
Preterm Infants on Early Solid Foods and Vitamin D Status in the First Year of Life—A Secondary Outcome Analysis of a Randomized Controlled Trial

 , , , , ,
, , , , , 
Abstract
:
1. Introduction
2. Materials and Methods
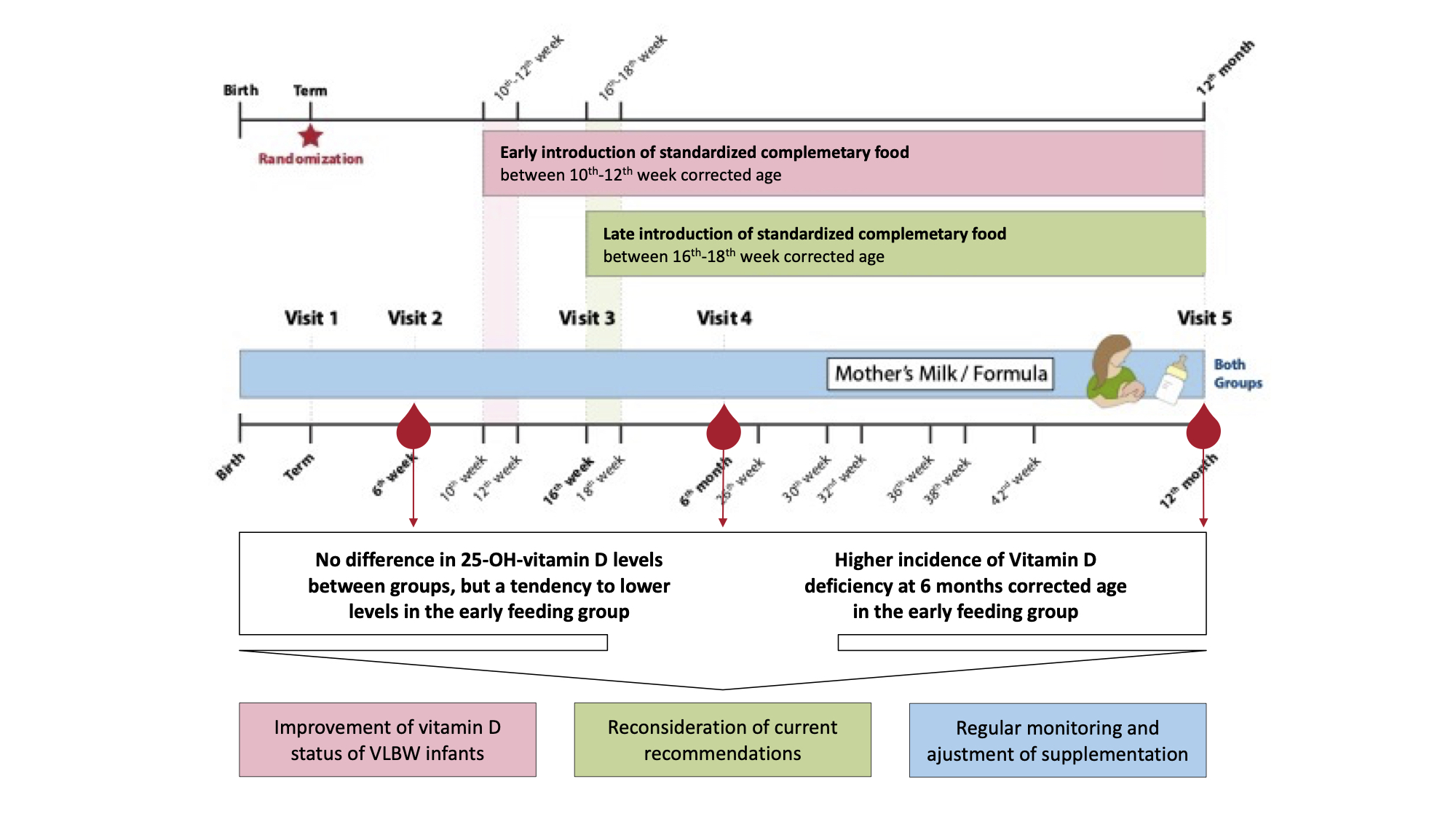
2.1. Study Visits
2.2. Statistical Analysis
3. Results
3.1. Screening and Participants
3.2. Baseline Characteristics and Neonatal Morbidity
3.3. Primary Outcome
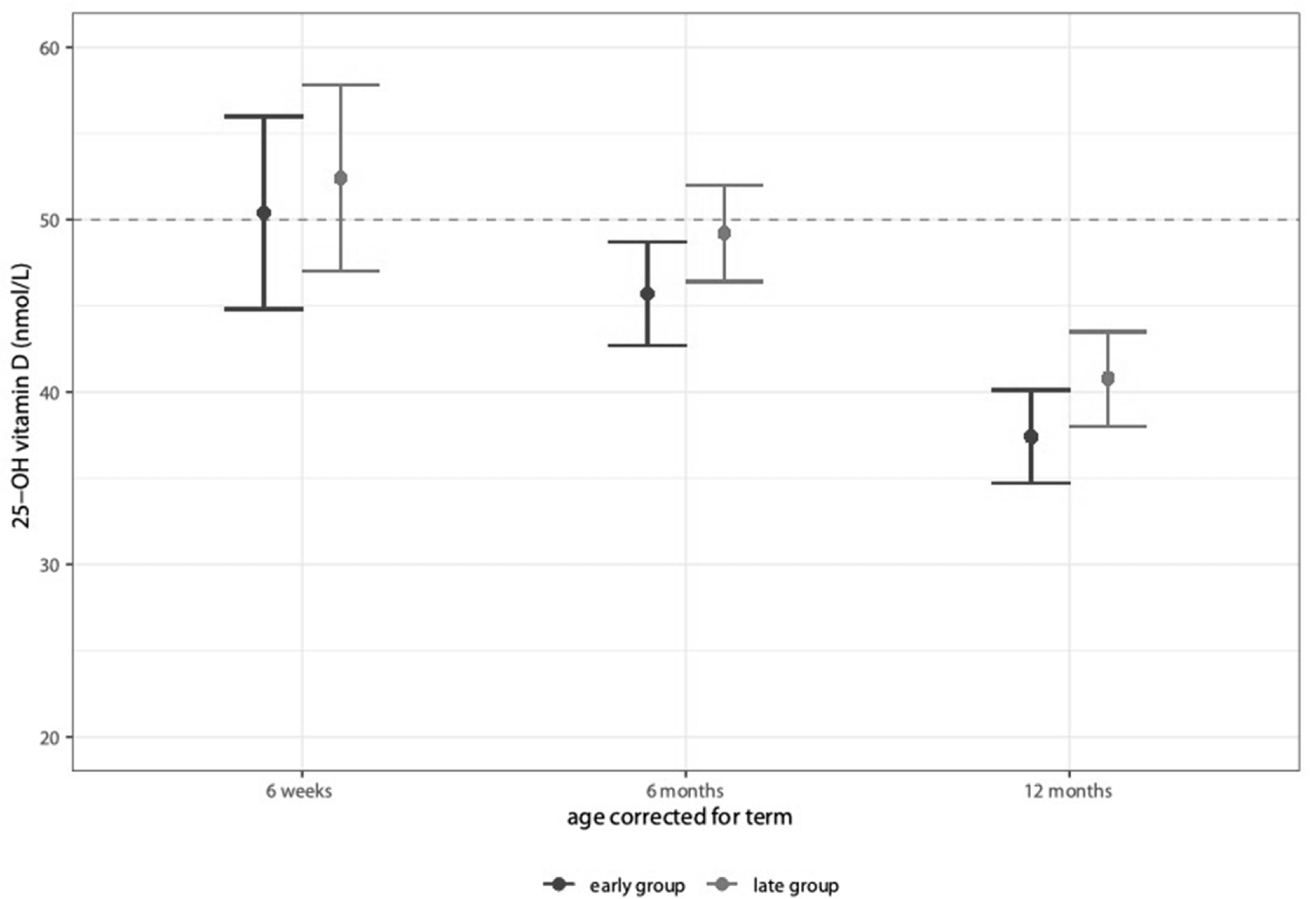
3.4. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ellis, K.; Shypailo, R.; Schanler, R. Body composition of the preterm infant. Ann. Hum. Biol. 1994, 21, 533–545. [Google Scholar] [CrossRef]
- Basile, L.A.; Taylor, S.N.; Wagner, C.L.; Quinones, L.; Hollis, B.W. Neonatal vitamin D status at birth at latitude 32°72′: Evidence of deficiency. J. Perinatol. 2007, 27, 568–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burris, H.H.; Van Marter, L.J.; McElrath, T.F.; Tabatabai, P.; Litonjua, A.A.; Weiss, S.T.; Christou, H. Vitamin D status among preterm and full-term infants at birth. Pediatr. Res. 2013, 75, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Cadario, F.; Savastio, S.; Pozzi, E.; Capelli, A.; Dondi, E.; Gatto, M.; Zaffaroni, M.; Bona, G. Vitamin D status in cord blood and newborns: Ethnic differences. Ital. J. Pediatr. 2013, 39, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinkhuyzen, A.A.; Eyles, D.W.; Burne, T.H.; Blanken, L.M.; Kruithof, C.J.; Verhulst, F.; Jaddoe, V.W.; Tiemeier, H.; McGrath, J.J. Prevalence and predictors of vitamin D deficiency based on maternal mid-gestation and neonatal cord bloods: The Generation R Study. J. Steroid Biochem. Mol. Biol. 2016, 164, 161–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiely, M.; O’Donovan, S.M.; Kenny, L.C.; Hourihane, J.O.; Irvine, A.D.; Murray, D.M. Vitamin D metabolite concentrations in umbilical cord blood serum and associations with clinical characteristics in a large prospective mother-infant cohort in Ireland. J. Steroid Biochem. Mol. Biol. 2017, 167, 162–168. [Google Scholar] [CrossRef]
- Abrams, S.A. Vitamin D and bone minerals in neonates. Early Hum. Dev. 2021, 162, 105461. [Google Scholar] [CrossRef] [PubMed]
- Lykkedegn, S.; Sorensen, G.L.; Beck-Nielsen, S.S.; Christesen, H.T. The impact of vitamin D on fetal and neonatal lung maturation. A systematic review. Am. J. Physiol. Cell. Mol. Physiol. 2015, 308, L587–L602. [Google Scholar] [CrossRef]
- Hibbs, A.M.; Ross, K.; Kerns, L.A.; Wagner, C.; Fuloria, M.; Groh-Wargo, S.; Zimmerman, T.; Minich, N.; Tatsuoka, C. Effect of Vitamin D Supplementation on Recurrent Wheezing in Black Infants Who Were Born Preterm: The D-Wheeze Randomized Clinical Trial. JAMA 2018, 319, 2086–2094. [Google Scholar] [CrossRef] [PubMed]
- Marino, R.; Misra, M. Extra-Skeletal Effects of Vitamin D. Nutrients 2019, 11, 1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aly, H.; Mohsen, L.; Bhattacharjee, I.; Malash, A.; Atyia, A.; Elanwary, S.; El Hawary, R. Vitamin D Supplementation and T Cell Regulation in Preterm Infants: A Randomized Controlled Trial. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Cheah, F.-C.; Domellöf, M.; van Goudoever, J.B.; Poindexter, B.B.; Vain, N. Scientific Basis and Practical Application of Nutritional Care for Preterm Infants. World Rev. Nutr. Diet. 2021, 122, XIII–XIV. [Google Scholar] [CrossRef]
- Abrams, S.A.; The Committee on Nutrition; Bhatia, J.J.S.; Corkins, M.R.; De Ferranti, S.D.; Golden, N.H.; Silverstein, J. Calcium and Vitamin D Requirements of Enterally Fed Preterm Infants. Pediatrics 2013, 131, e1676–e1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrams, S.A. Vitamin D in Preterm and Full-Term Infants. Ann. Nutr. Metab. 2020, 76 (Suppl. 2), 6–14. [Google Scholar] [CrossRef] [PubMed]
- Zung, A.; Topf-Olivestone, C.; Shinwell, E.S.; Hofi, L.; Juster-Reicher, A.; Flidel-Rimon, O. Reassessing vitamin D supplementation in preterm infants: A prospective study and review of the literature. J. Pediatr. Endocrinol. Metab. 2020, 33, 1273–1281. [Google Scholar] [CrossRef]
- Fort, P.; Salas, A.A.; Nicola, T.; Craig, C.M.; Carlo, W.A.; Ambalavanan, N. A Comparison of 3 Vitamin D Dosing Regimens in Extremely Preterm Infants: A Randomized Controlled Trial. J. Pediatr. 2016, 174, 132–138.e1. [Google Scholar] [CrossRef] [Green Version]
- Hanson, C.; Jones, G.; Lyden, E.; Kaufmann, M.; Armas, L.; Anderson-Berry, A. Vitamin D metabolism in the premature newborn: A randomized trial. Clin. Nutr. 2016, 35, 835–841. [Google Scholar] [CrossRef]
- Jung, J.-H.; Kim, E.-A.; Lee, S.-Y.; Moon, J.-E.; Lee, E.-J.; Park, S.-H. Vitamin D Status and Factors Associated with Vitamin D Deficiency during the First Year of Life in Preterm Infants. Nutrients 2021, 13, 2019. [Google Scholar] [CrossRef] [PubMed]
- Hooven, E.H.V.D.; Gharsalli, M.; Heppe, D.H.M.; Raat, H.; Hofman, A.; Franco, O.H.; Rivadeneira, F.; Jaddoe, V.W.V. Associations of breast-feeding patterns and introduction of solid foods with childhood bone mass: The Generation R Study. Br. J. Nutr. 2016, 115, 1024–1032. [Google Scholar] [CrossRef] [Green Version]
- Haiden, N.; Thanhaeuser, M.; Eibensteiner, F.; Huber-Dangl, M.; Gsoellpointner, M.; Ristl, R.; Kroyer, B.; Brandstetter, S.; Kornsteiner-Krenn, M.; Binder, C.; et al. Randomized Controlled Trial of Two Timepoints for Introduction of Standardized Complementary Food in Preterm Infants. Nutrients 2022, 14, 697. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.; Cole, C.R.; Hansen, N.I.; Duncan, A.F.; Hintz, S.R.; Adams-Chapman, I.; Eunice Kennedy Shriver National Institute of Child Health; Human Development Neonatal Research Network. Neurodevelopmental and Growth Outcomes of Extremely Preterm Infants with Short Bowel Syndrome. J. Pediatr. 2020, 230, 76–83.e5. [Google Scholar] [CrossRef] [PubMed]
- Strobel, K.M.; Purdy, I.; Romero, T.; Calkins, K.L. Growth from Birth to 30 months for Infants Born with Congenital Gastrointestinal Anomalies and Disorders. Am. J. Perinatol. 2020, 38, e33–e38. [Google Scholar] [CrossRef] [PubMed]
- Taminiau, J.A. Review article: The clinical importance of growth in children with inflammatory bowel disease: Is it important to the gastroenterologist? Aliment. Pharmacol. Ther. 2007, 26 (Suppl. 2), 53–56. [Google Scholar] [CrossRef]
- Poindexter, B.B.; Martin, C.R. Impact of Nutrition on Bronchopulmonary Dysplasia. Clin. Perinatol. 2015, 42, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Karpen, H.E. Nutrition in the Cardiac Newborns: Evidence-based Nutrition Guidelines for Cardiac Newborns. Clin. Perinatol. 2016, 43, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayannavar, A.; Calabria, A.C. Screening for Metabolic Bone Disease of prematurity. Semin. Fetal Neonatal Med. 2020, 25, 101086. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.N.; Wahlquist, A.; Wagner, C.L.; Ramakrishnan, V.; Ebeling, M.; Hollis, B.W. Functional indicators of vitamin D adequacy for very low birth weight infants. J. Perinatol. 2018, 38, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Chinoy, A.; Mughal, M.Z.; Padidela, R. Metabolic bone disease of prematurity: Causes, recognition, prevention, treatment and long-term consequences. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F560–F566. [Google Scholar] [CrossRef]
- Czech-Kowalska, J. Mineral and nutritional requirements of preterm infant. Semin. Fetal Neonatal Med. 2020, 25, 101071. [Google Scholar] [CrossRef]
- Artman, A.; Huang, A.; Bowker, R.; Cerwinske, L.; Cooper, S.; Johnson, T.; Patel, A.L. Evaluation of vitamin D protocol in the neonatal intensive care unit at Rush University Medical Center. J. Parenter. Enter. Nutr. 2021, 46, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Kołodziejczyk-Nowotarska, A.; Bokiniec, R.; Seliga-Siwecka, J. Monitored Supplementation of Vitamin D in Preterm Infants: A Randomized Controlled Trial. Nutrients 2021, 13, 3442. [Google Scholar] [CrossRef]
- Palacios, C.; Kostiuk, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2019, 7, CD008873. [Google Scholar] [CrossRef]
- Hossein-Nezhad, A.; Holick, M.F. Vitamin D for Health: A Global Perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Parameter | Early Group (n = 89) | Late Group (n = 88) |
|---|---|---|
| Obstetric and parental parameters | ||
| Multiple pregnancy | 32 (36) | 28 (31.8) |
| Cesarean delivery | 78 (87.6) | 84 (95.5) |
| Prenatal steroids (full course) | 47 (52.8) | 57 (64.8) |
| Premature rupture of membranes | 39 (43.8) | 39 (44.3) |
| Preeclampsia | 9 (10.1) | 8 (9.1) |
| Gestational diabetes | 3 (3.4) | 3 (3.4) |
| Smoking habits | ||
| Before pregnancy | 19 (21.3) | 14 (15.9) |
| During pregnancy | 3 (3.4) | 1 (1.1) |
| After pregnancy | 1 (1.1) | 2 (2.3) |
| Always | 9 (10.1) | 14 (15.9) |
| Age of mother at birth | 32.5 [±5] | 32.6 [±6.8] |
| Dark skin | 7 (7.9) | 4 (4.5) |
| Neonatal parameters | ||
| Male sex | 56 (62.9) | 42 (47.7) |
| Gestational age (days) | 190 [±16]–27 + 1 | 190 [±16]–27 + 1 |
| Birth weight (g) | 941 [±253] | 932 [±256] |
| Small for gestational age | 7 (7.9) | 5 (5.7) |
| Born in winter | 22 (24.7) | 16 (18.2) |
| Gestational age (days) at discharge | 265 [±12]–37 + 6 | 265 [±15]–37 + 6 |
| Breast milk feeding at discharge | 30 (33.7) | 21 (23.9) |
| Calcium-Phosphorus supplementation | ||
| CaPh suppl. after discharge | 16 (18) | 18 (20.5) |
| CaPh suppl. after discharge, days | 12.7 [±38.6] | 10.2 [±23.3] |
| Neonatal morbidity | ||
| NEC grade I and II | 4 (4.5) | 0 (0) |
| PDA | 34 (38.2) | 33 (37.5) |
| ROP ≥ grade III | 5 (5.6) | 5 (5.7) |
| IVH grade I and II | 9 (10.1) | 4 (4.5) |
| IVH grade ≥ grade III | 4 (4.5) | 6 (6.8) |
| PVL | 0 (0) | 2 (2.3) |
| Parameter | 6 Weeks Corrected Age | 6 Months Corrected Age | 12 Months Corrected Age | |||
|---|---|---|---|---|---|---|
| Early Group (n = 89) | Late Group (n = 88) | Early Group (n = 89) | Late Group (n = 88) | Early Group (n = 89) | Late Group (n = 88) | |
| Vitamin D intake by supplements (IE/day) | 656 (631–682) | 664 (638–689) | 649 (622–676) | 666 (640–692) | 598 (563–634) | 612 (576–647) |
| Vitamin D status | ||||||
| 25-OH-vitamin D (nmol/L) | 50.4 (44.8–56.0) | 52.4 (47.0–57.8) | 45.7 (42.7–48.7) | 49.2 (46.4–52.0) | 37.4 (34.7–40.1) | 40.8 (38.0–43.5) |
| Calcium (mmol/L) | 2.6 (2.5–2.7) | 2.6 (2.5–2.6) | 2.6 (2.6–2.6) | 2.6 (2.6–2.6) | 2.6 (2.5–2.6) | 2.6 (2.6–2.6) |
| Albumin (g/dL) | 3.5 (3.4–3.6) | 3.4 (3.4–3.5) | 4.1 (4.0–4.1) | 4.1 (4.1–4.2) | 4.2 (4.2–4.3) | 4.2 (4.1–4.3) |
| Calcium corrected (mmol/L) | 3.0 (2.9–3.1) | 3.0 (2.9–3.1) | 2.6 (2.5–2.6) | 2.5 (2.5–2.6) | 2.4 (2.3–2.4) | 2.4 (2.4–2.5) |
| Phosphorus (mmol/L) | 2.1 (2.1–2.2) | 2.2 (2.1–2.2) | 2.1 (2.0–2.1) | 2.1 (2.0–2.1) | 1.9 (1.9–2.0) | 2.0 (1.9–2.0) |
| PTH (pg/mL) | 35.7 (25.1–46.2) | 38.5 (28.3–48.6) | 29.7 (25.6–33.7) | 30.5 (26.8–34.3) | 29.4 (25.9–33.0) | 30.7 (27.1–34.4) |
| AP (U/L) | 310.3 (283–337) | 321.9 (296–348) | 234.4 (219–250) | 243.1 (229–258) | 293.8 (214–373) | 279.0 (196–362) |
| Incidence of vitamin D deficiency | ||||||
| Vitamin D deficiency | 41/76 (54%) | 45/79 (57%) | 47/70 (67%) * | 35/71 (49%) * | 58/65 (89%) | 50/62 (81%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thanhaeuser, M.; Eibensteiner, F.; Kornsteiner-Krenn, M.; Gsoellpointner, M.; Brandstetter, S.; Koeller, U.; Huf, W.; Huber-Dangl, M.; Binder, C.; Thajer, A.; et al. Preterm Infants on Early Solid Foods and Vitamin D Status in the First Year of Life—A Secondary Outcome Analysis of a Randomized Controlled Trial. Nutrients 2022, 14, 3105. https://doi.org/10.3390/nu14153105
Thanhaeuser M, Eibensteiner F, Kornsteiner-Krenn M, Gsoellpointner M, Brandstetter S, Koeller U, Huf W, Huber-Dangl M, Binder C, Thajer A, et al. Preterm Infants on Early Solid Foods and Vitamin D Status in the First Year of Life—A Secondary Outcome Analysis of a Randomized Controlled Trial. Nutrients. 2022; 14(15):3105. https://doi.org/10.3390/nu14153105
Chicago/Turabian StyleThanhaeuser, Margarita, Fabian Eibensteiner, Margit Kornsteiner-Krenn, Melanie Gsoellpointner, Sophia Brandstetter, Ursula Koeller, Wolfgang Huf, Mercedes Huber-Dangl, Christoph Binder, Alexandra Thajer, and et al. 2022. "Preterm Infants on Early Solid Foods and Vitamin D Status in the First Year of Life—A Secondary Outcome Analysis of a Randomized Controlled Trial" Nutrients 14, no. 15: 3105. https://doi.org/10.3390/nu14153105
APA StyleThanhaeuser, M., Eibensteiner, F., Kornsteiner-Krenn, M., Gsoellpointner, M., Brandstetter, S., Koeller, U., Huf, W., Huber-Dangl, M., Binder, C., Thajer, A., Jilma, B., Berger, A., & Haiden, N. (2022). Preterm Infants on Early Solid Foods and Vitamin D Status in the First Year of Life—A Secondary Outcome Analysis of a Randomized Controlled Trial. Nutrients, 14(15), 3105. https://doi.org/10.3390/nu14153105