
Preterm Infants on Early Solid Foods and Iron Status in the First Year of Life—A Secondary Outcome Analysis of a Randomized Controlled Trial

 , , , , , , ,
, , , , , , , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Visits
2.2. Statistical Analysis
3. Results
3.1. Screening and Participants
3.2. Baseline Characteristics and Neonatal Morbidity
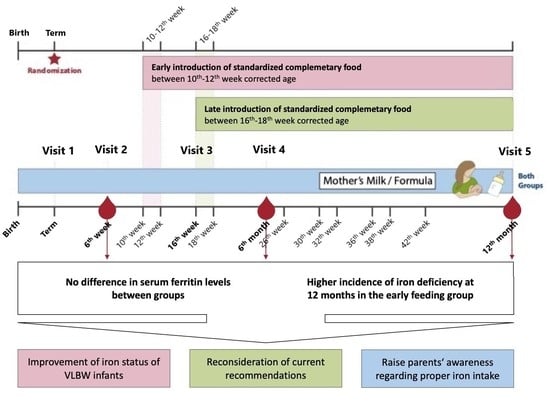
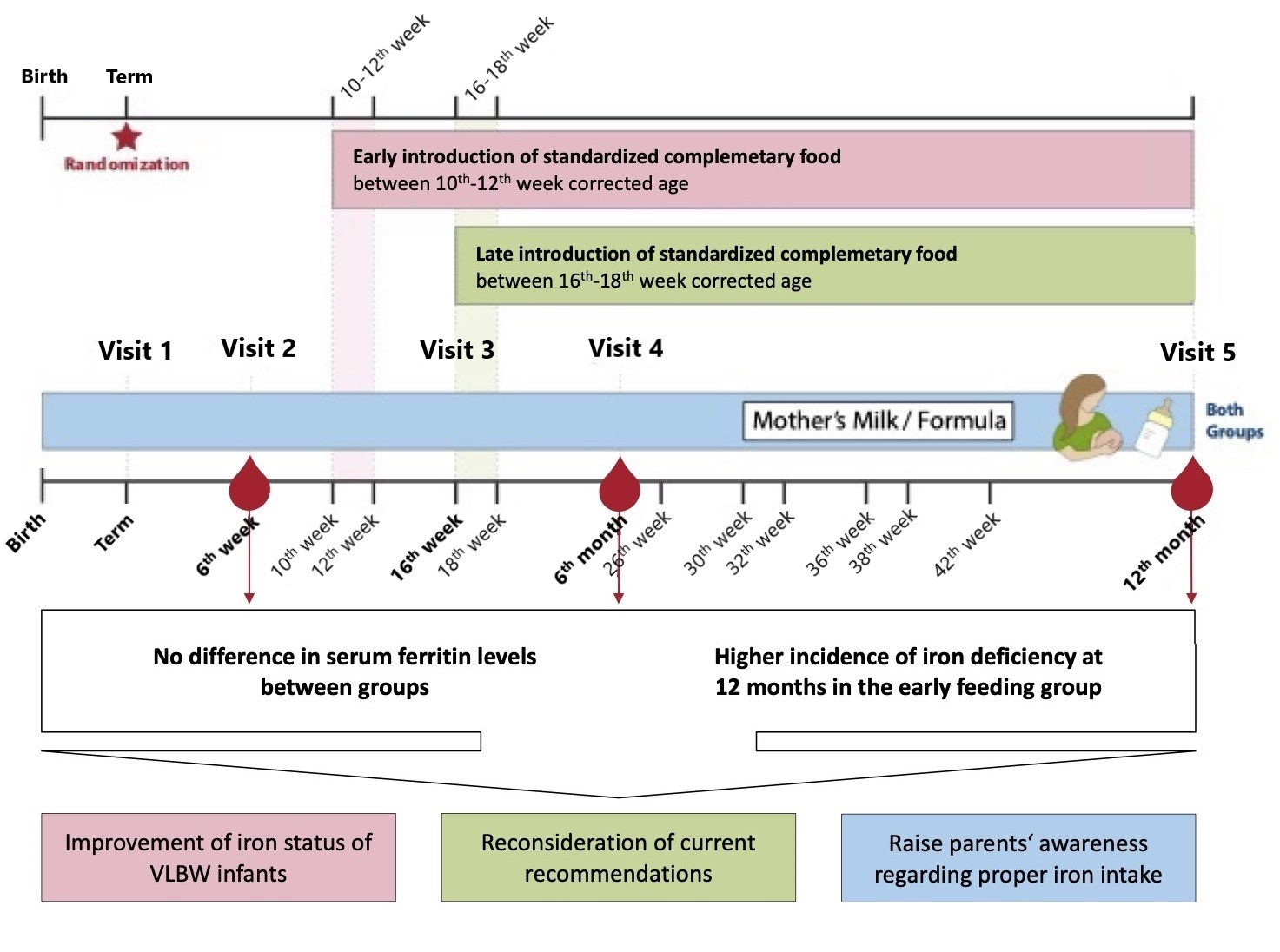
3.3. Primary Outcome
3.4. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moreno-Fernandez, J.; Ochoa, J.J.; Latunde-Dada, G.O.; Diaz-Castro, J. Iron Deficiency and Iron Homeostasis in Low Birth Weight Preterm Infants: A Systematic Review. Nutrients 2019, 11, 1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenz, L.; Peter, A.; Poets, C.F.; Franz, A.R. A Review of Cord Blood Concentrations of Iron Status Parameters to Define Reference Ranges for Preterm Infants. Neonatology 2013, 104, 194–202. [Google Scholar] [CrossRef]
- McCarthy, E.K.; Kenny, L.C.; Hourihane, J.O.B.; Irvine, A.D.; Murray, D.M.; Kiely, M.E. Impact of maternal, antenatal and birth-associated factors on iron stores at birth: Data from a prospective maternal-infant birth cohort. Eur. J. Clin. Nutr. 2017, 71, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Lozoff, B.; Beard, J.; Connor, J.; Felt, B.; Georgieff, M.; Schallert, T. Long-Lasting Neural and Behavioral Effects of Iron Deficiency in Infancy. Nutr. Rev. 2006, 64, 34–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lozoff, B. Iron deficiency and child development. Food Nutr. Bull. 2007, 28, S560–S571. [Google Scholar] [CrossRef] [PubMed]
- German, K.R.; Juul, S.E. Iron and Neurodevelopment in Preterm Infants: A Narrative Review. Nutrients 2021, 13, 3737. [Google Scholar] [CrossRef] [PubMed]
- Domellof, M. Microminerals: Iron, Zinc, Copper, Selenium, Manganese, Iodine, Chromium and Molybdenum. World Rev. Nutr. Diet. 2021, 122, 140–148. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, E.K.; Dempsey, E.M.; Kiely, M.E. Iron supplementation in preterm and low-birth-weight infants: A systematic review of intervention studies. Nutr. Rev. 2019, 77, 865–877. [Google Scholar] [CrossRef]
- Haiden, N.; Klebermass, K.; Cardona, F.; Schwindt, J.; Berger, A.; Kohlhauser-Vollmuth, C.; Jilma, B.; Pollak, A. A randomized, controlled trial of the effects of adding vitamin B12 and folate to erythropoietin for the treatment of anemia of prematurity. Pediatrics 2006, 118, 180–188. [Google Scholar] [CrossRef]
- Haiden, N. Erythropoetin in neonatology. Mon. Kinderheilkd. 2007, 12, 1131–1136. [Google Scholar] [CrossRef]
- Domellöf, M. Meeting the Iron Needs of Low and Very Low Birth Weight Infants. Ann. Nutr. Metab. 2017, 71, 16–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonsdottir, O.H.; Thorsdottir, I.; Hibberd, P.L.; Fewtrell, M.S.; Wells, J.C.; Palsson, G.I.; Lucas, A.; Gunnlaugsson, G.; Kleinman, R.E. Timing of the Introduction of Complementary Foods in Infancy: A Randomized Controlled Trial. Pediatrics 2012, 130, 1038–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haiden, N.; Thanhaeuser, M.; Eibensteiner, F.; Huber-Dangl, M.; Gsoellpointner, M.; Ristl, R.; Kroyer, B.; Brandstetter, S.; Kornsteiner-Krenn, M.; Binder, C.; et al. Randomized Controlled Trial of Two Timepoints for Introduction of Standardized Complementary Food in Preterm Infants. Nutrients 2022, 14, 697. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.; Cole, C.R.; Hansen, N.I.; Duncan, A.F.; Hintz, S.R.; Adams-Chapman, I. Eunice Kennedy Shriver National Institute of Child, H.; Human Development Neonatal Research, N. Neurodevelopmental and Growth Outcomes of Extremely Preterm Infants with Short Bowel Syndrome. J. Pediatr. 2021, 230, 76–83.e75. [Google Scholar] [CrossRef]
- Strobel, K.M.; Purdy, I.; Romero, T.; Calkins, K.L. Growth from Birth to 30 months for Infants Born with Congenital Gastrointestinal Anomalies and Disorders. Am. J. Perinatol. 2021, 38, e33–e38. [Google Scholar] [CrossRef]
- Taminiau, J.A. Review article: The clinical importance of growth in children with inflammatory bowel disease: Is it important to the gastroenterologist? Aliment. Pharmacol. Ther. 2007, 26 (Suppl. S2), 53–56. [Google Scholar] [CrossRef]
- Poindexter, B.B.; Martin, C.R. Impact of Nutrition on Bronchopulmonary Dysplasia. Clin. Perinatol. 2015, 42, 797–806. [Google Scholar] [CrossRef]
- Karpen, H.E. Nutrition in the Cardiac Newborns: Evidence-based Nutrition Guidelines for Cardiac Newborns. Clin. Perinatol. 2016, 43, 131–145. [Google Scholar] [CrossRef]
- Shannon, K.M.; Keith, J.F., 3rd; Mentzer, W.C.; Ehrenkranz, R.A.; Brown, M.S.; Widness, J.A.; Gleason, C.A.; Bifano, E.M.; Millard, D.D.; Davis, C.B.; et al. Recombinant human erythropoietin stimulates erythropoiesis and reduces erythrocyte transfusions in very low birth weight preterm infants. Pediatrics 1995, 95, 1–8. [Google Scholar] [CrossRef]
- Haiden, N.; Schwindt, J.; Cardona, F.; Berger, A.; Klebermass, K.; Wald, M.; Kohlhauser-Vollmuth, C.; Jilma, B.; Pollak, A. Effects of a combined therapy of erythropoietin, iron, folate, and vitamin B12 on the transfusion requirements of extremely low birth weight infants. Pediatrics 2006, 118, 2004–2013. [Google Scholar] [CrossRef]
- Dewey, K.G.; Cohen, R.J.; Rivera, L.L.; Brown, K.H. Effects of age of introduction of complementary foods on iron status of breast-fed infants in Honduras. Am. J. Clin. Nutr. 1998, 67, 878–884. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Agarwal, R.; Aggarwal, K.C.; Chellani, H.; Duggal, A.; Arya, S.; Bhatia, S.; Sankar, M.J.; Sreenivas, V.; Jain, V.; et al. Complementary feeding at 4 versus 6 months of age for preterm infants born at less than 34 weeks of gestation: A randomised, open-label, multicentre trial. Lancet Glob. Health 2017, 5, e501–e511. [Google Scholar] [CrossRef] [Green Version]
- Cooke, R.J.; Griffin, I. Iron Balance and Iron Nutritional Status in Preterm Infants During the First 4 m of Life. J. Pediatr. Gastroenterol. Nutr. 2021. Publish Ahead of Print. [Google Scholar] [CrossRef] [PubMed]
- Ruangkit, C.; Prachakittikul, N.; Hemprachitchai, N.; Dumrongwongsiri, O.; Soonsawad, S. Association of Infant Feeding Practices with Iron Status and Hematologic Parameters in 6-Month-Old Infants. Children 2021, 8, 1159. [Google Scholar] [CrossRef] [PubMed]
- Domellöf, M.; Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Fewtrell, M.; Hojsak, I.; Mihatsch, W.; Molgaard, C.; Shamir, R.; et al. Iron requirements of infants and toddlers. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 119–129. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Parameter | Early Group (n = 89) | Late Group (n = 88) |
|---|---|---|
| Obstetric and parental parameters | ||
| Multiple pregnancy | 32 (36) | 28 (31.8) |
| Cesarean delivery | 78 (87.6) | 84 (95.5) |
| Prenatal steroids (full course) | 47 (52.8) | 57 (64.8) |
| Premature rupture of membranes | 39 (43.8) | 39 (44.3) |
| Preeclampsia | 9 (10.1) | 8 (9.1) |
| Gestational diabetes | 3 (3.4) | 3 (3.4) |
| IGDM | 1 (1.1) | 2 (2.3) |
| Smoking habits | ||
| Before pregnancy | 19 (21.3) | 14 (15.9) |
| During pregnancy | 3 (3.4) | 1 (1.1) |
| After pregnancy | 1 (1.1) | 2 (2.3) |
| Always | 9 (10.1) | 14 (15.9) |
| Age of mother at birth | 32.5 [±5] | 32.6 [±6.8] |
| Neonatal parameters | ||
| Male sex | 56 (62.9) | 42 (47.7) |
| Gestational age (days) | 190 [±16] − 27 + 1 | 190 [±16] − 27 + 1 |
| Birth weight (g) | 941 [±253] | 932 [±256] |
| Small for gestational age | 7 (7.9) | 5 (5.7) |
| Gestational age (days) at discharge | 265 [±12] − 37 + 6 | 265 [±15] − 37 + 6 |
| Breast milk feeding at discharge | 30 (33.7) | 21 (23.9) |
| Before discharge | ||
| Anemia | 77 (86.5) | 82 (93.2) |
| Number of PRBC | 3.3 [±4] | 3.1 [±4] |
| Erythropoietin therapy | 62 (69.7) | 75 (85.2) |
| Neonatal morbidity | ||
| NEC grade I and II | 4 (4.5) | 0 (0) |
| PDA | 34 (38.2) | 33 (37.5) |
| ROP ≥ grade III | 5 (5.6) | 5 (5.7) |
| IVH grade I and II | 9 (10.1) | 4 (4.5) |
| IVH grade ≥ grade III | 4 (4.5) | 6 (6.8) |
| PVL | 0 (0) | 2 (2.3) |
| Parameter | 6 Weeks Corrected Age | 6 Months Corrected Age | 12 Months Corrected Age | |||
|---|---|---|---|---|---|---|
| Early Group (n = 89) | Late Group (n = 88) | Early Group (n = 89) | Late Group (n = 88) | Early Group (n = 89) | Late Group (n = 88) | |
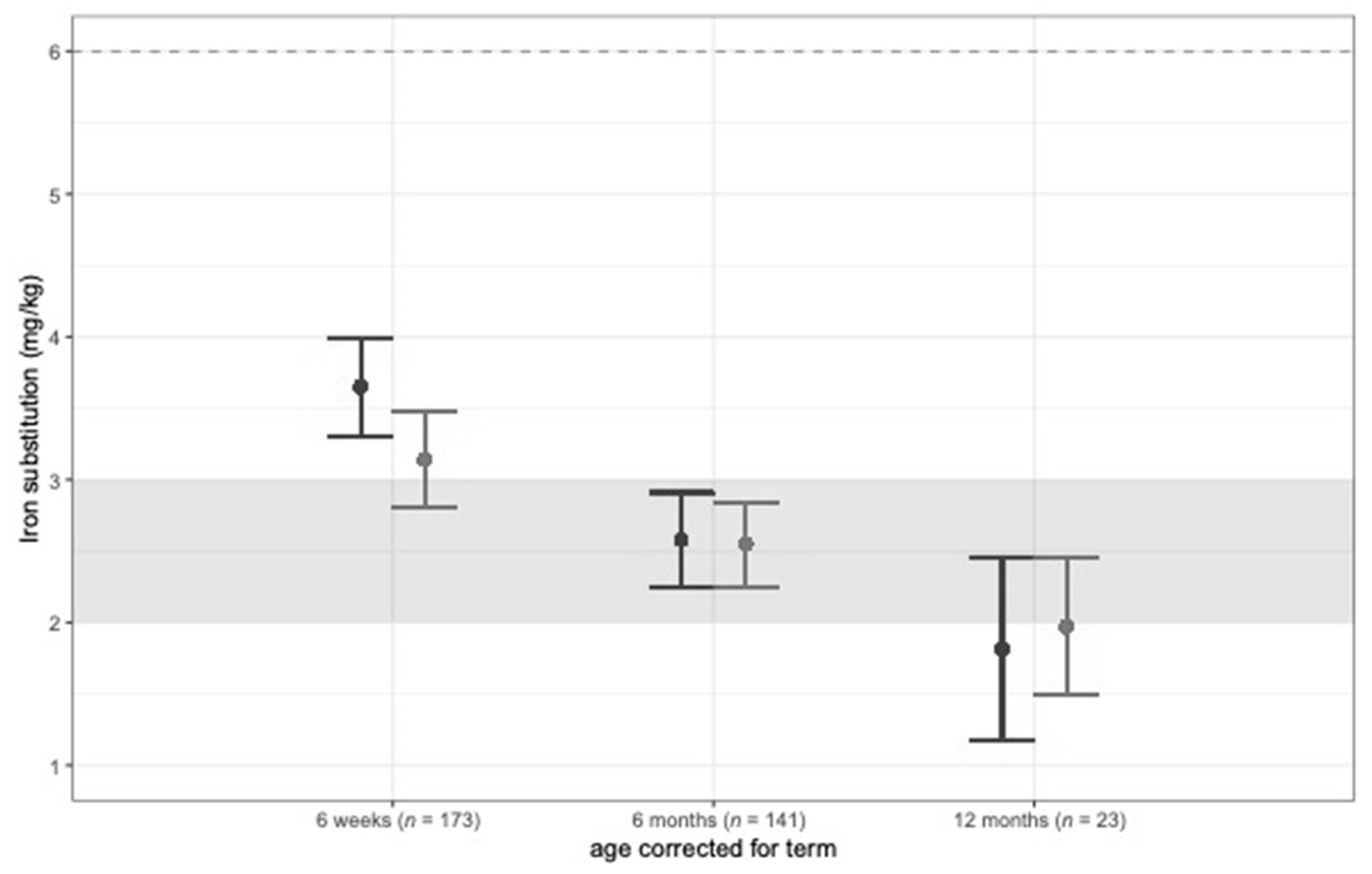
| Iron intake by supplements (mg/kg/d) | 3.7 (3.3–4.0) * | 3.1 (2.8–3.5) * | 2.6 (2.3–2.9) | 2.6 (2.3–2.8) | 1.8 (1.2–2.5) | 2.0 (1.5–2.5) |
| Hematologic parameters | ||||||
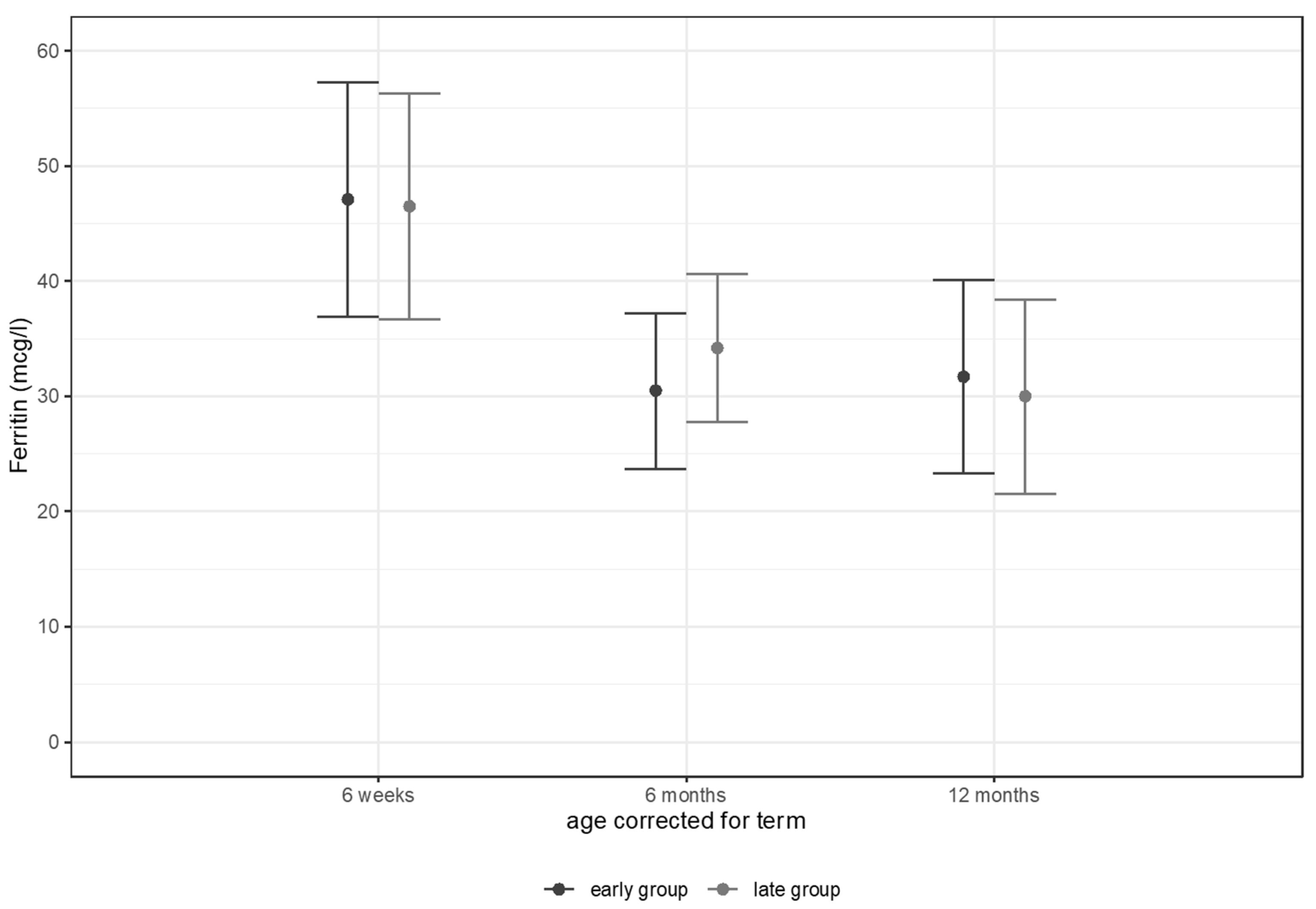
| Ferritin (mcg/L) | 47.1 (36.9–57.3) | 46.5 (36.7–56.3) | 30.5 (23.7–37.2) | 34.2 (27.8–40.6) | 31.7 (23.3–40.1) | 30.0 (21.5–38.4) |
| Hemoglobin (g/dL) | 10.9 (10.6–11.1) * | 11.2 (11.0–11.4) * | 12.2 (12.0–12.4) | 12.3 (12.1–12.5) | 12.3 (12.1–12.5) | 12.3 (12.1–12.5) |
| Hematocrit (%) | 31.4 (30.7–32.0) | 32.3 (31.6–32.9) | 34.6 (34.1–35.1) | 34.9 (34.4–35.4) | 35.3 (34.7–35.8) | 35.3 (34.7–35.9) |
| RBC (/pl) | 4.0 (4.0–4.1) | 4.2 (4.1–4.3) | 4.7 (4.6–4.8) | 4.7 (4.6–4.8) | 4.8 (4.7–4.9) | 4.7 (4.6–4.8) |
| MCV (fl) | 78.5 (77.5–79.4) | 78.1 (77.3–79.0) | 74.4 (73.5–75.3) | 74.3 (73.5–75.2) | 74.5 (73.5–75.4) | 74.9 (73.9–75.9) |
| MCH (pg) | 27.1 (26.8–27.5) | 27.2 (26.9–27.5) | 26.2 (25.8–26.6) | 26.2 (25.9–26.6) | 26.0 (25.5–26.4) | 26.0 (25.6–26.5) |
| MCHC (g/dL) | 34.6 (34.3–34.8) | 34.8 (34.5–35.0) | 35.2 (34.9–35.6) | 35.1 (34.8–35.4) | 34.8 (34.6–35.1) | 34.8 (34.5–35.0) |
| Reticulocytes relative (‰) | 17.0 (15.3–18.7) | 15.3 (13.6–17.0) | 10.8 (10.0–11.7) | 10.5 (9.7–11.3) | 10.0 (9.0–11.0) | 9.4 (8.3–10.4) |
| Transferrin (g/L) | 2.4 (2.3–2.5) | 2.5 (2.4–2.6) | 2.6 (2.5–2.7) | 2.6 (2.5–2.7) | 2.9 (2.8–3.0) | 2.7 (2.6–2.8) |
| sTRF (mg/L) | 1.6 (1.5–1.7) | 1.7 (1.5–1.8) | 1.7 (1.5–1.8) | 1.6 (1.5–1.8) | 1.7 (1.6–1.8) | 1.8 (1.7–1.9) |
| Iron (mcg/dL) | 85.4 (75.9–94.8) | 89.1 (79.9–98.3) | 70.5 (63.7–77.2) | 72.9 (66.4–79.3) | 60.7 (53.3–68.1) | 64.4 (56.9–71.9) |
| Transferrin saturation (%) | 25.4 (22.5–28.3) | 26.2 (23.4–29.0) | 19.1 (17.0–21.2) | 20.2 (18.2–22.2) | 15.4 (13.4–17.4) | 16.9 (14.8–18.9) |
| Iron deficiency and anemia | ||||||
| Iron deficiency | 42/75 (56%) | 48/76 (63%) | 4/68 (6%) | 5/67 (8%) | 8/62 (13%) * | 1/61 (2%) * |
| Anemia | 1/88 (1%) | 2/87 (2%) | 3/79 (4%) | 0/81 (0%) | 0/74 (0%) | 0/73 (0%) |
| Iron deficiency anemia | 0/74 (0%) | 2/76 (3%) | 0/68 (0%) | 0/67 (0%) | 0/62 (0%) | 0/61 (0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thanhaeuser, M.; Eibensteiner, F.; Kornsteiner-Krenn, M.; Gsoellpointner, M.; Brandstetter, S.; Fuiko, R.; Koeller, U.; Huf, W.; Huber-Dangl, M.; Binder, C.; et al. Preterm Infants on Early Solid Foods and Iron Status in the First Year of Life—A Secondary Outcome Analysis of a Randomized Controlled Trial. Nutrients 2022, 14, 2732. https://doi.org/10.3390/nu14132732
Thanhaeuser M, Eibensteiner F, Kornsteiner-Krenn M, Gsoellpointner M, Brandstetter S, Fuiko R, Koeller U, Huf W, Huber-Dangl M, Binder C, et al. Preterm Infants on Early Solid Foods and Iron Status in the First Year of Life—A Secondary Outcome Analysis of a Randomized Controlled Trial. Nutrients. 2022; 14(13):2732. https://doi.org/10.3390/nu14132732
Chicago/Turabian StyleThanhaeuser, Margarita, Fabian Eibensteiner, Margit Kornsteiner-Krenn, Melanie Gsoellpointner, Sophia Brandstetter, Renate Fuiko, Ursula Koeller, Wolfgang Huf, Mercedes Huber-Dangl, Christoph Binder, and et al. 2022. "Preterm Infants on Early Solid Foods and Iron Status in the First Year of Life—A Secondary Outcome Analysis of a Randomized Controlled Trial" Nutrients 14, no. 13: 2732. https://doi.org/10.3390/nu14132732
APA StyleThanhaeuser, M., Eibensteiner, F., Kornsteiner-Krenn, M., Gsoellpointner, M., Brandstetter, S., Fuiko, R., Koeller, U., Huf, W., Huber-Dangl, M., Binder, C., Thajer, A., Jilma, B., Berger, A., & Haiden, N. (2022). Preterm Infants on Early Solid Foods and Iron Status in the First Year of Life—A Secondary Outcome Analysis of a Randomized Controlled Trial. Nutrients, 14(13), 2732. https://doi.org/10.3390/nu14132732