]
- Rompelberg, C.; Heringa, M.B.; Van Donkersgoed, G.; Drijvers, J.; Roos, A.; Westenbrink, S.; Peters, R.; Van Bemmel, G.; Brand, W.; Oomen, A.G. Oral intake of added titanium dioxide and its nanofraction from food products, food supplements and toothpaste by the Dutch population. Nanotoxicology 2016, 10, 1404–1414. [Google Scholar] [CrossRef] [Green Version]
- Huvaere, K.; Vandevijvere, S.; Hasni, M.; Vinkx, C.; Van Loco, J. Dietary intake of artificial sweeteners by the Belgian population. Food Addit. Contam. Part A 2012, 29, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Ishiwata, H.; Yamada, T.; Yoshiike, N.; Nishijima, M.; Kawamoto, A.; Uyama, Y. Daily intake of food additives in Japan in five age groups estimated by the market basket method. Eur. Food Res. Technol. 2002, 215, 367–374. [Google Scholar] [CrossRef]
- Buffini, M.; Goscinny, S.; Van Loco, J.; Nugent, A.P.; Walton, J.; Flynn, A.; Gibney, M.J.; McNulty, B.A. Dietary intakes of six intense sweeteners by Irish adults. Food Addit Contam. Part A Chem. Anal. Control. Exp. Risk Assess 2018, 35, 425–438. [Google Scholar] [CrossRef] [PubMed]
- Suh, H.-J.; Choi, S. Use of Sodium Saccharin and Sucralose in Foodstuffs and the Estimated Daily Intakes of Both Products in Korea. Korean J. Food Sci. Technol. 2013, 45, 642–651. [Google Scholar] [CrossRef]
- Tian, Z.; Zhuang, X.; Zhao, M.; Zhuo, S.; Li, X.; Ma, R.; Li, N.; Liu, C.; Zhu, Y.; Tang, C.; et al. Index-Based Dietary Patterns and Inflammatory Bowel Disease: A Systematic Review of Observational Studies. Adv. Nutr. Int. Rev. J. 2021, 12, 2288–2300. [Google Scholar] [CrossRef]
- Principi, M.; Losurdo, G.; Iannone, A.; Contaldo, A.; Deflorio, V.; Ranaldo, N.; Pisani, A.; Ierardi, E.; Di Leo, A.; Barone, M. Differences in dietary habits between patients with inflammatory bowel disease in clinical remission and a healthy population. Ann Gastroenterol 2018, 31, 469–473. [Google Scholar] [CrossRef]
- Opstelten, J.L.; de Vries, J.H.; Wools, A.; Siersema, P.D.; Oldenburg, B.; Witteman, B.J. Dietary intake of patients with inflammatory bowel disease: A comparison with individuals from a general population and associations with relapse. Clin. Nutr. 2018, 38, 1892–1898. [Google Scholar] [CrossRef]
- Naqvi, S.A.; Taylor, L.M.; Panaccione, R.; Ghosh, S.; Barkema, H.W.; Hotte, N.; Shommu, N.; Kaur, S.; Reimer, R.A.; Madsen, K.L.; et al. Dietary patterns, food groups and nutrients in Crohn’s disease: Associations with gut and systemic inflammation. Sci. Rep. 2021, 11, 1674. [Google Scholar] [CrossRef]
- Mirmiran, P.; Moslehi, N.; Morshedzadeh, N.; Shivappa, N.; Hébert, J.R.; Farsi, F.; Daryani, N.E. Does the inflammatory potential of diet affect disease activity in patients with inflammatory bowel disease? Nutr. J. 2019, 18, 65. [Google Scholar] [CrossRef]
- Lamers, C.R.; De Roos, N.M.; Witteman, B.J.M. The association between inflammatory potential of diet and disease activity: Results from a cross-sectional study in patients with inflammatory bowel disease. BMC Gastroenterol. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Rothman, K.J. No adjustments are needed for multiple comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C. Improving long-term recall in epidemiologic studies. Epidemiology 1994, 5, 1–4. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Chen, L.; Catalan-Dibene, J.; Bongers, G.; Faith, J.J.; Suebsuwong, C.; DeVita, R.J.; Shen, Z.; Fox, J.G.; Lafaille, J.J.; et al. Food colorants metabolized by commensal bacteria promote colitis in mice with dysregulated expression of interleukin-23. Cell Metab. 2021, 33, 1358–1371.e5. [Google Scholar] [CrossRef] [PubMed]
- Naimi, S.; Viennois, E.; Gewirtz, A.T.; Chassaing, B. Direct impact of commonly used dietary emulsifiers on human gut microbiota. Microbiome 2021, 9, 66. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| All Regions Combined (n = 531) | Australia (n = 180) | Hong Kong (n = 160) | Mainland China (n = 191) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All Subjects Combined | CD (274) | HHM (83) | FDR (82) | HC (92) | CD (100) | HHM (32) | FDR (28) | HC (20) | CD (95) | HHM (22) | FDR (21) | HC (22) | CD (79) | HHM (29) | FDR (33) | HC (50) | |
| Gender Male | 297 (53) | 160 (59) | 55 (47) | 39 (48) | 43 (47) | 49 (49) | 25 (50) | 9 (32) | 8 (40) | 64 (68) | 15 (39) | 7 (33) | 9 (41) | 47 (60) | 15 (52) | 23 (70) | 26 (52) |
| n (%) | |||||||||||||||||
| Age | 43 | 36 | 47.5 | 49 | 47 | 38.1 | 46.8 | 50.2 | 51.1 | 39.7 | 50.9 | 55.4 | 47.9 | 36 | 38 | 43 | 42 |
| (median, year) | |||||||||||||||||
| BMI | 23.1 | 22.5 | 23.8 | 24.2 | 22.6 | 25.1 | 27.6 | 25.9 | 27.4 | 22.7 | 23.9 | 25.5 | 23.7 | 19.6 | 22.3 | 21.5 | 22 |
| (median, kg/m2) | |||||||||||||||||
| All | Australia | Hong Kong | China | p-Value | |
|---|---|---|---|---|---|
| Age at Diagnosis | 25.0 | 22.0 | 27.5 | 37.9 | |
| (median, years [IQR, Range]) | (18, 7–69) | (13, 7–65) | (22, 8–69) | (24, 19–68) | 0.029 |
| Time since Diagnosis | 8.0 | 9.0 | 6.0 | 3.0 | |
| (median, years ([IQR, Range]) | (13, 0–41) | (12, 0–41) | (12, 0–30) | (4, 1–23) | 0.048 |
| CDAI | |||||
| median (IQR) | 63.9 (78.4) | 48.6 (73.4) | 74.3 (75.2) | <0.001 | |
| Remission (%) | 85.3 | 85.7 | 84.9 | 0.910 | |
| Mildly active (%) | 12.0 | 11.2 | 12.8 | ||
| Moderately active (%) | 2.7 | 3.1 | 2.3 | ||
| CRP | |||||
| median (IQR) | 0.9 (5.1) | 0.0 (4.0) | 2.6 (6.2) | 4.1 (6.1) | <0.001 |
| Normal (%) | 70.4 | 74.2 | 66.7 | 69.7 | 0.261 |
| Above normal (%) | 29.6 | 25.8 | 33.3 | 30.3 | |
| Hemoglobin | |||||
| (median, IQR)) | 138.0 (18.0) | 135.5 (20.55) | 136.0 (20.0) | 142.4 (2.65) | 0.066 |
| Normal (%) | 77.1 | 80.6 | 73.7 | 72.0 | 0.256 |
| Below normal (%) | 22.9 | 19.4 | 26.3 | 28.0 |
| Dietary Inflammatory Index (DII) |
|
| Food Additives | |
| Total Additive Intake | Recent (12 months)
|
| Total Artificial Sweetener Intake | Recent (12 months)
|
| Total Emulsifier Intake | Recent (12 months)
|
| Energy (calories) | Current (last 3 days)
|
| Individual Additives | |
| Polysorbate-80 | Recent (12-month)
|
| Carboxymethylcellulose | Recent (12-month)
|
| Carrageenan | Recent (12-month)
|
| Aluminosilicates | Recent (12-month)
|
| Sulphites | Recent (12 months)
|
| Titanium Dioxide | Recent (12-month)
|
| Aspartame | Recent (12-month)
|
| Sucralose | Recent (12-month)
|
| Saccharin | Recent (12-month)
|
| Additive | Usual Intake | Recent Intake (Mean or Median) | Acceptable Daily Intake (ADI) mg/kg Body Weight/Day | Population | Estimated Population Intakes (Tier Estimate) |
|---|---|---|---|---|---|
| Polysorbate-80 | 11.3 | 0.00 (mean) 0.09 (median) | 0–25 | USA, 2 years and older | 5–10 (T2) [56] |
| USA, 2 years and older | 5 (T1) [56] | ||||
| Europe (UK, Ireland, France, Italy), 8 years to 97 years | 1.850–2.218 (T2) [57] 0.610–1.177 (T3) [57] includes all polysorbates | ||||
| Carboxymethylcellulose | 19.5 | 0.18 (mean) | Not specified | USA, 2 years and older | 24–30 (T2) [56] |
| 0.00 (median) | |||||
| Carrageenan | 13.9 | 0.17 (mean) | Not specified | Finland, whole population | 0.67 * [58] 18.07 (female)–31.19 (male) (T3) ** [59] 18.96 [55] |
| 0.00 (median) | USA (Florida), over 17 years France, 18 years and older | ||||
| Aluminosilicates | 0.04 | 0 | Not specified | N/A | Not available |
| Sulphites | 0.2 | 0.00 (median) | 0–0.7 | Europe (UK, Ireland, France, Italy), 8 years to 97 years New Zealand, 15 years and olderFinland, whole population France, 18 years and older | 0.296–0.620 (Europe, T2) [57] 0.017–0.132 (Europe, T3) [57] 0.05 (>65 years female) 0.27 (19–24 years female) (New Zealand, T3) [60] 0.05 * [58] 0.00 [55] |
| 0.03 (mean) | |||||
| Titanium Dioxide | 0.2 | 0.11 (mean) (median) | Not limited | Dutch, 7 to 69 years | 0.17 (T3 ***) [61] |
| Aspartame | 1.9 | 0.0 (median) | 0–40 | Europe (UK, Ireland, France, Italy), 8 years to 97 years | 0.957–4.928 (Europe, T2) [57] 0.182–1.018 (Europe, T3) [57] |
| Belgium, 15 years and older | 1.95 (T2) [62] | ||||
| 0.19 (mean) | Belgium, 15 years and older | 0.60 (T3) [62] | |||
| Japan, 20 years and older | 0.0435 (adults) [63] 0.0320 (elderly)(T3) [63] | ||||
| Ireland, 18 to 90 years France, 18 years and older | 1.05 (T1) [64] 0.62 (T2) [64] 0.28 (T3) [64] 0.000 [55] | ||||
| Sucralose | 0.8 | 0 (median) | 0–15 | Korea, whole population | 0.059 (T3); 0.044 (>65 years) to 0.95 (1–2 years) [65] |
| 0.006 (mean) | Belgium, 15 years and older | 0.42 [62] | |||
| Ireland, 18 to 90 years France, 18 years and older | 0.06 (T1) [64] 0.09 (T2) [64] 0.05(T3) [64] 0.000 [55] | ||||
| Saccharin | 0.6 | 0 | 0–5 | Korea, whole population Ireland, 18 to 90 years Finland, whole population France, 18 years and older | 0.0832 (T3); 0.049 (>65 years) to 0.1 (20–29 years) [65] |
| 0.34 (T2) [62] 0.15 (T3) [62] 0.24 (T1) [64] 0.06 (T2) [64] 0.03 (T3) [64] | |||||
| 0.8 * [58] 0.00 [55] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trakman, G.L.; Lin, W.Y.Y.; Hamilton, A.L.; Wilson-O’Brien, A.L.; Stanley, A.; Ching, J.Y.; Yu, J.; Mak, J.W.Y.; Sun, Y.; Niu, J.; et al. Processed Food as a Risk Factor for the Development and Perpetuation of Crohn’s Disease—The ENIGMA Study. Nutrients 2022, 14, 3627. https://doi.org/10.3390/nu14173627
Trakman GL, Lin WYY, Hamilton AL, Wilson-O’Brien AL, Stanley A, Ching JY, Yu J, Mak JWY, Sun Y, Niu J, et al. Processed Food as a Risk Factor for the Development and Perpetuation of Crohn’s Disease—The ENIGMA Study. Nutrients. 2022; 14(17):3627. https://doi.org/10.3390/nu14173627
Chicago/Turabian StyleTrakman, Gina L., Winnie Y. Y. Lin, Amy L. Hamilton, Amy L. Wilson-O’Brien, Annalise Stanley, Jessica Y. Ching, Jun Yu, Joyce W. Y. Mak, Yang Sun, Junkun Niu, and et al. 2022. "Processed Food as a Risk Factor for the Development and Perpetuation of Crohn’s Disease—The ENIGMA Study" Nutrients 14, no. 17: 3627. https://doi.org/10.3390/nu14173627
APA StyleTrakman, G. L., Lin, W. Y. Y., Hamilton, A. L., Wilson-O’Brien, A. L., Stanley, A., Ching, J. Y., Yu, J., Mak, J. W. Y., Sun, Y., Niu, J., Miao, Y., Lin, X., Feng, R., Chen, M., Shivappa, N., Hebert, J. R., Morrison, M., Ng, S. C., & Kamm, M. A. (2022). Processed Food as a Risk Factor for the Development and Perpetuation of Crohn’s Disease—The ENIGMA Study. Nutrients, 14(17), 3627. https://doi.org/10.3390/nu14173627