
Parkinson’s Disease and Sugar Intake—Reasons for and Consequences of a Still Unclear Craving

Abstract
1. Introduction
2. Methods
3. Sugar Intake, Dopamine and Insulin in Parkinson’s Disease
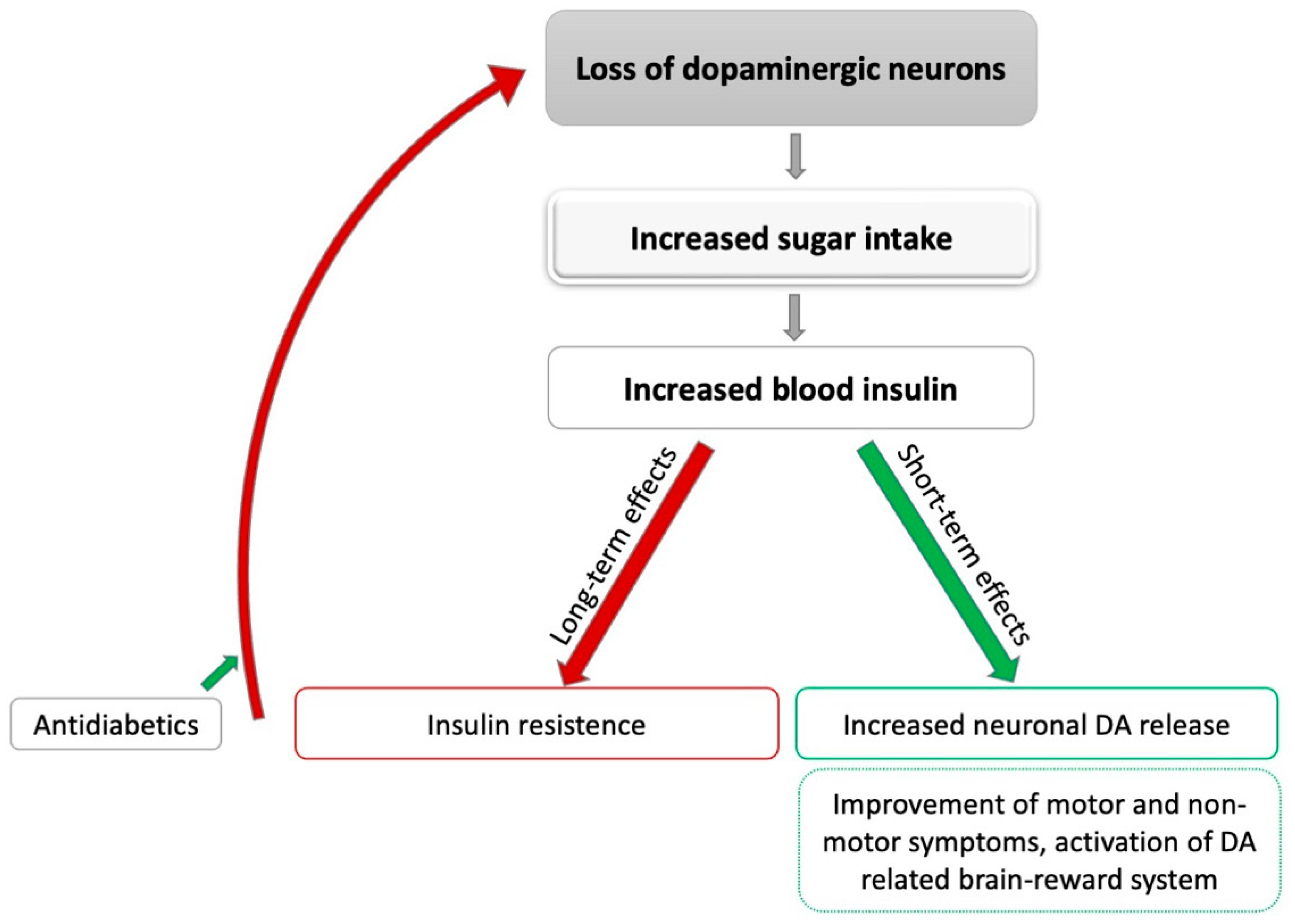
3.1. Effects of Sugar Intake on Dopamine Concentrations in the Brain via Insulin
3.2. Potential Interactions between Insulin Metabolism and Neurodegeneration in PD
3.3. Insulin Pathways in the Brain
3.4. Effects of Diabetes Medication on Risk of Developing PD
3.5. Effects of Diabetes Medication on Disease Progression in PD
4. Brain Reward Circuit—Dopamine, Insulin and Depression
5. Limitations and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Palavra, N.C.; Lubomski, M.; Flood, V.M.; Davis, R.L.; Sue, C.M. Increased Added Sugar Consumption Is Common in Parkinson’s Disease. Front. Nutr. 2021, 8, 628845. [Google Scholar] [CrossRef] [PubMed]
- Adén, E.; Carlsson, M.; Poortvliet, E.; Stenlund, H.; Linder, J.; Edström, M.; Forsgren, L.; Haglin, L. Dietary Intake and Olfactory Function in Patients with Newly Diagnosed Parkinson’s Disease: A Case-Control Study. Nutr. Neurosci. 2011, 14, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Cassani, E.; Barichella, M.; Ferri, V.; Pinelli, G.; Iorio, L.; Bolliri, C.; Caronni, S.; Faierman, S.A.; Mottolese, A.; Pusani, C. Dietary Habits in Parkinson’s Disease: Adherence to Mediterranean Diet. Parkinsonism Relat. Disord. 2017, 42, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Wolz, M.; Kaminsky, A.; Löhle, M.; Koch, R.; Storch, A.; Reichmann, H. Chocolate Consumption Is Increased in Parkinson’s Disease. J. Neurol. 2009, 256, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Lorefält, B.; Granérus, A.-K.; Unosson, M. Avoidance of Solid Food in Weight Losing Older Patients with Parkinson’s Disease. J. Clin. Nurs. 2006, 15, 1404–1412. [Google Scholar] [CrossRef] [PubMed]
- Meyers, C.; Amick, M.A.; Friedman, J.H. Ice Cream Preference in Parkinson’s Disease. Med. Health 2010, 93, 66–96. [Google Scholar]
- Wolz, M.; Schleiffer, C.; Klingelhöfer, L.; Schneider, C.; Proft, F.; Schwanebeck, U.; Reichmann, H.; Riederer, P.; Storch, A. Comparison of Chocolate to Cacao-Free White Chocolate in Parkinson’s Disease: A Single-Dose, Investigator-Blinded, Placebo-Controlled, Crossover Trial. J. Neurol. 2012, 259, 2447–2451. [Google Scholar] [CrossRef] [PubMed]
- Wills, A.-M.; Li, R.; Pérez, A.; Ren, X.; Boyd, J. Predictors of Weight Loss in Early Treated Parkinson’s Disease from the NET-PD LS-1 Cohort. J. Neurol. 2017, 264, 1746–1753. [Google Scholar] [CrossRef]
- Akbar, U.; He, Y.; Dai, Y.; Hack, N.; Malaty, I.; McFarland, N.R.; Hess, C.; Schmidt, P.; Wu, S.; Okun, M.S. Weight Loss and Impact on Quality of Life in Parkinson’s Disease. PLoS ONE 2015, 10, e0124541. [Google Scholar] [CrossRef]
- Uc, E.Y.; Struck, L.K.; Rodnitzky, R.L.; Zimmerman, B.; Dobson, J.; Evans, W.J. Predictors of Weight Loss in Parkinson’s Disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2006, 21, 930–936. [Google Scholar] [CrossRef]
- Craft, S.; Watson, G.S. Insulin and Neurodegenerative Disease: Shared and Specific Mechanisms. Lancet Neurol. 2004, 3, 169–178. [Google Scholar] [CrossRef]
- Morris, J.K.; Bomhoff, G.L.; Stanford, J.A.; Geiger, P.C. Neurodegeneration in an Animal Model of Parkinson’s Disease Is Exacerbated by a High-Fat Diet. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 299, R1082–R1090. [Google Scholar] [CrossRef] [PubMed]
- Shaughness, M.; Acs, D.; Brabazon, F.; Hockenbury, N.; Byrnes, K.R. Role of Insulin in Neurotrauma and Neurodegeneration: A Review. Front. Neurosci. 2020, 14, 940. [Google Scholar] [CrossRef] [PubMed]
- Bratanova-Tochkova, T.K.; Cheng, H.; Daniel, S.; Gunawardana, S.; Liu, Y.-J.; Mulvaney-Musa, J.; Schermerhorn, T.; Straub, S.G.; Yajima, H.; Sharp, G.W. Triggering and Augmentation Mechanisms, Granule Pools, and Biphasic Insulin Secretion. Diabetes 2002, 51, S83–S90. [Google Scholar] [CrossRef]
- Wilcox, G. Insulin and Insulin Resistance. Clin. Biochem. Rev. 2005, 26, 19. [Google Scholar]
- Figlewicz, D.P.; Evans, S.B.; Murphy, J.; Hoen, M.; Baskin, D.G. Expression of Receptors for Insulin and Leptin in the Ventral Tegmental Area/Substantia Nigra (VTA/SN) of the Rat. Brain Res. 2003, 964, 107–115. [Google Scholar] [CrossRef]
- Houten, M.V.; Posner, B.I.; Kopriwa, B.M.; Brawer, J.R. Insulin-Binding Sites in the Rat Brain: In Vivo Localization to the Circumventricular Organs by Quantitative Radioautography. Endocrinology 1979, 105, 666–673. [Google Scholar] [CrossRef]
- Unger, J.W.; Livingston, J.N.; Moss, A.M. Insulin Receptors in the Central Nervous System: Localization, Signalling Mechanisms and Functional Aspects. Prog. Neurobiol. 1991, 36, 343–362. [Google Scholar] [CrossRef]
- Levin, B.E. Glucose-Regulated Dopamine Release from Substantia Nigra Neurons. Brain Res. 2000, 874, 158–164. [Google Scholar] [CrossRef]
- Könner, A.C.; Hess, S.; Tovar, S.; Mesaros, A.; Sánchez-Lasheras, C.; Evers, N.; Verhagen, L.A.; Brönneke, H.S.; Kleinridders, A.; Hampel, B. Role for Insulin Signaling in Catecholaminergic Neurons in Control of Energy Homeostasis. Cell Metab. 2011, 13, 720–728. [Google Scholar]
- Stouffer, M.A.; Woods, C.A.; Patel, J.C.; Lee, C.R.; Witkovsky, P.; Bao, L.; Machold, R.P.; Jones, K.T.; De Vaca, S.C.; Reith, M.E. Insulin Enhances Striatal Dopamine Release by Activating Cholinergic Interneurons and Thereby Signals Reward. Nat. Commun. 2015, 6, 8543. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.C.; Stouffer, M.A.; Mancini, M.; Nicholson, C.; Carr, K.D.; Rice, M.E. Interactions between Insulin and Diet on Striatal Dopamine Uptake Kinetics in Rodent Brain Slices. Eur. J. Neurosci. 2019, 49, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Kleinridders, A.; Cai, W.; Cappellucci, L.; Ghazarian, A.; Collins, W.R.; Vienberg, S.G.; Pothos, E.N.; Kahn, C.R. Insulin Resistance in Brain Alters Dopamine Turnover and Causes Behavioral Disorders. Proc. Natl. Acad. Sci. USA 2015, 112, 3463–3468. [Google Scholar] [CrossRef]
- Kastner, A.; Hirsch, E.C.; Agid, Y.; Javoy-Agid, F. Tyrosine Hydroxylase Protein and Messenger RNA in the Dopaminergic Nigral Neurons of Patients with Parkinson’s Disease. Brain Res. 1993, 606, 341–345. [Google Scholar] [CrossRef]
- Takahashi, M.; Yamada, T.; Tooyama, I.; Moroo, I.; Kimura, H.; Yamamoto, T.; Okada, H. Insulin Receptor MRNA in the Substantia Nigra in Parkinson’s Disease. Neurosci. Lett. 1996, 204, 201–204. [Google Scholar] [CrossRef]
- Moroo, I.; Yamada, T.; Makino, H.; Tooyama, I.; McGeer, P.L.; McGeer, E.G.; Hirayama, K. Loss of Insulin Receptor Immunoreactivity from the Substantia Nigra Pars Compacta Neurons in Parkinson’s Disease. Acta Neuropathol. 1994, 87, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Manson, J.E.; Stampfer, M.J.; Hu, F.B.; Giovannucci, E.; Colditz, G.A.; Hennekens, C.H.; Willett, W.C. A Prospective Study of Whole-Grain Intake and Risk of Type 2 Diabetes Mellitus in US Women. Am. J. Public Health 2000, 90, 1409. [Google Scholar] [PubMed]
- Sahu, S.; Priyan, G.I. Consumption of Sweets as a Risk Factor for Diabetes Mellitus among Adults in Odisha-A Cross-Sectional Study. J. Adv. Med. Med. Res. 2018, 26, 1–5. [Google Scholar] [CrossRef]
- Steyn, N.P.; Mann, J.; Bennett, P.H.; Temple, N.; Zimmet, P.; Tuomilehto, J.; Lindström, J.; Louheranta, A. Diet, Nutrition and the Prevention of Type 2 Diabetes. Public Health Nutr. 2004, 7, 147–165. [Google Scholar] [CrossRef]
- Chohan, H.; Senkevich, K.; Patel, R.K.; Bestwick, J.P.; Jacobs, B.M.; Bandres Ciga, S.; Gan-Or, Z.; Noyce, A.J. Type 2 Diabetes as a Determinant of Parkinson’s Disease Risk and Progression. Mov. Disord. 2021, 36, 1420–1429. [Google Scholar] [CrossRef]
- Softic, S.; Stanhope, K.L.; Boucher, J.; Divanovic, S.; Lanaspa, M.A.; Johnson, R.J.; Kahn, C.R. Fructose and Hepatic Insulin Resistance. Crit. Rev. Clin. Lab. Sci. 2020, 57, 308–322. [Google Scholar] [CrossRef] [PubMed]
- De Pablo-Fernandez, E.; Goldacre, R.; Pakpoor, J.; Noyce, A.J.; Warner, T.T. Association between Diabetes and Subsequent Par-kinson Disease: A Record-Linkage Cohort Study. Neurology 2018, 91, e139–e142. [Google Scholar] [CrossRef] [PubMed]
- Schernhammer, E.; Hansen, J.; Rugbjerg, K.; Wermuth, L.; Ritz, B. Diabetes and the Risk of Developing Parkinson’s Disease in Denmark. Diabetes Care 2011, 34, 1102–1108. [Google Scholar] [CrossRef]
- Xu, Q.; Park, Y.; Huang, X.; Hollenbeck, A.; Blair, A.; Schatzkin, A.; Chen, H. Diabetes and Risk of Parkinson’s Disease. Diabetes Care 2011, 34, 910–915. [Google Scholar] [CrossRef]
- Yang, Y.-W.; Hsieh, T.-F.; Li, C.-I.; Liu, C.-S.; Lin, W.-Y.; Chiang, J.-H.; Li, T.-C.; Lin, C.-C. Increased Risk of Parkinson Disease with Diabetes Mellitus in a Population-Based Study. Medicine 2017, 96, e5921. [Google Scholar] [CrossRef]
- Yue, X.; Li, H.; Yan, H.; Zhang, P.; Chang, L.; Li, T. Risk of Parkinson Disease in Diabetes Mellitus: An Updated Meta-Analysis of Population-Based Cohort Studies. Medicine 2016, 95, e3549. [Google Scholar] [CrossRef] [PubMed]
- De Pablo-Fernandez, E.; Sierra-Hidalgo, F.; Benito-León, J.; Bermejo-Pareja, F. Association between Parkinson’s Disease and Diabetes: Data from NEDICES Study. Acta Neurol. Scand. 2017, 136, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Rhee, S.Y.; Han, K.-D.; Kwon, H.; Park, S.-E.; Park, Y.-G.; Kim, Y.-H.; Yoo, S.-J.; Rhee, E.-J.; Lee, W.-Y. Association between Glycemic Status and the Risk of Parkinson Disease: A Nationwide Population-Based Study. Diabetes Care 2020, 43, 2169–2175. [Google Scholar] [CrossRef]
- Deischinger, C.; Dervic, E.; Kaleta, M.; Klimek, P.; Kautzky-Willer, A. Diabetes Mellitus Is Associated with a Higher Relative Risk for Parkinson’s Disease in Women than in Men. J. Parkinson’s Dis. 2021, 11, 793–800. [Google Scholar] [CrossRef]
- Becker, C.; Brobert, G.P.; Johansson, S.; Jick, S.S.; Meier, C.R. Diabetes in Patients with Idiopathic Parkinson’s Disease. Diabetes Care 2008, 31, 1808–1812. [Google Scholar] [CrossRef]
- Cereda, E.; Barichella, M.; Pedrolli, C.; Klersy, C.; Cassani, E.; Caccialanza, R.; Pezzoli, G. Diabetes and Risk of Parkinson’s Disease: A Systematic Review and Meta-Analysis. Diabetes Care 2011, 34, 2614–2623. [Google Scholar] [CrossRef] [PubMed]
- Palacios, N.; Gao, X.; McCullough, M.L.; Jacobs, E.J.; Patel, A.V.; Mayo, T.; Schwarzschild, M.A.; Ascherio, A. Obesity, Diabetes, and Risk of Parkinson’s Disease. Mov. Disord. 2011, 26, 2253–2259. [Google Scholar] [CrossRef] [PubMed]
- Savica, R.; Grossardt, B.R.; Ahlskog, J.E.; Rocca, W.A. Metabolic Markers or Conditions Preceding Parkinson’s Disease: A Case-Control Study. Mov. Disord. 2012, 27, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Kotagal, V.; Albin, R.L.; Müller, M.L.; Koeppe, R.A.; Frey, K.A.; Bohnen, N.I. Diabetes Is Associated with Postural Instability and Gait Difficulty in Parkinson Disease. Parkinsonism Relat. Disord. 2013, 19, 522–526. [Google Scholar] [CrossRef]
- Wang, H. MicroRNAs, Parkinson’s Disease, and Diabetes Mellitus. Int. J. Mol. Sci. 2021, 22, 2953. [Google Scholar] [CrossRef]
- Pagano, G.; Polychronis, S.; Wilson, H.; Giordano, B.; Ferrara, N.; Niccolini, F.; Politis, M. Diabetes Mellitus and Parkinson Disease. Neurology 2018, 90, e1654–e1662. [Google Scholar] [CrossRef]
- Bosco, D.; Plastino, M.; Cristiano, D.; Colica, C.; Ermio, C.; De Bartolo, M.; Mungari, P.; Fonte, G.; Consoli, D.; Consoli, A. Dementia Is Associated with Insulin Resistance in Patients with Parkinson’s Disease. J. Neurol. Sci. 2012, 315, 39–43. [Google Scholar] [CrossRef]
- Bohnen, N.I.; Kotagal, V.; Müller, M.L.; Koeppe, R.A.; Scott, P.J.; Albin, R.L.; Frey, K.A.; Petrou, M. Diabetes Mellitus Is Inde-pendently Associated with More Severe Cognitive Impairment in Parkinson Disease. Parkinsonism Relat. Disord. 2014, 20, 1394–1398. [Google Scholar] [CrossRef]
- Athauda, D.; Foltynie, T. Insulin Resistance and Parkinson’s Disease: A New Target for Disease Modification? Prog. Neurobiol. 2016, 145, 98–120. [Google Scholar] [CrossRef]
- Cheong, J.L.; de Pablo-Fernandez, E.; Foltynie, T.; Noyce, A.J. The Association between Type 2 Diabetes Mellitus and Parkinson’s Disease. J. Parkinson’s Dis. 2020, 10, 775–789. [Google Scholar] [CrossRef]
- Hong, C.-T.; Chen, K.-Y.; Wang, W.; Chiu, J.-Y.; Wu, D.; Chao, T.-Y.; Hu, C.-J.; Chau, K.-Y.D.; Bamodu, O.A. Insulin Resistance Promotes Parkinson’s Disease through Aberrant Expression of α-Synuclein, Mitochondrial Dysfunction, and Deregulation of the Polo-like Kinase 2 Signaling. Cells 2020, 9, 740. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.-W.; Lin, Y.-T.; Ho, W.-Y.; Lu, P.-J.; Chen, H.-H.; Lai, C.-C.; Sun, G.-C.; Yeh, T.-C.; Hsiao, M.; Tseng, C.-J. Fructose Induced Neurogenic Hypertension Mediated by Overactivation of P38 MAPK to Impair Insulin Signaling Transduction Caused Central Insulin Resistance. Free Radic. Biol. Med. 2017, 112, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.K.; Zhang, H.; Gupte, A.A.; Bomhoff, G.L.; Stanford, J.A.; Geiger, P.C. Measures of Striatal Insulin Resistance in a 6-Hydroxydopamine Model of Parkinson’s Disease. Brain Res. 2008, 1240, 185–195. [Google Scholar] [CrossRef]
- Brauer, R.; Wei, L.; Ma, T.; Athauda, D.; Girges, C.; Vijiaratnam, N.; Auld, G.; Whittlesea, C.; Wong, I.; Foltynie, T. Diabetes Medications and Risk of Parkinson’s Disease: A Cohort Study of Patients with Diabetes. Brain 2020, 143, 3067–3076. [Google Scholar] [CrossRef] [PubMed]
- Svenningsson, P.; Wirdefeldt, K.; Yin, L.; Fang, F.; Markaki, I.; Efendic, S.; Ludvigsson, J.F. Reduced Incidence of Parkinson’s Disease after Dipeptidyl Peptidase-4 Inhibitors—A Nationwide Case-Control Study. Mov. Disord. 2016, 31, 1422–1423. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.; Singh, A.; Baxi, H.; Taylor, B.; Burgess, J.; Antony, B. Thiazolidinedione Use Is Associated with Reduced Risk of Parkinson’s Disease in Patients with Diabetes: A Meta-Analysis of Real-World Evidence. Neurol. Sci. 2020, 41, 3697–3703. [Google Scholar] [CrossRef]
- Connolly, J.G.; Bykov, K.; Gagne, J.J. Thiazolidinediones and Parkinson Disease: A Cohort Study. Am. J. Epidemiol. 2015, 182, 936–944. [Google Scholar] [CrossRef]
- Wu, H.-F.; Kao, L.-T.; Shih, J.-H.; Kao, H.-H.; Chou, Y.-C.; Li, I.-H.; Kao, S. Pioglitazone Use and Parkinson’s Disease: A Retro-spective Cohort Study in Taiwan. BMJ Open 2018, 8, e023302. [Google Scholar] [CrossRef]
- Wahlqvist, M.L.; Lee, M.-S.; Hsu, C.-C.; Chuang, S.-Y.; Lee, J.-T.; Tsai, H.-N. Metformin-Inclusive Sulfonylurea Therapy Reduces the Risk of Parkinson’s Disease Occurring with Type 2 Diabetes in a Taiwanese Population Cohort. Parkinsonism Relat. Disord. 2012, 18, 753–758. [Google Scholar] [CrossRef]
- Kang, H.; Khang, R.; Ham, S.; Jeong, G.R.; Kim, H.; Jo, M.; Lee, B.D.; Lee, Y.I.; Jo, A.; Park, C. Activation of the ATF2/CREB-PGC-1α Pathway by Metformin Leads to Dopaminergic Neuroprotection. Oncotarget 2017, 8, 48603. [Google Scholar] [CrossRef]
- Saewanee, N.; Praputpittaya, T.; Malaiwong, N.; Chalorak, P.; Meemon, K. Neuroprotective Effect of Metformin on Dopaminergic Neurodegeneration and α-Synuclein Aggregation in C. Elegans Model of Parkinson’s Disease. Neurosci. Res. 2019, 162, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Neurol, L. Pioglitazone in Early Parkinson’s Disease: A Phase 2, Multicentre, Double-Blind, Randomised Trial. Lancet Neurol. 2015, 14, 795–803. [Google Scholar]
- Fine, J.M.; Stroebel, B.M.; Faltesek, K.A.; Terai, K.; Haase, L.; Knutzen, K.E.; Kosyakovsky, J.; Bowe, T.J.; Fuller, A.K.; Frey, W.H. Intranasal Delivery of Low-Dose Insulin Ameliorates Motor Dysfunction and Dopaminergic Cell Death in a 6-OHDA Rat Model of Parkinson’s Disease. Neurosci. Lett. 2020, 714, 134567. [Google Scholar] [CrossRef] [PubMed]
- Iravanpour, F.; Dargahi, L.; Rezaei, M.; Haghani, M.; Heidari, R.; Valian, N.; Ahmadiani, A. Intranasal Insulin Improves Mitochondrial Function and Attenuates Motor Deficits in a Rat 6-OHDA Model of Parkinson’s Disease. CNS Neurosci. Ther. 2021, 27, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhang, X.; Li, S.; Wang, H.; Zhang, X.; Liu, L.; Xie, A. Intranasal Insulin Ameliorates Cognitive Impairment in a Rat Model of Parkinson’s Disease through Akt/GSK3β Signaling Pathway. Life Sci. 2020, 259, 118159. [Google Scholar] [CrossRef]
- Pang, Y.; Lin, S.; Wright, C.; Shen, J.; Carter, K.; Bhatt, A.; Fan, L.-W. Intranasal Insulin Protects against Substantia Nigra Dopaminergic Neuronal Loss and Alleviates Motor Deficits Induced by 6-OHDA in Rats. Neuroscience 2016, 318, 157–165. [Google Scholar] [CrossRef]
- Ramalingam, M.; Kim, S.-J. The Neuroprotective Role of Insulin Against MPP+-Induced Parkinson’s Disease in Differentiated SH-SY5Y Cells. J. Cell. Biochem. 2016, 117, 917–926. [Google Scholar] [CrossRef]
- Novak, P.; Pimentel Maldonado, D.A.; Novak, V. Safety and Preliminary Efficacy of Intranasal Insulin for Cognitive Impairment in Parkinson Disease and Multiple System Atrophy: A Double-Blinded Placebo-Controlled Pilot Study. PLoS ONE 2019, 14, e0214364. [Google Scholar] [CrossRef]
- Lu, M.; Su, C.; Qiao, C.; Bian, Y.; Ding, J.; Hu, G. Metformin Prevents Dopaminergic Neuron Death in MPTP/P-Induced Mouse Model of Parkinson’s Disease via Autophagy and Mitochondrial ROS Clearance. Int. J. Neuropsychopharmacol. 2016, 19, pyw047. [Google Scholar] [CrossRef]
- Mor, D.E.; Sohrabi, S.; Kaletsky, R.; Keyes, W.; Tartici, A.; Kalia, V.; Miller, G.W.; Murphy, C.T. Metformin Rescues Parkinson’s Disease Phenotypes Caused by Hyperactive Mitochondria. Proc. Natl. Acad. Sci. USA 2020, 117, 26438–26447. [Google Scholar] [CrossRef]
- Patil, S.P.; Jain, P.D.; Ghumatkar, P.J.; Tambe, R.; Sathaye, S. Neuroprotective Effect of Metformin in MPTP-Induced Parkinson’s Disease in Mice. Neuroscience 2014, 277, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Ryu, Y.-K.; Go, J.; Park, H.-Y.; Choi, Y.-K.; Seo, Y.J.; Choi, J.H.; Rhee, M.; Lee, T.G.; Lee, C.-H.; Kim, K.-S. Metformin Regulates Astrocyte Reactivity in Parkinson’s Disease and Normal Aging. Neuropharmacology 2020, 175, 108173. [Google Scholar] [CrossRef]
- Fitzgerald, J.C.; Zimprich, A.; Carvajal Berrio, D.A.; Schindler, K.M.; Maurer, B.; Schulte, C.; Bus, C.; Hauser, A.-K.; Kübler, M.; Lewin, R. Metformin Reverses TRAP1 Mutation-Associated Alterations in Mitochondrial Function in Parkinson’s Disease. Brain 2017, 140, 2444–2459. [Google Scholar] [CrossRef] [PubMed]
- El-Ghaiesh, S.H.; Bahr, H.I.; Ibrahiem, A.T.; Ghorab, D.; Alomar, S.Y.; Farag, N.E.; Zaitone, S.A. Metformin Protects from Rotenone–Induced Nigrostriatal Neuronal Death in Adult Mice by Activating AMPK-FOXO3 Signaling and Mitigation of Angiogenesis. Front. Mol. Neurosci. 2020, 13, 84. [Google Scholar] [CrossRef]
- Yan, Q.; Han, C.; Wang, G.; Waddington, J.L.; Zheng, L.; Zhen, X. Activation of AMPK/MTORC1-Mediated Autophagy by Metformin Reverses Clk1 Deficiency-Sensitized Dopaminergic Neuronal Death. Mol. Pharmacol. 2017, 92, 640–652. [Google Scholar] [CrossRef]
- Katila, N.; Bhurtel, S.; Park, P.-H.; Choi, D.-Y. Metformin Attenuates Rotenone-Induced Oxidative Stress and Mitochondrial Damage via the AKT/Nrf2 Pathway. Neurochem. Int. 2021, 148, 105120. [Google Scholar] [CrossRef] [PubMed]
- Katila, N.; Bhurtel, S.; Shadfar, S.; Srivastav, S.; Neupane, S.; Ojha, U.; Jeong, G.-S.; Choi, D.-Y. Metformin Lowers α-Synuclein Phosphorylation and Upregulates Neurotrophic Factor in the MPTP Mouse Model of Parkinson’s Disease. Neuropharmacology 2017, 125, 396–407. [Google Scholar] [CrossRef]
- Ozbey, G.; Nemutlu-Samur, D.; Parlak, H.; Yildirim, S.; Aslan, M.; Tanriover, G.; Agar, A. Metformin Protects Rotenone-Induced Dopaminergic Neurodegeneration by Reducing Lipid Peroxidation. Pharmacol. Rep. 2020, 72, 1397–1406. [Google Scholar] [CrossRef]
- Tayara, K.; Espinosa-Oliva, A.M.; García-Domínguez, I.; Ismaiel, A.A.; Boza-Serrano, A.; Deierborg, T.; Machado, A.; Herrera, A.J.; Venero, J.L.; de Pablos, R.M. Divergent Effects of Metformin on an Inflammatory Model of Parkinson’s Disease. Front. Cell. Neurosci. 2018, 12, 440. [Google Scholar] [CrossRef]
- Wang, D.-X.; Chen, A.-D.; Wang, Q.-J.; Xin, Y.-Y.; Yin, J.; Jing, Y.-H. Protective Effect of Metformin against Rotenone-Induced Parkinsonism in Mice. Toxicol. Mech. Methods 2020, 30, 350–357. [Google Scholar] [CrossRef]
- Ismaiel, A.A.; Espinosa-Oliva, A.M.; Santiago, M.; García-Quintanilla, A.; Oliva-Martín, M.J.; Herrera, A.J.; Venero, J.L.; de Pablos, R.M. Metformin, besides Exhibiting Strong In Vivo Anti-Inflammatory Properties, Increases Mptp-Induced Damage to the Nigrostriatal Dopaminergic System. Toxicol. Appl. Pharmacol. 2016, 298, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Abdelsalam, R.M.; Safar, M.M. Neuroprotective Effects of Vildagliptin in Rat Rotenone Parkinson’s Disease Model: Role of RAGE-NF ΚB and Nrf2-Antioxidant Signaling Pathways. J. Neurochem. 2015, 133, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.H.; Chung, S.J.; Yoo, H.S.; Hong, N.; Jung, J.H.; Baik, K.; Lee, Y.H.; Sohn, Y.H.; Lee, P.H. Beneficial Effects of Dipeptidyl Peptidase-4 Inhibitors in Diabetic Parkinson’s Disease. Brain 2021, 144, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhang, L.; Li, L.; Hölscher, C. Neuroprotective Effects of the Novel GLP-1 Long Acting Analogue Semaglutide in the MPTP Parkinson’s Disease Mouse Model. Neuropeptides 2018, 71, 70–80. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Li, L.; Hölscher, C. Neuroprotective Effects of (Val8) GLP-1-Glu-PAL in the MPTP Parkinson’s Disease Mouse Model. Behav. Brain Res. 2015, 293, 107–113. [Google Scholar] [CrossRef]
- Liu, W.; Jalewa, J.; Sharma, M.; Li, G.; Li, L.; Hölscher, C. Neuroprotective Effects of Lixisenatide and Liraglutide in the 1-Methyl-4-Phenyl-1, 2, 3, 6-Tetrahydropyridine Mouse Model of Parkinson’s Disease. Neuroscience 2015, 303, 42–50. [Google Scholar] [CrossRef]
- Elbassuoni, E.A.; Ahmed, R.F. Mechanism of the Neuroprotective Effect of GLP-1 in a Rat Model of Parkinson’s with Pre-Existing Diabetes. Neurochem. Int. 2019, 131, 104583. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, L.; Li, L.; Hölscher, C. Semaglutide Is Neuroprotective and Reduces α-Synuclein Levels in the Chronic MPTP Mouse Model of Parkinson’s Disease. J. Parkinson’s Dis. 2019, 9, 157–171. [Google Scholar] [CrossRef]
- Wang, V.; Kuo, T.-T.; Huang, E.Y.-K.; Ma, K.-H.; Chou, Y.-C.; Fu, Z.-Y.; Lai, L.-W.; Jung, J.; Choi, H.-I.; Choi, D.-S. Sustained Release GLP-1 Agonist PT320 Delays Disease Progression in a Mouse Model of Parkinson’s Disease. ACS Pharmacol. Transl. Sci. 2021, 4, 858–869. [Google Scholar] [CrossRef]
- Aksoy, D.; Solmaz, V.; Çavuşoğlu, T.; Meral, A.; Ateş, U.; Erbaş, O. Neuroprotective Effects of Eexenatide in a Rotenone-Induced Rat Model of Parkinson’s Disease. Am. J. Med. Sci. 2017, 354, 319–324. [Google Scholar] [CrossRef]
- Chen, S.; Yu, S.-J.; Li, Y.; Lecca, D.; Glotfelty, E.; Kim, H.K.; Choi, H.-I.; Hoffer, B.J.; Greig, N.H.; Kim, D.S. Post-Treatment with PT302, a Long-Acting Exendin-4 Sustained Release Formulation, Reduces Dopaminergic Neurodegeneration in a 6-Hydroxydopamine Rat Model of Parkinson’s Disease. Sci. Rep. 2018, 8, 10722. [Google Scholar] [CrossRef] [PubMed]
- Harkavyi, A.; Abuirmeileh, A.; Lever, R.; Kingsbury, A.E.; Biggs, C.S.; Whitton, P.S. Glucagon-like Peptide 1 Receptor Stimulation Reverses Key Deficits in Distinct Rodent Models of Parkinson’s Disease. J. Neuroinflamm. 2008, 5, 19. [Google Scholar] [CrossRef]
- Lin, T.-K.; Lin, K.-J.; Lin, H.-Y.; Lin, K.-L.; Lan, M.-Y.; Wang, P.-W.; Wang, T.-J.; Wang, F.-S.; Tsai, P.-C.; Liou, C.-W. Glucagon-like Peptide-1 Receptor Agonist Ameliorates 1-Methyl-4-Phenyl-1, 2, 3, 6-Tetrahydropyridine (MPTP) Neurotoxicity through Enhancing Mitophagy Flux and Reducing α-Synuclein and Oxidative Stress. Front. Mol. Neurosci. 2021, 14, 697440. [Google Scholar] [CrossRef] [PubMed]
- Aviles-Olmos, I.; Dickson, J.; Kefalopoulou, Z.; Djamshidian, A.; Ell, P.; Soderlund, T.; Whitton, P.; Wyse, R.; Isaacs, T.; Lees, A. Exenatide and the Treatment of Patients with Parkinson’s Disease. J. Clin. Investig. 2013, 123, 2730–2736. [Google Scholar] [CrossRef] [PubMed]
- Aviles-Olmos, I.; Dickson, J.; Kefalopoulou, Z.; Djamshidian, A.; Kahan, J.; Ell, P.; Whitton, P.; Wyse, R.; Isaacs, T.; Lees, A. Motor and Cognitive Advantages Persist 12 Months after Exenatide Exposure in Parkinson’s Disease. J. Parkinson’s Dis. 2014, 4, 337–344. [Google Scholar] [CrossRef]
- Athauda, D.; Maclagan, K.; Skene, S.S.; Bajwa-Joseph, M.; Letchford, D.; Chowdhury, K.; Hibbert, S.; Budnik, N.; Zampedri, L.; Dickson, J. Exenatide Once Weekly versus Placebo in Parkinson’s Disease: A Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2017, 390, 1664–1675. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, L.; Li, Y.; Li, L.; Melchiorsen, J.U.; Rosenkilde, M.; Hölscher, C. The Novel Dual GLP-1/GIP Receptor Agonist DA-CH5 Is Superior to Single GLP-1 Receptor Agonists in the MPTP Model of Parkinson’s Disease. J. Parkinson’s Dis. 2020, 10, 523–542. [Google Scholar] [CrossRef]
- Feng, P.; Zhang, X.; Li, D.; Ji, C.; Yuan, Z.; Wang, R.; Xue, G.; Li, G.; Hölscher, C. Two Novel Dual GLP-1/GIP Receptor Agonists Are Neuroprotective in the MPTP Mouse Model of Parkinson’s Disease. Neuropharmacology 2018, 133, 385–394. [Google Scholar] [CrossRef]
- Yuan, Z.; Li, D.; Feng, P.; Xue, G.; Ji, C.; Li, G.; Hölscher, C. A Novel GLP-1/GIP Dual Agonist Is More Effective than Liraglutide in Reducing Inflammation and Enhancing GDNF Release in the MPTP Mouse Model of Parkinson’s Disease. Eur. J. Pharmacol. 2017, 812, 82–90. [Google Scholar] [CrossRef]
- Li, T.; Tu, L.; Gu, R.; Yang, X.-L.; Liu, X.-J.; Zhang, G.-P.; Wang, Q.; Ren, Y.-P.; Wang, B.-J.; Tian, J.-Y. Neuroprotection of GLP-1/GIP Receptor Agonist via Inhibition of Mitochondrial Stress by AKT/JNK Pathway in a Parkinson’s Disease Model. Life Sci. 2020, 256, 117824. [Google Scholar] [CrossRef]
- Cao, L.; Li, D.; Feng, P.; Li, L.; Xue, G.-F.; Li, G.; Hölscher, C. A Novel Dual GLP-1 and GIP Incretin Receptor Agonist Is Neuroprotective in a Mouse Model of Parkinson’s Disease by Reducing Chronic Inflammation in the Brain. Neuroreport 2016, 27, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Jalewa, J.; Sharma, M.K.; Gengler, S.; Hölscher, C. A Novel GLP-1/GIP Dual Receptor Agonist Protects from 6-OHDA Lesion in a Rat Model of Parkinson’s Disease. Neuropharmacology 2017, 117, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Ji, C.; Xue, G.-F.; Lijun, C.; Feng, P.; Li, D.; Li, L.; Li, G.; Hölscher, C. A Novel Dual GLP-1 and GIP Receptor Agonist Is Neuroprotective in the MPTP Mouse Model of Parkinson′ s Disease by Increasing Expression of BNDF. Brain Res. 2016, 1634, 1–11. [Google Scholar] [CrossRef]
- Lv, M.; Xue, G.; Cheng, H.; Meng, P.; Lian, X.; Hölscher, C.; Li, D. The GLP-1/GIP Dual-Receptor Agonist DA5-CH Inhibits the NF-ΚB Inflammatory Pathway in the MPTP Mouse Model of Parkinson’s Disease More Effectively than the GLP-1 Single-Receptor Agonist NLY01. Brain Behav. 2021, 11, e2231. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.-Y.; Jin, Q.-Q.; Hölscher, C.; Li, L. Glucagon-like Peptide-1/Glucose-Dependent Insulinotropic Polypeptide Dual Receptor Agonist DA-CH5 Is Superior to Exendin-4 in Protecting Neurons in the 6-Hydroxydopamine Rat Parkinson Model. Neural Regen. Res. 2021, 16, 1660. [Google Scholar]
- Breidert, T.; Callebert, J.; Heneka, M.T.; Landreth, G.; Launay, J.M.; Hirsch, E.C. Protective Action of the Peroxisome Proliferator-Activated Receptor-γ Agonist Pioglitazone in a Mouse Model of Parkinson’s Disease. J. Neurochem. 2002, 82, 615–624. [Google Scholar] [CrossRef]
- Dehmer, T.; Heneka, M.T.; Sastre, M.; Dichgans, J.; Schulz, J.B. Protection by Pioglitazone in the MPTP Model of Parkinson’s Disease Correlates with IκBα Induction and Block of NFκB and INOS Activation. J. Neurochem. 2004, 88, 494–501. [Google Scholar] [CrossRef]
- Schintu, N.; Frau, L.; Ibba, M.; Caboni, P.; Garau, A.; Carboni, E.; Carta, A.R. PPAR-Gamma-Mediated Neuroprotection in a Chronic Mouse Model of Parkinson’s Disease. Eur. J. Neurosci. 2009, 29, 954–963. [Google Scholar] [CrossRef]
- Bonato, J.M.; Bassani, T.B.; Milani, H.; Vital, M.A.B.F.; de Oliveira, R.M.W. Pioglitazone Reduces Mortality, Prevents Depressive-like Behavior, and Impacts Hippocampal Neurogenesis in the 6-OHDA Model of Parkinson’s Disease in Rats. Exp. Neurol. 2018, 300, 188–200. [Google Scholar] [CrossRef]
- Machado, M.M.F.; Bassani, T.B.; Cóppola-Segovia, V.; Moura, E.L.R.; Zanata, S.M.; Andreatini, R.; Vital, M.A.B.F. PPAR-γ Agonist Pioglitazone Reduces Microglial Proliferation and NF-ΚB Activation in the Substantia Nigra in the 6-Hydroxydopamine Model of Parkinson’s Disease. Pharmacol. Rep. 2019, 71, 556–564. [Google Scholar] [CrossRef]
- Lee, E.Y.; Lee, J.E.; Park, J.H.; Shin, I.C.; Koh, H.C. Rosiglitazone, a PPAR-γ Agonist, Protects against Striatal Dopaminergic Neurodegeneration Induced by 6-OHDA Lesions in the Substantia Nigra of Rats. Toxicol. Lett. 2012, 213, 332–344. [Google Scholar] [CrossRef] [PubMed]
- Martin, H.L.; Mounsey, R.B.; Mustafa, S.; Sathe, K.; Teismann, P. Pharmacological Manipulation of Peroxisome Proliferator-Activated Receptor γ (PPARγ) Reveals a Role for Anti-Oxidant Protection in a Model of Parkinson’s Disease. Exp. Neurol. 2012, 235, 528–538. [Google Scholar] [CrossRef] [PubMed]
- Ulusoy, G.K.; Celik, T.; Kayir, H.; Gürsoy, M.; Isik, A.T.; Uzbay, T.I. Effects of Pioglitazone and Retinoic Acid in a Rotenone Model of Parkinson’s Disease. Brain Res. Bull. 2011, 85, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Laloux, C.; Petrault, M.; Lecointe, C.; Devos, D.; Bordet, R. Differential Susceptibility to the PPAR-γ Agonist Pioglitazone in 1-Methyl-4-Phenyl-1, 2, 3, 6-Tetrahydropyridine and 6-Hydroxydopamine Rodent Models of Parkinson’s Disease. Pharmacol. Res. 2012, 65, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Barbiero, J.K.; Santiago, R.M.; Lima, M.M.; Ariza, D.; Morais, L.H.; Andreatini, R.; Vital, M.A. Acute but Not Chronic Administration of Pioglitazone Promoted Behavioral and Neurochemical Protective Effects in the MPTP Model of Parkinson’s Disease. Behav. Brain Res. 2011, 216, 186–192. [Google Scholar] [CrossRef]
- Carta, A.R.; Frau, L.; Pisanu, A.; Wardas, J.; Spiga, S.; Carboni, E. Rosiglitazone Decreases Peroxisome Proliferator Receptor-Gamma Levels in Microglia and Inhibits TNF-Alpha Production: New Evidences on Neuroprotection in a Progressive Parkinson’s Disease Model. Neuroscience 2011, 194, 250–261. [Google Scholar] [CrossRef]
- Hassanzadeh, K.; Rahimi, A.; Moloudi, M.R.; Maccarone, R.; Corbo, M.; Izadpanah, E.; Feligioni, M. Effect of Lobeglitazone on Motor Function in Rat Model of Parkinson’s Disease with Diabetes Co-Morbidity. Brain Res. Bull. 2021, 173, 184–192. [Google Scholar] [CrossRef]
- Swanson, C.; Emborg, M. Expression of Peroxisome Proliferator-Activated Receptor-Gamma in the Substantia Nigra of Hemiparkinsonian Nonhuman Primates. Neurol. Res. 2014, 36, 634–646. [Google Scholar] [CrossRef]
- Pisanu, A.; Lecca, D.; Mulas, G.; Wardas, J.; Simbula, G.; Spiga, S.; Carta, A.R. Dynamic Changes in Pro-and Anti-Inflammatory Cytokines in Microglia after PPAR-γ Agonist Neuroprotective Treatment in the MPTPp Mouse Model of Progressive Parkinson’s Disease. Neurobiol. Dis. 2014, 71, 280–291. [Google Scholar] [CrossRef]
- Jung, T.W.; Lee, J.Y.; Shim, W.S.; Kang, E.S.; Kim, S.K.; Ahn, C.W.; Lee, H.C.; Cha, B.S. Rosiglitazone Protects Human Neuroblastoma SH-SY5Y Cells against MPP+ Induced Cytotoxicity via Inhibition of Mitochondrial Dysfunction and ROS Production. J. Neurol. Sci. 2007, 253, 53–60. [Google Scholar] [CrossRef]
- Pinto, M.; Nissanka, N.; Peralta, S.; Brambilla, R.; Diaz, F.; Moraes, C.T. Pioglitazone Ameliorates the Phenotype of a Novel Par-kinson’s Disease Mouse Model by Reducing Neuroinflammation. Mol. Neurodegener. 2016, 11, 25. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Kaundal, R.K.; More, S.; Sharma, S.S. Beneficial Effects of Pioglitazone on Cognitive Impairment in MPTP Model of Parkinson’s Disease. Behav. Brain Res. 2009, 197, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Arab, H.H.; Safar, M.M.; Shahin, N.N. Targeting ROS-Dependent AKT/GSK-3β/NF-ΚB and DJ-1/Nrf2 Pathways by Dapagliflozin Attenuates Neuronal Injury and Motor Dysfunction in Rotenone-Induced Parkinson’s Disease Rat Model. ACS Chem. Neurosci. 2021, 12, 689–703. [Google Scholar] [CrossRef] [PubMed]
- Schultz, W. Dopamine Signals for Reward Value and Risk: Basic and Recent Data. Behav. Brain Funct. 2010, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M. Depression in Parkinson’s Disease: Its Prevalence, Diagnosis, and Neurochemical Background. J. Neurol. 2001, 248, III5–III11. [Google Scholar]
- Blum, K.; Braverman, E.R.; Holder, J.M.; Lubar, J.F.; Monastra, V.J.; Miller, D.; Lubar, J.O.; Chen, T.J.; Comings, D.E. The Reward Deficiency Syndrome: A Biogenetic Model for the Diagnosis and Treatment of Impulsive, Addictive and Compulsive Behaviors. J. Psychoact. Drugs 2000, 32, 1–112. [Google Scholar] [CrossRef]
- Delis, F.; Thanos, P.K.; Rombola, C.; Rosko, L.; Grandy, D.; Wang, G.-J.; Volkow, N.D. Chronic Mild Stress Increases Alcohol Intake in Mice with Low Dopamine D2 Receptor Levels. Behav. Neurosci. 2013, 127, 95. [Google Scholar] [CrossRef]
- Noble, E.P.; Blum, K.; Khalsa, M.E.; Ritchie, T.; Montgomery, A.; Wood, R.C.; Fitch, R.J.; Ozkaragoz, T.; Sheridan, P.J.; Anglin, M.D. Allelic Association of the D2 Dopamine Receptor Gene with Cocaine Dependence. Drug Alcohol Depend. 1993, 33, 271–285. [Google Scholar] [CrossRef]
- Noble, E.P.; Noble, R.E.; Ritchie, T.; Syndulko, K.; Bohlman, M.C.; Noble, L.A.; Zhang, Y.; Sparkes, R.S.; Grandy, D.K. D2 Dopamine Receptor Gene and Obesity. Int. J. Eat. Disord. 1994, 15, 205–217. [Google Scholar] [CrossRef]
- Jimenez-Jimenez, F.J.; Molina, J.A.; Vargas, C.; Gomez, P.; De Bustos, F.; Zurdo, M.; Gomez-Escalonilla, C.; Barcenilla, B.; Berbel, A.; Camacho, A. Normal Cerebrospinal Fluid Levels of Insulin in Patients with Parkinson’s Disease. J. Neural Transm. 2000, 107, 445–449. [Google Scholar] [CrossRef]
- Mashayekhi, F.; Mirzajani, E.; Naji, M.; Azari, M. Expression of Insulin-like Growth Factor-1 and Insulin-like Growth Factor Binding Proteins in the Serum and Cerebrospinal Fluid of Patients with Parkinson’s Disease. J. Clin. Neurosci. 2010, 17, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Ghazi Sherbaf, F.; Mohajer, B.; Ashraf-Ganjouei, A.; Mojtahed Zadeh, M.; Javinani, A.; Sanjari Moghaddam, H.; Shirin Shandiz, M.; Aarabi, M.H. Serum Insulin-like Growth Factor-1 in Parkinson’s Disease; Study of Cerebrospinal Fluid Biomarkers and White Matter Microstructure. Front. Endocrinol. 2018, 9, 608. [Google Scholar] [CrossRef] [PubMed]
- Fronczek, R.; Overeem, S.; Lee, S.Y.; Hegeman, I.M.; Van Pelt, J.; Van Duinen, S.G.; Lammers, G.J.; Swaab, D.F. Hypocretin (Orexin) Loss in Parkinson’s Disease. Brain 2007, 130, 1577–1585. [Google Scholar] [CrossRef]
- Thannickal, T.C.; Lai, Y.-Y.; Siegel, J.M. Hypocretin (Orexin) Cell Loss in Parkinson’s Disease. Brain 2007, 130, 1586–1595. [Google Scholar] [CrossRef]
- Asakawa, A.; Inui, A.; Inui, T.; Katsuura, G.; Fujino, M.A.; Kasuga, M. Orexin Reverses Cholecystokinin-Induced Reduction in Feeding. Diabetes Obes. Metab. 2002, 4, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Shimada, M.; Tritos, N.A.; Lowell, B.B.; Flier, J.S.; Maratos-Flier, E. Mice Lacking Melanin-Concentrating Hormone Are Hypophagic and Lean. Nature 1998, 396, 670–674. [Google Scholar] [CrossRef]
- Levin, F.; Edholm, T.; Schmidt, P.T.; Gryback, P.; Jacobsson, H.; Degerblad, M.; Hoybye, C.; Holst, J.J.; Rehfeld, J.F.; Hellstrom, P.M. Ghrelin Stimulates Gastric Emptying and Hunger in Normal-Weight Humans. J. Clin. Endocrinol. Metab. 2006, 91, 3296–3302. [Google Scholar] [CrossRef]
- Morton, G.J.; Blevins, J.E.; Williams, D.L.; Niswender, K.D.; Gelling, R.W.; Rhodes, C.J.; Baskin, D.G.; Schwartz, M.W. Leptin Action in the Forebrain Regulates the Hindbrain Response to Satiety Signals. J. Clin. Investig. 2005, 115, 703–710. [Google Scholar] [CrossRef]
- Cersosimo, M.G.; Raina, G.B.; Pecci, C.; Pellene, A.; Calandra, C.R.; Gutiérrez, C.; Micheli, F.E.; Benarroch, E.E. Gastrointestinal Manifestations in Parkinson’s Disease: Prevalence and Occurrence before Motor Symptoms. J. Neurol. 2013, 260, 1332–1338. [Google Scholar] [CrossRef]
- Alcalay, R.N.; Gu, Y.; Mejia-Santana, H.; Cote, L.; Marder, K.S.; Scarmeas, N. The Association between Mediterranean Diet Adherence and Parkinson’s Disease. Mov. Disord. 2012, 27, 771–774. [Google Scholar] [CrossRef]
- Mischley, L.K.; Lau, R.C.; Bennett, R.D. Role of Diet and Nutritional Supplements in Parkinson’s Disease Progression. Oxid. Med. Cell. Longev. 2017, 2017, 6405278. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, C.T.; Guyer, H.; Langa, K.M.; Yaffe, K. Neuroprotective Diets Are Associated with Better Cognitive Function: The Health and Retirement Study. J. Am. Geriatr. Soc. 2017, 65, 1857–1862. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Animal/Cell Model | Human | |||
|---|---|---|---|---|
| Drug | Positive Effects | No/Negative Effects | Positive Effects | No/Negative Effects |
| Intranasal insulin | Improvement of motor function [63,64] Improvement of mitochondrial function [63,64] Improvement of cognitive function [65] Increased neuroprotection (animal model [66]; cell model [67]) | Improvement of motor function [68] Improvement of cognitive function [68] | ||
| Metformin | Improvement of motor function [60,69,70,71,72] Improvement of mitochondrial function [69,70,71,72,73], Increased neuroprotection [60,61,74,75,76] Decreased alpha-synuclein aggregation [61,77,78] Improvement of neuronal inflammation Increased anti-oxidant effect [71,79,80] | Increased neurodegeneration [81] | ||
| DPP-4 inhibitors | Improvement of motor function [82] Increased neuroprotection [82] | Increase in cerebral dopamine transporter [83] Slower increase in L-dopa dose [83] Less L-dopa-induced dyskinesia [83] | ||
| GLP-1 agonists | Improvement of motor function [84,85,86,87,88,89] Improvement of neuronal inflammation [84,88,90] Increased neuroprotection [84,86,88,89,90,91,92,93] Increased anti-oxidant effect [90] Decreased alpha-synuclein aggregation [88] Improvement mitochondrial function [88,93] | Improvement of cognitive function [94,95] Improvement of motor function [94,95,96] | ||
| GLP-1 and GIP agonists | Improvement of motor function [97,98,99,100,101,102] Increased neuroprotection [97,98,99,100,101,102,103,104,105] Improvement of neuronal inflammation [97,98,99,104] Improvement of mitochondrial function [97] | |||
| Glitazones | Reduction in glial activation [106,107,108,109,110,111] Increased neuroprotection [106,107,109,110,111,112,113,114,115,116,117,118,119] Increased anti-oxidant effect [112,120] Improvement of motor function [110,113,121,122] Improvement of neuronal inflammation [108,116,118,120,121] Improvement of cognitive function [122] Anti-depressant effect [109] Reduction in mortality [109] | Reduction in striatal dopamine through chronic treatment [115] | No effect [62] | |
| SGLT-2 inhibitor | Improvement of motor function [123] Decreased alpha-synuclein aggregation [123] Increased dopamine concentration [123] Reduction in oxidative stress [123] Improvement of neuronal inflammation [123] | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haas, J.; Berg, D.; Bosy-Westphal, A.; Schaeffer, E. Parkinson’s Disease and Sugar Intake—Reasons for and Consequences of a Still Unclear Craving. Nutrients 2022, 14, 3240. https://doi.org/10.3390/nu14153240
Haas J, Berg D, Bosy-Westphal A, Schaeffer E. Parkinson’s Disease and Sugar Intake—Reasons for and Consequences of a Still Unclear Craving. Nutrients. 2022; 14(15):3240. https://doi.org/10.3390/nu14153240
Chicago/Turabian StyleHaas, Julienne, Daniela Berg, Anja Bosy-Westphal, and Eva Schaeffer. 2022. "Parkinson’s Disease and Sugar Intake—Reasons for and Consequences of a Still Unclear Craving" Nutrients 14, no. 15: 3240. https://doi.org/10.3390/nu14153240
APA StyleHaas, J., Berg, D., Bosy-Westphal, A., & Schaeffer, E. (2022). Parkinson’s Disease and Sugar Intake—Reasons for and Consequences of a Still Unclear Craving. Nutrients, 14(15), 3240. https://doi.org/10.3390/nu14153240