
The Association between Smoking Cessation and Depressive Symptoms: Diet Quality Plays a Mediating Role


Abstract
:1. Introduction
2. Method
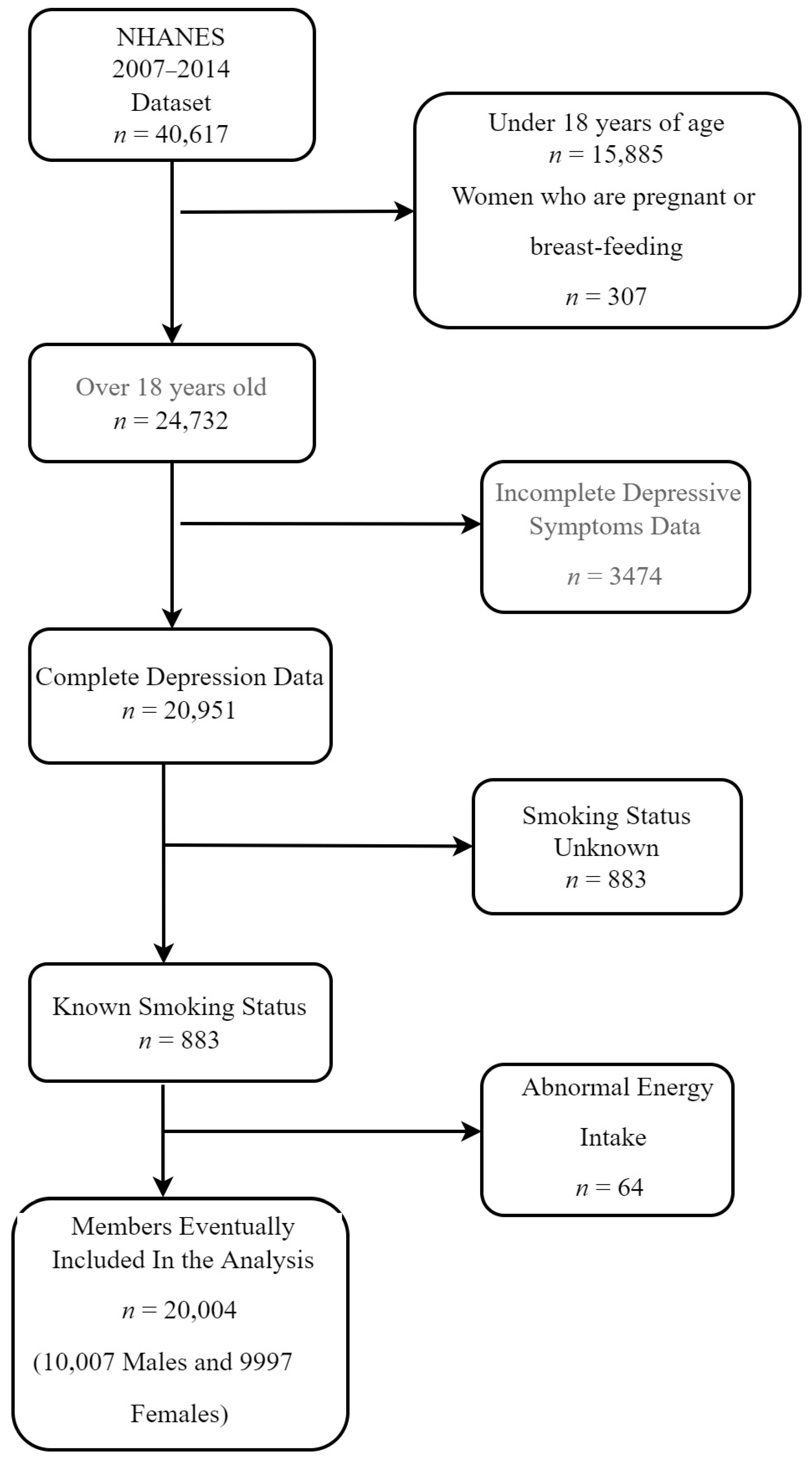
2.1. Study Population
2.2. Depressive Symptoms Assessment
2.3. Classification of Smoking Status
2.4. Dietary Quality Assessment
2.5. Covariates
2.6. Statistical Analyses
3. Results
3.1. Descriptive Analysis of the Study Participants
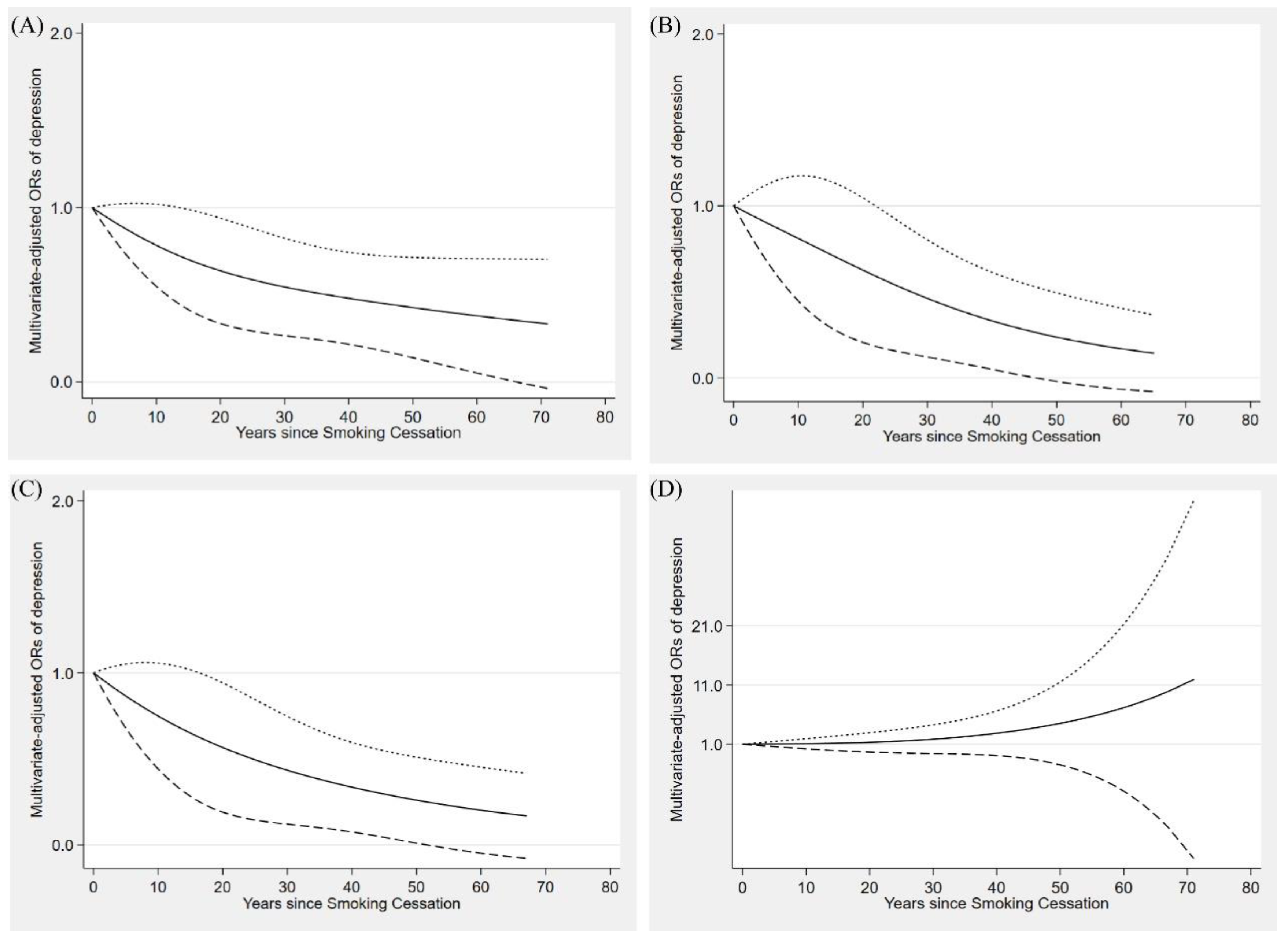
3.2. Smoking Cessation, HEI, and Depressive Symptoms
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murray, C.J.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. Health, Reports of the Surgeon General. In The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2014. [Google Scholar]
- Pirie, K.; Peto, R.; Reeves, G.K.; Green, J.; Beral, V. The 21st century hazards of smoking and benefits of stopping: A prospective study of one million women in the UK. Lancet 2013, 381, 133–141. [Google Scholar] [CrossRef] [Green Version]
- Kinnunen, T.; Haukkala, A.; Korhonen, T.; Quiles, Z.N.; Spiro, A., 3rd; Garvey, A.J. Depression and smoking across 25 years of the Normative Aging Study. Int. J. Psychiatry Med. 2006, 36, 413–426. [Google Scholar] [CrossRef] [PubMed]
- Berlin, I.; Chen, H.; Covey, L.S. Depressive mood, suicide ideation and anxiety in smokers who do and smokers who do not manage to stop smoking after a target quit day. Addiction 2010, 105, 2209–2216. [Google Scholar] [CrossRef] [PubMed]
- Dawkins, L.; Powell, J.H.; Pickering, A.; Powell, J.; West, R. Patterns of change in withdrawal symptoms, desire to smoke, reward motivation and response inhibition across 3 months of smoking abstinence. Addiction 2009, 104, 850–858. [Google Scholar] [CrossRef] [Green Version]
- Kahler, C.W.; Brown, R.A.; Ramsey, S.E.; Niaura, R.; Abrams, D.B.; Goldstein, M.G.; Mueller, T.I.; Miller, I.W. Negative mood, depressive symptoms, and major depression after smoking cessation treatment in smokers with a history of major depressive disorder. J. Abnorm. Psychol. 2002, 111, 670–675. [Google Scholar] [CrossRef]
- Kahler, C.W.; Spillane, N.S.; Leventhal, A.M.; Strong, D.R.; Brown, R.A.; Monti, P.M. Hostility and smoking cessation treatment outcome in heavy social drinkers. Psychol. Addict. Behav. J. Soc. Psychol. Addict. Behav. 2009, 23, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Mino, Y.; Shigemi, J.; Otsu, T.; Tsuda, T.; Babazono, A. Does smoking cessation improve mental health? Psychiatry Clin. Neurosci. 2000, 54, 169–172. [Google Scholar] [CrossRef]
- Steinberg, M.B.; Bover, M.T.; Richardson, D.L.; Schmelzer, A.C.; Williams, J.M.; Foulds, J. Abstinence and psychological distress in co-morbid smokers using various pharmacotherapies. Drug Alcohol Depend. 2011, 114, 77–81. [Google Scholar] [CrossRef]
- Cookson, C.; Strang, J.; Ratschen, E.; Sutherland, G.; Finch, E.; McNeill, A. Smoking and its treatment in addiction services: Clients’ and staff behaviour and attitudes. BMC Health Serv. Res. 2014, 14, 304. [Google Scholar] [CrossRef] [Green Version]
- Sheals, K.; Tombor, I.; McNeill, A.; Shahab, L. A mixed-method systematic review and meta-analysis of mental health professionals’ attitudes toward smoking and smoking cessation among people with mental illnesses. Addiction 2016, 111, 1536–1553. [Google Scholar] [CrossRef]
- Shivappa, N.; Zucchetto, A.; Serraino, D.; Rossi, M.; La Vecchia, C.; Hébert, J.R. Dietary inflammatory index and risk of esophageal squamous cell cancer in a case-control study from Italy. Cancer Causes Control 2015, 26, 1439–1447. [Google Scholar] [CrossRef]
- Berg, C.J.; Haardoerfer, R.; Escoffery, C.; Zheng, P.; Kegler, M. Cigarette users’ interest in using or switching to electronic nicotine delivery systems for smokeless tobacco for harm reduction, cessation, or novelty: A cross-sectional survey of US adults. Nicotine Tob. Res. Off. J. Soc. Res. Nicotine Tob. 2015, 17, 245–255. [Google Scholar] [CrossRef] [Green Version]
- Lunn, T.E.; Nowson, C.A.; Worsley, A.; Torres, S.J. Does personality affect dietary intake? Nutrition 2014, 30, 403–409. [Google Scholar] [CrossRef] [Green Version]
- Dyer, A.R.; Elliott, P.; Stamler, J.; Chan, Q.; Ueshima, H.; Zhou, B.F. Dietary intake in male and female smokers, ex-smokers, and never smokers: The INTERMAP study. J. Hum. Hypertens. 2003, 17, 641–654. [Google Scholar] [CrossRef] [Green Version]
- Strickland, D.; Graves, K.; Lando, H. Smoking status and dietary fats. Prev. Med. 1992, 21, 228–236. [Google Scholar] [CrossRef]
- Morabia, A.; Curtin, F.; Bernstein, M.S. Effects of smoking and smoking cessation on dietary habits of a Swiss urban population. Eur. J. Clin. Nutr. 1999, 53, 239–243. [Google Scholar] [CrossRef] [Green Version]
- Cade, J.E.; Margetts, B.M. Relationship between diet and smoking--is the diet of smokers different? J. Epidemiol. Community Health 1991, 45, 270–272. [Google Scholar] [CrossRef] [Green Version]
- Alkerwi, A.; Baydarlioglu, B.; Sauvageot, N.; Stranges, S.; Lemmens, P.; Shivappa, N.; Hébert, J.R. Smoking status is inversely associated with overall diet quality: Findings from the ORISCAV-LUX study. Clin. Nutr. 2017, 36, 1275–1282. [Google Scholar] [CrossRef]
- Gritz, E.R.; Carmack, C.L.; de Moor, C.; Coscarelli, A.; Schacherer, C.W.; Meyers, E.G.; Abemayor, E. First year after head and neck cancer: Quality of life. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1999, 17, 352–360. [Google Scholar] [CrossRef]
- Stamler, J.; Rains-Clearman, D.; Lenz-Litzow, K.; Tillotson, J.L.; Grandits, G.A. Relation of smoking at baseline and during trial years 1–6 to food and nutrient intakes and weight in the special intervention and usual care groups in the Multiple Risk Factor Intervention Trial. Am. J. Clin. Nutr. 1997, 65, 374s–402s. [Google Scholar] [CrossRef] [Green Version]
- Quirk, S.E.; Williams, L.J.; O’Neil, A.; Pasco, J.A.; Jacka, F.N.; Housden, S.; Berk, M.; Brennan, S.L. The association between diet quality, dietary patterns and depression in adults: A systematic review. BMC Psychiatry 2013, 13, 175. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Lv, M.R.; Wei, Y.J.; Sun, L.; Zhang, J.X.; Zhang, H.G.; Li, B. Dietary patterns and depression risk: A meta-analysis. Psychiatry Res. 2017, 253, 373–382. [Google Scholar] [CrossRef]
- Lassale, C.; Batty, G.D.; Baghdadli, A.; Jacka, F.; Sanchez-Villegas, A.; Kivimaki, M.; Akbaraly, T. Healthy dietary indices and risk of depressive outcomes: A systematic review and meta-analysis of observational studies. Mol. Psychiatry 2019, 24, 965–986. [Google Scholar] [CrossRef] [Green Version]
- Jacka, F.N.; O’Neil, A.; Opie, R.; Itsiopoulos, C.; Cotton, S.; Mohebbi, M.; Castle, D.; Dash, S.; Mihalopoulos, C.; Chatterton, M.L.; et al. A randomised controlled trial of dietary improvement for adults with major depression (the ‘SMILES’ trial). BMC Med. 2017, 15, 23. [Google Scholar] [CrossRef] [Green Version]
- Firth, J.; Marx, W.; Dash, S.; Carney, R.; Teasdale, S.B.; Solmi, M.; Stubbs, B.; Schuch, F.B.; Carvalho, A.F.; Jacka, F.; et al. The Effects of Dietary Improvement on Symptoms of Depression and Anxiety: A Meta-Analysis of Randomized Controlled Trials. Psychosom. Med. 2019, 81, 265–280. [Google Scholar] [CrossRef]
- Data. NHaNES. Centers for Disease Control and Prevention (CDC) Web Site. Available online: http://www.cdc.gov/NCHS/nhanes.htm (accessed on 3 May 2022).
- Parsons, V.L.; Moriarity, C.; Jonas, K.; Moore, T.F.; Davis, K.E.; Tompkins, L. Design and estimation for the national health interview survey, 2006–2015. Vital Health Statistics. Ser. 2 Data Eval. Methods Res. 2014, 130, 1–53. [Google Scholar]
- Manea, L.; Gilbody, S.; McMillan, D. A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. Gen. Hosp. Psychiatry 2015, 37, 67–75. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Nutrition and Your Health: 2015–2020. In Dietary Guidelines for Americans, 8th ed.; US Government Printing Office: Washington, DC, USA, 2015. Available online: https://health.gov/our-work/food-nutrition/previous-dietary-guidelines/2015 (accessed on 3 May 2022).
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Zhao, Y.; Nie, J.; Xu, H.; Yu, C.; Wang, S. Higher HEI-2015 Score Is Associated with Reduced Risk of Depression: Result from NHANES 2005–2016. Nutrients 2021, 13, 348. [Google Scholar] [CrossRef]
- De La Cruz, N.; Shabaneh, O.; Appiah, D. The Association of Ideal Cardiovascular Health and Ocular Diseases Among US Adults. Am. J. Med. 2021, 134, 252–259.e1. [Google Scholar] [CrossRef]
- Hu, Y.; Zong, G.; Liu, G.; Wang, M.; Rosner, B.; Pan, A.; Willett, W.C.; Manson, J.E.; Hu, F.B.; Sun, Q. Smoking Cessation, Weight Change, Type 2 Diabetes, and Mortality. N. Engl. J. Med. 2018, 379, 623–632. [Google Scholar] [CrossRef]
- ALHarthi, S.S.; Natto, Z.S.; Midle, J.B.; Gyurko, R.; O’Neill, R.; Steffensen, B. Association between time since quitting smoking and periodontitis in former smokers in the National Health and Nutrition Examination Surveys (NHANES) 2009 to 2012. J. Periodontol. 2019, 90, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Lee, E.J. Long-Term Effects of Smoking Cessation on Depressive Symptoms, Resilience, Coping Skills, and Serotonin. Psychiatr. Q. 2020, 91, 263–271. [Google Scholar] [CrossRef]
- Aubin, H.J. Management of emergent psychiatric symptoms during smoking cessation. Curr. Med. Res. Opin. 2009, 25, 519–525. [Google Scholar] [CrossRef]
- Rodríguez-Cano, R.; López-Durán, A.; del Río, E.F.; Martínez-Vispo, C.; Martínez, Ú.; Becoña, E. Smoking cessation and depressive symptoms at 1-, 3-, 6-, and 12-months follow-up. J. Affect. Disord. 2016, 191, 94–99. [Google Scholar] [CrossRef] [Green Version]
- Cinciripini, P.M.; Robinson, J.D.; Karam-Hage, M.; Minnix, J.A.; Lam, C.; Versace, F.; Brown, V.L.; Engelmann, J.M.; Wetter, D.W. Effects of varenicline and bupropion sustained-release use plus intensive smoking cessation counseling on prolonged abstinence from smoking and on depression, negative affect, and other symptoms of nicotine withdrawal. JAMA Psychiatry 2013, 70, 522–533. [Google Scholar] [CrossRef] [Green Version]
- Chatzi, L.; Melaki, V.; Sarri, K.; Apostolaki, I.; Roumeliotaki, T.; Georgiou, V.; Vassilaki, M.; Koutis, A.; Bitsios, P.; Kogevinas, M. Dietary patterns during pregnancy and the risk of postpartum depression: The mother-child ‘Rhea’ cohort in Crete, Greece. Public Health Nutr. 2011, 14, 1663–1670. [Google Scholar] [CrossRef] [Green Version]
- Tangney, C.C.; Young, J.A.; Murtaugh, M.A.; Cobleigh, M.A.; Oleske, D.M. Self-reported dietary habits, overall dietary quality and symptomatology of breast cancer survivors: A cross-sectional examination. Breast Cancer Res. Treat. 2002, 71, 113–123. [Google Scholar] [CrossRef]
- Aihara, Y.; Minai, J.; Aoyama, A.; Shimanouchi, S. Depressive symptoms and past lifestyle among Japanese elderly people. Community Ment. Health J. 2011, 47, 186–193. [Google Scholar] [CrossRef]
- Kuczmarski, M.F.; Cremer Sees, A.; Hotchkiss, L.; Cotugna, N.; Evans, M.K.; Zonderman, A.B. Higher Healthy Eating Index-2005 scores associated with reduced symptoms of depression in an urban population: Findings from the Healthy Aging in Neighborhoods of Diversity Across the Life Span (HANDLS) study. J. Am. Diet. Assoc. 2010, 110, 383–389. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Non-Depressive Symptoms (PHQ < 10) | Depressive Symptoms (PHQ ≥ 10) | p Value | |
|---|---|---|---|
| Number of participants (%) a | 18,100 (90.48) | 1904 (9.52) | |
| Age | 50 (35, 64) | 50 (37, 62) | 0.001 |
| Age (year) a | <0.001 | ||
| 18–39 | 6124 (36.07) | 590 (34.15) | |
| 40–59 | 5818 (37.76) | 772 (45.10) | |
| ≥60 | 6158 (21.17) | 542 (20.75) | |
| Gender (%) a | <0.001 | ||
| Male | 9334 (50.91) | 673 (34.85) | |
| Female | 8766 (49.09) | 1231 (65.15) | |
| Race or ethnicity (%) a | <0.001 | ||
| Mexican American | 2677 (8.28) | 290 (8.82) | |
| Other Hispanic | 1761 (5.13) | 266 (8.12) | |
| Non-Hispanic White | 8125 (69.22) | 824 (63.70) | |
| Non-Hispanic Black | 3798 (10.77) | 408 (13.98) | |
| Other races | 1739 (6.61) | 116 (5.97) | |
| Educational level (%) a | <0.001 | ||
| <High school | 1704 (4.89) | 286 (9.10) | |
| High school | 6638 (33.18) | 884 (46.14) | |
| >High school | 9446 (61.93) | 713 (44.76) | |
| Household income (%) a | <0.001 | ||
| Under USD 20,000 | 3509 (13.35) | 721 (30.28) | |
| USD 20,000 and over | 13,854 (86.65) | 1090 (69.72) | |
| Body mass index b | 27.80(24.20, 32.20) | 29.77(25.09, 34.98) | |
| Body mass index (%) a | <0.001 | ||
| <18.5 kg/m2 | 275 (1.42) | 38 (1.92) | |
| 18.5–25 kg/m2 | 5107 (29.16) | 425 (23.50) | |
| 25–30 kg/m2 | 6057 (33.82) | 497 (27.11) | |
| ≥30 kg/m2 | 6661 (35.59) | 944 (47.48) | |
| Work activity (%) a | 0.0012 | ||
| Vigorous | 3372 (20.49) | 327 (18.54) | |
| Moderate | 3880 (23.35) | 343 (19.05) | |
| Other | 10,846 (56.17) | 1232 (62.41) | |
| Recreational activity (%) a | <0.001 | ||
| Vigorous | 4047 (26.28) | 180 (9.18) | |
| Moderate | 4942 (29.32) | 359 (21.87) | |
| Other | 9110 (44.39) | 1365 (68.95) | |
| Alcohol consumption (%) a | 13,054 (77.71) | 1361 (75.73) | 0.1039 |
| Smoke status (%) a | <0.001 | ||
| Never smoker | 10,181 (56.46) | 791 (39.51) | |
| Former smoker | 4378 (24.55) | 408 (21.01) | |
| Current smoker | 3540 (19.00) | 715 (39.48) | |
| Healthy Eating Index b | 55.52 (44.37, 63.20) | 49.56 (41.18, 58.88) | |
| Healthy Eating Index (%) a | |||
| <50 | 7031 (40.72) | 940 (53.62) | |
| 50–70 | 8245 (46.39) | 755 (40.08) | |
| ≥70 | 2241 (12.88) | 131 (6.30) | |
| Diabetes (%) a | 3214 (13.54) | 511 (21.45) | <0.001 |
| Hypertension (%) a | 9766 (49.83) | 1162 (56.94) | <0.001 |
| Total energy (kcal/day) b | 1907.5 (1466, 2462) | 1799.5 (1360.5, 2354) | <0.001 |
| Caffeine intake (mg/day) b | 96.5 (28.5, 200) | 101 (32.221) | 0.0051 |
| Variable | Crude Model | Model 1 | Model 2 | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Time since quitting (years) | 0.983 | 0.973–0.995 | 0.977 | 0.954–0.990 | 0.985 | 0.971–0.999 |
| Smoking status | ||||||
| Current smokers | 1 | (ref) | 1 | (ref) | 1 | (ref) |
| Time since quitting (years) | ||||||
| <10 years | 0.524 | 0.409–0.671 | 0.524 | 0.411–0.668 | 0.636 | 0.485–0.833 |
| 10–20 years | 0.360 | 0.274–0.474 | 0.349 | 0.263–0.464 | 0.364 | 0.264–0.503 |
| 20–30 years | 0.389 | 0.258–0.586 | 0.385 | 0.251–0.591 | 0.563 | 0.357–0.889 |
| ≥30 years | 0.308 | 0.217–0.438 | 0.305 | 0.202–0.459 | 0.449 | 0.290–0.695 |
| Never smoked | 0.337 | 0.295–0.384 | 0.306 | 0.265–0.354 | 0.433 | 0.363–0.518 |
| Age (years) | 1.00 | 0.996–1.006 | 0.987 | 0.981–0.994 | ||
| Sex | ||||||
| Male | 1 | (ref) | 1 | (ref) | ||
| Female | 2.127 | 1.855–2.439 | 1.876 | 1.542 | ||
| Race | ||||||
| Mexican American | 1 | (ref) | ||||
| Other Hispanic | 1.630 | 1.219–2.107 | ||||
| Non-Hispanic White | 1.100 | 0.913–1.327 | ||||
| Non-Hispanic Black | 1.133 | 0.915–1.405 | ||||
| Other Race | 1.443 | 1.086–1.919 | ||||
| Education | ||||||
| Below high school | 1 | (ref) | ||||
| High school level | 0.834 | 0.686–1.017 | ||||
| Above high school | 0.678 | 0.540–0.853 | ||||
| Annual household income | ||||||
| Less than USD 20,000 | 1 | (ref) | ||||
| Over USD 20,000 | 0.489 | 0.424–0.565 | ||||
| Caffeine intake (mg) | 1.000 | 1.000–1.000 | ||||
| Energy intake (kcal) | 0.999 | 0.999–1.000 | ||||
| Drinking status | ||||||
| Drinkers | 1.195 | 1.009–1.415 | ||||
| Non-drinkers | 1 | (ref) | ||||
| Hypertension status | ||||||
| Hypertension | 1.277 | 1.050–1.554 | ||||
| No hypertension | 1 | (ref) | ||||
| Diabetes status | ||||||
| Diabetes | 1.477 | 1.202–1.813 | ||||
| No diabetes | 1 | (ref) | ||||
| Intensity of work activities | ||||||
| Vigorous | 1 | (ref) | ||||
| Moderate | 1.739 | 1.328–2.278 | ||||
| Mile | 2.681 | 2.121–3.412 | ||||
| Intensity of recreational activities | ||||||
| Vigorous | 1 | (ref) | ||||
| Moderate | 0.861 | 0.679–1.092 | ||||
| Mild | 1.149 | 0.938–1.406 | ||||
| Body Mass Index (kg/m2) | 1.022 | 1.013–1.032 | ||||
| Healthy Eating Index | 0.987 | 0.982–0.993 | ||||
| Effect | β | SE | Z | p | 95% CI | Mediation (%) | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Depression symptoms | |||||||
| Total effect | −0.017 | 0.005 | −3.32 | <0.01 | −0.027 | −0.007 | |
| Direct effect | −0.018 | 0.005 | −3.46 | <0.01 | −0.028 | −0.008 | |
| Indirect effect | −0.001 | 0.001 | −2.08 | 0.037 | −0.024 | −0.001 | 6.91 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.; Jiang, H.; Zhang, D.; Luo, J.; Zhang, H. The Association between Smoking Cessation and Depressive Symptoms: Diet Quality Plays a Mediating Role. Nutrients 2022, 14, 3047. https://doi.org/10.3390/nu14153047
Liu S, Jiang H, Zhang D, Luo J, Zhang H. The Association between Smoking Cessation and Depressive Symptoms: Diet Quality Plays a Mediating Role. Nutrients. 2022; 14(15):3047. https://doi.org/10.3390/nu14153047
Chicago/Turabian StyleLiu, Shuo, Hongbin Jiang, Dongfeng Zhang, Jia Luo, and Hua Zhang. 2022. "The Association between Smoking Cessation and Depressive Symptoms: Diet Quality Plays a Mediating Role" Nutrients 14, no. 15: 3047. https://doi.org/10.3390/nu14153047
APA StyleLiu, S., Jiang, H., Zhang, D., Luo, J., & Zhang, H. (2022). The Association between Smoking Cessation and Depressive Symptoms: Diet Quality Plays a Mediating Role. Nutrients, 14(15), 3047. https://doi.org/10.3390/nu14153047