
Association between Legume Consumption and Risk of Hypertension in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk Cohort

 ,
,  and
and 
Abstract
:1. Introduction
2. Methods
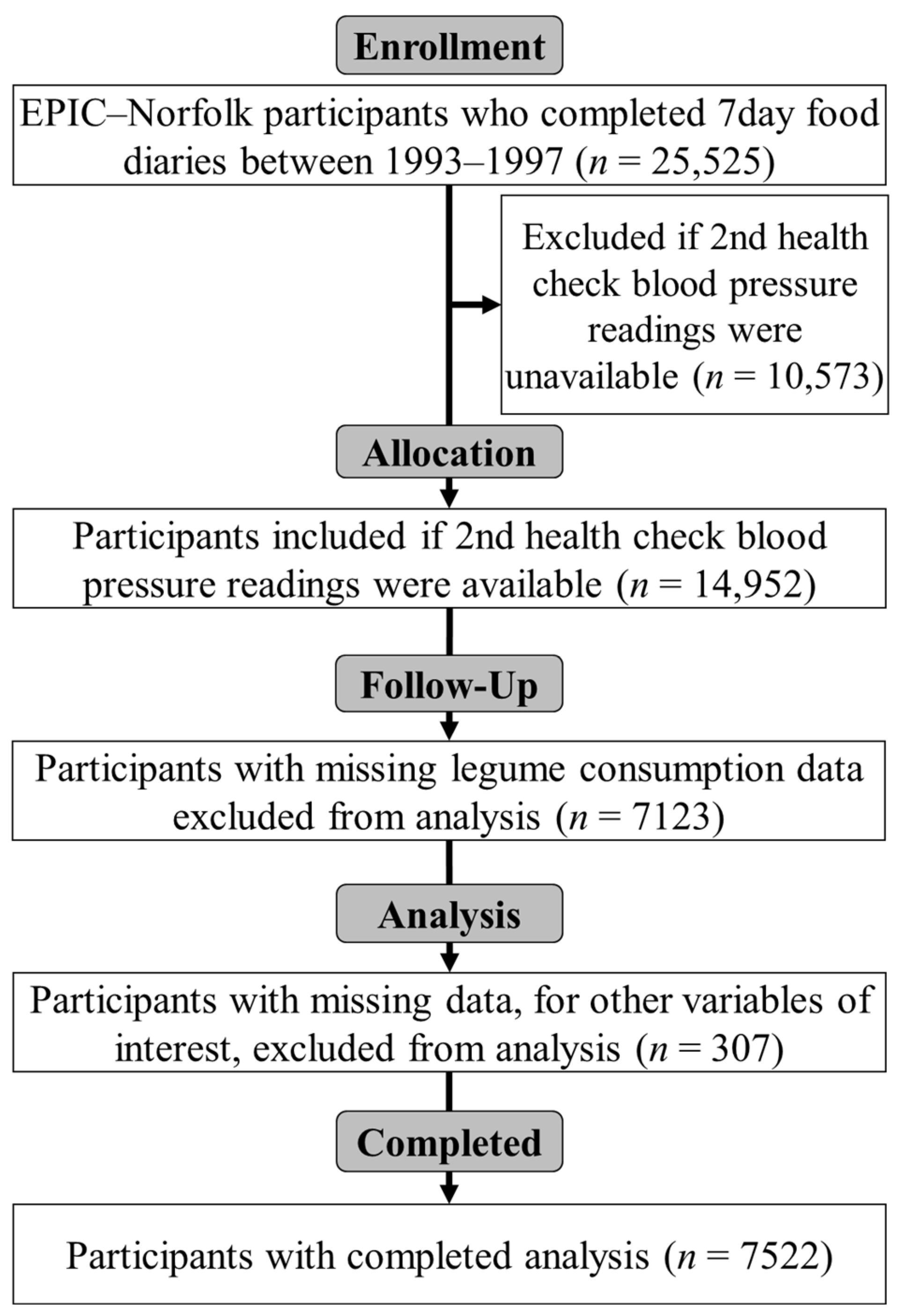
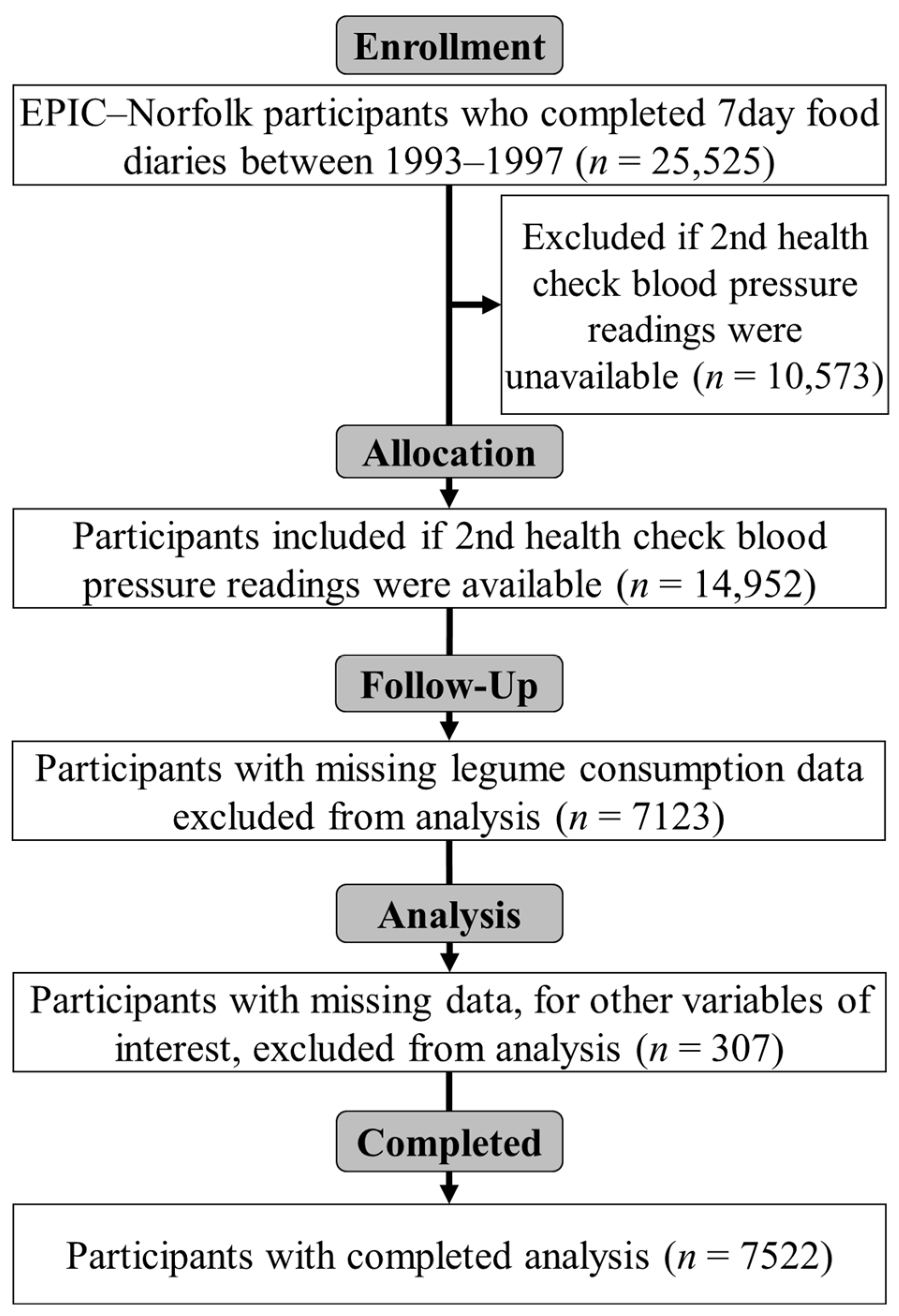
2.1. Study Population
2.2. Exposure Variables
2.3. Outcome Measurement
2.4. Confounding Variables
2.5. Statistical Analysis
3. Results
3.1. Participants
3.2. Legume Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| 1 | We would like to know the type and amount of physical activity involved in your work. Please tick what best corresponds to your present activities from the following four possibilities. | |
| ___ Sedentary occupation | You spend most of your time sitting (such as in an office). | |
| ___ Standing occupation | You spend most of your time standing or walking. However, your work does not require intense physical efforts (e.g., shop assistant, hairdresser, guard). | |
| ___ Physical work | This involves some physical effort including handling of heavy objects and use of tools (e.g., plumber, cleaner, nurse, sports instructor, electrician, carpenter). | |
| ___ Heavy manual work | This involves very vigorous physical activity including handling of very heavy objects (e.g., docker, miner, bricklayer, construction worker). | |
| 2 | In a typical week during the past 12 months, how many hours did you spend on each of the following activities? (Put ‘0’ if none.) Cycling, including cycling to work and during leisure time | |
| In summer ____ hours per week | ||
| In winter ____ hours per week | ||
| Other physical exercise such as keep fit, aerobics, swimming, jogging | ||
| In summer ____ hours per week | ||
| In winter ____ hours per week | ||
| Hours per day of recreational activity computed from [(mean of summer and winter hours per week cycling) + (mean of summer and winter hours per week other physical exercise)]/7 | ||
Appendix B
| Category Description | |
| Inactive | Sedentary job and no recreational activity |
| Moderately inactive | Sedentary job with <0.5 h recreational activity per day inactive or standing job with no recreational activity |
| Moderately active | Sedentary job with 0.5–1 h recreational activity per dayor standing job with 0.5 h recreational activity per day or physical job with no recreational activity |
| Active | Sedentary job with >1 h recreational activity per dayor standing job with >1 h recreational activity per dayor physical job with at least some recreational activity or heavy manual job |
| These categories are derived from the two questions in Appendix A. | |
References
- Hall, M.E.; Cohen, J.B.; Ard, J.D.; Egan, B.M.; Hall, J.E.; Lavie, C.J.; Ma, J.; Ndumele, C.E.; Schauer, P.R.; Shimbo, D.; et al. Weight-loss strategies for prevention and treatment of hypertension: A scientific statement from the American heart association. Hypertension 2021, 78, e38–e50. [Google Scholar] [CrossRef] [PubMed]
- Filippou, C.D.; Tsioufis, C.P.; Thomopoulos, C.G.; Mihas, C.C.; Dimitriadis, K.S.; Sotiropoulou, L.I.; Chrysochoou, C.A.; Nihoyannopoulos, P.I.; Tousoulis, D.M. Dietary approaches to stop hypertension (DASH) diet and blood pressure reduction in adults with and without hypertension: A systematic review and meta-analysis of randomized controlled trials. Adv. Nutr. 2020, 11, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.B. Hypertension in obesity and the impact of weight loss. Curr. Cardiol. Rep. 2017, 19, 98. [Google Scholar] [CrossRef] [PubMed]
- Ozemek, C.; Laddu, D.R.; Arena, R.; Lavie, C.J. The role of diet for prevention and management of hypertension. Curr. Opin. Cardiol. 2018, 33, 388–393. [Google Scholar] [CrossRef]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef]
- Vogt, T.M.; Appel, L.J.; Obarzanek, E.V.A.; Moore, T.J.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Cutler, J.A.; Windhauser, M.M.; et al. Dietary approaches to stop hypertension: Rationale, design, and methods. DASH Collaborative Research Group. J. Am. Diet. Assoc. 1999, 99, S12–S18. [Google Scholar] [CrossRef]
- Huang, L.; Trieu, K.; Yoshimura, S.; Neal, B.; Woodward, M.; Campbell, N.R.; Li, Q.; Lackland, D.T.; Leung, A.A.; Anderson, C.A.; et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: Systematic review and meta-analysis of randomised trials. Brit. Med. J. 2020, 368, m315. [Google Scholar] [CrossRef]
- DASH Eating Plan. National Heart, Lung, and Blood Institute; US Department of Health and Human Services. 2021. Available online: https://www.nhlbi.nih.gov/health-topics/dash-eating-plan (accessed on 7 February 2022).
- Schwingshackl, L.; Schwedhel, C.; Hoffmann, G.; Knüppel, S.; Iqbal, K.; Andriolo, V.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food Groups and Risk of Hypertension: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv Nutr. 2017, 8, 793–803, Erratum in Adv. Nutr. 2018, 9, 163–164. [Google Scholar] [CrossRef]
- Lonnie, M.; Johnstone, A.M. The public health rationale for promoting plant protein as an important part of a sustainable and healthy diet. Nutr. Bull. 2020, 45, 281–293. [Google Scholar] [CrossRef]
- De Pergola, G.; D’Alessandro, A. Influence of Mediterranean diet on blood pressure. Nutrients 2018, 10, 1700. [Google Scholar] [CrossRef]
- Filippou, C.D.; Thomopoulos, C.G.; Kouremeti, M.M.; Sotiropoulou, L.I.; Nihoyannopoulos, P.I.; Tousoulis, D.M.; Tsioufis, C.P. Mediterranean diet and blood pressure reduction in adults with and without hypertension: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2021, 40, 3191–3200. [Google Scholar] [CrossRef] [PubMed]
- Aljuraiban, G.S.; Griep, L.M.; Chan, Q.; Daviglus, M.L.; Stamler, J.; Van Horn, L.; Elliott, P.; Frost, G.S. Total, insoluble and soluble dietary fibre intake in relation to blood pressure: The INTERMAP Study. Br. J. Nutr. 2015, 114, 1480–1486. [Google Scholar] [CrossRef] [PubMed]
- Lairon, D.; Arnault, N.; Bertrais, S.; Planells, R.; Clero, E.; Hercberg, S.; Boutron-Ruault, M.C. Dietary fiber intake and risk factors for cardiovascular disease in French adults. Am. J. Clin. Nutr. 2005, 82, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Pandey, G. Biofortification of pulses and legumes to enhance nutrition. Heliyon 2020, 6, e03682. [Google Scholar] [CrossRef]
- Polak, R.; Phillips, E.M.; Campbell, A. Legumes: Health benefits and culinary approaches to increase intake. Clin. Diabetes 2015, 33, 198–205. [Google Scholar] [CrossRef]
- Willet, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Jenkins, D.J.A.; Kendall, C.W.C.; Faulkner, D.A.; Kemp, T.; Marchie, A.; Nguyen, T.H.; Wong, J.M.W.; De Souza, R.; Emam, A.; Vidgen, E.; et al. Long-term effects of a plant-based dietary portfolio of cholesterol-lowering foods on blood pressure. Eur. J. Clin. Nutr. 2008, 62, 781–788. [Google Scholar] [CrossRef]
- Sun, B.; Shi, X.; Wang, T.; Zhang, D. Exploration of the association between dietary fiber intake and hypertension among US adults using 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines: NHANES 2007–2014. Nutrients 2018, 10, 1091. [Google Scholar] [CrossRef]
- Miranda, A.M.; Steluti, J.; Fisberg, R.M.; Marchioni, D.M. Association between polyphenol intake and hypertension in adults and older adults: A population-based study in Brazil. PLoS ONE 2016, 11, e0165791. [Google Scholar] [CrossRef]
- Angeles, J.G.C.; Villanueva, J.C.; Uy, L.Y.C.; Mercado, S.M.Q.; Tsuchiya, M.C.L.; Lado, J.P.; Angelia, M.R.N.; Bercansil-Clemencia, M.C.M.; Estacio, M.A.C.; Torio, M.A.O. Legumes as functional food for cardiovascular disease. Appl. Sci. 2021, 11, 5475. [Google Scholar] [CrossRef]
- Jayalath, H.V.; de Souza, R.J.; Sievenpiper, J.L.; Ha, V.; Chiavaroli, L.; Mirrahimi, A.; Di Buono, M.; Bernstein, A.M.; Leiter, L.A.; Kris-Etherton, P.M.; et al. Effect of dietary pulses on blood pressure: A systematic review and meta-analysis of controlled feeding trials. Am. J. Hypertens. 2013, 27, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Zhang, Q.; Yin, Y.; Liu, Y.; Jiang, H.; Yan, N.; Lin, J.; Liu, X.H.; Ma, L. Legume consumption and risk of hypertension in a prospective cohort of Chinese men and women. Br. J. Nutr. 2020, 123, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Bard, D. The United Kingdom’s Pulse Renaissance. Pulse Pod. Available online: https://pulsepod.globalpulses.com/pod-feed/post/the-united-kingdom-pulse-renaissance (accessed on 4 May 2021).
- Nozue, M.; Shimazu, T.; Sasazuki, S.; Charvat, H.; Mori, N.; Mutoh, M.; Sawada, N.; Iwasaki, M.; Yamaji, T.; Inoue, M.; et al. Fermented soy product intake is inversely associated with the development of high blood pressure: The Japan Public Health Center–Based Prospective Study. J. Nutr. 2017, 147, 1749–1756. [Google Scholar] [CrossRef]
- Li, H.; Prairie, N.; Udenigwe, C.C.; Adebiyi, A.P.; Tappia, P.S.; Aukema, H.M.; Jones, P.J.; Aluko, R.E. Blood pressure lowering effect of a pea protein hydrolysate in hypertensive rats and humans. J. Agric. Food Chem. 2011, 59, 9854–9860. [Google Scholar] [CrossRef]
- Bähr, M.; Fechner, A.; Kiehntopf, M.; Jahreis, G. Consuming a mixed diet enriched with lupin protein beneficially affects plasma lipids in hypercholesterolemic subjects: A randomized controlled trial. Clin. Nutr. 2015, 34, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Day, N.; Oakes, S.; Luben, R.; Khaw, K.T.; Bingham, S.; Welch, A. EPIC-Norfolk: Study design and characteristics of the cohort. Br. J. Cancer. 1999, 80 (Suppl. 1), 95–103. [Google Scholar]
- The EPIC-Norfolk Study. MRC Epidemiology Unit. University of Cambridge. Available online: https://www.epic-norfolk.org.uk/ (accessed on 27 June 2021).
- Welch, A.A.; McTaggart, A.; Mulligan, A.A.; Luben, R.; Walker, N.; Khaw, K.T.; Day, N.E.; Bingham, S.A. DINER (Data into Nutrients for Epidemiological Research)—A new data-entry program for nutritional analysis in the EPIC–Norfolk cohort and the 7-day diary method. Public Health Nutr. 2001, 4, 1253–1265. [Google Scholar] [CrossRef]
- Lentjes, M.A.H.; McTaggart, A.; Mulligan, A.A.; Powell, N.A.; Parry-Smith, D.; Luben, R.A.; Bhaniani, A.; Welch, A.A.; Khaw, K.T. Dietary intake measurement using 7 d diet diaries in British men and women in the European Prospective Investigation into Cancer-Norfolk study: A focus on methodological issues. Br. J. Nutr. 2013, 111, 516–526. [Google Scholar] [CrossRef]
- The EPIC-Norfolk Study: Health checks & follow-ups. MRC Epidemiology Unit. University of Cambridge. Available online: https://www.epic-norfolk.org.uk/about-epic-norfolk/nutritional-methods/7ddd/ (accessed on 7 August 2022).
- Vallée, A.; Gabet, A.; Deschamps, V.; Blacher, J.; Olié, V. Relationship between nutrition and alcohol consumption with blood pressure: The ESTEBAN survey. Nutrients 2019, 11, 1433. [Google Scholar] [CrossRef]
- Your guide to lowering blood pressure. National Heart, Lung, and Blood Institute. US Department of Health and Human Services. 2003. Available online: https://www.nhlbi.nih.gov/files/docs/public/heart/hbp_low.pdf (accessed on 9 July 2021).
- Brummett, B.H.; Babyak, M.A.; Siegler, I.C.; Shanahan, M.; Harris, K.M.; Elder, G.H.; Williams, R.B. Systolic blood pressure, socioeconomic status, and biobehavioral risk factors in a nationally representative US young adult sample. Hypertension 2011, 58, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Melse-Boonstra, A.; Pan, X.; Zhao, J.; Yuan, B.; Dai, Y.; Zhou, M.; Geleijnse, J.M.; Kok, F.J.; Shi, Z. Association of dietary pattern and body weight with blood pressure in Jiangsu Province, China. BMC Public Health 2014, 14, 948. [Google Scholar] [CrossRef] [PubMed]
- Myint, P.K.; Luben, R.N.; Wareham, N.J.; Welch, A.A.; Bingham, S.A.; Day, N.E.; Khaw, K.T. Combined work and leisure physical activity and risk of stroke in men and women in the European Prospective Investigation into Cancer-Norfolk Prospective Population study. Neuroepidemiology 2006, 27, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Townsend, P.; Davidson, N.; Whitehead, M. (Eds.) The Black Report. Inequalities in Health; Penguin: London, UK, 1988. [Google Scholar]
- Wiinberg, N.; Høegholm, A.; Christensen, H.R.; Bang, L.E.; Mikkelsen, K.L.; Nielsen, P.E.; Svendsen, T.L.; Kampmann, J.P.; Madsen, N.H.; Bentzon, M.W. 24-h ambulatory blood pressure in 352 normal Danish subjects, related to age and gender. Am. J. Hypertens. 1995, 8, 978–986. [Google Scholar] [CrossRef]
- Malaguti, M.; Dinelli, G.; Leoncini, E.; Bregola, V.; Bosi, S.; Cicero, A.F.; Hrelia, S. Bioactive peptides in cereals and legumes: Agronomical, biochemical and clinical aspects. Int. J. Mol. Sci. 2014, 15, 21120–21135. [Google Scholar] [CrossRef] [PubMed]
- de Freitas, M.A.G.; Amaral, N.O.; Álvares, A.D.C.M.; de Oliveira, S.A.; Mehdad, A.; Honda, D.E.; Bessa, A.S.M.; Ramada, M.H.S.; Naves, L.M.; Pontes, C.N.R.; et al. Blood pressure-lowering effects of a Bowman-Birk inhibitor and its derived peptides in normotensive and hypertensive rats. Sci. Rep. 2020, 10, 11680. [Google Scholar] [CrossRef]
- The National Diet and Nutrition Survey. United Kingdom Office for National Statistics. 2013. Available online: https://data.gov.uk/dataset/4f78ff58-86ec-47cc-b386-dafa9aa30cf8/the-national-diet-and-nutrition-survey (accessed on 9 July 2021).
- Macdiarmid, J.I. The food system and climate change: Are plant-based diets becoming unhealthy and less environmentally sustainable? Proc. Nutr. Soc. 2021, 81, 162–167. [Google Scholar] [CrossRef]
- Curtain, F.; Grafenauer, S. Plant-based meat substitutes in the flexitarian age: An audit of products on supermarket shelves. Nutrients 2019, 11, 2603. [Google Scholar] [CrossRef]
- Geraldo, R.; Santos, C.S.; Pinto, E.; Vasconcelos, M.W. Widening the perspectives for legume consumption: The case of bioactive non-nutrients. Front. Plant Sci. 2022, 56, 772054. [Google Scholar] [CrossRef]
- Day, N.E.; McKeown, N.; Wong, M.Y.; Welch, A.; Bingham, S. Epidemiological assessment of diet: A comparison of a 7-day diary with a food frequency questionnaire using urinary markers of nitrogen, potassium and sodium. Int. J. Epidemiol. 2001, 30, 309–317. [Google Scholar] [CrossRef]
| All (n = 7522) | Men (n = 3492) | Women (n = 4030) | p | |
|---|---|---|---|---|
| Mean (SD) | ||||
| Age at entry (years) | 58.0 (8.9) | 58.7 (8.9) | 57.4 (8.8) | <0.001 |
| BMI (kg/m2) | 26.0 (3.7) | 26.4 (3.2) | 25.7 (4.1) | <0.001 |
| Legume intake (g/day) | 17.3 (16.3) | 20.0 (18.6) | 14.9 (13.6) | <0.001 |
| Energy intake (kJ/day) | 8505 (2144) | 9770 (2031) | 7409 (1553) | <0.001 |
| Alcohol intake (g/day) | 12.3 (17.0) | 17.1 (20.8) | 8.1 (11.3) | <0.001 |
| Protein intake (g/day) | 75.3 (17.5) | 84.7 (17.0) | 67.2 (13.4) | <0.001 |
| Sodium intake (mg/day) | 2924 (844) | 3359 (845) | 2546 (636) | <0.001 |
| Fruit and vegetable intake (g/day) | 333 (162) | 320 (158) | 343 (164) | <0.001 |
| Red meat intake (g/day) | 33.2 (26.7) | 39.7 (29.4) | 27.6 (22.7) | <0.001 |
| Systolic blood pressure (mmHg) | 134.5 (17.8) | 136.8 (16.9) | 132.4 (18.3) | <0.001 |
| Diastolic blood pressure (mmHg) | 82.2 (11.1) | 84.3 (10.9) | 80.4 (1.0) | <0.001 |
| Townsend Deprivation Index (index) | −2.15 (2.0) | −2.19 (2.1) | −2.12 (2.1) | 0.144 |
| Number (%) | ||||
| Self-reported high blood pressure | 942 (12.5) | 457 (13.1) | 485 (12.0) | 0.173 |
| Smoking status at baseline | <0.001 | |||
| Current smoker | 697 (9.3) | 338 (9.7) | 359 (8.9) | |
| Former smoked | 3166 (42.1) | 1902 (54.5) | 1264 (31.4) | |
| Never smoked | 3659 (48.6) | 1252 (35.8) | 2407 (59.7) | |
| Physical Activity Level at baseline: | <0.001 | |||
| Inactive | 1933 (25.7) | 923 (26.4) | 1010 (25.1) | |
| Moderately inactive | 2199 (29.2) | 884 (25.3) | 1315 (32.6) | |
| Moderately active | 1832 (24.4) | 857 (24.5) | 975 (24.2) | |
| Active | 1558 (20.7) | 828 (23.7) | 730 (18.1) | |
| Education level: | <0.001 | |||
| No education | 2492 (33.1) | 954 (27.3) | 1538 (38.1) | |
| GCSE/O Level | 823 (10.9) | 308 (8.8) | 515 (12.8) | |
| A-Level | 3176 (42.3) | 1670 (47.8) | 1506 (37.4) | |
| Degree or higher | 1031 (13.7) | 560 (16.0) | 471 (11.7) | |
| Social class by occupation: | <0.001 | |||
| Unknown | 52 (0.7) | 25 (0.7) | 27 (0.7) | |
| Professional | 349 (4.6) | 277 (7.9) | 72 (1.8) | |
| Manager | 2504 (33.3) | 1365 (39.1) | 1139 (28.3) | |
| Skilled non-manual | 2058 (27.4) | 432 (12.4) | 1626 (40.3) | |
| Skilled manual | 1109 (14.7) | 856 (24.5) | 253 (6.2) | |
| Semi-skilled | 1127 (14.9) | 459 (13.1) | 668 (16.6) | |
| Non-skilled | 323 (4.3) | 78 (2.2) | 245 (6.1) | |
| Percentile (g/day) | Unadjusted Model | Model A | Model B | Model C | Model D | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| 3rd (1.84) | 1.47 ** | 1.12, 1.91 | 1.34 * | 1.02, 1.77 | 1.33 * | 1.01, 1.76 | 1.34 * | 1.01, 1.77 | 1.36 * | 1.03, 1.80 |
| 5th (3.15) | 1.43 *** | 1.16, 1.77 | 1.33 * | 1.07, 1.65 | 1.32 * | 1.06, 1.65 | 1.34 ** | 1.08, 1.68 | 1.37 ** | 1.10, 1.71 |
| 10th (4.14) | 1.11 | 0.96, 1.29 | 1.02 | 0.88, 1.20 | 1.04 | 0.88, 1.21 | 1.04 | 0.89, 1.22 | 1.05 | 0.90, 1.24 |
| 50th (13.8) | 0.96 | 0.87, 1.05 | 1.02 | 0.92, 1.12 | 1.00 | 0.91, 1.11 | 1.01 | 0.91, 1.12 | 1.00 | 0.90, 1.10 |
| 90th (33.9) | 0.84 * | 0.72, 0.99 | 0.956 | 0.81, 1.12 | 0.95 | 0.80, 1.12 | 0.95 | 0.80, 1.12 | 0.93 | 0.79, 1.10 |
| 95th (45.2) | 0.83 | 0.67, 1.04 | 0.94 | 0.75, 1.18 | 0.92 | 0.73, 1.16 | 0.94 | 0.75, 1.19 | 0.93 | 0.74, 1.17 |
| 97th (56.6) | 0.65 ** | 0.49, 0.87 | 0.72 * | 0.54, 0.97 | 0.69 * | 0.52, 0.94 | 0.72 * | 0.53, 0.97 | 0.71 * | 0.52, 0.96 |
| Men | ||||||||||
| 3rd (2.55) | 1.66 * | 1.12, 2.47 | 1.53 * | 1.01, 2.30 | 1.43 | 0.94, 2.16 | 1.38 | 0.91, 2.09 | 1.42 | 0.94, 2.17 |
| 5th (3.49) | 1.26 | 0.93, 1.70 | 1.15 | 0.84, 1.57 | 1.08 | 0.79, 1.49 | 1.06 | 0.77, 1.46 | 1.09 | 0.79, 1.51 |
| 10th (5.23) | 1.16 | 0.93, 1.45 | 1.07 | 0.85, 1.35 | 1.04 | 0.82, 1.31 | 1.03 | 0.81, 1.30 | 1.06 | 0.83, 1.34 |
| 50th (14.9) | 0.92 | 0.80, 1.05 | 0.96 | 0.83, 1.10 | 0.97 | 0.84, 1.12 | 0.98 | 0.85, 1.13 | 0.96 | 0.84, 1.11 |
| 90th (39.5) | 0.79* | 0.63, 0.99 | 0.89 | 0.71, 1.12 | 0.91 | 0.72, 1.16 | 0.93 | 0.74, 1.19 | 0.91 | 0.72, 1.16 |
| 95th (54.6) | 0.69* | 0.50, 0.94 | 0.76 | 0.55, 1.06 | 0.78 | 0.56, 1.09 | 0.82 | 0.58, 1.14 | 0.80 | 0.57, 1.12 |
| 97th (66.2) | 0.81 | 0.54, 1.21 | 0.90 | 0.60, 1.35 | 0.94 | 0.62, 1.43 | 1.00 | 0.66, 1.53 | 0.98 | 0.65, 1.50 |
| Women | ||||||||||
| 3rd (1.84) | 1.52 * | 1.09, 2.12 | 1.31 | 0.92, 1.87 | 1.31 | 0.92, 1.86 | 1.35 | 0.95, 1.93 | 1.36 | 0.95, 1.95 |
| 5th (2.75) | 1.62 *** | 1.23, 2.15 | 1.51 ** | 1.13, 2.03 | 1.50 ** | 1.12, 2.02 | 1.55 ** | 1.15, 2.10 | 1.58 ** | 1.17, 2.13 |
| 10th (3.67) | 1.09 | 0.90, 1.34 | 1.02 | 0.83, 1.27 | 1.02 | 0.82, 1.26 | 1.04 | 0.84, 1.29 | 1.05 | 0.84, 1.30 |
| 50th (11.4) | 0.88 * | 0.77, 0.99 | 0.97 | 0.85, 1.12 | 0.98 | 0.85, 1.13 | 0.99 | 0.86, 1.14 | 0.99 | 0.86, 1.14 |
| 90th (30.2) | 0.83 | 0.66, 1.03 | 0.93 | 0.74, 1.18 | 0.95 | 0.75, 1.20 | 0.97 | 0.76, 1.23 | 0.97 | 0.77, 1.24 |
| 95th (38.3) | 0.61 ** | 0.44, 0.85 | 0.73 | 0.52, 1.03 | 0.74 | 0.53, 1.05 | 0.75 | 0.53, 1.06 | 0.75 | 0.53, 1.07 |
| 97th (44.8) | 0.58 * | 0.38, 0.88 | 0.70 | 0.45, 1.08 | 0.70 | 0.46, 1.10 | 0.73 | 0.46, 1.14 | 0.73 | 0.47, 1.14 |
| Legume Intake (g/day) | All (n = 7522) | Men (n = 3492) | Women (n = 4030) | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| >46 | 0.95 | 0.75, 1.21 | 0.99 | 0.75, 1.32 | 0.76 | 0.48, 1.20 |
| >47 | 0.96 | 0.75, 1.23 | 0.99 | 0.74, 1.33 | 0.79 | 0.50, 1.25 |
| >48 | 0.92 | 0.72, 1.19 | 0.97 | 0.72, 1.30 | 0.73 | 0.45, 1.18 |
| >49 | 0.90 | 0.70, 1.16 | 0.96 | 0.71, 1.30 | 0.63 | 0.37, 1.07 |
| >50 | 0.90 | 0.69, 1.17 | 0.96 | 0.70, 1.31 | 0.63 | 0.37, 1.09 |
| >51 | 0.89 | 0.68, 1.16 | 0.93 | 0.68, 1.28 | 0.63 | 0.36, 1.10 |
| >52 | 0.84 | 0.64, 1.11 | 0.88 | 0.64, 1.22 | 0.61 | 0.35, 1.09 |
| >53 | 0.80 | 0.61, 1.07 | 0.86 | 0.62, 1.19 | 0.55 | 0.30, 1.02 |
| >54 | 0.74 * | 0.55, 0.99 | 0.83 | 0.60, 1.16 | 0.37 ** | 0.18, 0.75 |
| >55 | 0.72 * | 0.54, 0.97 | 0.79 | 0.56, 1.11 | 0.40 * | 0.20, 0.82 |
| >56 | 0.70 * | 0.52, 0.94 | 0.76 | 0.54, 1.07 | 0.40 * | 0.20, 0.82 |
| >57 | 0.73 * | 0.54, 0.99 | 0.79 | 0.56, 1.12 | 0.43 * | 0.21, 0.87 |
| >58 | 0.79 | 0.58, 1.09 | 0.84 | 0.59, 1.21 | 0.48 * | 0.24, 1.00 |
| >59 | 0.79 | 0.57, 1.08 | 0.86 | 0.60, 1.24 | 0.44 * | 0.21, 0.94 |
| >60 | 0.77 | 0.56, 1.08 | 0.83 | 0.57, 1.21 | 0.47 | 0.22, 1.02 |
| >61 | 0.82 | 0.58, 1.15 | 0.88 | 0.60, 1.30 | 0.50 | 0.24, 1.08 |
| >62 | 0.82 | 0.58, 1.16 | 0.91 | 0.62, 1.34 | 0.45 * | 0.20, 0.99 |
| >63 | 0.86 | 0.60, 1.22 | 0.98 | 0.66, 1.47 | 0.41 * | 0.18, 0.95 |
| >64 | 0.87 | 0.61, 1.23 | 0.97 | 0.65, 1.46 | 0.44 | 0.19, 1.02 |
| >65 | 0.88 | 0.62, 1,27 | 1.01 | 0.67, 1.53 | 0.41 | 0.17, 1.01 |
| >66 | 0.89 | 0.61, 1.28 | 1.01 | 0.67, 1.54 | 0.42 | 0.17, 1.03 |
| Legume Intake (g/day) | All (n = 7522) | Men (n = 3492) | Women (n = 4030) | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| 10–24.9 | 0.90 | 0.89, 1.11 | 0.98 | 0.83, 1.16 | 0.97 | 0.84, 1.13 |
| 25–39.9 | 1.08 | 0.92, 1.27 | 0.94 | 0.75, 1.17 | 1.23 | 0.96, 1.56 |
| 40–54.9 | 1.01 | 0.78, 1.32 | 1.00 | 0.71, 1.41 | 0.92 | 0.60, 1.42 |
| 55–69.9 | 0.57 * | 0.37, 0.88 | 0.64 | 0.38, 1.03 | 0.32 * | 0.12, 0.88 |
| 70–84.9 | 0.70 | 0.34, 1.46 | 0.58 | 0.26, 1.31 | 0.87 | 0.17, 4.53 |
| 85–99.9 | 1.29 | 0.64, 2.60 | 1.32 | 0.59, 2.93 | 0.95 | 0.18, 4.94 |
| >100 | 0.89 | 0.44, 1.78 | 1.12 | 0.51, 2.47 | 0.18 | 0.02, 1.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hartley, M.; Fyfe, C.L.; Wareham, N.J.; Khaw, K.-T.; Johnstone, A.M.; Myint, P.K. Association between Legume Consumption and Risk of Hypertension in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk Cohort. Nutrients 2022, 14, 3363. https://doi.org/10.3390/nu14163363
Hartley M, Fyfe CL, Wareham NJ, Khaw K-T, Johnstone AM, Myint PK. Association between Legume Consumption and Risk of Hypertension in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk Cohort. Nutrients. 2022; 14(16):3363. https://doi.org/10.3390/nu14163363
Chicago/Turabian StyleHartley, Michael, Claire L. Fyfe, Nicholas J. Wareham, Kay-Tee Khaw, Alexandra M. Johnstone, and Phyo K. Myint. 2022. "Association between Legume Consumption and Risk of Hypertension in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk Cohort" Nutrients 14, no. 16: 3363. https://doi.org/10.3390/nu14163363
APA StyleHartley, M., Fyfe, C. L., Wareham, N. J., Khaw, K.-T., Johnstone, A. M., & Myint, P. K. (2022). Association between Legume Consumption and Risk of Hypertension in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk Cohort. Nutrients, 14(16), 3363. https://doi.org/10.3390/nu14163363