
Association between Dietary Patterns and the Risk of Depressive Symptoms in the Older Adults in Rural China

 ,
,
Abstract
:1. Introduction
2. Methods
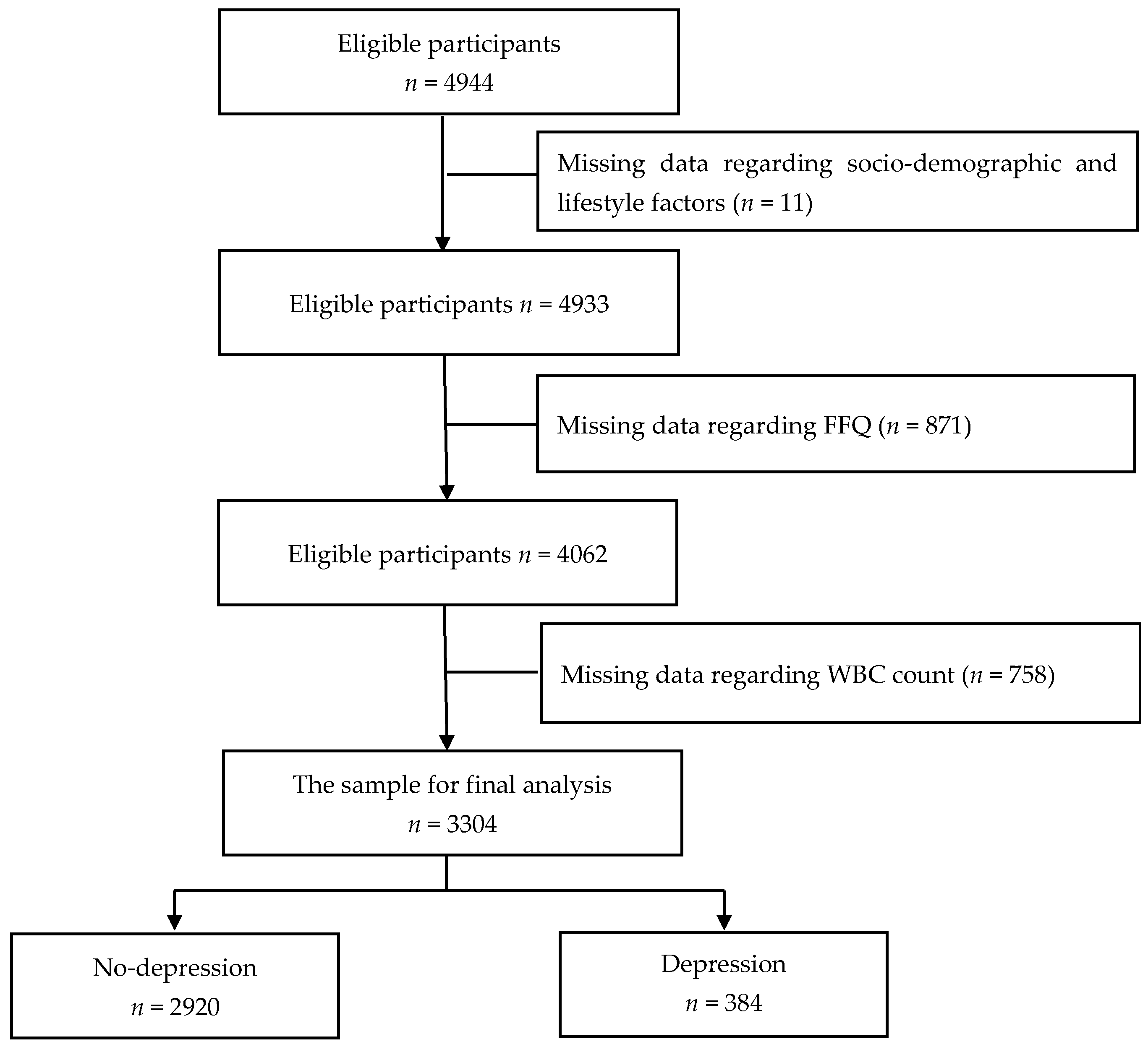
2.1. Design and Study Population
2.2. Assessment of Dietary Patters
2.3. Laboratory Procedures of Inflammatory Markers
2.4. Assessment of Depressive Symptoms
2.5. Covariates
2.6. Statistical Analyses
3. Results
3.1. Characteristics According to the Risk of Depression
3.2. Factor Loading for Dietary Patterns
3.3. Associations between Dietary Patterns and Depression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | analysis of variance |
| BDNF | brain-derived neurotrophic factor |
| CI | confidence interval |
| CNY | Chinese Yuan |
| FFQ | food frequency questionnaire |
| KMO | Kaiser-Meyer-Olkin |
| NLR | neutrophil to lymphocyte ratio |
| OR | odds ratio |
| PCA | principal component analysis |
| RRR | reduced-rank regression |
| SD | standard deviation |
| SDS | self-rating depression scale |
| WBC | white blood cell |
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Vicinanza, R.; Bersani, F.S.; D’Ottavio, E.; Murphy, M.; Bernardini, S.; Crisciotti, F.; Frizza, A.; Mazza, V.; Biondi, M.; Troisi, G.; et al. Adherence to Mediterranean diet moderates the association between multimorbidity and depressive symptoms in older adults. Arch. Gerontol. Geriatr. 2020, 88, 104022. [Google Scholar] [PubMed]
- Verhaak, P.F.; Dekker, J.H.; de Waal, M.W.; van Marwijk, H.W.; Comijs, H.C. Depression, disability and somatic diseases among elderly. J. Affect. Disord. 2014, 167, 187–191. [Google Scholar] [PubMed]
- Matison, A.P.; Mather, K.A.; Flood, V.M.; Reppermund, S. Associations between nutrition and the incidence of depression in middle-aged and older adults: A systematic review and meta-analysis of prospective observational population-based studies. Ageing Res. Rev. 2021, 70, 101403. [Google Scholar]
- Zhang, L.; Xu, Y.; Nie, H.; Zhang, Y.; Wu, Y. The prevalence of depressive symptoms among the older in China: A meta-analysis. Int. J. Geriatr. Psychiatry 2012, 27, 900–906. [Google Scholar] [PubMed]
- Gao, S.; Jin, Y.; Unverzagt, F.W.; Liang, C.; Hall, K.S.; Ma, F.; Murrell, J.R.; Cheng, Y.; Matesan, J.; Li, P.; et al. Correlates of depressive symptoms in rural elderly Chinese. Int. J. Geriatr. Psychiatry 2009, 24, 1358–1366. [Google Scholar]
- Altun, A.; Brown, H.; Szoeke, C.; Goodwill, A.M. The Mediterranean dietary pattern and depression risk: A systematic review. Neurol. Psychiatry Brain Res. 2019, 33, 1–10. [Google Scholar]
- Ullah, H.; Khan, A.; Rengasamy, K.R.R.; Di Minno, A.; Sacchi, R.; Daglia, M. The Efficacy of S-Adenosyl Methionine and Probiotic Supplementation on Depression: A Synergistic Approach. Nutrients 2022, 14, 2751. [Google Scholar]
- Marx, W.; Lane, M.; Hockey, M.; Aslam, H.; Berk, M.; Walder, K.; Borsini, A.; Firth, J.; Pariante, C.M.; Berding, K.; et al. Diet and depression: Exploring the biological mechanisms of action. Mol. Psychiatry 2021, 26, 134–150. [Google Scholar]
- Yin, W.; Löf, M.; Chen, R.; Hultman, C.M.; Fang, F.; Sandin, S. Mediterranean diet and depression: A population-based cohort study. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 153. [Google Scholar]
- Wang, C.J.; Yang, T.F.; Wang, G.S.; Zhao, Y.Y.; Yang, L.J. Association between dietary patterns and depressive symptoms among middle-aged adults in China in 2016–2017. Psychiatry Res. 2018, 260, 123–129. [Google Scholar]
- Li, Y.; Lv, M.R.; Wei, Y.J.; Sun, L.; Zhang, J.X.; Zhang, H.G.; Li, B. Dietary patterns and depression risk: A meta-analysis. Psychiatry Res. 2017, 253, 373–382. [Google Scholar] [CrossRef]
- Vermeulen, E.; Brouwer, I.A.; Stronks, K.; Bandinelli, S.; Ferrucci, L.; Visser, M.; Nicolaou, M. Inflammatory dietary patterns and depressive symptoms in Italian older adults. Brain Behav. Immun. 2018, 67, 290–298. [Google Scholar] [CrossRef]
- Tolkien, K.; Bradburn, S.; Murgatroyd, C. An anti-inflammatory diet as a potential intervention for depressive disorders: A systematic review and meta-analysis. Clin. Nutr. 2019, 38, 2045–2052. [Google Scholar] [CrossRef]
- Jorgensen, D.; White, G.E.; Sekikawa, A.; Gianaros, P. Higher dietary inflammation is associated with increased odds of depression independent of Framingham Risk Score in the National Health and Nutrition Examination Survey. Nutr. Res. 2018, 54, 23–32. [Google Scholar] [CrossRef]
- Shin, D.; Kwon, S.C.; Kim, M.H.; Lee, K.W.; Choi, S.Y.; Shivappa, N.; Hébert, J.R.; Chung, H.K. Inflammatory potential of diet is associated with cognitive function in an older adult Korean population. Nutrition 2018, 55, 56–62. [Google Scholar] [CrossRef]
- Quirk, S.E.; Williams, L.J.; O’Neil, A.; Pasco, J.A.; Jacka, F.N.; Housden, S.; Berk, M.; Brennan, S.L. The association between diet quality, dietary patterns and depression in adults: A systematic review. BMC Psychiatry 2013, 13, 175. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, G.; Pan, X. China Food Composition, 2nd ed.; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Weikert, C.; Schulze, M.B. Evaluating dietary patterns: The role of reduced rank regression. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 341–346. [Google Scholar] [CrossRef]
- Cao, L.; Liu, Y.; Liang, X.; Zheng, Y.; Li, W.; Yan, J.; Huang, G. Association between dietary patterns during the third trimester and the risk of postpartum depression in China. J. Affect. Disord. 2020, 264, 370–372. [Google Scholar] [CrossRef]
- Zhang, C.; Xue, Y.; Zhao, H.; Zheng, X.; Zhu, R.; Du, Y.; Zheng, J.; Yang, T. Prevalence and related influencing factors of depressive symptoms among empty-nest elderly in Shanxi, China. J. Affect. Disord. 2019, 245, 750–756. [Google Scholar] [CrossRef]
- Gu, Y.; Li, X.; Zhang, Q.; Liu, L.; Meng, G.; Wu, H.; Zhang, S.; Wang, Y.; Zhang, T.; Wang, X.; et al. Grip strength and depressive symptoms in a large-scale adult population: The TCLSIH cohort study. J. Affect. Disord. 2021, 279, 222–228. [Google Scholar] [CrossRef]
- Zung, W.W. The measurement of affects: Depression and anxiety. Mod. Probl. Pharmacopsychiatr. 1974, 7, 170–188. [Google Scholar]
- Zung, W.W.; Richards, C.B.; Short, M.J. Self-rating depression scale in an outpatient clinic: Further validation of the SDS. Arch. Gen. Psychiatry 1965, 13, 508–515. [Google Scholar] [CrossRef]
- Jokelainen, J.; Timonen, M.; Keinänen-Kiukaanniemi, S.; Härkönen, P.; Jurvelin, H.; Suija, K. Validation of the Zung self-rating depression scale (SDS) in older adults. Scand. J. Prim. Health Care 2019, 37, 353–357. [Google Scholar] [CrossRef]
- Lin, H.; Jin, M.; Liu, Q.; Yue, D.; Fu, J.; Sun, C.; Ma, F.; Li, W.; Liu, H.; Zhang, X.; et al. Gender-specific prevalence and influencing factors of depression in elderly in rural China: A cross-sectional study. J. Affect. Disord 2021, 288, 99–106. [Google Scholar] [CrossRef]
- Luppa, M.; Sikorski, C.; Luck, T.; Ehreke, L.; Konnopka, A.; Wiese, B.; Weyerer, S.; Konig, H.H.; Riedel-Heller, S.G. Age- and gender-specific prevalence of depression in latest-life–systematic review and meta-analysis. J. Affect. Disord. 2012, 136, 212–221. [Google Scholar] [CrossRef]
- Volkert, J.; Schulz, H.; Harter, M.; Wlodarczyk, O.; Andreas, S. The prevalence of mental disorders in older people in Western countries-a meta-analysis. Ageing Res. Rev. 2013, 12, 339–353. [Google Scholar] [CrossRef]
- Adjibade, M.; Assmann, K.E.; Andreeva, V.A.; Lemogne, C.; Hercberg, S.; Galan, P.; Kesse-Guyot, E. Prospective association between adherence to the mediterranean diet and risk of depressive symptoms in the French SU. VI. MAX cohort. Eur. J. Nutr. 2018, 57, 1225–1235. [Google Scholar] [CrossRef]
- Hershey, M.S.; Sanchez-Villegas, A.; Sotos-Prieto, M.; Fernandez-Montero, A.; Pano, O.; Lahortiga-Ramos, F.; Martínez-González, M.Á.; Ruiz-Canela, M. The Mediterranean lifestyle and the risk of depression in middle-aged adults. J. Nutr. 2022, 152, 227–234. [Google Scholar] [CrossRef]
- Crichton, G.E.; Bryan, J.; Hodgson, J.M.; Murphy, K.J. Mediterranean diet adherence and self-reported psychological functioning in an Australian sample. Appetite 2013, 70, 53–59. [Google Scholar] [CrossRef]
- Miki, T.; Kochi, T.; Kuwahara, K.; Eguchi, M.; Kurotani, K.; Tsuruoka, H.; Ito, R.; Kabe, I.; Kawakami, N.; Mizoue, T.; et al. Dietary patterns derived by reduced rank regression (RRR) and depressive symptoms in Japanese employees: The Furukawa nutrition and health study. Psychiatry Res. 2015, 229, 214–219. [Google Scholar] [CrossRef]
- Akbaraly, T.N.; Brunner, E.J.; Ferrie, J.E.; Marmot, M.G.; Kivimaki, M.; Singh-Manoux, A. Dietary pattern and depressive symptoms in middle age. Br. J. Psychiatry 2009, 195, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Cumming, R.G.; Naganathan, V.; Ribeiro, R.V.; Le Couteur, D.G.; Handelsman, D.J.; Waite, L.M.; Hirani, V. The association between antioxidant intake, dietary pattern and depressive symptoms in older Australian men: The Concord Health and Ageing in Men Project. Eur. J. Nutr. 2021, 60, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Bayes, J.; Schloss, J.; Sibbritt, D. Effects of Polyphenols in a Mediterranean Diet on Symptoms of Depression: A Systematic Literature. Adv. Nutr. 2020, 11, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.; Hughes, C.F.; Ward, M.; Hoey, L.; McNulty, H. Diet, nutrition and the ageing brain: Current evidence and new directions. Proc. Nutr. Soc. 2018, 77, 152–163. [Google Scholar] [CrossRef]
- Su, Q.; Yu, B.; He, H.; Zhang, Q.; Meng, G.; Wu, H.; Du, H.; Liu, L.; Shi, H.; Xia, Y.; et al. Nut Consumption is associated with depressive symptoms among Chinese adults. Depress. Anxiety 2016, 33, 1065–1072. [Google Scholar] [CrossRef]
- Wang, J.; Um, P.; Dickerman, B.A.; Liu, J. Zinc, Magnesium, Selenium and Depression: A Review of the Evidence, Potential Mechanisms and Implications. Nutrients 2018, 10, 58410. [Google Scholar] [CrossRef]
- Masana, M.F.; Haro, J.M.; Mariolis, A.; Piscopo, S.; Valacchi, G.; Bountziouka, V.; Anastasiou, F.; Zeimbekis, A.; Tyrovola, D.; Gotsis, E.; et al. Mediterranean diet and depression among older individuals: The multinational MEDIS study. Exp. Gerontol. 2018, 110, 67–72. [Google Scholar] [CrossRef]
- Bergmans, R.S.; Malecki, K.M. The association of dietary inflammatory potential with depression and mental well-being among U.S. adults. Prev. Med. 2017, 99, 313–319. [Google Scholar] [CrossRef]
- Chan, R.; Chan, D.; Woo, J. A prospective cohort study to examine the association between dietary patterns and depressive symptoms in older Chinese people in Hong Kong. PLoS ONE 2014, 9, e105760. [Google Scholar] [CrossRef]
- Gougeon, L.; Payette, H.; Morais, J.; Gaudreau, P.; Shatenstein, B.; Gray-Donald, K. Dietary patterns and incidence of depression in a cohort of communitydwelling older Canadians. J. Nutr. Health Aging 2015, 19, 431–436. [Google Scholar] [CrossRef]
- Lane, M.M.; Gamage, E.; Travica, N.; Dissanayaka, T.; Ashtree, D.N.; Gauci, S.; Lotfaliany, M.; O’Neil, A.; Jacka, F.N.; Marx, W. Ultra-Processed Food Consumption and Mental Health: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2022, 14, 2568. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Food Groups | Food Items |
|---|---|
| Tubers | Sweet potato, yam, taro, potato and products |
| Fruits | Stone fruits, pome fruits, melon fruits, berry fruits, citrus fruits and grape |
| Bacteria and algae | Mushroom, fungi, white fungus, kelp, seaweed and other algae |
| Legumes | Soybeans, other beans and soy products |
| Vegetables | Leaf vegetables, root vegetables, stem vegetables, melon and eggplant vegetables and flower vegetables |
| Nuts | Nuts, walnuts, peanuts, sesame, other nuts and products |
| Poultry meat | Chicken, duck, goose |
| Offal | Heart, liver, kidney, lung |
| Seafood | Fish and shellfish |
| Red meat | Pork, mutton, lamb, beef |
| Fried foods | Fried dough twist, deep-fried cake, fried dough sticks and instant noodles |
| Snacks | Ice cream, cake, pastry, snacks, butter products, candied fruits, confections and added sugar |
| Pickles | Pickles |
| Grains | Whole grains and refined grains |
| Dairy products | Milk, yoghurt and other dairy products |
| Eggs | Eggs, duck eggs and preserved eggs |
| Beverages | Fruit- and vegetable juices, soft beverages, tea, red wine, white spirits, beer and other alcoholic beverages |
| Characteristics | Total (n = 3304) | Depression | |||
|---|---|---|---|---|---|
| Yes (n = 384) | No (n = 2920) | pa | |||
| Age (years) | 67.73 ± 4.88 | 67.77 ± 4.85 | 67.72 ± 4.89 | 0.864 | |
| Sex | Male | 1486 (44.98%) | 134 (9.02%) | 1352 (90.98%) | <0.001 |
| Female | 1818 (55.02%) | 250 (13.75%) | 1568 (86.25%) | ||
| Education (years) | <6 | 792 (23.97%) | 125 (15.78%) | 667 (84.22%) | <0.001 |
| 6- | 1108 (33.54%) | 134 (12.09%) | 974 (87.91%) | ||
| ≥9 | 1404 (42.49%) | 125 (8.90%) | 1279 (91.10%) | ||
| Household income per month (CNY) | <5000 | 2782 (84.20%) | 358 (12.87%) | 2424 (87.13%) | <0.001 |
| ≥5000 | 522 (15.80%) | 26 (4.98%) | 496 (95.02%) | ||
| Employment | Employed or retired | 1140 (34.50%) | 88 (7.72%) | 1052 (92.28%) | <0.001 |
| Unemployed | 2164 (65.50%) | 296 (13.68%) | 1868 (86.32%) | ||
| Living alone | Yes | 245 (7.42%) | 45 (18.37%) | 200 (81.63%) | 0.001 |
| No | 3059 (92.58%) | 339 (11.08%) | 2720 (88.92%) | ||
| Social activities | Yes | 1063 (32.17%) | 90 (8.47%) | 973 (91.53%) | <0.001 |
| No | 2241 (67.83%) | 294 (13.12%) | 1947 (86.88%) | ||
| Physical exercises | Yes | 2913 (88.17%) | 304 (10.44%) | 2609 (89.56%) | <0.001 |
| No | 391 (11.83%) | 80 (20.46%) | 311 (79.54%) | ||
| Sleep duration (h) | <6 | 58 (1.76%) | 6 (10.34%) | 52 (89.66%) | 0.016 |
| 6- | 944 (28.57%) | 101 (10.70%) | 843 (89.30%) | ||
| 8- | 1986 (60.11%) | 223 (11.23%) | 1763 (88.77%) | ||
| ≥10 | 316 (9.56%) | 54 (17.09%) | 262 (82.91%) | ||
| No. chronic diseases | 0 | 1576 (47.70%) | 190 (12.06%) | 1386 (87.94%) | 0.059 |
| 1 | 1284 (38.86%) | 131 (10.20%) | 1153 (89.80%) | ||
| ≥2 | 444 (13.44%) | 63 (14.19%) | 381 (85.81%) | ||
| Food Groups | PCA | RRR | |||
|---|---|---|---|---|---|
| Vegetables-Fruit Pattern | Animal Food Pattern | Processed Food Pattern | Milk-Egg Pattern | Inflammatory Dietary Pattern | |
| Tubers | 0.606 | 0.114 | −0.037 | −0.084 | −0.232 |
| Fruits | 0.596 | 0.039 | 0.031 | 0.239 | 0.297 |
| Bacteria and algae | 0.595 | 0.103 | 0.196 | −0.120 | −0.181 |
| Legumes | 0.573 | 0.257 | 0.191 | −0.117 | −0.245 |
| Vegetables | 0.572 | 0.153 | −0.203 | 0.051 | −0.209 |
| Nuts | 0.560 | −0.007 | 0.124 | 0.153 | −0.033 |
| Poultry meat | 0.157 | 0.771 | 0.062 | 0.040 | −0.145 |
| Offal | −0.074 | 0.758 | 0.128 | 0.014 | 0.143 |
| Seafood | 0.324 | 0.615 | −0.032 | 0.013 | −0.099 |
| Red meat | 0.360 | 0.439 | −0.084 | 0.045 | −0.202 |
| Fried foods | −0.011 | 0.130 | 0.690 | 0.060 | 0.516 |
| Snacks | 0.002 | 0.111 | 0.602 | 0.364 | 0.372 |
| Pickles | 0.296 | 0.046 | 0.406 | −0.300 | 0.305 |
| Grains | 0.038 | −0.075 | 0.256 | −0.120 | −0.009 |
| Dairy products | 0.319 | −0.066 | 0.002 | 0.601 | −0.086 |
| Eggs | −0.030 | 0.078 | 0.120 | 0.442 | 0.039 |
| Beverages | −0.023 | 0.003 | −0.135 | 0.440 | 0.348 |
| Explained variation in food groups (%) | 14.71 | 11.19 | 7.43 | 6.54 | 6.23 |
| Explained variation in WBC count and NLR (%) | -- | -- | -- | -- | 0.70 |
| Dietary Patterns | Quartiles of Dietary Patterns | p | |||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | ||
| Vegetables-fruits pattern | |||||
| n | 826 | 826 | 826 | 826 | |
| SDS score | 41.04 ± 9.27 | 38.56 ± 8.97 | 36.32 ± 9.06 | 34.96 ± 8.35 | <0.001 |
| Pervasive affective | 2.68 ± 1.07 | 2.53 ± 1.00 | 2.42 ± 0.90 | 2.40 ± 0.85 | <0.001 |
| Physiological | 13.31 ± 3.01 | 12.69 ± 3.25 | 12.11 ± 3.28 | 11.89 ± 3.09 | <0.001 |
| Psychomotor | 3.40 ± 1.29 | 3.10 ± 1.20 | 2.91 ± 1.20 | 2.87 ± 1.21 | <0.001 |
| Psychological | 13.45 ± 4.06 | 12.52 ± 4.10 | 11.61 ± 3.92 | 10.81 ± 3.60 | <0.001 |
| Animal foods pattern | |||||
| n | 826 | 826 | 826 | 826 | |
| SDS score | 38.23 ± 9.38 | 39.49 ± 9.58 | 37.32 ± 9.12 | 35.85 ± 8.33 | <0.001 |
| Pervasive affective | 2.52 ± 1.00 | 2.63 ± 1.04 | 2.43 ± 0.86 | 2.46 ± 0.95 | <0.001 |
| Physiological | 12.76 ± 3.26 | 12.94 ± 3.12 | 12.29 ± 3.21 | 12.01 ± 3.15 | <0.001 |
| Psychomotor | 3.14 ± 1.34 | 3.20 ± 1.26 | 3.00 ± 1.17 | 2.94 ± 1.19 | <0.001 |
| Psychological | 12.17 ± 4.11 | 12.82 ± 4.25 | 12.13 ± 4.06 | 11.28 ± 3.58 | <0.001 |
| Processed foods pattern | |||||
| n | 826 | 826 | 826 | 826 | |
| SDS score | 35.39 ± 9.25 | 39.06 ± 9.57 | 37.99 ± 8.63 | 38.44 ± 8.94 | <0.001 |
| Pervasive affective | 2.43 ± 0.91 | 2.56 ± 1.01 | 2.49 ± 0.93 | 2.54 ± 1.01 | 0.033 |
| Physiological | 11.97 ± 3.33 | 12.82 ± 3.21 | 12.50 ± 2.94 | 12.72 ± 3.28 | <0.001 |
| Psychomotor | 2.86 ± 1.25 | 3.15 ± 1.24 | 3.08 ± 1.19 | 3.19 ± 1.27 | <0.001 |
| Psychological | 11.05 ± 3.85 | 12.72 ± 4.18 | 12.33 ± 4.01 | 12.30 ± 3.94 | <0.001 |
| Milk-eggs pattern | |||||
| n | 826 | 826 | 826 | 826 | |
| SDS score | 37.57 ± 9.23 | 39.08 ± 9.67 | 37.40 ± 9.01 | 36.84 ± 8.77 | <0.001 |
| Pervasive affective | 2.50 ± 0.96 | 2.59 ± 1.04 | 2.52 ± 0.97 | 2.42 ± 0.88 | 0.005 |
| Physiological | 12.38 ± 3.14 | 12.83 ± 3.29 | 12.40 ± 3.14 | 12.39 ± 3.24 | 0.010 |
| Psychomotor | 3.07 ± 1.23 | 3.14 ± 1.23 | 3.05 ± 1.24 | 3.02 ± 1.28 | 0.217 |
| Psychological | 12.10 ± 4.10 | 12.71 ± 4.21 | 11.95 ± 3.94 | 11.64 ± 3.85 | <0.001 |
| Inflammatory dietary pattern | |||||
| n | 831 | 824 | 824 | 825 | |
| SDS score | 35.43 ± 8.91 | 38.17 ± 9.53 | 38.70 ± 9.18 | 38.60 ± 8.82 | <0.001 |
| Pervasive affective | 2.39 ± 0.85 | 2.50 ± 0.94 | 2.55 ± 1.02 | 2.59 ± 1.04 | <0.001 |
| Physiological | 12.00 ± 3.30 | 12.58 ± 3.30 | 12.67 ± 3.05 | 12.76 ± 3.12 | <0.001 |
| Psychomotor | 2.87 ± 1.23 | 3.11 ± 1.25 | 3.13 ± 1.21 | 3.17 ± 1.27 | <0.001 |
| Psychological | 11.09 ± 3.82 | 12.35 ± 4.21 | 12.61 ± 4.07 | 12.35 ± 3.90 | <0.001 |
| Dietary Patterns | Quartiles of Dietary Patterns | |||
|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |
| Vegetables-fruits pattern | ||||
| n | 826 | 826 | 826 | 826 |
| Model 1 a | 1.00 | 0.58 (0.44,0.76) * | 0.46 (0.34,0.61) * | 0.31 (0.23,0.43) * |
| Model 2 b | 1.00 | 0.60 (0.44,0.80) * | 0.47 (0.34,0.65) * | 0.31 (0.21,0.45) * |
| Model 3 c | 1.00 | 0.62 (0.46,0.83) * | 0.54 (0.38,0.75) * | 0.39 (0.26,0.57) * |
| Animal foods pattern | ||||
| n | 826 | 826 | 826 | 826 |
| Model 1 a | 1.00 | 1.26 (0.96,1.67) | 0.73 (0.54,0.99) * | 0.54 (0.39,0.75) * |
| Model 2 b | 1.00 | 0.94 (0.70,1.26) | 0.65 (0.47,0.90) * | 0.51 (0.37,0.72) * |
| Model 3 c | 1.00 | 0.94 (0.69,1.26) | 0.69 (0.50,0.95) * | 0.58 (0.41,0.82) * |
| Processed foods pattern | ||||
| n | 826 | 826 | 826 | 826 |
| Model 1 a | 1.00 | 1.51 (1.11,2.04) * | 1.08 (0.79,1.44) | 1.33 (0.98,1.81) |
| Model 2 b | 1.00 | 0.86 (0.62,1.21) | 0.82 (0.59,1.15) | 1.12 (0.81,1.55) |
| Model 3 c | 1.00 | 0.92 (0.65,1.28) | 0.83 (0.59,1.17) | 1.11 (0.80,1.54) |
| Milk-eggs pattern | ||||
| n | 826 | 826 | 826 | 826 |
| Model 1 a | 1.00 | 1.35 (1.01,1.81) * | 0.99 (0.73,1.34) | 0.82 (0.60,1.13) |
| Model 2 b | 1.00 | 0.87 (0.63,1.22) | 0.79 (0.58,1.09) | 0.77 (0.56,1.07) |
| Model 3 c | 1.00 | 0.93 (0.67,1.30) | 0.84 (0.61,1.17) | 0.84 (0.60,1.18) |
| Inflammatory dietary pattern | ||||
| n | 831 | 824 | 824 | 825 |
| Model 1 a | 1.00 | 1.85 (1.34,2.55) * | 1.87 (1.35,2.58) * | 1.63 (1.17,2.27) * |
| Model 2 d | 1.00 | 1.71 (1.23,2.38) * | 1.70 (1.22,2.36) * | 1.44 (1.03,2.03) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, J.; Ren, Q.; Lin, H.; Liu, Q.; Fu, J.; Sun, C.; Li, W.; Ma, F.; Zhu, Y.; Li, Z.; et al. Association between Dietary Patterns and the Risk of Depressive Symptoms in the Older Adults in Rural China. Nutrients 2022, 14, 3538. https://doi.org/10.3390/nu14173538
Yan J, Ren Q, Lin H, Liu Q, Fu J, Sun C, Li W, Ma F, Zhu Y, Li Z, et al. Association between Dietary Patterns and the Risk of Depressive Symptoms in the Older Adults in Rural China. Nutrients. 2022; 14(17):3538. https://doi.org/10.3390/nu14173538
Chicago/Turabian StyleYan, Jing, Qinghan Ren, Hongyan Lin, Qian Liu, Jingzhu Fu, Changqing Sun, Wen Li, Fei Ma, Yun Zhu, Zhenshu Li, and et al. 2022. "Association between Dietary Patterns and the Risk of Depressive Symptoms in the Older Adults in Rural China" Nutrients 14, no. 17: 3538. https://doi.org/10.3390/nu14173538
APA StyleYan, J., Ren, Q., Lin, H., Liu, Q., Fu, J., Sun, C., Li, W., Ma, F., Zhu, Y., Li, Z., Zhang, G., Du, Y., Liu, H., Zhang, X., Chen, Y., Wang, G., & Huang, G. (2022). Association between Dietary Patterns and the Risk of Depressive Symptoms in the Older Adults in Rural China. Nutrients, 14(17), 3538. https://doi.org/10.3390/nu14173538