
Low Vitamin D Status Relates to the Poor Response of Peripheral Pulse Wave Velocity Following Acute Maximal Exercise in Healthy Young Men

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Acute Maximal Exercise
2.4. Blood Pressure (BP)
2.5. pPWV
2.6. Plasma Analysis
2.7. Statistical Analysis
3. Results
3.1. Plasma Total 25(OH)D Concentrations and Baseline Characteristics
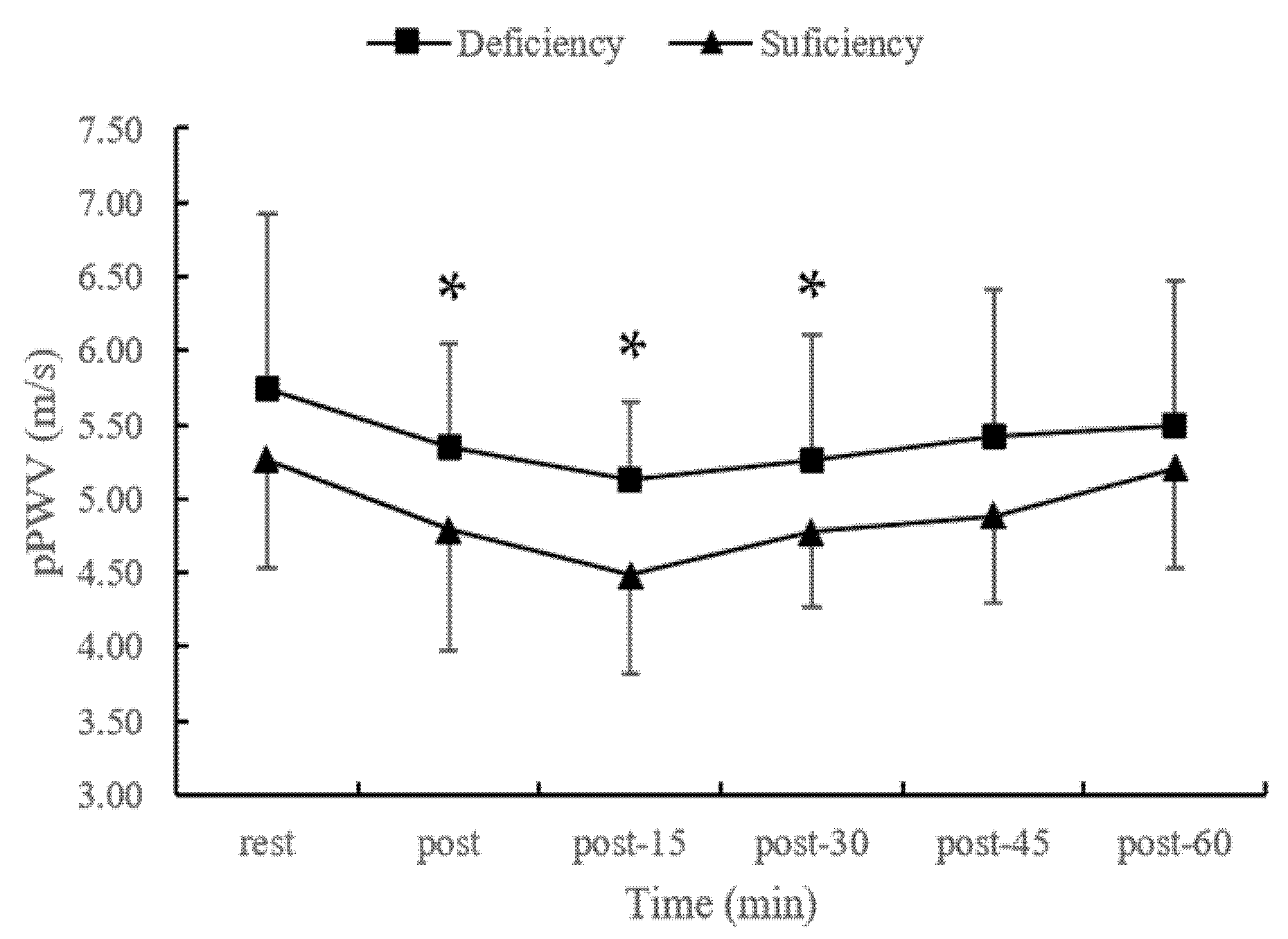
3.2. pPWV Responses Following Acute Maximal Exercise
3.3. Correlations between Vitamin D Levels and pPWV
3.4. Blood Pressure Following Acute Maximal Exercise
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- He, C.S.; Yong, X.M.A.; Walsh, N.P.; Gleeson, M. Is there an optimal vitamin D status for immunity in athletes and military personnel? Exerc. Immunol. Rev. 2016, 22, 42–64. [Google Scholar] [PubMed]
- de la Guía-Galipienso, F.; Martínez-Ferran, M.; Vallecillo, N.; Lavie, C.J.; Sanchis-Gomar, F.; Pareja-Galeano, H. Vitamin D and cardiovascular health. Clin. Nutr. 2020, 40, 2946–2957. [Google Scholar] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar]
- Public Health England. Vitamin D and Health Report. The Scientific Advisory Committee on Nutrition. Available online: https://reurl.cc/0220rM (accessed on 19 September 2021).
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar]
- Krishna, S.M. Vitamin D as a protector of arterial health: Potential role in peripheral arterial disease formation. Int. J. Mol. Sci. 2019, 20, 4907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, A.; Selvanayagam, J.B.; Hyppönen, E. Non-linear Mendelian randomization analyses support a role for vitamin D defi-ciency in cardiovascular disease risk. Eur. Heart J. 2022, 43, 1731–1739. [Google Scholar] [CrossRef] [PubMed]
- Obeid, H.; Soulat, G.; Mousseaux, E.; Laurent, S.; Stergiopulos, N.; Boutouyrie, P.; Segers, P. Numerical assessment and comparison of pulse wave velocity methods aiming at measuring aortic stiffness. Physiol. Meas. 2017, 38, 1953. [Google Scholar]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.S.; Protogerou, A.D.; et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [PubMed] [Green Version]
- Pereira, T.; Correia, C.; Cardoso, J. Novel methods for pulse wave velocity measurement. J. Med. Biol. Eng. 2015, 35, 555–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obeid, H.; Khettab, H.; Marais, L.; Hallab, M.; Laurent, S.; Boutouyrie, P. Evaluation of arterial stiffness by finger–toe pulse wave velocity: Optimization of signal processing and clinical validation. J. Hypertens. 2017, 35, 1618–1625. [Google Scholar] [CrossRef] [PubMed]
- Shim, C.Y.; Yang, W.I.; Park, S.; Kang, M.K.; Ko, Y.G.; Choi, D.; Chung, N.; Ha, J.W. Overweight and its association with aortic pressure wave re-flection after exercise. Am. J. Hypertens. 2011, 24, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Ranadive, S.M.; Heffernan, K.S.; Lane, A.D.; Kappus, R.M.; Cook, M.D.; Wu, P.T.; Sun, P.; Harvey, I.S.; Woods, J.A.; et al. Hemodynamic and arterial stiffness differences between African-Americans and Caucasians after maximal exercise. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H60–H68. [Google Scholar] [CrossRef] [PubMed]
- Naka, K.K.; Tweddel, A.C.; Parthimos, D.; Henderson, A.; Goodfellow, J.; Frenneaux, M.P. Arterial distensibility: Acute changes following dynamic exercise in normal subjects. Am. J. Physiol. Heart Circ. Physiol. 2003, 284, H970–H978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rakobowchuk, M.; Stuckey, M.I.; Millar, P.J.; Gurr, L.; MacDonald, M.J. Effect of acute sprint interval exercise on central and pe-ripheral artery distensibility in young healthy males. Eur. J. Appl. Physiol. 2009, 105, 787–795. [Google Scholar] [CrossRef]
- Campbell, R.; Fisher, J.P.; Sharman, J.E.; McDonnell, B.J.; Frenneaux, M.P. Contribution of nitric oxide to the blood pressure and arterial responses to exercise in humans. J. Hum. Hypertens. 2011, 25, 262–270. [Google Scholar] [CrossRef] [Green Version]
- Madhura, M.; Sandhya, T.A. Effect of different phases of menstrual cycle on reflection index, stiffness index and pulse wave velocity in healthy subjects. J. Clin. Diagn. Res. 2014, 8, BC01. [Google Scholar]
- Kim, D.H.; Meza, C.A.; Clarke, H.; Kim, J.S.; Hickner, R.C. Vitamin D and endothelial function. Nutrients 2020, 12, 575. [Google Scholar] [CrossRef] [Green Version]
- Cakal, S.; Çakal, B.; Karaca, O. Association of vitamin D deficiency with arterial stiffness in newly diagnosed hypertension. Blood Press. Monit. 2021, 26, 113–117. [Google Scholar] [CrossRef]
- Trachsel, Y.; Herzig, D.; Marcin, T.; Zenger, N.; Dysli, M.; Trachsel, L.D.; Wilhelm, M.; Ester, P. Response of peripheral arterial pulse wave velocity to acute exercise in patients after recent myocardial infarction and healthy controls. PLoS ONE 2019, 14, e0219146. [Google Scholar] [CrossRef]
- Nimitphong, H.; Holick, M.F. Vitamin D status and sun exposure in Southeast Asia. Derm.-Endocrinol. 2013, 5, 34–37. [Google Scholar] [CrossRef] [Green Version]
- Bunsawat, K.; Ranadive, S.M.; Lane-Cordova, A.D.; Yan, H.; Kappus, R.M.; Fernhall, B.; Baynard, T. The effect of acute maximal ex-ercise on postexercise hemodynamics and central arterial stiffness in obese and normal-weight individuals. Physiol. Rep. 2017, 5, e13226. [Google Scholar]
- Moore, S.M.; Berrones, A.J.; Clasey, J.L.; Abel, M.G.; Fleenor, B.S. Arterial hemodynamics are impaired at rest and following acute exercise in overweight young men. Vasc. Med. 2016, 21, 497–505. [Google Scholar]
- Bauer, P.; Kraushaar, L.; Dörr, O.; Bauer, T.; Nef, H.; Hamm, C.W.; Most, A. Association of 25-hydroxy vitamin D level with the blood pressure response to a maximum exercise test among professional indoor athletes. Eur. J. Appl. Physiol. 2020, 120, 1931–1941. [Google Scholar] [CrossRef]
- Ward, M.; Langton, J.A. Blood pressure measurement. Anaesth. Crit. Care Pain Med. 2007, 7, 122–126. [Google Scholar] [CrossRef] [Green Version]
- Tsai, W.C.; Chen, J.Y.; Wang, M.C.; Wu, H.T.; Chi, C.K.; Chen, Y.K.; Chen, J.H.; Lin, L.J. Association of risk factors with increased pulse wave velocity detected by a novel method using dual-channel photoplethysmography. Am. J. Hypertens. 2005, 18, 1118–1122. [Google Scholar] [PubMed] [Green Version]
- He, C.-S.; Fraser, W.D.; Tang, J.; Brown, K.; Renwick, S.; Rudland-Thomas, J.; Teah, J.; Tanqueray, E.; Gleeson, M. The effect of 14 weeks of vitamin D3 supplementation on antimicrobial peptides and proteins in athletes. J. Sports Sci. 2015, 34, 67–74. [Google Scholar] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. CDC Vitamin D Standardization-Certification Program (CDC VDSCP). Certified Total 25-Hydroxyvitamin D Assays. Available online: https://reurl.cc/b2ZMKr (accessed on 1 July 2022).
- Altieri, B.; Cavalier, E.; Bhattoa, H.P.; Perez-Lopez, F.R.; Lopez-Baena, M.T.; Perez-Roncero, G.R.; Chedraui, P.; Annweiler, C.; Casa, S.D.; Zelzer, S.; et al. Vitamin D testing: Advantages and limits of the current assays. Eur. J. Clin. Nutr. 2020, 74, 231–247. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, R.; Hatakeyama, H.; Hashimoto, Y.; Okamoto, T. Acute effects of accumulated aerobic exercise on aortic and peripheral pulse wave velocity in young males. J. Phys. Ther. Sci. 2018, 30, 181–184. [Google Scholar]
- Casey, D.P.; Nichols, W.W.; Braith, R.W. Impact of aging on central pressure wave reflection characteristics during exercise. Am. J. Hypertens. 2008, 21, 419–424. [Google Scholar]
- Mitchell, G.F.; Lacourciere, Y.; Arnold, J.M.; Dunlap, M.E.; Conlin, P.R.; Izzo, J.L., Jr. Changes in aortic stiffness and aug-mentation index after acute converting enzyme or vasopeptidase inhibition. Hypertension 2005, 46, 1111–1117. [Google Scholar]
- Al Mheid, I.; Patel, R.; Murrow, J.; Morris, A.; Rahman, A.; Fike, L.; Kavtaradze, N.; Uphoff, I.; Hooper, C.; Tangpricha, V.; et al. Vitamin D status is associated with arterial stiffness and vascular dysfunction in healthy humans. J. Am. Coll. Cardiol. 2011, 58, 186–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zehnder, D.; Bland, R.; Chana, R.S.; Wheeler, D.C.; Howie, A.J.; Williams, M.C.; Stewart, P.M.; Hewison, M. Synthesis of 1, 25-dihydroxyvitamin D3 by human endothelial cells is regulated by inflammatory cytokines: A novel autocrine determinant of vascular cell adhesion. J. Am. Soc. Nephrol. 2002, 13, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Kong, J.; Wei, M.; Chen, Z.F.; Liu, S.Q.; Cao, L.P. 1, 25-Dihydroxyvitamin D3 is a negative endocrine regulator of the renin-angiotensin system. J. Clin. Investig. 2002, 110, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Martins, D.; Wolf, M.; Pan, D.; Zadshir, A.; Tareen, N.; Thadhani, R.; Felsenfeld, A.; Levine, B.; Mehrotra, R.; Norris, K. Prevalence of cardiovascular risk factors and the serum levels of 25-hydroxyvitamin D in the United States: Data from the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2007, 167, 1159–1165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Heijden-Spek, J.J.; Staessen, J.A.; Fagard, R.H.; Hoeks, A.P.; Boudier, H.A.; van Bortel, L.M. Effect of age on brachial artery wall properties differs from the aorta and is gender dependent: A population study. Hypertension 2000, 35, 637–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, P.C.; He, C.S. Effects of different stretching modes on the vascular function in adults after acute resistance exercise. Sports Coach. Sci. 2021, 63, 13–24. [Google Scholar]


{kind=link}
{kind=link}
| Variable | Sufficiency | Deficiency |
|---|---|---|
| Age (years old) | 20.96 ± 1.78 | 21.36 ± 2.12 |
| BMI (kg/m2) | 23.17 ± 2.61 | 22.97 ± 2.92 |
| Rest-pPWV (m/s) | 5.26 ± 0.72 | 5.75 ±1.18 |
| Vitamin D (nmol/L) | 60.21 ± 6.75 * | 40.68 ± 7.5 |
| O2max (mL/kg/min) | 43.97 ± 5.69 | 40.78 ± 7.17 |
| Activity (minute/week) | 534.29 ± 271.35 | 519.55 ± 300.75 |
| Rest | Post-0 min | Post-15 min | Post-30 min | Post-45 min | Post-60 min | Trial; Time; Trial × Time | ||
|---|---|---|---|---|---|---|---|---|
| SBP (bpm) | Deficient group | 121.47 ± 10.70 | 150.05 ± 13.98 * | 119.26 ± 17.17 | 115.47 ± 9.85 * | 112.63 ± 13.37 * | 113.58 ± 13.52 * | 0.204; 0.000; 0.177 |
| Sufficient group | 126.96 ± 9.32 | 158.38 ± 15.95 * | 123.88 ± 10.76 | 115.75 ± 12.16 * | 111.92 ± 13.32 * | 119.38 ± 10.42 * | ||
| DBP (bpm) | Deficient group | 63.84 ± 9.05 | 60.37 ± 11.48 | 60.58 ± 9.61 | 61.32 ± 7.55 | 62.00 ± 10.02 | 61.32 ± 9.66 | 0.693; 0.437; 0.575 |
| Sufficient group | 64.08 ± 8.60 | 63.38 ± 10.84 | 62.79 ± 10.13 | 60.79 ± 10.13 | 59.83 ± 8.71 | 63.46 ± 6.66 | ||
| MAP (bpm) | Deficient group | 83.05 ± 8.75 | 90.26 ± 9.60 * | 80.14 ± 10.91 | 79.37 ± 7.38 | 78.88 ± 8.28 * | 78.74 ± 9.25 * | 0.389; 0.000; 0.199 |
| Sufficient group | 85.04 ± 7.52 | 95.04 ± 10.35 * | 83.15 ± 9.06 | 79.11 ± 7.75 * | 77.19 ± 9.17 * | 82.10 ± 6.77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, L.-Y.; Wang, C.-W.; Chen, L.-A.; Fang, S.-H.; Wang, S.-C.; He, C.-S. Low Vitamin D Status Relates to the Poor Response of Peripheral Pulse Wave Velocity Following Acute Maximal Exercise in Healthy Young Men. Nutrients 2022, 14, 3074. https://doi.org/10.3390/nu14153074
Chen L-Y, Wang C-W, Chen L-A, Fang S-H, Wang S-C, He C-S. Low Vitamin D Status Relates to the Poor Response of Peripheral Pulse Wave Velocity Following Acute Maximal Exercise in Healthy Young Men. Nutrients. 2022; 14(15):3074. https://doi.org/10.3390/nu14153074
Chicago/Turabian StyleChen, Liang-You, Chun-Wei Wang, Lu-An Chen, Shih-Hua Fang, Soun-Cheng Wang, and Cheng-Shiun He. 2022. "Low Vitamin D Status Relates to the Poor Response of Peripheral Pulse Wave Velocity Following Acute Maximal Exercise in Healthy Young Men" Nutrients 14, no. 15: 3074. https://doi.org/10.3390/nu14153074
APA StyleChen, L.-Y., Wang, C.-W., Chen, L.-A., Fang, S.-H., Wang, S.-C., & He, C.-S. (2022). Low Vitamin D Status Relates to the Poor Response of Peripheral Pulse Wave Velocity Following Acute Maximal Exercise in Healthy Young Men. Nutrients, 14(15), 3074. https://doi.org/10.3390/nu14153074