
Altered Tryptophan Metabolism on the Kynurenine Pathway in Depressive Patients with Small Intestinal Bacterial Overgrowth

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Laboratory Tests
2.3. Therapeutic Procedures
2.4. Ethical Issues
2.5. Data Analysis
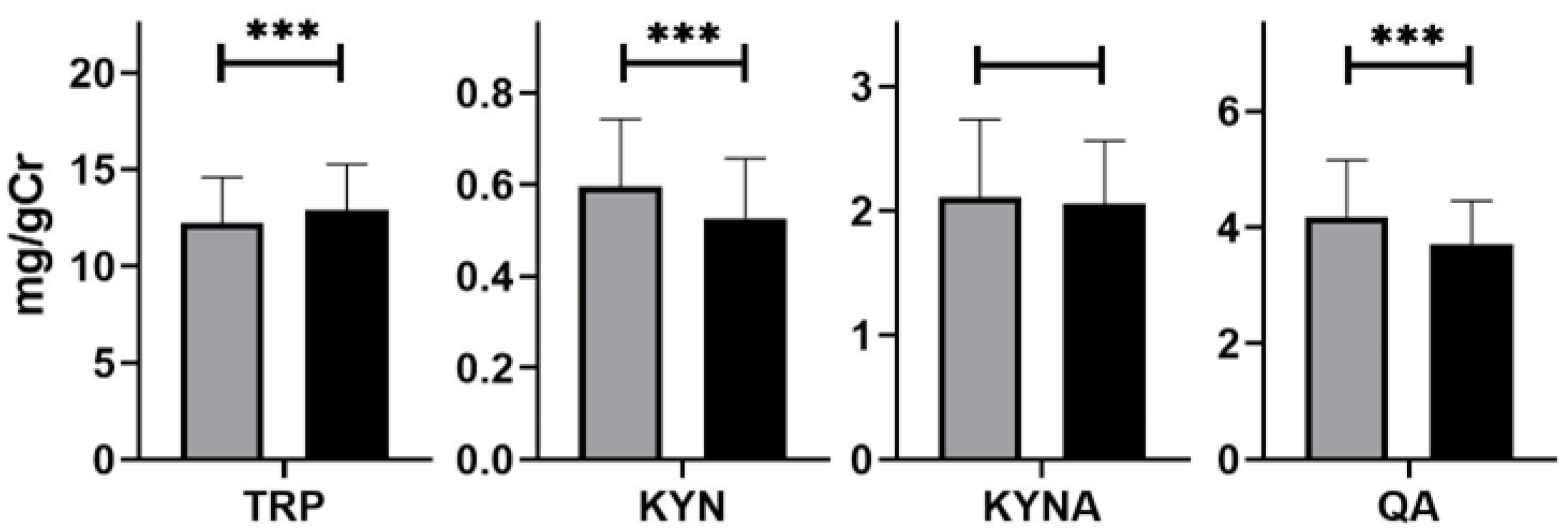
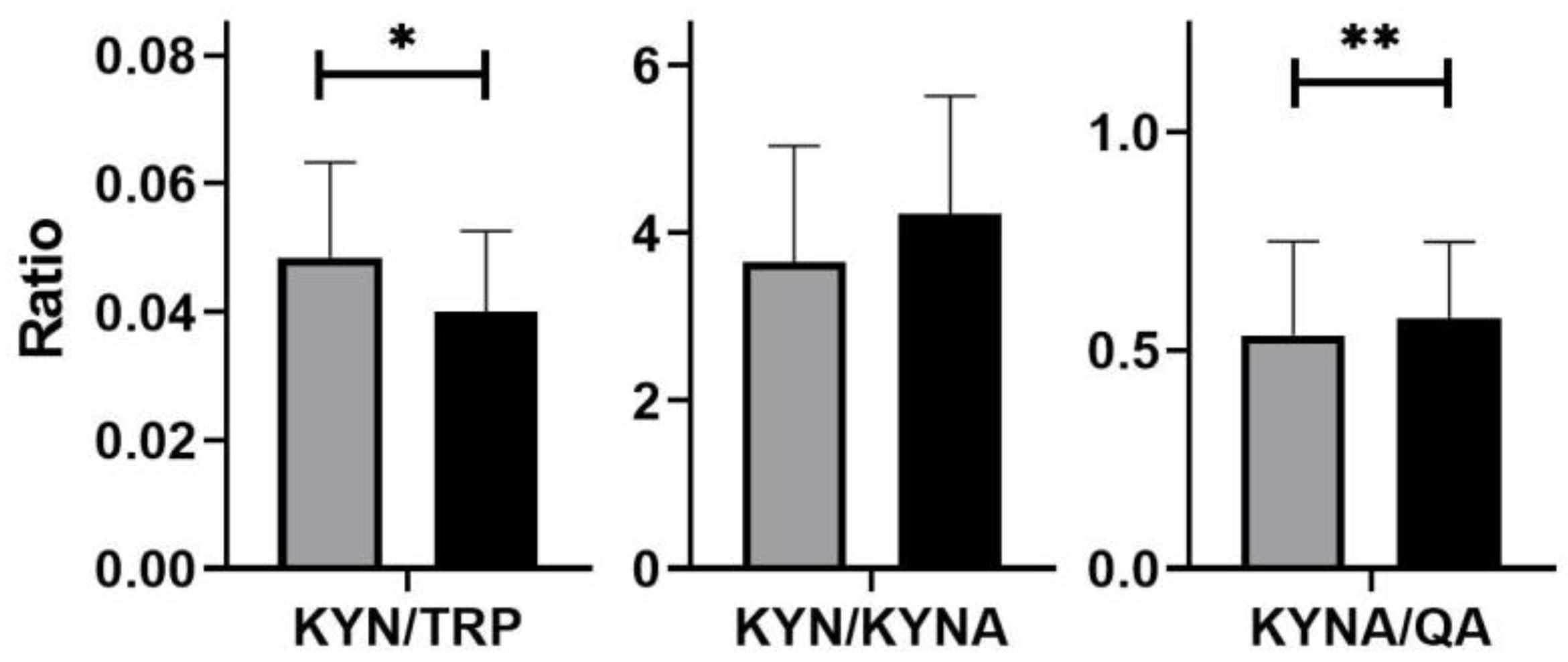
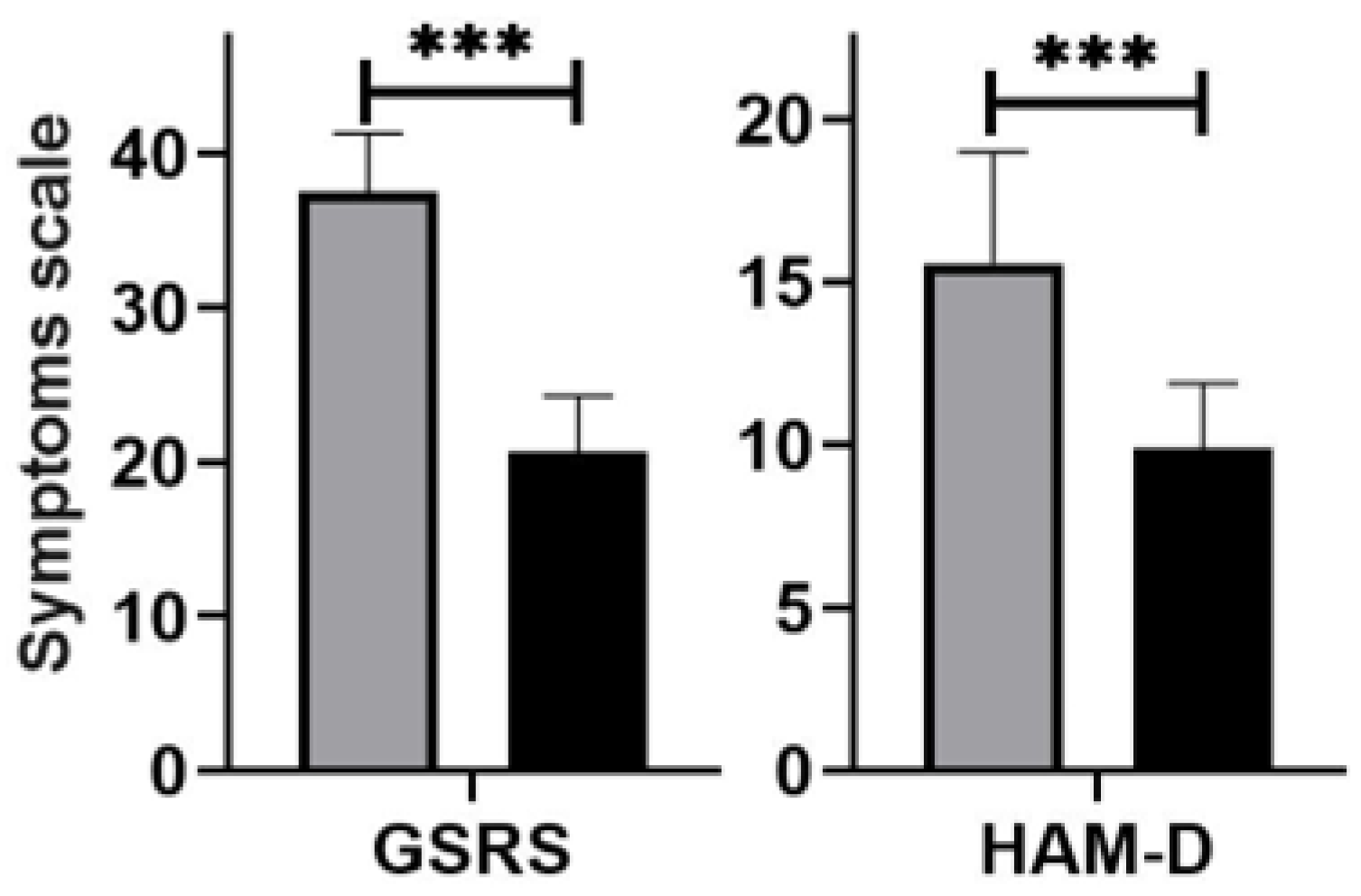
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saveanu, R.D.; Nemeroff, C.B. Etiology of Depression: Genetic and Environmental Factors. Psychiatr. Clin. 2012, 35, 51–71. [Google Scholar] [CrossRef] [PubMed]
- Arnone, D.; Saraykar, S.; Salem, H.; Teixeira, A.L.; Dantzer, R.; Selvaraj, S. Role of Kynurenine Pathway and Its Metabolites in Mood Disorders: A Systematic Review and Meta-Analysis of Clinical Studies. Neurosci. Biobehav. Rev. 2018, 92, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.W.; Terentis, A.C.; King, N.J.; Thomas, S.R. Role of indoleamine 2,3-dioxygenase in health and disease. Clin. Sci. 2015, 129, 601–672. [Google Scholar] [CrossRef] [PubMed]
- Palego, L.; Betti, L.; Rossi, A.; Giannaccini, G. Tryptophan Biochemistry: Structural, Nutritional, Metabolic, and Medical Aspects in Humans. J. Amino Acids 2016, 2016, 8952520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miura, H.; Ozaki, N.; Sawada, M.; Isobe, K.; Ohta, T.; Nagatsu, T. A Link between Stress and Depression: Shifts in the Balance between the Kynurenine and Serotonin Pathways of Tryptophan Metabolism and the Etiology and Pathophysiology of Depression. Stress 2008, 11, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Myint, A.M.; Kim, Y.K. Network beyond IDO in Psychiatric Disorders: Revisiting Neurodegeneration Hypothesis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 48, 304–313. [Google Scholar] [CrossRef]
- Savitz, J. Role of Kynurenine Metabolism Pathway Activation in Major Depressive Disorders. Curr. Top. Behav. Neurosci. 2017, 31, 249–268. [Google Scholar] [CrossRef]
- Dantzer, R.; O’Connor, J.C.; Lawson, M.C.; Kelley, K.W. Inflammation-Associated Depression: From Serotonin to Kynurenine. Psychoneuroendocrinology 2011, 36, 426–436. [Google Scholar] [CrossRef] [Green Version]
- Wichers, M.C.; Koek, G.H.; Robaeys, G.; Verkerk, R.; Scharpé, S.; Maes, M. IDO and Interferon-Alpha-Induced Depressive Symptoms: A Shift in Hypothesis from Tryptophan Depletion to Neurotoxicity. Mol. Psychiatry 2005, 10, 538–544. [Google Scholar] [CrossRef] [Green Version]
- Peyrot, F.; Ducrocq, C. Potential role of tryptophan derivates in stress responses characterized by the generation of reactive oxygen and nitrogen species. Pineal Res. 2008, 45, 235–246. [Google Scholar] [CrossRef]
- Braidy, N.; Grant, R.; Adams, S.; Brew, B.J.; Guillemin, G.J. Mechanism for Quinolinic Acid Cytotoxicity in Human Astrocytes and Neurons. Neurotox. Res. 2009, 16, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Guillemin, G.J. Quinolinic acid, the inescapable neurptoxin. FEBS J. 2012, 279, 1356–1365. [Google Scholar] [CrossRef] [PubMed]
- Oxenkrug, G. Serotonin-Kynurenine Hypothesis of Depression: Historical Overview and Recent Developments. Curr. Drug Targets 2013, 14, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, L.A.; Pérez-Padilla, E.A.; García-Oscos, F.; Salgado, H.; Atzori, M.; Pineda, J.C. A New Theory of Depression Based on the Serotonin/Kynurenine Relationship and the Hypothalamicpituitary- Adrenal Axis. Biomedica 2018, 38, 437–450. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, T.A.; Nguyen, J.C.; Polglaze, K.E.; Bertrand, P.P. Influence of Tryptophan and Serotonin on Mood and Cognition with a Possible Role of the Gut-Brain Axis. Nutrients 2016, 8, 56. [Google Scholar] [CrossRef]
- Kaur, H.; Bose, C.; Mande, S.S. Tryptophan Metabolism by Gut Microbiome and Gut-Brain-Axis: An in Silico Analysis. Front. Neurosci. 2019, 13, 1365. [Google Scholar] [CrossRef]
- Lindseth, G.; Holland, B.; Caspers, J. The effects of Diatary Tryptophanm on Affective Disorders. Arvives Psychiatr. Nurs. 2016, 29, 102–107. [Google Scholar] [CrossRef] [Green Version]
- Ruddick, J.P.; Evans, A.K.; Nutt, D.J.; Lightman, S.L.; Rook, G.A.; Lowry, C.A. Tryptophan Metabolism in the Central Nervous System: Medical Implications. Expert Rev. Mol. Med. 2006, 8, 1–27. [Google Scholar] [CrossRef]
- Gao, K.; Mu, C.; Farzi, A.; Zhu, W. Tryptophan Metabolism: A link Between the Gut Microbiota and Brain. Advences Nutr. 2020, 11, 709–723. [Google Scholar] [CrossRef]
- Takada, A.; Shimizu, F.; Takao, T. Tryptophan Metabolites in Plasma of Patients with Depression. Brain Nerve 2018, 70, 1025–1031. [Google Scholar] [CrossRef]
- Kim, Y.K.; Jeon, S.W. Neuroinflammation and the IMMUNe-Kynurenine Pathway in Anxiety Disorders. Curr. Neuropharmacoligy 2018, 16, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Quak, j.; Doornbos, B.; Roest, A.M.; Duivis, H.E.; Vogelzangs, N.; Nolen, W.A.; Penninx, B.W.; Kema, I.P.; de Jonge, P. Does tryptophan degradation along tke kynurenine pathway medaite the association between pro-inflammatory immune activity and depressive symptoms? Psychoneuroendocrinology 2014, 45, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Pompili, M.; Lionetto, L.; Curto, M.; Erbuto, D.; Montebovi, F.; Seretti, M.E.; Berardelli, I.; Serafini, G.; Innamorati, M.; Baldwssarini, R.J.; et al. Tryptophan and Kynurenine Metabolites: Are They Related to Depression? Neuropsychobiology 2019, 77, 23–28. [Google Scholar] [CrossRef]
- Colle, R.; Masson, P.; Verstuyft, C.; Feve, B.; Werner, E.; Boursier-Neyret, C.; Walther, B.; David, D.J.; Boniface, B.; Falissard, B.; et al. Peripheral tryptophan, serotonin, kynurenine, and their metabolites in major depression: A case control study. Psychiatry Clin. Neurosci. 2020, 74, 112–117. [Google Scholar] [CrossRef]
- Ogyu, K.; Kubo, K.; Noda, Y.; Iwata, Y.; Tsugawa, S.; Omura, Y.; Wada, M.; Tarumi, R.; Plitman, E.; Moriguchi, S.; et al. Kynurenine pathway in depression: A systemic review and meta-anaysis. Neuroscence Biobehav. Rev. 2018, 90, 16–25. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, S.M.; Claeke, G.; Borre, Y.E.; Dinan, T.G.; Cryan, J.F. Serotonin, tryptophan metabolism and the brain-gut-microbiome axis. Behav. Brain Res. 2015, 277, 32–48. [Google Scholar] [CrossRef] [PubMed]
- Regan, T.; Gill, A.C.; Barnett, M.W.; Pariante, C.M.; Harrison, N.A.; Hume, D.A.; Bullmore, E.T.; Freeman, T.C. Effects of anti-inflammatory drugs on the expression of tryptophan-metabolism genes by human macrophages. J. Leukoc. Biol. 2018, 103, 681–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beurel, E.; Toups, M.; Nemeroff, C.B. The Bideroctional Relationship of Depression and Inflammation: Doble Trouble. Neuron 2020, 107, 234–242. [Google Scholar] [CrossRef]
- Baranyi, A.; Amouzadeh-Ghadikolai, O.; von Lewinski, D.; Breitenecker, R.; Stojakovic, T.; Marz, W.; Robier, C.; Rothenhausler, H.B.; Mangge, H.; Meinitzer, A. Beta-trace Protein as a non-invasive immunological Marker for Quinolinic Acid- induced impaired Blod-Brain Barrier Integrity. Sci. Rep. 2017, 7, 43642. [Google Scholar] [CrossRef] [Green Version]
- Ljotsson, B.; Jones, M.; Talley, N.J.; Kjellstrom, L.; Agreus, L.; Andreasson, A. Discriminant and convergent validity of the GSRS-IBS symptom severity measure for irritable bowel syndrome: A population study. United Eur. Gastroenterol. J. 2020, 8, 284–292. [Google Scholar] [CrossRef] [Green Version]
- Carrozzino, D.; Patierno, C.; Fava, G.A.; Guidi, J. The Hamilton Rating Scales for Depression: A Critical Review of Clinimetric Properties of Different Versions. Psychother. Psychosom. 2020, 89, 133–150. [Google Scholar] [CrossRef] [PubMed]
- Evrensel, A.; Ünsalver, B.Ö.; Ceylan, M.E. Immune-Kynurenine Pathways and the Gut Microbiota-Brain Axis in Anxiety Disorders. Adv. Exp. Med. Biol. 2020, 1191, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Badawy, A.A. Kynurenine Pathway of Tryptophan Metabolism: Regulatory and Functional Aspects. Int. J. Tryptophan Res. IJTR 2017, 15, 1178646917691938. [Google Scholar] [CrossRef] [Green Version]
- Schwarcz, R.; Bruno, J.P.; Muchowski, P.J.; Wu, H.-Q. Kynurenines in the mammalian brain: When physiology meets pathology. Neuroscience 2012, 13, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Clarke, G.; Fitzgerald, P.; Cryan, J.F.; Cassidy, E.M.; Quigley, E.M.; Dinan, T.G. Tryptophan Degradation in Irritable Bowel Syndrome: Evidence of Indoleamine 2,3-Dioxygenase Activation in a Male Cohort. BMC Gastroenterol. 2009, 9, 6. [Google Scholar] [CrossRef] [Green Version]
- Heitkemper, M.M.; Han, C.J.; Jarrett, M.E.; Gu, H.; Djukovic, D.; Shulman, R.J.; Raftery, D.; Henderson, W.A.; Cain, K.C. Serum Tryptophan Metabolite Levels During Sleep in Patients With and Without Irritable Bowel Syndrome (IBS). Biol. Res. Nurs. 2016, 18, 193–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keszthelyi, D.; Troost, F.J.; Jonkers, D.M.; Kruimel, J.W.; Leue, C.; Masclee, A.A. Decreased Levels of Kynurenic Acid in the Intestinal Mucosa of IBS Patients: Relation to Serotonin and Psychological State. J. Psychosom. Res. 2013, 74, 501–504. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, P.; Cassidy Eugene, M.; Clarke, G.; Scully, P.; Barry, S.; Quigley Eamonn, M.M.; Shanahan, F.; Cryan, J.; Dinan Timothy, G. Tryptophan Catabolism in Females with Irritable Bowel Syndrome: Relationship to Interferon-Gamma, Severity of Symptoms and Psychiatric Co-Morbidity. Neurogastroenterol. Motil. 2008, 20, 1291–1297. [Google Scholar] [CrossRef]
- Christmas, D.M.; Badawy, A.; Hince, D.; Davies, S.; Probert, C.S.J.; Creed, T.; Smithson, J.E.; Afzal, M.; Nutt, D.J.; Potokar, J.P. Increased Serum Free Tryptophan in Patients with Diarrhea-Predominant Irritable Bowel Syndrome. Nutr. Res. 2010, 30, 678–688. [Google Scholar] [CrossRef]
- Ciorba, M.A. Indoleamine 2,3-dioxygenase in intestinal disease. Curr. Opin. Gastroenterol. 2013, 29, 146–152. [Google Scholar] [CrossRef] [Green Version]
- Acovic, A.; Simovic Markovic, B.; Gazdic, M.; Arsenijevic, A.; Jovicic, N.; Gajovic, N.; Janovic, M.; Zdravkovic, N.; Kanjevac, T.; Harrell, C.R.; et al. Indoleamine 2,3-dioxygenase-dependent expansion of T-regulatory cells maintains mucosal healing in ulcerative colitis. Ther. Advences Gastroenterol. 2018, 11, 1756284818793558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sofia, M.A.; Ciorba, M.A.; Meckel, K.; Lim, C.K.; Guillemin, G.J.; Weber, C.R.; Bissonette, M.; Pekow, J.R. Tryptophan Metabolism trough the Kynurenine PaThway is Associated wit Endoscopic Inflammation in Ulcerative Colitis. Infalammatory Bowel Dis. 2018, 24, 1471–1480. [Google Scholar] [CrossRef] [PubMed]
- Nikolaus, S.; Schulte, B.; Al-Massad, N.; Thieme, F.; Dchulte, D.M.; Bethge, J.; Rehman, A.; Tran, F.; Aden, K.; Häsler, R.; et al. Increased Tryptophan Metabolism Is Associated With Activity of Inflammatory Bowel Diseases. Gastroenterology 2017, 153, 1504–1516.ed. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, P.J.; Cryan, J.F.; Dinan, T.G.; Clarke, G. Kynurenine pathway metabolism and the microbiota-gut-brain axis. Neuropharmacology 2017, 112, 399–412. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.K.; Haker, A.I.; Kanuri, N.K.; Riehl, T.R.; Rowley, C.W.; Stenson, W.F.; Ciorba, M.A. Serum Analysis of Tryptophan Catabolism Pathway: Correlation with Crohn’s Disease Activity. Inflamm. Bowel Dis. 2012, 18, 1214–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montalban-Arques, A.; Chaparro, M.; Gisbert, J.P.; Bernardo, D. The Innate Immune System in the Gastrointestinal Tract: Role if Intraepithelial Lymphocytes and Lamina Propria Innate Lynphoid Cells in Intestinal Inflammation. Inflamm. Bowel Dis. 2018, 24, 1649–1659. [Google Scholar] [CrossRef]
- Konjar, S.; Ferreira, C.; Blankenhaus, B.; Veldhoen, M. Intestinal Barrier Infections with Specialized CD8 T Cells. Front. Immunol. 2017, 8, 1281. [Google Scholar] [CrossRef]
- Finke, D.; Acha-Orbea, H. Differential migration of in vivo primed B and T lymphocytes to lymphoid and non-lymphoid organs. Eur. J. Immunol. 2001, 31, 2603–2611. [Google Scholar] [CrossRef]
- Dudzińska, E.; Szymona, K.; Kloc, R.; Kocki, T.; Swistowska, M.; Kocki, J.; Urbańska, E.M. Increased expression of kynyrenine aminotransferase mRNA in lymphocytes of patientys with inflammatory bowel disease. Ther. Advences Gastroenterol. 2019, 12, 1756284819881304. [Google Scholar] [CrossRef]
- Roager, H.M.; Licht, T.R. Microbial tryptophan catabolites in health and disease. Nat. Commun. 2018, 9, 3294. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Liu, H.; McKenzie, G.; Witting, P.K.; Stasch, J.P.; Hahn, M.; Changsirivathamrong, D.; Wu, B.J.; Ball, H.J.; Thomas, S.R.; et al. Kynurenine is an endothelium-drived relaxing factors produced during inflammation. Nat. Med. 2010, 16, 279–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, S.W.; Kim, Y.K. Inflammation-induced depression: Its pathophysiology and therapeytic implications. J. Neuroimmunol. 2017, 13, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, D.M.; Chen, B.; Iticovici, M.; Thaker, A.I.; Dai, N.; VanDussen, K.L.; Shaikh, N.; Lim, C.K.; Guillemin, G.J.; Tarr, P.I.; et al. Epithelial Indeloamine 2,3-Dioxygenase 1 Modulates Aryl Hydrocarbon Receptor and Notch Signaling to Increase Differerentiation of Secretory Cells and Alter Mucus-Associated Microbiota. Gastroenterology 2019, 157, 1093–1108.e11. [Google Scholar] [CrossRef] [PubMed]
- Wachowska, K.; Szemraj, J.; Śmigielski, J.; Gałecki, P. Inflammatory Markers and Episodic Memory Functioning in Depressive Disorders. J. Clin. Med. 2022, 11, 693. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, N.; Hoshikawa, T.; Ikenouchi, A.; Yoshimura, R. Comparison of psychiatrics symptoms between patients with major depression with higher and lower levels of high-sensitivity C-reactive protein in the serum: A preliminary study. Ther. Adv. Psychopharmacol. 2021, 11, 20451263211060228. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Controls | Patients |
|---|---|---|
| Age (years) | 44.7 ± 7.3 | 45.2 ± 9.4 |
| Gender-(M/F) | 17/23 | 15/25 |
| BMI (kg/m2) | 23.8 ± 1.6 | 22.4 ± 2.1 |
| CRP (mg/L) | 1.59 ± 0.28 | 6.72 ± 2.91 * |
| FC (µg/g) | 24.5 ± 6.4 | 46.2 ± 19.2 * |
| AST (U/L) | 16.2 ± 3.1 | 17.1 ± 7.8 |
| ALT (U/L) | 17.4 ± 4.9 | 21.9 ± 7.6 |
| Amylase (U/L) | 35.7 ± 12.4 | 43.8 ± 19.2 |
| Lipase (U/L) | 72.6 ± 21.1 | 47.3 ± 15.4 |
| Creatinine (mg/dL) | 0.75 ± 0.23 | 0.86 ± 0.21 |
| GFR (ml/min) | 97.2 ± 10.3 | 88.9 ± 10.1 |
| LHBT (ppm) | 10.6 ± 4.19 | 69.2 ± 16.2 *** |
| HAM-D score | 9.85 ± 2.21 | 26.3 ± 4.26 *** |
| TRP (mg daily) | 1368 ± 193 | 1428 ± 203 |
| A Pairs of Variable | Rho-Spearman | p-Value |
|---|---|---|
| HAM-D and LHBT | 0.36024 | 0.05041 |
| HAM-D and CRP | 0.27976 | 0.13616 |
| HAM-D and FC | 0.33455 | 0.03486 |
| HAM-D and IEL | 0.37491 | 0.01752 |
| HAM-D and KYN | 0.35333 | 0.02545 |
| HAM-D and KYNA | 0.33134 | 0.07480 |
| HAM-D and QA | 0.50612 | 0.00430 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chojnacki, C.; Konrad, P.; Błońska, A.; Medrek-Socha, M.; Przybylowska-Sygut, K.; Chojnacki, J.; Poplawski, T. Altered Tryptophan Metabolism on the Kynurenine Pathway in Depressive Patients with Small Intestinal Bacterial Overgrowth. Nutrients 2022, 14, 3217. https://doi.org/10.3390/nu14153217
Chojnacki C, Konrad P, Błońska A, Medrek-Socha M, Przybylowska-Sygut K, Chojnacki J, Poplawski T. Altered Tryptophan Metabolism on the Kynurenine Pathway in Depressive Patients with Small Intestinal Bacterial Overgrowth. Nutrients. 2022; 14(15):3217. https://doi.org/10.3390/nu14153217
Chicago/Turabian StyleChojnacki, Cezary, Paulina Konrad, Aleksandra Błońska, Marta Medrek-Socha, Karolina Przybylowska-Sygut, Jan Chojnacki, and Tomasz Poplawski. 2022. "Altered Tryptophan Metabolism on the Kynurenine Pathway in Depressive Patients with Small Intestinal Bacterial Overgrowth" Nutrients 14, no. 15: 3217. https://doi.org/10.3390/nu14153217
APA StyleChojnacki, C., Konrad, P., Błońska, A., Medrek-Socha, M., Przybylowska-Sygut, K., Chojnacki, J., & Poplawski, T. (2022). Altered Tryptophan Metabolism on the Kynurenine Pathway in Depressive Patients with Small Intestinal Bacterial Overgrowth. Nutrients, 14(15), 3217. https://doi.org/10.3390/nu14153217