
Maternal Factors Associated with Non-Exclusive Breastfeeding in Haitian Immigrant Women in Southern Chile

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Organization for Migration. World Migration Report 2020. Available online: https://publications.iom.int/system/files/pdf/wmr_2020.pdf (accessed on 23 May 2022).
- Maury-Sintjago, E.; Rodríguez-Fernández, A.; García, D.; Parra-Flores, J. High prevalence of food insecurity and factors associated with Haitian immigrants in Southern Chile. J. Immigr. Minority Health 2019, 21, 1436–1439. [Google Scholar] [CrossRef] [PubMed]
- Chang, C. Social determinants of health and health disparities among immigrants and their children. Curr. Probl. Pediatric Adolesc. Health Care 2019, 49, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Donato, K.M.; Hamilton, E.R.; Bernard-Sasges, A. Gender and health in Mexico: Differences between returned migrants and non-migrants. ANNALS Am. Acad. Political Soc. Sci. 2019, 684, 165–187. [Google Scholar] [CrossRef]
- Mosca, F.; Gianni, M. Human Milk: Composition and health benefits. Pediatr. Med. Chir. 2017, 39, 155. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Gutiérrez, L.; González-Stager, M.A.; Pastén-Dué, G.; Rodríguez-Fernández, A.; Parra-Flores, J.; Maury-Sintjago, E. Association between high pre-pregnancy body mass index, excess gestational weight gain, and poor breastfeeding with overweight in 3-4-year-old Chilean children. Nutrition 2020, 77, 110786. [Google Scholar] [CrossRef]
- UNICEF. From the First Hour of Life: Making the Case for Improved Infant and Young Child Feeding Everywhere; UNICEF: New York, NY, USA, 2016. [Google Scholar]
- Horta, B.; de Mola, C.L.; Victora, C. Breastfeeding and intelligence: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 14–19. [Google Scholar] [CrossRef]
- Boutwell, B.; Young, J.; Meldrum, R. On the positive relationship between breastfeeding & intelligence. Dev. Psychol 2018, 54, 1426–1433. [Google Scholar] [CrossRef]
- Durán-Agüero, S.; Castro-Villarroel, P. Evolución de la lactancia materna exclusiva en Chile entre 2011 y 2015: ¿influyó el Permiso Postnatal Parental? Rev. Esp. Nutr. Hum. Diet. 2018, 22, 14–20. [Google Scholar] [CrossRef]
- McLennan, J.; Sampasa-Kanyinga, H. Do Differences in Prelacteal Feeding Explain Differences in Subsequent Breastfeeding Between Haiti and the Dominican Republic? Matern. Child Health J. 2020, 24, 462–471. [Google Scholar] [CrossRef]
- Victoria, C.; Bahl, R.; Darros, A.; Franca, G.; Horton, S.; Krasevec, E. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Nolan, A.; Layte, R. The ‘healthy immigrant effect’: Breastfeeding behavior in Ireland. Eur. J. Public Health 2015, 25, 626–631. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dennis, C.; Shiri, R.; Brown, H.; Santos, H.; Schmied, V.; Falah-Hassani, K. Breastfeeding rates in immigrant and non-immigrant women: A systematic review and meta-analysis. Matern. Child Nutr. 2019, 15, e12809. [Google Scholar] [CrossRef]
- Do Espíritu Santo, L.C.; de Oliveira, L.D.; Justo, E. Factors Associated with Low Incidence of Exclusive Breastfeeding for the First 6 Months. Birth 2007, 34, 212–219. [Google Scholar] [CrossRef]
- Agho, K.; Dibley, M.; Odiase, J.; Ogbonmwan, S. Determinants of exclusive breastfeeding in Nigeria. BMC Pregnancy Childbirth 2011, 112, 11. [Google Scholar] [CrossRef] [PubMed]
- Kyoko, N.; Michiko, K.; Ayumi, T.; Kazumichi, A. Prepregnancy obesity as a risk factor for exclusive breastfeeding initiation in Japanese women. Nutrition 2019, 62, 93–99. [Google Scholar] [CrossRef]
- Al Sabbah, H.; Assaf, E.; Taha, Z.; Qasrawi, R.; Radwan, H. Determinants of exclusive breastfeeding and mixed feeding among mothers of infants in Dubai and Sharjah, United Arab Emirates. Front. Nutr. 2022, 9, 872217. [Google Scholar] [CrossRef]
- Barreras, G. Evaluación Nutricional Del Crecimiento y Del Riesgo Cardiovascular y Metabólico, 13th ed.; Editorial U Chile: Santiago, Chile, 2018. [Google Scholar]
- MINSAL. Norma Técnica De Los Programas Alimentarios. Ministerio De Salud (Chile). Available online: http://www.minsal.cl (accessed on 30 May 2022).
- Azad, M.; Nickel, N.; Bode, L.; Brockway, M.; Brown, A.; Chambers, C. Breastfeeding and the origins of health: Interdisciplinary perspectives and priorities. Matern. Child Nutr. 2021, 17, e13109. [Google Scholar] [CrossRef]
- Vanderlinden, K.; Van de Putte, B. Pathways of equality through education: Impact of gender (in)equality and maternal education on exclusive breastfeeding among natives and migrants in Belgium. Matern. Child. Nutr. 2017, 13, e12309. [Google Scholar] [CrossRef]
- Tavoulari, E.; Benetou, V.; Vlastarakos, P.; Kreatsas, G.; Linos, A. Immigrant status as important determinant of breastfeeding practice in Southern Europe. Cent. Eur. J. Public Health 2015, 23, 39–44. [Google Scholar] [CrossRef][Green Version]
- Dennis, C.; Brown, H.; Chung-Lee, L.; Abbass-Dick, J.; Shorey, S.; Marini, F. Prevalence and predictors of exclusive breastfeeding among immigrant and Canadian-born Chinese women. Matern. Child Nutr. 2019, 15, e12687. [Google Scholar] [CrossRef]
- Gardner, W.; Kassebaum, N. Global, Regional, and National Prevalence and Trends in Infant Breastfeeding Status in 204 Countries and Territories, 1990–2019. Curr. Dev. Nutr. 2020, 4, 992. [Google Scholar] [CrossRef]
- Oakley, L.; Benova, L.; Macleod, D.; Lynch, C.; Campbell, O. Early breastfeeding practices: Descriptive analysis of recent Demographic and Health Surveys. Matern. Child Nutr. 2017, 14, e12535. [Google Scholar] [CrossRef] [PubMed]
- Wan, K.; Li, D.; Chan, N.; Wong, J.; Tarrant, M. The impact of immigration on the breastfeeding practices of mainland Chinese immigrants in Hong Kong. Birth 2017, 45, 94–102. [Google Scholar] [CrossRef]
- Gibson-Davis, C.; Brooks-Gunn, J. Couples immigration status and ethnicity as determinants of breastfeeding. Am. J. Public Health 2006, 96, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Pak-Gorstein, S.; Haq, A.; Graham, E. Cultural influences on infant feeding practices. Pediatrics Rev. 2009, 30, e11–e21. [Google Scholar] [CrossRef]
- Hunter-Adams, J.; Myer, L.; Rother, H.A. Perceptions related to breastfeeding and the early introduction of complementary foods amongst migrants in Cape Town, South Africa. Int. Breastfeed. J. 2019, 11, 29. [Google Scholar] [CrossRef]
- Brenne, S.; Breckenkamp, J.; David, M.; Brode, T.; Razum, O. Influence of a migration background on the implementation of breastfeeding and premature weaning. Z. Geburtshilfe Neonatol. 2018, 222, 254–261. [Google Scholar] [CrossRef]
- Abubakar, M.; Rodrigues, C.; Fonseca, M.; Santos, A.; Barros, H. Effect of maternal country of birth on breastfeeding practices: Results from Portuguese GXXI birth cohort. Int. Breastfeed. J. 2018, 13, 15. [Google Scholar] [CrossRef]
- Cohen, S.; Alexander, D.; Krebs, N.; Young, B.; Cabana, M.; Erdmann, P. Factors associated with breastfeeding initiation and continuation: A meta-analysis. J. Pediatrics 2018, 203, 190–196. [Google Scholar] [CrossRef]
- Ogbo, F.; Vijaybhai, M.; Awosemo, A.; Olusanya, B.; Olusanya, J.; Osuagwu, U. Regional prevalence and determinants of exclusive breastfeeding in India. Int. Breastfeed. J. 2019, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Chen, Z.; Yu, M.; Hui, F.; Tian, C.; Jia, L. What is the impact of rural-to-urban migration on exclusive breastfeeding: A population-based cross-sectional study. Int. Breastfeed. J. 2020, 15, 86. [Google Scholar] [CrossRef]
- Celi, A.; Rich-Edwards, J.; Richardson, M.; Kleinman, K.; Gillman, M. Immigration, race/ethnicity, and social and economic factors as predictors of breastfeeding initiation. Arch. Pediatrics Adolesc. Med. 2005, 159, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Pitikultang, S.; Khin, M.; Siri, S.; Taechaboonsermsak, P. Six-month exclusive breastfeeding among Myanmar migrants in Samut Sakhon Province, Thailand. Southeast Asian J. Trop. Med. Public Health 2017, 48, 662–673. [Google Scholar]
- Khanlou, N.; Haque, N.; Skinner, A.; Mantini, A.; Kurtz, C. Scoping Review on Maternal Health among Immigrant and Refugee Women in Canada: Prenatal, Intrapartum, and Postnatal Care. J. Pregnancy 2017, 2017, 8783294. [Google Scholar] [CrossRef] [PubMed]
- Lisi, C.; Freitas, C.; Barros, H. Maternal country of birth and in-hospital exclusive breastfeeding: Results from a Portuguese study. Eur. J. Public Health 2019, 29, ckz186.068. [Google Scholar] [CrossRef]

{kind=link}
| Variable | n = 173 |
|---|---|
| Age | |
| <35 years old | 118 (68.2) |
| ≥35 years old | 55 (31.8) |
| Marital status | |
| Married or common-law partner | 37 (21.4) |
| Single | 136 (78.6) |
| Educational attainment | |
| ≤12 years | 39 (22.5) |
| >12 years | 134 (77.5) |
| Parity (number of live births) | |
| 1 | 75 (43.4) |
| 2 | 58 (33.5) |
| ≥3 | 40 (23.1) |
| Residency in Chile | |
| ≤12 months | 32 (18.5) |
| >12 months | 141(81.5) |
| Immigration status | |
| Undocumented | 36 (20.8) |
| Permanent residency | 137 (79.2) |
| Employed | |
| Yes | 130 (75.1) |
| No | 43 (24.9) |
| Limited Spanish proficiency | |
| Yes | 114 (65.9) |
| No | 59 (34.1) |
| Access to basic services | |
| Yes | 136 (78.6) |
| No | 37 (21.4) |
| Weight status | |
| Normal | 55 (31.8) |
| Overnutrition | 118 (68.2) |
| Knowledge of breastfeeding | |
| Score < 8 | 47 (27.2) |
| Score ≥ 8 | 126 (72.8) |
| Exclusive breastfeeding | |
| <6 months | 79 (45.7) |
| ≥6 months | 94 (54.3) |
| Variable | NEBF (n = 79) | EBF (n = 94) | p |
|---|---|---|---|
| Age | |||
| <35 years old | 51 (64.6) | 67 (71.3) | 0.413 |
| ≥35 years old | 28 (35.4) | 27 (28.7) | |
| Marital status | |||
| Married or common-law partner | 14 (17.7) | 23 (24.5) | 0.353 |
| Single | 65 (82.3) | 71 (75.5) | |
| Educational attainment | |||
| ≤12 years | 24 (30.4) | 15 (15.9) | 0.029 |
| >12 years | 55 (69.6) | 79 (84.1) | |
| Parity (number of live births) | |||
| 1 | 33 (41.8) | 42 (44.7) | 0.250 |
| 2 | 28 (35.4) | 30 (31.9) | |
| ≥3 | 18 (22.8) | 22 (23.4) | |
| Residency in Chile | |||
| ≤12 months | 21 (26.6) | 11 (11.7) | 0.018 |
| >12 months | 58 (73.4) | 83 (88.3) | |
| Immigration status | |||
| Undocumented | 23 (29.1) | 13 (13.8) | 0.008 |
| Permanent residency | 56 (70.9) | 81 (86.2) | |
| Employed | |||
| Yes | 53 (67.1) | 77 (81.9) | 0.034 |
| No | 26 (32.9) | 17 (18.1) | |
| Limited Spanish proficiency | |||
| Yes | 45 (57.0) | 69 (73.4) | 0.025 |
| No | 34 (43.0) | 25 (26.6) | |
| Access to basic services | |||
| Yes | 57 (72.2) | 79 (84.0) | 0.065 |
| No | 22 (27.8) | 15 (16.0) | |
| Nutritional status | |||
| Normal | 24 (30.4) | 31 (33.0) | 0.745 |
| Overnutrition | 55 (69.6) | 63 (67.0) | |
| Knowledge of breastfeeding | |||
| Score < 8 | 28 (35.4) | 19 (20.2) | 0.027 |
| Score ≥ 8 | 51 (64.6) | 75 (79.8) | |
| Independent Variable | OR Raw (95% CI) | OR Adjusted (95% CI) |
|---|---|---|
| Risk factors | ||
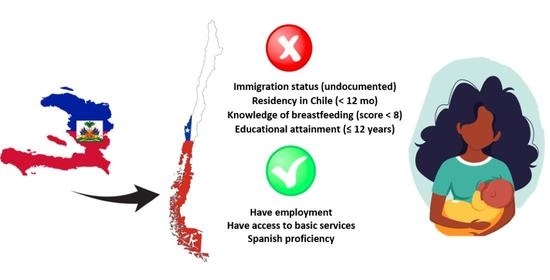
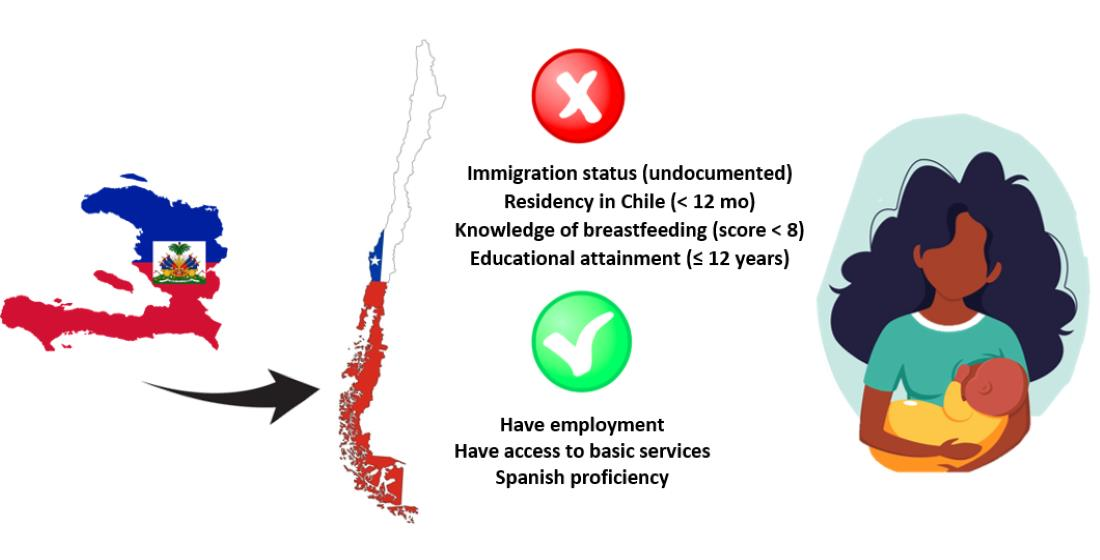
| Immigration status (undocumented) | 2.56 (1.21–5.52) | 2.34 (2.18–2.83) |
| Residency in Chile (<12 months) | 2.76 (1.22–6.13) | 2.23 (2.09–2.78) |
| Knowledge of breastfeeding (score < 8) | 2.17 (1.11–4.33) | 1.96 (1.81–2.27) |
| Educational attainment (≤12 years) | 2.29 (1.15–4.84) | 1.78 (1.61–2.11) |
| Protective factors | ||
| Have employment | 0.45 (0.22–0.91) | 0.36 (0.28–0.40) |
| Have access to basic services | 0.49 (0.23–1.03) | 0.32 (0.22–0.48) |
| Spanish proficiency | 0.48 (0.25–0.91) | 0.29 (0.20–0.51) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Fernández, A.; Sanhueza-Riquelme, X.; Cárcamo-Vargas, G.; Parra-Flores, J.; Rojas-Rodríguez, A.L.; Fuente, M.R.-D.l.; Maury-Sintjago, E. Maternal Factors Associated with Non-Exclusive Breastfeeding in Haitian Immigrant Women in Southern Chile. Nutrients 2022, 14, 3173. https://doi.org/10.3390/nu14153173
Rodríguez-Fernández A, Sanhueza-Riquelme X, Cárcamo-Vargas G, Parra-Flores J, Rojas-Rodríguez AL, Fuente MR-Dl, Maury-Sintjago E. Maternal Factors Associated with Non-Exclusive Breastfeeding in Haitian Immigrant Women in Southern Chile. Nutrients. 2022; 14(15):3173. https://doi.org/10.3390/nu14153173
Chicago/Turabian StyleRodríguez-Fernández, Alejandra, Ximena Sanhueza-Riquelme, Gloria Cárcamo-Vargas, Julio Parra-Flores, Ana Lizette Rojas-Rodríguez, Marcela Ruíz-De la Fuente, and Eduard Maury-Sintjago. 2022. "Maternal Factors Associated with Non-Exclusive Breastfeeding in Haitian Immigrant Women in Southern Chile" Nutrients 14, no. 15: 3173. https://doi.org/10.3390/nu14153173
APA StyleRodríguez-Fernández, A., Sanhueza-Riquelme, X., Cárcamo-Vargas, G., Parra-Flores, J., Rojas-Rodríguez, A. L., Fuente, M. R.-D. l., & Maury-Sintjago, E. (2022). Maternal Factors Associated with Non-Exclusive Breastfeeding in Haitian Immigrant Women in Southern Chile. Nutrients, 14(15), 3173. https://doi.org/10.3390/nu14153173