
Dyslipidemia Increases the Risk of Incident Hypertension in a Large Taiwanese Population Follow-Up Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. The Taiwan Biobank (TWB)
2.2. Laboratory, Medical, and Demographic Variables
2.3. Definition of Baseline and Incident Hypertension
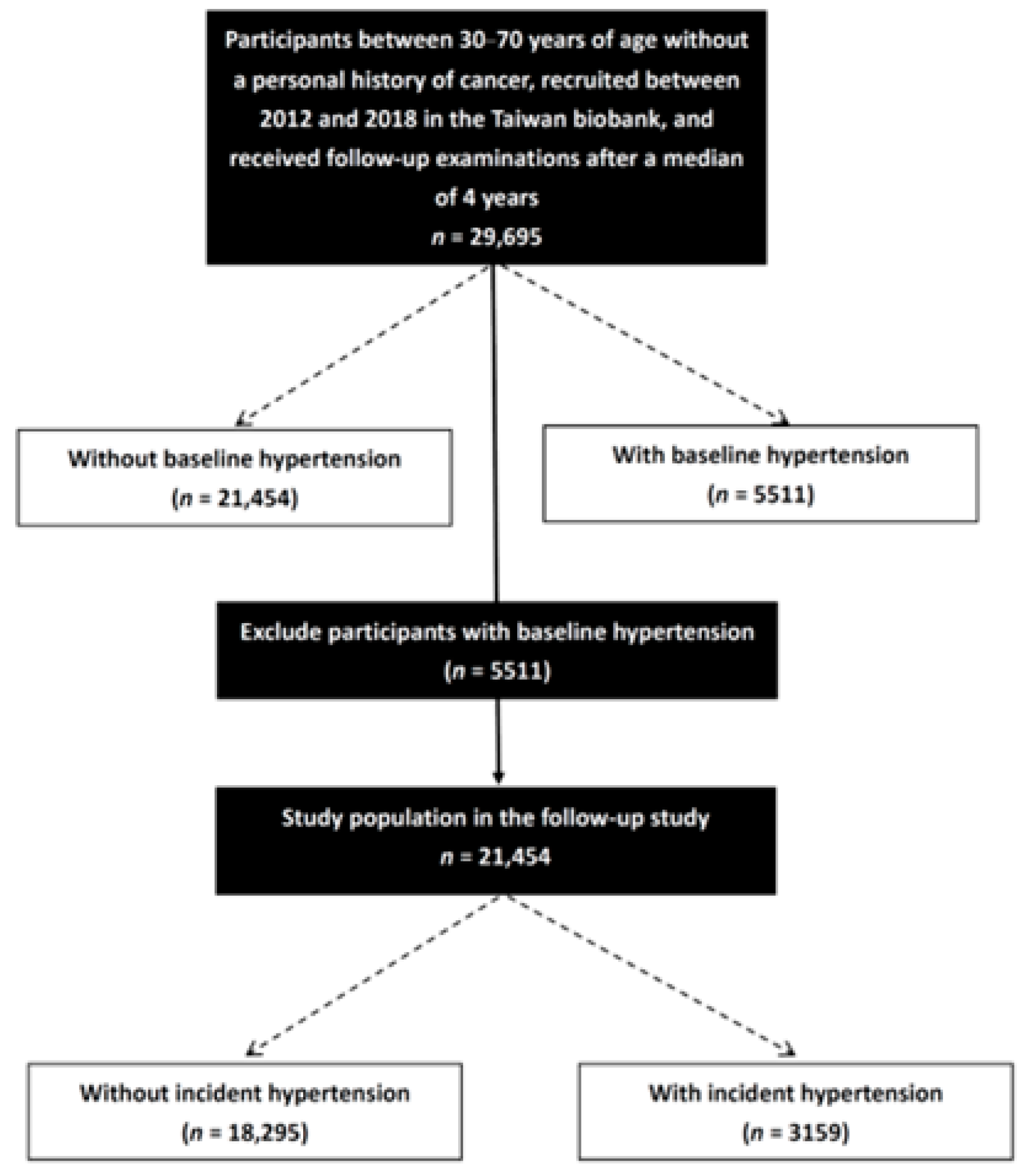
2.4. Study Participants
2.5. Statistical Analysis
3. Results
3.1. Comparisons of Clinical Characteristics between Baseline Hypertension Groups
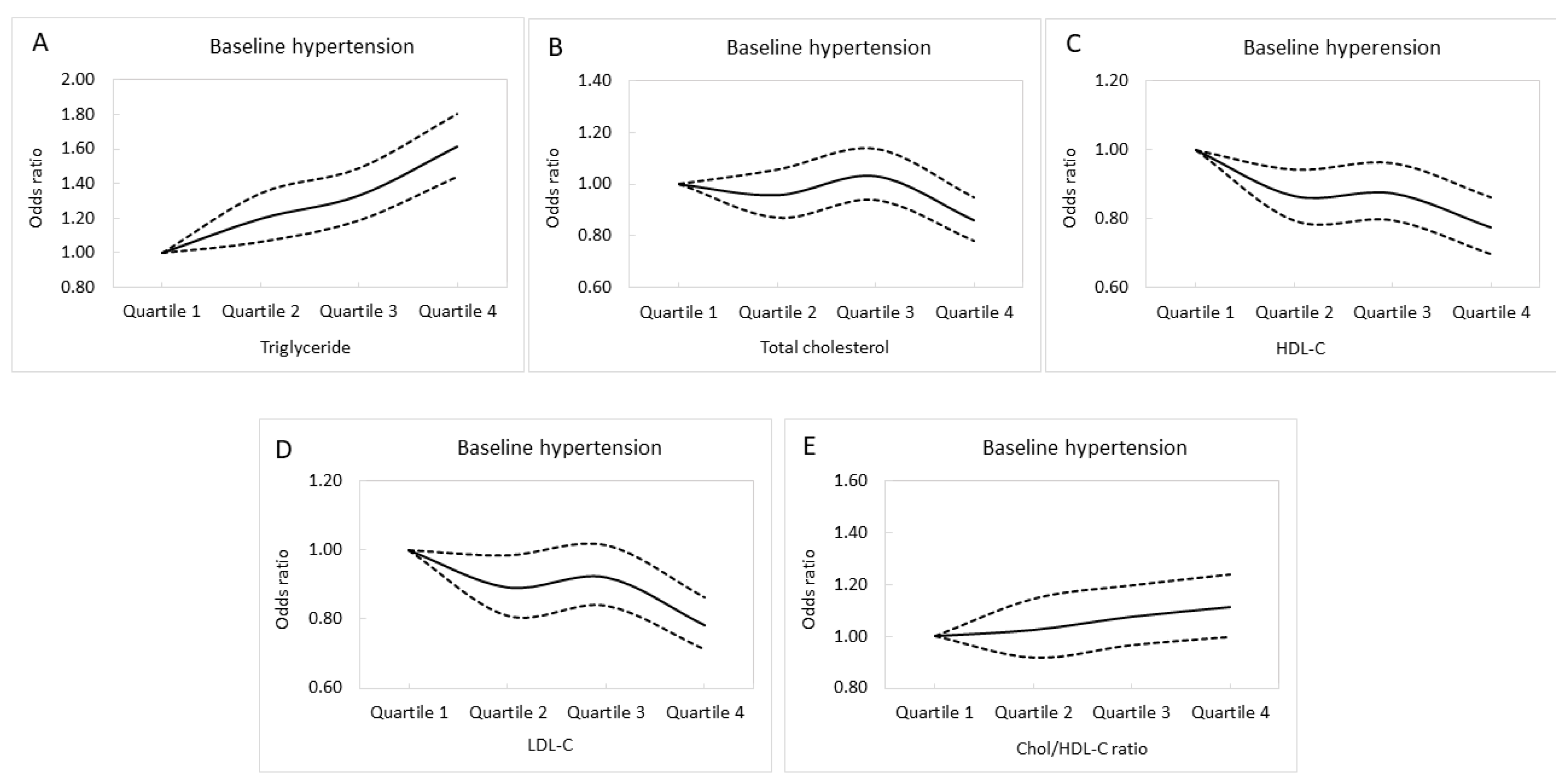
3.2. Associations between Lipid Profile Quartiles and Baseline Hypertension
3.3. Comparisons of Clinical Characteristics between Those with and without Incident Hypertension
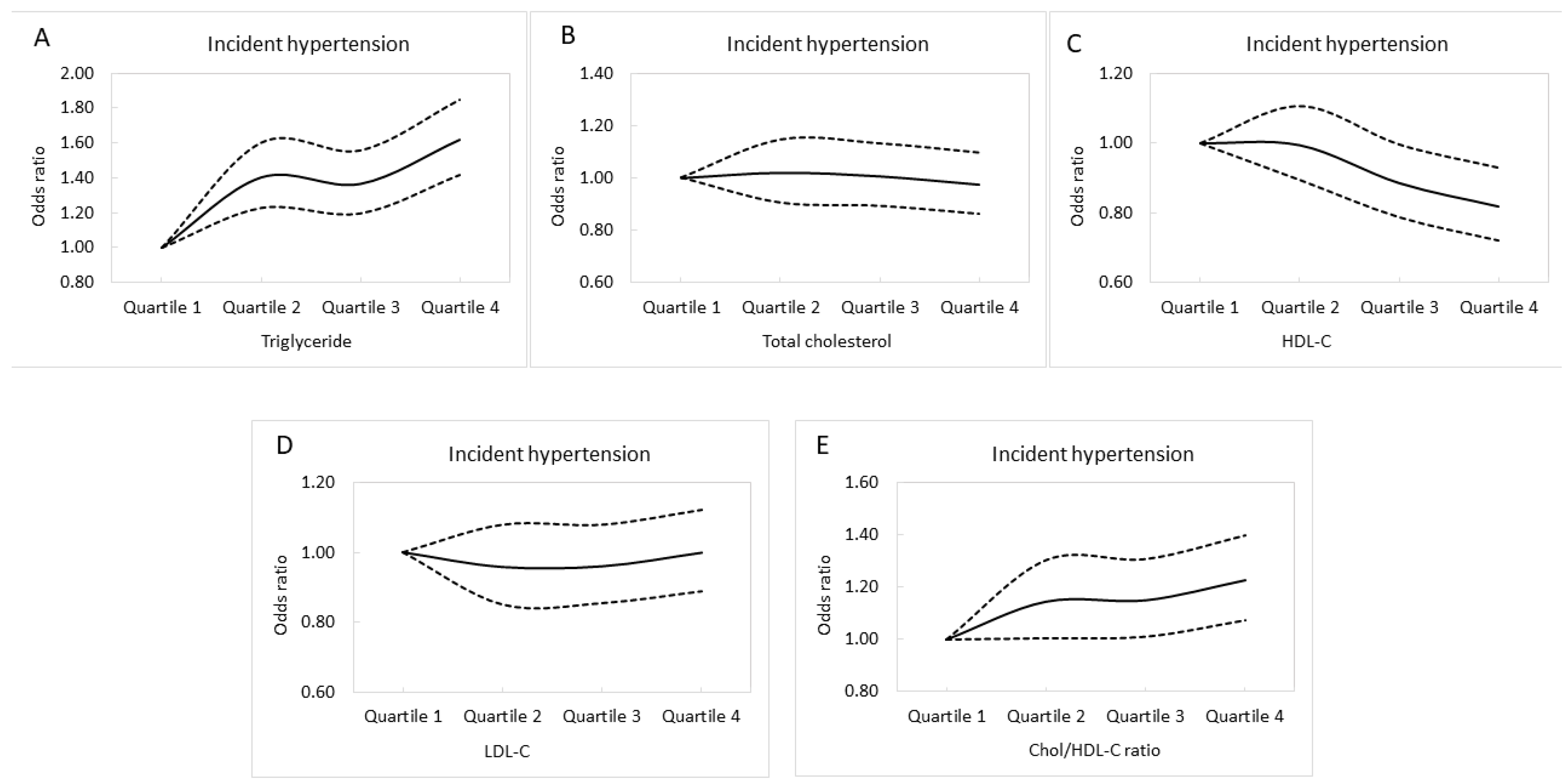
3.4. Associations between Lipid Profile Quartiles and Incident Hypertension
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Su, T.C.; Bai, C.H.; Chang, H.Y.; You, S.L.; Chien, K.L.; Chen, M.F.; Chen, H.J.; Pan, W.H.; Tseng, C.H.; Cheng, S.H.; et al. Evidence for improved control of hypertension in Taiwan: 1993–2002. J. Hypertens. 2008, 26, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Saxena, T.; Ali, A.O.; Saxena, M. Pathophysiology of essential hypertension: An update. Expert Rev. Cardiovasc. Ther. 2018, 16, 879–887. [Google Scholar] [CrossRef]
- Vokonas, P.S.; Kannel, W.B.; Cupples, L.A. Epidemiology and risk of hypertension in the elderly: The Framingham Study. J. Hypertens. Suppl. 1988, 6, S3–S9. [Google Scholar]
- Forman, J.P.; Stampfer, M.J.; Curhan, G.C. Diet and lifestyle risk factors associated with incident hypertension in women. JAMA 2009, 302, 401–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, N.Y.; Young, J.H.; Meoni, L.A.; Ford, D.E.; Erlinger, T.P.; Klag, M.J. Blood pressure change and risk of hypertension associated with parental hypertension: The Johns Hopkins Precursors Study. Arch. Intern. Med. 2008, 168, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Carson, A.P.; Howard, G.; Burke, G.L.; Shea, S.; Levitan, E.B.; Muntner, P. Ethnic differences in hypertension incidence among middle-aged and older adults: The multi-ethnic study of atherosclerosis. Hypertension 2011, 57, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Keller, G.; Zimmer, G.; Mall, G.; Ritz, E.; Amann, K. Nephron number in patients with primary hypertension. N. Engl. J. Med. 2003, 348, 101–108. [Google Scholar] [CrossRef]
- Appel, L.J.; Brands, M.W.; Daniels, S.R.; Karanja, N.; Elmer, P.J.; Sacks, F.M. Dietary approaches to prevent and treat hypertension: A scientific statement from the American Heart Association. Hypertension 2006, 47, 296–308. [Google Scholar] [CrossRef] [Green Version]
- Carnethon, M.R.; Evans, N.S.; Church, T.S.; Lewis, C.E.; Schreiner, P.J.; Jacobs, D.R., Jr.; Sternfeld, B.; Sidney, S. Joint associations of physical activity and aerobic fitness on the development of incident hypertension: Coronary artery risk development in young adults. Hypertension 2010, 56, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Lawlor, D.A.; Nordestgaard, B.G.; Benn, M.; Zuccolo, L.; Tybjaerg-Hansen, A.; Davey Smith, G. Exploring causal associations between alcohol and coronary heart disease risk factors: Findings from a Mendelian randomization study in the Copenhagen General Population Study. Eur. Heart J. 2013, 34, 2519–2528. [Google Scholar] [CrossRef] [Green Version]
- Zhou, B.; Perel, P.; Mensah, G.A.; Ezzati, M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat. Rev. Cardiol. 2021, 18, 785–802. [Google Scholar] [CrossRef]
- Lawes, C.M.; Vander Hoorn, S.; Rodgers, A. Global burden of blood-pressure-related disease, 2001. Lancet 2008, 371, 1513–1518. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Pirillo, A.; Casula, M.; Olmastroni, E.; Norata, G.D.; Catapano, A.L. Global epidemiology of dyslipidaemias. Nat. Rev. Cardiol. 2021, 18, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Wong, N.D. Epidemiological studies of CHD and the evolution of preventive cardiology. Nat. Rev. Cardiol. 2014, 11, 276–289. [Google Scholar] [CrossRef]
- Ference, B.A.; Ginsberg, H.N.; Graham, I.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef] [Green Version]
- Yaghi, S.; Elkind, M.S. Lipids and Cerebrovascular Disease: Research and Practice. Stroke 2015, 46, 3322–3328. [Google Scholar] [CrossRef] [Green Version]
- Bønaa, K.H.; Thelle, D.S. Association between blood pressure and serum lipids in a population. The Tromsø Study. Circulation 1991, 83, 1305–1314. [Google Scholar] [CrossRef] [Green Version]
- Selwyn, A.P.; Kinlay, S.; Libby, P.; Ganz, P. Atherogenic lipids, vascular dysfunction, and clinical signs of ischemic heart disease. Circulation 1997, 95, 5–7. [Google Scholar] [CrossRef]
- Urbina, E.M.; Srinivasan, S.R.; Kieltyka, R.L.; Tang, R.; Bond, M.G.; Chen, W.; Berenson, G.S. Correlates of carotid artery stiffness in young adults: The Bogalusa Heart Study. Atherosclerosis 2004, 176, 157–164. [Google Scholar] [CrossRef]
- Otsuka, T.; Takada, H.; Nishiyama, Y.; Kodani, E.; Saiki, Y.; Kato, K.; Kawada, T. Dyslipidemia and the Risk of Developing Hypertension in a Working-Age Male Population. J. Am. Heart Assoc. 2016, 5, e003053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiss, A.B.; Voloshyna, I.; De Leon, J.; Miyawaki, N.; Mattana, J. Cholesterol Metabolism in CKD. Am. J. Kidney Dis. 2015, 66, 1071–1082. [Google Scholar] [CrossRef] [Green Version]
- Freitas, M.P.; Loyola Filho, A.I.; Lima-Costa, M.F. Dyslipidemia and the risk of incident hypertension in a population of community-dwelling Brazilian elderly: The Bambuí Cohort Study of Aging. Cad. Saude Publica 2011, 27 (Suppl. S3), S351–S359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.H.; Yang, J.H.; Chiang, C.W.K.; Hsiung, C.N.; Wu, P.E.; Chang, L.C.; Chu, H.W.; Chang, J.; Song, I.W.; Yang, S.L.; et al. Population structure of Han Chinese in the modern Taiwanese population based on 10,000 participants in the Taiwan Biobank project. Hum. Mol. Genet 2016, 25, 5321–5331. [Google Scholar] [CrossRef] [Green Version]
- Fan, C.T.; Hung, T.H.; Yeh, C.K. Taiwan Regulation of Biobanks. J. Law Med. Ethics 2015, 43, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Yang, Z.; Wang, S.; Sun, F.; Zhan, S. The associations of metabolic syndrome with incident hypertension, type 2 diabetes mellitus and chronic kidney disease: A cohort study. Endocrine 2018, 60, 282–291. [Google Scholar] [CrossRef]
- Laaksonen, D.E.; Niskanen, L.; Nyyssönen, K.; Lakka, T.A.; Laukkanen, J.A.; Salonen, J.T. Dyslipidaemia as a predictor of hypertension in middle-aged men. Eur. Heart J. 2008, 29, 2561–2568. [Google Scholar] [CrossRef]
- Paynter, N.P.; Sesso, H.D.; Conen, D.; Otvos, J.D.; Mora, S. Lipoprotein subclass abnormalities and incident hypertension in initially healthy women. Clin. Chem. 2011, 57, 1178–1187. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Íñigo, L.; Navarro-González, D.; Pastrana-Delgado, J.; Fernández-Montero, A.; Martínez, J.A. Association of triglycerides and new lipid markers with the incidence of hypertension in a Spanish cohort. J. Hypertens. 2016, 34, 1257–1265. [Google Scholar] [CrossRef]
- Tohidi, M.; Hatami, M.; Hadaegh, F.; Azizi, F. Triglycerides and triglycerides to high-density lipoprotein cholesterol ratio are strong predictors of incident hypertension in Middle Eastern women. J. Hum. Hypertens. 2012, 26, 525–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kume, N.; Kita, T. Apoptosis of vascular cells by oxidized LDL: Involvement of caspases and LOX-1 and its implication in atherosclerotic plaque rupture. Circ. Res. 2004, 94, 269–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mogane, C.; Mokotedi, L.P.; Millen, A.M.E.; Michel, F.S. Increased systolic blood pressure associated with hypertriglyceridemia in female Sprague-Dawley rats. Can. J. Physiol. Pharmacol. 2019, 97, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Goto, K.; Ohtsubo, T.; Kitazono, T. Endothelium-Dependent Hyperpolarization (EDH) in Hypertension: The Role of Endothelial Ion Channels. Int. J. Mol. Sci. 2018, 19, 315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Kreutzenberg, S.V.; Puato, M.; Kiwanuka, E.; Del Prato, S.; Pauletto, P.; Pasini, L.; Tiengo, A.; Avogaro, A. Elevated non-esterified fatty acids impair nitric oxide independent vasodilation, in humans: Evidence for a role of inwardly rectifying potassium channels. Atherosclerosis 2003, 169, 147–153. [Google Scholar] [CrossRef]
- Sang, Y.; Cao, M.; Wu, X.; Ruan, L.; Zhang, C. Use of lipid parameters to identify apparently healthy men at high risk of arterial stiffness progression. BMC Cardiovasc. Disord 2021, 21, 34. [Google Scholar] [CrossRef]
- Keech, A.; Simes, R.J.; Barter, P.; Best, J.; Scott, R.; Taskinen, M.R.; Forder, P.; Pillai, A.; Davis, T.; Glasziou, P.; et al. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): Randomised controlled trial. Lancet 2005, 366, 1849–1861. [Google Scholar] [CrossRef]
- Kim, J.I.; Tsujino, T.; Fujioka, Y.; Saito, K.; Yokoyama, M. Bezafibrate improves hypertension and insulin sensitivity in humans. Hypertens. Res. 2003, 26, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Koh, K.K.; Quon, M.J.; Han, S.H.; Chung, W.J.; Ahn, J.Y.; Kim, J.A.; Lee, Y.; Shin, E.K. Additive beneficial effects of fenofibrate combined with candesartan in the treatment of hypertriglyceridemic hypertensive patients. Diabetes Care 2006, 29, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Jonkers, I.J.; de Man, F.H.; van der Laarse, A.; Frölich, M.; Gevers Leuven, J.A.; Kamper, A.M.; Blauw, G.J.; Smelt, A.H. Bezafibrate reduces heart rate and blood pressure in patients with hypertriglyceridemia. J. Hypertens. 2001, 19, 749–755. [Google Scholar] [CrossRef]
- He, D.; Fan, F.; Jia, J.; Jiang, Y.; Sun, P.; Wu, Z.; Li, J.; Huo, Y.; Zhang, Y. Lipid profiles and the risk of new-onset hypertension in a Chinese community-based cohort. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Casino, P.R.; Kilcoyne, C.M.; Quyyumi, A.A.; Hoeg, J.M.; Panza, J.A. The role of nitric oxide in endothelium-dependent vasodilation of hypercholesterolemic patients. Circulation 1993, 88, 2541–2547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gimbrone, M.A., Jr.; García-Cardeña, G. Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef] [Green Version]
- Triantafyllidi, H.; Benas, D.; Vlachos, S.; Vlastos, D.; Pavlidis, G.; Schoinas, A.; Varoudi, M.; Birmpa, D.; Moutsatsou, P.; Lekakis, J.; et al. HDL cholesterol levels and endothelial glycocalyx integrity in treated hypertensive patients. J. Clin. Hypertens. 2018, 20, 1615–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemieux, I.; Lamarche, B.; Couillard, C.; Pascot, A.; Cantin, B.; Bergeron, J.; Dagenais, G.R.; Després, J.P. Total cholesterol/HDL cholesterol ratio vs LDL cholesterol/HDL cholesterol ratio as indices of ischemic heart disease risk in men: The Quebec Cardiovascular Study. Arch. Intern. Med. 2001, 161, 2685–2692. [Google Scholar] [CrossRef]
- Wang, F.; Han, L.; Hu, D. Fasting insulin, insulin resistance and risk of hypertension in the general population: A meta-analysis. Clin. Chim. Acta 2017, 464, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Calling, S.; Johansson, S.E.; Wolff, M.; Sundquist, J.; Sundquist, K. Total cholesterol/HDL-C ratio versus non-HDL-C as predictors for ischemic heart disease: A 17-year follow-up study of women in southern Sweden. BMC Cardiovasc. Disord. 2021, 21, 163. [Google Scholar] [CrossRef]
- Cho, K.H.; Park, H.J.; Kim, J.R. Decrease in Serum HDL-C Level Is Associated with Elevation of Blood Pressure: Correlation Analysis from the Korean National Health and Nutrition Examination Survey 2017. Int. J. Environ. Res. Public Health 2020, 17, 1101. [Google Scholar] [CrossRef] [Green Version]
- Wen, J.; Huang, Y.; Lu, Y.; Yuan, H. Associations of non-high-density lipoprotein cholesterol, triglycerides and the total cholesterol/HDL-c ratio with arterial stiffness independent of low-density lipoprotein cholesterol in a Chinese population. Hypertens. Res. 2019, 42, 1223–1230. [Google Scholar] [CrossRef] [Green Version]
- Safar, M.E. Arterial stiffness as a risk factor for clinical hypertension. Nat. Rev. Cardiol. 2018, 15, 97–105. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Baseline Hypertension (−) (n = 21,454) | Baseline Hypertension (+) (n = 5511) | p |
|---|---|---|---|
| Age (years) | 49.7 ± 10.3 | 57.2 ± 8.3 | <0.001 |
| Male sex (%) | 32.2 | 48.0 | <0.001 |
| DM (%) | 3.5 | 12.2 | <0.001 |
| Smoking history (%) | 23.9 | 32.2 | <0.001 |
| Alcohol history (%) | 2.7 | 3.6 | 0.001 |
| Regular exercise (%) | 46.1 | 56.6 | <0.001 |
| Systolic BP (mmHg) | 112.0 ± 13.0 | 139.3 ± 16.5 | <0.001 |
| Diastolic BP (mmHg) | 69.8 ± 9.0 | 83.0 ± 11.0 | <0.001 |
| Body mass index (kg/m2) | 23.6 ± 3.4 | 25.9 ± 3.7 | <0.001 |
| Laboratory parameters | |||
| Fasting glucose (mg/dL) | 94.5 ± 18.7 | 102.8 ± 24.6 | <0.001 |
| Hemoglobin (g/dL) | 13.6 ± 1.6 | 14.2 ± 1.5 | <0.001 |
| Triglyceride (mg/dL) | 107.9 ± 79.9 | 137.7 ± 90.5 | <0.001 |
| Total cholesterol (mg/dL) | 195.1 ± 35.3 | 196.9 ± 35.6 | <0.001 |
| HDL-C (mg/dL) | 55.2 ± 13.2 | 50.5 ± 12.4 | <0.001 |
| LDL-C (mg/dL) | 121.3 ± 31.6 | 122.8 ± 31.5 | 0.002 |
| Chol/HDL-C ratio | 3.70 ± 1.01 | 4.07 ± 1.02 | <0.001 |
| eGFR (mL/min/1.73 m2) | 111.1 ± 24.9 | 101.5 ± 25.7 | <0.001 |
| Uric acid (mg/dL) | 5.3 ± 1.4 | 6.0 ± 1.5 | <0.001 |
| Lipid Profile Quartile | Univariable (Baseline Hypertension) | Multivariable (Baseline Hypertension) | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| Triglyceride | ||||
| Quartile 1 | Reference | Reference | ||
| Quartile 2 | 1.888 (1.726–2.066) | <0.001 | 1.197 (1.064–1.345) | 0.003 |
| Quartile 3 | 2.671 (2.449–2.912) | <0.001 | 1.330 (1.188–1.490) | <0.001 |
| Quartile 4 | 4.042 (3.718–4.395) | <0.001 | 1.612 (1.440–1.804) | <0.001 |
| Total cholesterol | ||||
| Quartile 1 | Reference | Reference | ||
| Quartile 2 | 1.071 (0.993–1.154) | 0.074 | 0.958 (0.869–1.055) | 0.382 |
| Quartile 3 | 1.225 (1.138–1.319) | <0.001 | 1.032 (0.938–1.135) | 0.518 |
| Quartile 4 | 1.284 (1.192–1.382) | <0.001 | 0.860 (0.779–0.948) | 0.002 |
| HDL-C | ||||
| Quartile 1 | Reference | Reference | ||
| Quartile 2 | 0.698 (0.652–0.747) | <0.001 | 0.886 (0.794–0.943) | 0.001 |
| Quartile 3 | 0.530 (0.493–0.570) | <0.001 | 0.874 (0.795–0.962) | 0.006 |
| Quartile 4 | 0.388 (0.359–0.419) | <0.001 | 0.774 (0.696–0.862) | <0.001 |
| LDL-C | ||||
| Quartile 1 | Reference | Reference | ||
| Quartile 2 | 1.044 (0.968–1.126) | 0.265 | 0.893 (0.810–0.985) | 0.023 |
| Quartile 3 | 1.177 (1.093–1.268) | <0.001 | 0.922 (0.839–1.014) | 0.096 |
| Quartile 4 | 1.329 (1.234–1.431) | <0.001 | 0.784 (0.712–0.864) | <0.001 |
| Chol/HDL-C ratio | ||||
| Quartile 1 | Reference | Reference | ||
| Quartile 2 | 1.548 (1.421–1.686) | <0.001 | 1.024 (0.916–1.145) | 0.676 |
| Quartile 3 | 2.235 (2.059–2.425) | <0.001 | 1.075 (0.965–1.197) | 0.189 |
| Quartile 4 | 2.951 (2.727–3.199) | <0.001 | 1.112 (0.997–1.239) | 0.056 |
| Characteristics | Incident Hypertension (−) (n = 18,295) | Incident Hypertension (+) (n = 3159) | p |
|---|---|---|---|
| Age (years) | 47.8 ± 10.2 | 54.8 ± 9.2 | <0.001 |
| Male sex (%) | 30.2 | 43.3 | <0.001 |
| DM (%) | 3.0 | 6.6 | <0.001 |
| Smoking history (%) | 22.9 | 29.9 | <0.001 |
| Alcohol history (%) | 2.5 | 4.2 | <0.001 |
| Regular exercise habits (%) | 45.0 | 52.7 | <0.001 |
| Systolic BP (mmHg) | 109.8 ± 12.3 | 124.3 ± 10.1 | <0.001 |
| Diastolic BP (mmHg) | 68.7 ± 8.6 | 76.5 ± 8.1 | <0.001 |
| Body mass index (kg/m2) | 23.4 ± 3.3 | 25.0 ± 3.4 | <0.001 |
| Laboratory parameters | |||
| Fasting glucose (mg/dL) | 93.6 ± 17.3 | 99.5 ± 24.9 | <0.001 |
| Hemoglobin (g/dL) | 13.6 ± 1.5 | 14.0 ± 1.5 | <0.001 |
| Triglyceride (mg/dL) | 104.2 ± 75.8 | 129.3 ± 97.9 | <0.001 |
| Total cholesterol (mg/dL) | 194.3 ± 35.3 | 199.5 ± 35.5 | <0.001 |
| HDL-C (mg/dL) | 55.8 ± 13.3 | 120.6 ± 31.4 | <0.001 |
| LDL-C (mg/dL) | 120.6 ± 31.4 | 125.8 ± 32.6 | <0.001 |
| Chol/HDL-C ratio | 3.65 ± 1.00 | 4.00 ± 1.05 | <0.001 |
| eGFR (mL/min/1.73 m2) | 112.2 ± 24.8 | 104.7 ± 24.6 | <0.001 |
| Uric acid (mg/dL) | 5.3 ± 1.3 | 5.8 ± 1.4 | <0.001 |
| Quartile of Lipid Profile | Univariable (Incident Hypertension) | Multivariable (Incident Hypertension) | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| Triglyceride | ||||
| Quartile 1 | Reference | Reference | ||
| Quartile 2 | 1.877 (1.652–2.132) | <0.001 | 1.402 (1.227–1.602) | <0.001 |
| Quartile 3 | 2.354 (2.078–2.666) | <0.001 | 1.365 (1.196–1.558) | <0.001 |
| Quartile 4 | 3.393 (3.009–3.825) | <0.001 | 1.617 (1.415–1.848) | <0.001 |
| Total cholesterol | ||||
| Quartile 1 | Reference | Reference | ||
| Quartile 2 | 1.185 (1.061–1.324) | 0.003 | 1.021 (0.907–1.148) | 0.733 |
| Quartile 3 | 1.300 (1.165–1.450) | <0.001 | 1.007 (0.895–1.133) | 0.911 |
| Quartile 4 | 1.477 (1.326–1.645) | <0.001 | 0.974 (0.865–1.097) | 0.663 |
| HDL-C | ||||
| Quartile 1 | Reference | Reference | ||
| Quartile 2 | 0.792 (0.718–0.873) | <0.001 | 0.994 (0.895–1.105) | 0.914 |
| Quartile 3 | 0.595 (0.535–0.661) | <0.001 | 0.886 (0.788–0.996) | 0.042 |
| Quartile 4 | 0.471 (0.422–0.526) | <0.001 | 0.819 (0.721–0.930) | 0.002 |
| LDL-C | ||||
| Quartile 1 | Reference | Reference | ||
| Quartile 2 | 1.132 (1.011–1.267) | 0.031 | 0.958 (0.850–1.080) | 0.481 |
| Quartile 3 | 1.283 (1.150–1.433) | <0.001 | 0.960 (0.854–1.080) | 0.499 |
| Quartile 4 | 1.579 (1.418–1.759) | <0.001 | 0.999 (0.888–1.123) | 0.987 |
| Chol/HDL-C ratio | ||||
| Quartile 1 | Reference | Reference | ||
| Quartile 2 | 1.547 (1.367–1.751) | <0.001 | 1.144 (1.005–1.302) | 0.042 |
| Quartile 3 | 2.076 (1.843–2.338) | <0.001 | 1.149 (1.011–1.306) | 0.034 |
| Quartile 4 | 2.745 (2.445–3.081) | <0.001 | 1.225 (1.075–1.396) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-H.; Liu, Y.-H.; Wu, D.-W.; Su, H.-M.; Chen, S.-C. Dyslipidemia Increases the Risk of Incident Hypertension in a Large Taiwanese Population Follow-Up Study. Nutrients 2022, 14, 3277. https://doi.org/10.3390/nu14163277
Lin Y-H, Liu Y-H, Wu D-W, Su H-M, Chen S-C. Dyslipidemia Increases the Risk of Incident Hypertension in a Large Taiwanese Population Follow-Up Study. Nutrients. 2022; 14(16):3277. https://doi.org/10.3390/nu14163277
Chicago/Turabian StyleLin, Yu-Hsuan, Yi-Hsueh Liu, Da-Wei Wu, Ho-Ming Su, and Szu-Chia Chen. 2022. "Dyslipidemia Increases the Risk of Incident Hypertension in a Large Taiwanese Population Follow-Up Study" Nutrients 14, no. 16: 3277. https://doi.org/10.3390/nu14163277
APA StyleLin, Y.-H., Liu, Y.-H., Wu, D.-W., Su, H.-M., & Chen, S.-C. (2022). Dyslipidemia Increases the Risk of Incident Hypertension in a Large Taiwanese Population Follow-Up Study. Nutrients, 14(16), 3277. https://doi.org/10.3390/nu14163277