
Mediterranean Diet and Atrial Fibrillation: Lessons Learned from the AFHRI Case–Control Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
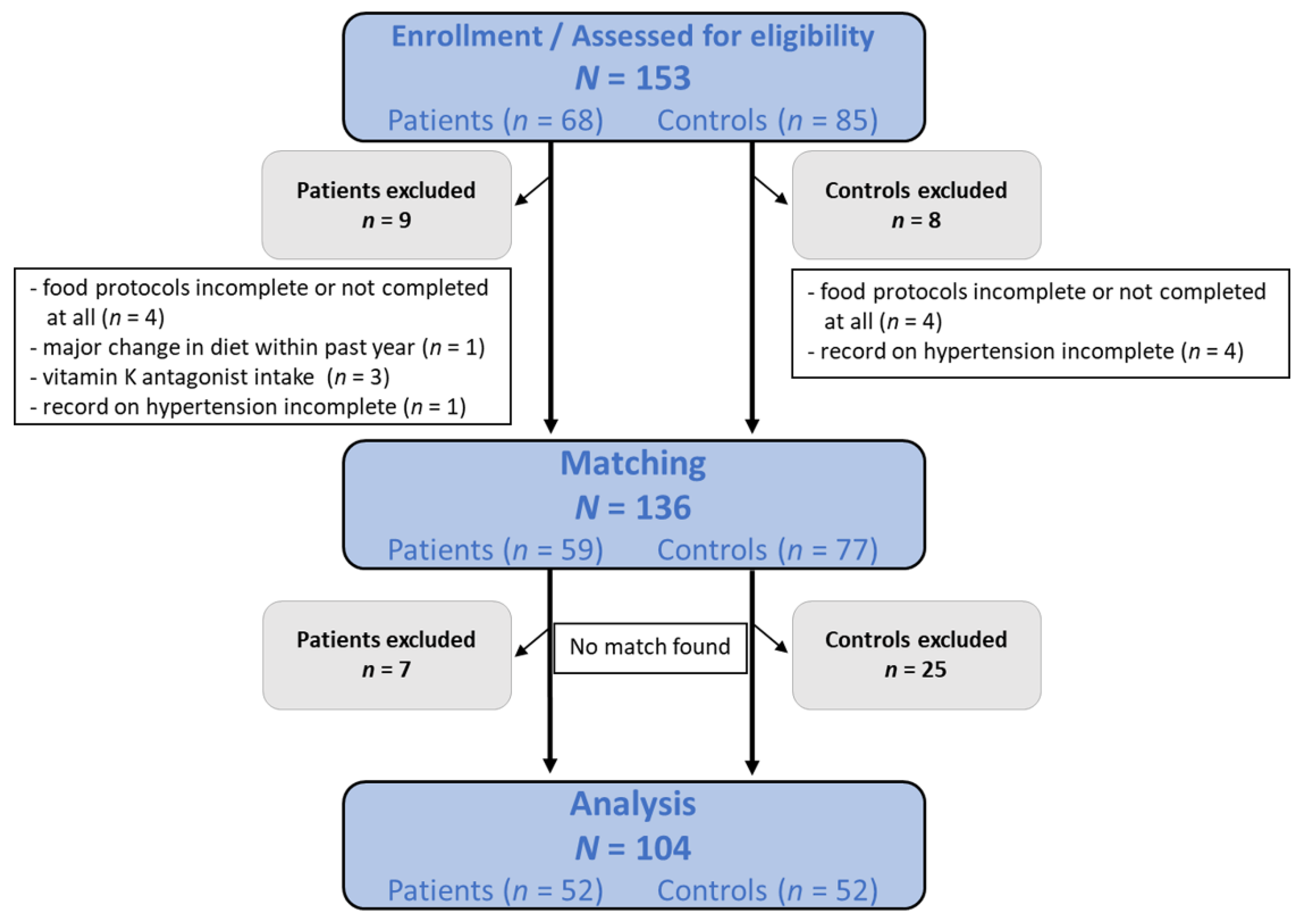
2.1. Design, Setting and Participants
2.2. Variables, Measurements and Processes
2.3. Data Handling
2.4. Participants and Matching
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
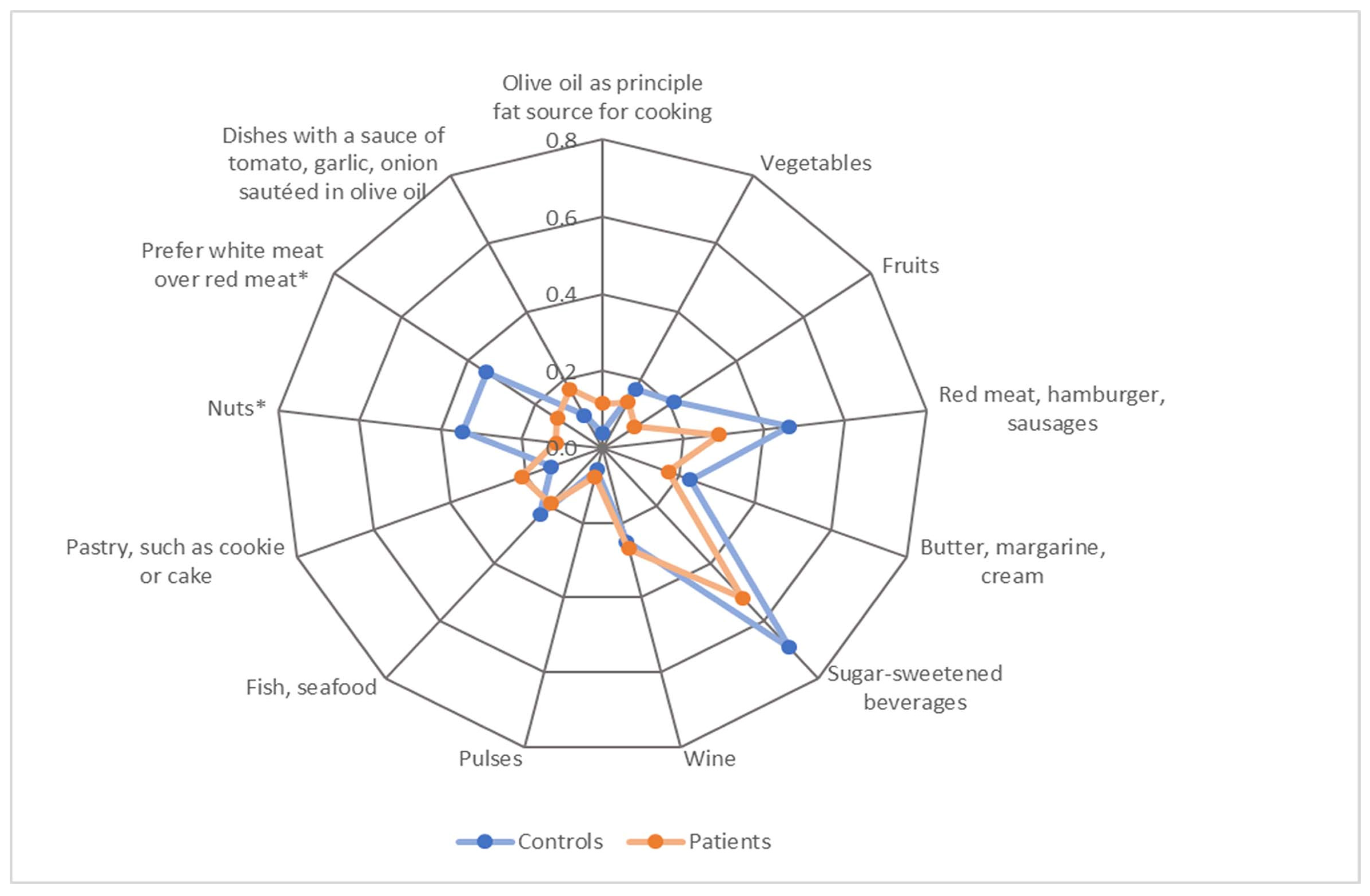
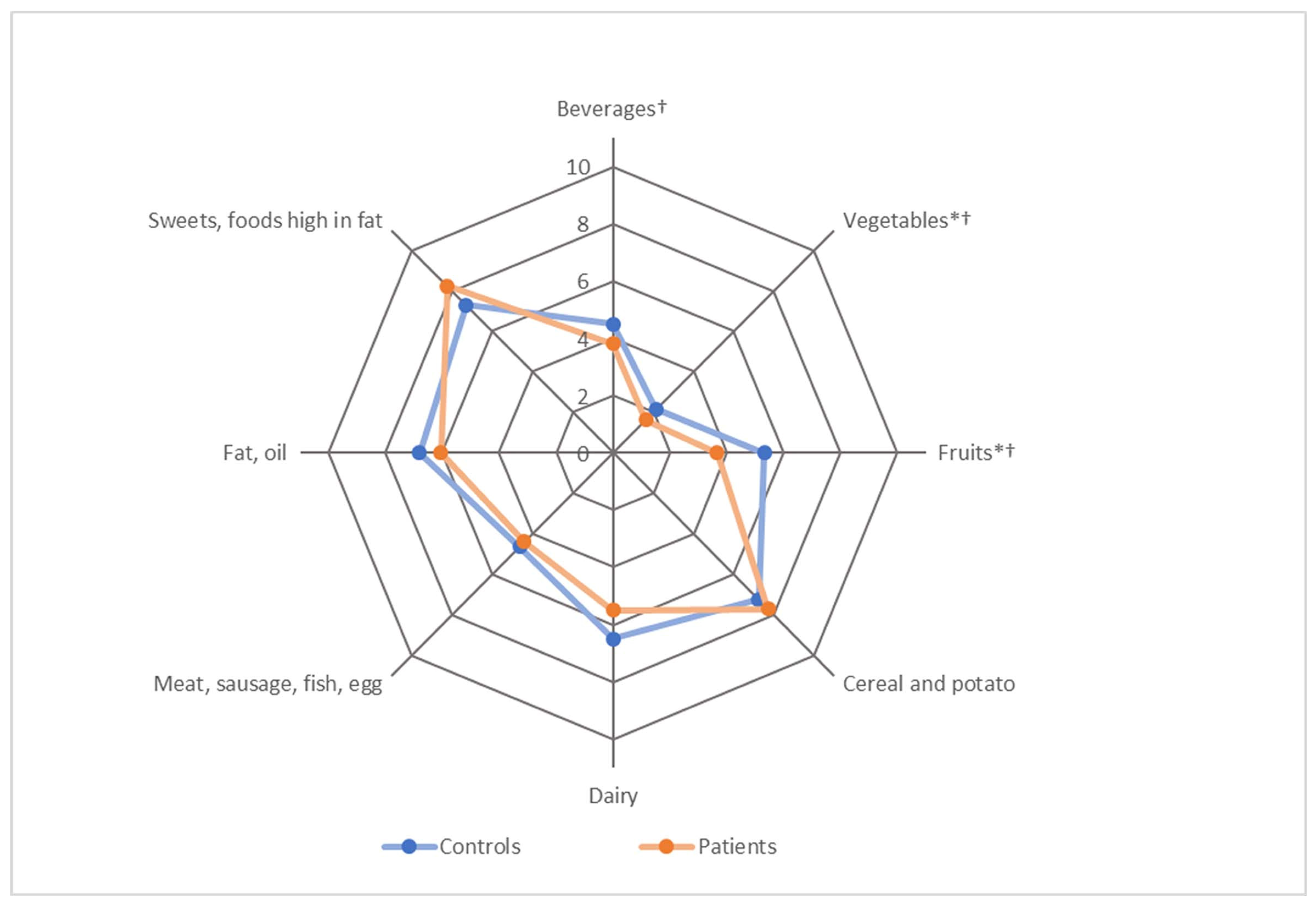
3.2. Group Differences in Dietary Patterns
3.3. Correlation Analysis
3.4. Association of MEDAS and HEI with the Presence of AF
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Heart disease and stroke statistics—2014 update: A report from the American Heart Association. Circulation 2014, 129, e28–e292. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.Q.; Birnbaum, H.G.; Mareva, M.; Tuttle, E.; Castor, A.R.; Jackman, W.; Ruskin, J. Economic burden and co-morbidities of atrial fibrillation in a privately insured population. Curr. Med. Res. Opin. 2005, 21, 1693–1699. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001, 285, 2370–2375. [Google Scholar] [CrossRef] [PubMed]
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.-H.; McAnulty, J.H.; Zheng, Z.-J.; et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Pagola, J.; Juega, J.; Francisco-Pascual, J.; Bustamante, A.; Penalba, A.; Pala, E.; Rodriguez, M.; de Lera-Alfonso, M.; Arenillas, J.F.; Cabezas, J.A.; et al. Predicting Atrial Fibrillation with High Risk of Embolization with Atrial Strain and NT-proBNP. Transl. Stroke Res. 2021, 12, 735–741. [Google Scholar] [CrossRef]
- Pistoia, F.; Sacco, S.; Tiseo, C.; Degan, D.; Ornello, R.; Carolei, A. The Epidemiology of Atrial Fibrillation and Stroke. Cardiol. Clin. 2016, 34, 255–268. [Google Scholar] [CrossRef]
- Ruddox, V.; Sandven, I.; Munkhaugen, J.; Skattebu, J.; Edvardsen, T.; Otterstad, J.E. Atrial fibrillation and the risk for myocardial infarction, all-cause mortality and heart failure: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2017, 24, 1555–1566. [Google Scholar] [CrossRef]
- Menezes, A.R.; Lavie, C.J.; DiNicolantonio, J.J.; O’Keefe, J.; Morin, D.P.; Khatib, S.; Milani, R.V. Atrial fibrillation in the 21st century: A current understanding of risk factors and primary prevention strategies. Mayo Clin. Proc. 2013, 88, 394–409. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. The Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef]
- Grundvold, I.; Skretteberg, P.T.; Liestøl, K.; Gjesdal, K.; Erikssen, G.; Kjeldsen, S.E.; Arnesen, H.; Erikssen, J.; Bodegard, J. Importance of physical fitness on predictive effect of body mass index and weight gain on incident atrial fibrillation in healthy middle-age men. Am. J. Cardiol. 2012, 110, 425–432. [Google Scholar] [CrossRef]
- Karasoy, D.; Bo Jensen, T.; Hansen, M.L.; Schmiegelow, M.; Lamberts, M.; Gislason, G.H.; Hansen, J.; Torp-Pedersen, C.; Olesen, J.B. Obesity is a risk factor for atrial fibrillation among fertile young women: A nationwide cohort study. Europace 2013, 15, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Tedrow, U.B.; Conen, D.; Ridker, P.M.; Cook, N.R.; Koplan, B.A.; Manson, J.E.; Buring, J.E.; Albert, C.M. The long- and short-term impact of elevated body mass index on the risk of new atrial fibrillation the WHS (women’s health study). J. Am. Coll. Cardiol. 2010, 55, 2319–2327. [Google Scholar] [CrossRef]
- Wanahita, N.; Messerli, F.H.; Bangalore, S.; Gami, A.S.; Somers, V.K.; Steinberg, J.S. Atrial fibrillation and obesity--results of a meta-analysis. Am. Heart J. 2008, 155, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Aldaas, O.M.; Lupercio, F.; Han, F.T.; Hoffmayer, K.S.; Krummen, D.; Ho, G.; Raissi, F.; Birgersdotter-Green, U.; Feld, G.K.; Hsu, J.C. Meta-analysis of Effect of Modest (≥10%) Weight Loss in Management of Overweight and Obese Patients with Atrial Fibrillation. Am. J. Cardiol. 2019, 124, 1568–1574. [Google Scholar] [CrossRef] [PubMed]
- Berkovitch, A.; Kivity, S.; Klempfner, R.; Segev, S.; Milwidsky, A.; Erez, A.; Sabbag, A.; Goldenberg, I.; Sidi, Y.; Maor, E. Body mass index and the risk of new-onset atrial fibrillation in middle-aged adults. Am. Heart J. 2016, 173, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Shan, Z.; Li, Y.; Baden, M.Y.; Bhupathiraju, S.N.; Wang, D.D.; Sun, Q.; Rexrode, K.M.; Rimm, E.B.; Qi, L.; Willett, W.C.; et al. Association Between Healthy Eating Patterns and Risk of Cardiovascular Disease. JAMA Intern. Med. 2020, 180, 1090–1100. [Google Scholar] [CrossRef]
- Martínez-González, M.Á.; Toledo, E.; Arós, F.; Fiol, M.; Corella, D.; Salas-Salvadó, J.; Ros, E.; Covas, M.I.; Fernández-Crehuet, J.; Lapetra, J.; et al. Extravirgin olive oil consumption reduces risk of atrial fibrillation: The PREDIMED (Prevención con Dieta Mediterránea) trial. Circulation 2014, 130, 18–26. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Larsson, S.C.; Drca, N.; Wolk, A. Alcohol consumption and risk of atrial fibrillation: A prospective study and dose-response meta-analysis. J. Am. Coll. Cardiol. 2014, 64, 281–289. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Nalliah, C.J.; Sanders, P.; Kalman, J.M. The Impact of Diet and Lifestyle on Atrial Fibrillation. Curr. Cardiol. Rep. 2018, 20, 137. [Google Scholar] [CrossRef] [PubMed]
- Storz, M.A.; Helle, P. Atrial fibrillation risk factor management with a plant-based diet: A review. J. Arrhythm. 2019, 35, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, A.V.; Miloro, C.; Pennella, S.; Pedrazzi, P.; Farinetti, A. Adherence to Mediterranean diet and intake of antioxidants influence spontaneous conversion of atrial fibrillation. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 115–121. [Google Scholar] [CrossRef]
- Mostofsky, E.; Johansen, M.B.; Lundbye-Christensen, S.; Tjønneland, A.; Mittleman, M.A.; Overvad, K. Risk of atrial fibrillation associated with coffee intake: Findings from the Danish Diet, Cancer, and Health study. Eur. J. Prev. Cardiol. 2016, 23, 922–930. [Google Scholar] [CrossRef]
- Klatsky, A.L.; Hasan, A.S.; Armstrong, M.A.; Udaltsova, N.; Morton, C. Coffee, Caffeine, and Risk of Hospitalization for Arrhythmias. Perm. J. 2011, 15, 19–25. [Google Scholar] [CrossRef]
- Cheng, M.; Hu, Z.; Lu, X.; Huang, J.; Gu, D. Caffeine intake and atrial fibrillation incidence: Dose response meta-analysis of prospective cohort studies. Can. J. Cardiol. 2014, 30, 448–454. [Google Scholar] [CrossRef]
- Li, F.-R.; Chen, G.-C.; Qin, J.; Wu, X. Dietary Fish and Long-Chain n-3 Polyunsaturated Fatty Acids Intake and Risk of Atrial Fibrillation: A Meta-Analysis. Nutrients 2017, 9, 955. [Google Scholar] [CrossRef]
- Albert, C.M.; Cook, N.R.; Pester, J.; Moorthy, M.V.; Ridge, C.; Danik, J.S.; Gencer, B.; Siddiqi, H.K.; Ng, C.; Gibson, H.; et al. Effect of Marine Omega-3 Fatty Acid and Vitamin D Supplementation on Incident Atrial Fibrillation: A Randomized Clinical Trial. JAMA 2021, 325, 1061–1073. [Google Scholar] [CrossRef]
- Bruno, E.; Manoukian, S.; Venturelli, E.; Oliverio, A.; Rovera, F.; Iula, G.; Morelli, D.; Peissel, B.; Azzolini, J.; Roveda, E.; et al. Adherence to Mediterranean Diet and Metabolic Syndrome in BRCA Mutation Carriers. Integr. Cancer Ther. 2018, 17, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Hebestreit, K.; Yahiaoui-Doktor, M.; Engel, C.; Vetter, W.; Siniatchkin, M.; Erickson, N.; Halle, M.; Kiechle, M.; Bischoff, S.C. Validation of the German version of the Mediterranean Diet Adherence Screener (MEDAS) questionnaire. BMC Cancer 2017, 17, 341. [Google Scholar] [CrossRef] [PubMed]
- Kiechle, M.; Dukatz, R.; Yahiaoui-Doktor, M.; Berling, A.; Basrai, M.; Staiger, V.; Niederberger, U.; Marter, N.; Lammert, J.; Grill, S.; et al. Feasibility of structured endurance training and Mediterranean diet in BRCA1 and BRCA2 mutation carriers—An interventional randomized controlled multicenter trial (LIBRE-1). BMC Cancer 2017, 17, 752. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; de Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Guenther, P.M.; Reedy, J.; Krebs-Smith, S.M. Development of the Healthy Eating Index-2005. J. Am. Diet. Assoc. 2008, 108, 1896–1901. [Google Scholar] [CrossRef] [PubMed]
- Reedy, J.; Krebs-Smith, S.M.; Miller, P.E.; Liese, A.D.; Kahle, L.L.; Park, Y.; Subar, A.F. Higher diet quality is associated with decreased risk of all-cause, cardiovascular disease, and cancer mortality among older adults. J. Nutr. 2014, 144, 881–889. [Google Scholar] [CrossRef]
- Haghighatdoost, F.; Sarrafzadegan, N.; Mohammadifard, N.; Sajjadi, F.; Maghroon, M.; Boshtam, M.; Alikhasi, H.; Azadbakht, L. Healthy eating index and cardiovascular risk factors among Iranians. J. Am. Coll. Nutr. 2013, 32, 111–121. [Google Scholar] [CrossRef]
- Jagodzinski, A.; Johansen, C.; Koch-Gromus, U.; Aarabi, G.; Adam, G.; Anders, S.; Augustin, M.; der Kellen, R.B.; Beikler, T.; Behrendt, C.-A.; et al. Rationale and Design of the Hamburg City Health Study. Eur. J. Epidemiol. 2020, 35, 169–181. [Google Scholar] [CrossRef]
- French, S.A.; Tangney, C.C.; Crane, M.M.; Wang, Y.; Appelhans, B.M. Nutrition quality of food purchases varies by household income: The SHoPPER study. BMC Public Health 2019, 19, 231. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- von Rüsten, A.; Illner, A.-K.; Boeing, H.; Flothkötter, M. Die Bewertung der Lebensmittelaufnahme mittels eines, Healthy Eating Index‘ (HEI-EPIC). Ernährungsumschau 2009, 7, 450–456. [Google Scholar]
- West, R.M. Best practice in statistics: The use of log transformation. Ann. Clin. Biochem. 2021, 59, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef] [PubMed]
- Baranzini, D. SPSS Single Dataframe Aggregating SPSS Multiply Imputed Split Files. Available online: https://www.researchgate.net/profile/Daniele_Baranzini/publication/328887514_SPSS_Single_dataframe_aggregating_SPSS_Multiply_Imputed_split_files/data/5be9a1cf299bf1124fce0d62/The-Bar-Procedure.docx (accessed on 16 March 2022).
- Hinkle, D.E.; Wiersma, W.; Jurs, S.G. Applied Statistics for the Behavioral Sciences, 5th ed.; Houghton Mifflin Company: Boston, MA, USA, 2003. [Google Scholar]
- Terschüren, C.; Damerau, L.; Petersen, E.L.; Harth, V.; Augustin, M.; Zyriax, B.-C. Association of Dietary Pattern, Lifestyle and Chronotype with Metabolic Syndrome in Elderly-Lessons from the Population-Based Hamburg City Health Study. Int. J. Environ. Res. Public Health 2021, 19, 377. [Google Scholar] [CrossRef]
- Leonhäuser, I.-U.; Dorandt, S.; Willmund, E.; Honsel, J. The benefit of the Mediterranean diet—Considerations to modify German food patterns. Eur. J. Nutr. 2004, 43 (Suppl. 1), I/31–38. [Google Scholar] [CrossRef]
- Zhong, V.W.; van Horn, L.; Greenland, P.; Carnethon, M.R.; Ning, H.; Wilkins, J.T.; Lloyd-Jones, D.M.; Allen, N.B. Associations of Processed Meat, Unprocessed Red Meat, Poultry, or Fish Intake with Incident Cardiovascular Disease and All-Cause Mortality. JAMA Intern. Med. 2020, 180, 503–512. [Google Scholar] [CrossRef]
- Khaw, K.-T.; Sharp, S.J.; Finikarides, L.; Afzal, I.; Lentjes, M.; Luben, R.; Forouhi, N.G. Randomised trial of coconut oil, olive oil or butter on blood lipids and other cardiovascular risk factors in healthy men and women. BMJ Open 2018, 8, e020167. [Google Scholar] [CrossRef]
- McCullough, M.L.; Feskanich, D.; Stampfer, M.J.; Giovannucci, E.L.; Rimm, E.B.; Hu, F.B.; Spiegelman, D.; Hunter, D.J.; Colditz, G.A.; Willett, W.C. Diet quality and major chronic disease risk in men and women: Moving toward improved dietary guidance. Am. J. Clin. Nutr. 2002, 76, 1261–1271. [Google Scholar] [CrossRef]
- Mu, M.; Xu, L.-F.; Hu, D.; Wu, J.; Bai, M.-J. Dietary Patterns and Overweight/Obesity: A Review Article. Iran. J. Public Health 2017, 46, 869–876. [Google Scholar]
- Ozemek, C.; Laddu, D.R.; Arena, R.; Lavie, C.J. The role of diet for prevention and management of hypertension. Curr. Opin. Cardiol. 2018, 33, 388–393. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Food Items | Total (N = 104) | Patients (n = 52) | Controls (n = 52) | |Standardised Test Statistic| | p-Value |
|---|---|---|---|---|---|
| Sociodemographic and Clinical Data | |||||
| Male | 76 (73.1%) | 38 (73.1%) | 38 (73.1%) | 0 a | 1.000 |
| Age, years | 63.0 (53.8, 69.4) | 63.7 (53.8, 69.6) | 62.5 (53.3, 69.4) | 0.23 c | 0.820 |
| Age categories | 2.06 b | 0.336 | |||
| <65 | 58 (55.8%) | 27 (51.9%) | 31 (59.6%) | ||
| 65 < 75 | 42 (40.4%) | 24 (46.2%) | 18 (34.6%) | ||
| >75 | 4 (3.8%) | 1 (1.9%) | 3 (5.8%) | ||
| Income categories | 0.35 a | 0.866 | |||
| low (<2500€) | 19 (18.3%) | 9 (17.3%) | 10 (19.2%) | ||
| middle (2500€ < 5000€) | 55 (52.9%) | 29 (55.8%) | 26 (50.0%) | ||
| high (>5000€) | 30 (28.8%) | 14 (26.9%) | 16 (30.8%) | ||
| Body mass index, kg/m2 | 25.2 (23.0, 27.3) | 26.3 (23.9, 28.6) | 24.2 (22.2, 26.9) | 3.32 c | 0.001 |
| Body mass index categories | 9.48 b | 0.011 | |||
| Underweight | 1 (1.0%) | 0 (0%) | 1 (1.9%) | ||
| Normal weight | 49 (47.1%) | 18 (34.6%) | 31 (59.6%) | ||
| Overweight | 47 (45.2%) | 28 (53.8%) | 19 (36.5%) | ||
| Obesity | 7 (6.7%) | 6 (11.5%) | 1 (1.9%) | ||
| NT-proBNP, pg/ml | 95.25 (50.5, 225.6) | 210.7 (96.1, 379.1) | 64.7 (40.4, 93.8) | 5.61 c | <0.001 |
| Resting heart rate, bpm | 61.0 (56.0, 68.3) | 64.0 (58.0, 71.3) | 59.0 (54.0, 66.5) | 2.33 c | 0.020 |
| Prevalent diseases | |||||
| Type 2 diabetes mellitus | 2 (1.9%) | 0 (0%) | 2 (3.8%) | 2.81 b | 0.495 |
| Arterial hypertension | 14 (13.5%) | 7 (13.5%) | 7 (13.5%) | 0 a | 1.000 |
| Dyslipidaemia | 19 (18.3%) | 8 (15.4%) | 11 (21.2%) | 0.58 a | 0.613 |
| Blood-thinning medications d | 0 (0%) | 0 (0%) | 0 (0%) | 0 b | 1.000 |
| Anticoagulants e | 18 (17.3%) | 18 (34.6%) | 0 (0%) | 19.20 a | <0.001 |
| Lifestyle factors | |||||
| MEDAS, points | 3 (1.25, 4) | 2 (1, 4) | 3 (2, 5) | 2.47 c | 0.014 |
| Healthy Eating Index, points | 54.9 (47.2, 60.6) | 51.7 (45.1, 57.5) | 56.5 (51.0, 63.8) | 2.93 c | 0.003 |
| Healthy Eating Index, categories | 8.85 a | 0.011 | |||
| poor (≤40 pts.) | 11 (10.6%) | 8 (15.4%) | 3 (5.8%) | ||
| improvable (>40–64 pts.) | 77 (74.0%) | 41 (78.8%) | 36 (69.2%) | ||
| good (>64 pts.) | 16 (15.4%) | 3 (5.8%) | 14 (25.0%) | ||
| Diet change past 12 months | 0.54 a | 0.626 | |||
| no | 83 (79.8%) | 40 (76.9%) | 43 (82.7%) | ||
| yes, partially | 12 (23.1%) | 12 (23.1%) | 9 (17.3%) | ||
| Energy intake, kcal/day | 2179.5 (1901.7, 2484.2) | 2137.4 (1885.3, 2417.0) | 2206.3 (1918.9, 2544.8) | 0.54 c | 0.589 |
| Physical activity, MET-h/day | 2162.0 (1350.4, 3981.8) | 2857.0 (1360.1, 5716.5) | 2016.8 (1350.4, 3154.5) | 1.69 c | 0.091 |
| Alcohol consumption | 84 (80.8%) | 42 (80.8%) | 42 (80.8%) | 0 a | 1.000 |
| Current and former smoking | 67 (64.4%) | 37 (71.2%) | 30 (57.7%) | 2.06 a | 0.219 |
| MEDAS | HEI | |||
|---|---|---|---|---|
| R | p | R | p | |
| Presence of AF | −0.243 | 0.013 | −0.289 | 0.003 |
| MEDAS | - | 0.322 | 0.001 | |
| HEI | 0.322 | 0.001 | - | |
| Age | 0.092 | 0.352 | 0.217 | 0.027 |
| Income | 0.069 | 0.488 | −0.008 | 0.939 |
| BMI | −0.300 | 0.002 | −0.394 | <0.001 |
| Log NT-proBNP | −0.090 | 0.364 | −0.129 | 0.190 |
| Resting heart rate | −0.185 | 0.060 | −0.226 | 0.021 |
| Diet change past year | 0.215 | 0.028 | −0.020 | 0.838 |
| Energy intake | −0.050 | 0.614 | 0.198 | 0.044 |
| Log MET | 0.120 | 0.225 | −0.161 | 0.102 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neumann, F.A.; Jagemann, B.; Makarova, N.; Börschel, C.S.; Aarabi, G.; Gutmann, F.; Schnabel, R.B.; Zyriax, B.-C. Mediterranean Diet and Atrial Fibrillation: Lessons Learned from the AFHRI Case–Control Study. Nutrients 2022, 14, 3615. https://doi.org/10.3390/nu14173615
Neumann FA, Jagemann B, Makarova N, Börschel CS, Aarabi G, Gutmann F, Schnabel RB, Zyriax B-C. Mediterranean Diet and Atrial Fibrillation: Lessons Learned from the AFHRI Case–Control Study. Nutrients. 2022; 14(17):3615. https://doi.org/10.3390/nu14173615
Chicago/Turabian StyleNeumann, Felix Alexander, Bettina Jagemann, Nataliya Makarova, Christin Susanna Börschel, Ghazal Aarabi, Friederike Gutmann, Renate B. Schnabel, and Birgit-Christiane Zyriax. 2022. "Mediterranean Diet and Atrial Fibrillation: Lessons Learned from the AFHRI Case–Control Study" Nutrients 14, no. 17: 3615. https://doi.org/10.3390/nu14173615
APA StyleNeumann, F. A., Jagemann, B., Makarova, N., Börschel, C. S., Aarabi, G., Gutmann, F., Schnabel, R. B., & Zyriax, B.-C. (2022). Mediterranean Diet and Atrial Fibrillation: Lessons Learned from the AFHRI Case–Control Study. Nutrients, 14(17), 3615. https://doi.org/10.3390/nu14173615