
Association of Household Type and Fast-Food Consumption in Korean Adolescents

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data and Study Population
2.2. Variables
2.3. Statistical Analysis
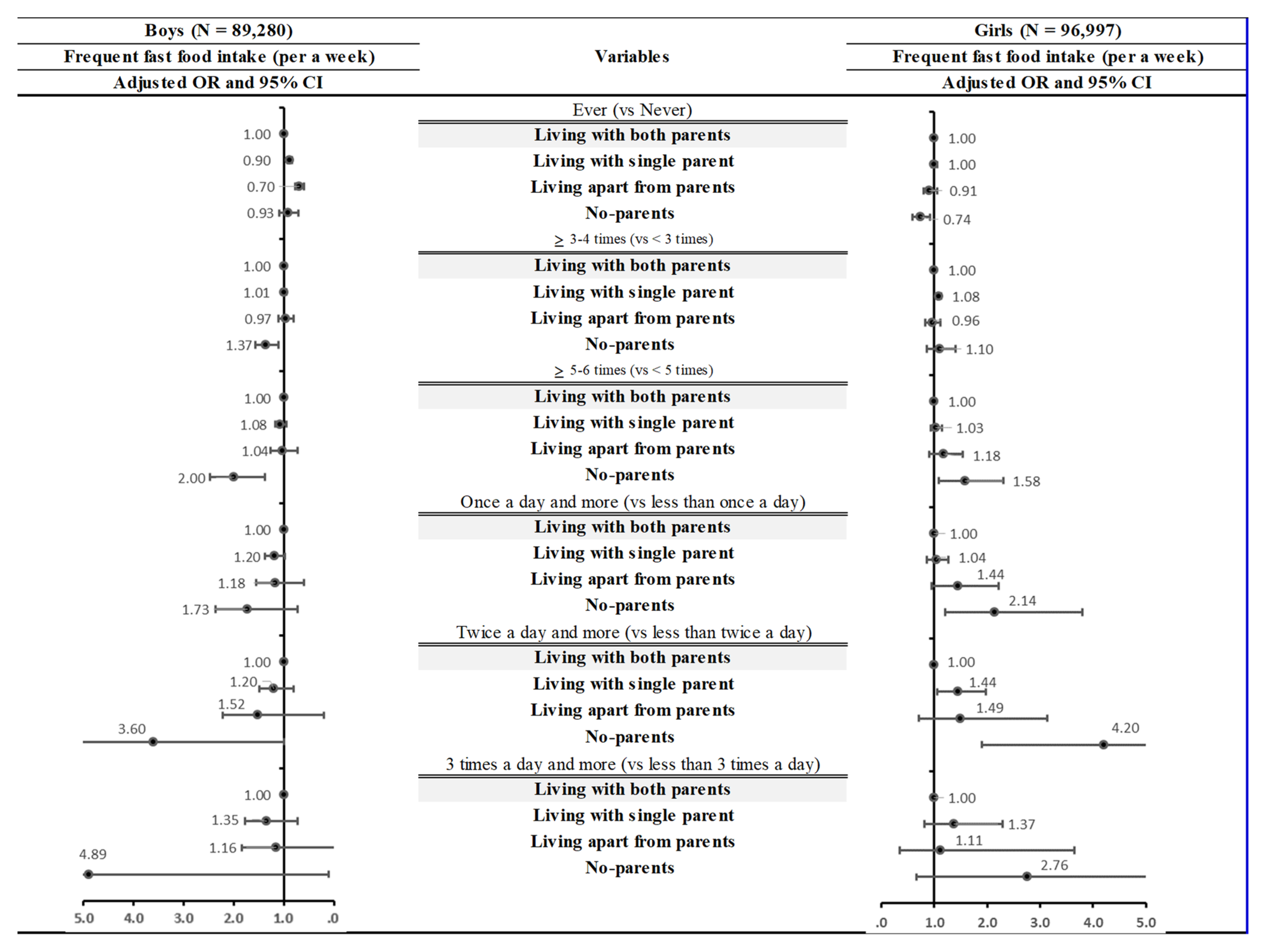
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jo, Y.W. Analysis on Consumption of Fast-Foods and Sugar Sweetened Beverages, and Health Condition and Behavior; Korea Centers for Disease Control and Prevention: Seoul, Korea, 2011. [Google Scholar]
- Bowman, S.A.; Gortmaker, S.L.; Ebbeling, C.B.; Pereira, M.A.; Ludwig, D.S. Effects of Fast-Food Consumption on Energy Intake and Diet Quality Among Children in a National Household Survey. Pediatrics 2004, 113, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Bowman, S.A.; Vinyard, B.T. Fast Food Consumption of U.S. Adults: Impact on Energy and Nutrient Intakes and Overweight Status. J. Am. Coll. Nutr. 2004, 23, 163–168. [Google Scholar] [CrossRef]
- French, S.A.; Story, M.; Neumark-Sztainer, D.; Fulkerson, J.A.; Hannan, P. Fast food restaurant use among adolescents: Associations with nutrient intake, food choices and behavioral and psychosocial variables. Int. J. Obes. 2001, 25, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Vartanian, L.R.; Schwartz, M.B.; Brownell, K.D. Effects of Soft Drink Consumption on Nutrition and Health: A Systematic Review and Meta-Analysis. Am. J. Public Health 2007, 97, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Giammattei, J.; Blix, G.; Marshak, H.H.; Wollitzer, A.O.; Pettitt, D.J. Television Watching and Soft Drink Consumption: Associations With Obesity in 11- to 13-Year-Old Schoolchildren. Arch. Pediatrics Adolesc. Med. 2003, 157, 882–886. [Google Scholar] [CrossRef]
- Kowen, M.-R.; Jang, M.; Lee, N.-K. Transforming in awareness of relationship problems due to excessive private education in Korea. Int. J. Qual. Stud. Health Well-Being 2019, 14, 1586624. [Google Scholar] [CrossRef]
- You, J.S.; Kim, S.M.; Chang, K.J. Nutritional Knowledge and Dietary Behavior of the 6th Grade Elementary School Students in Daejeon Area by Gender and Skipping Breakfast. Korean J. Nutr. 2009, 42, 256–267. [Google Scholar] [CrossRef][Green Version]
- Hong, S.; Bae, H.C.; Kim, H.S.; Park, E.-C. Variation in meal-skipping rates of Korean adolescents according to socio-economic status: Results of the Korea Youth Risk Behavior Web-based Survey. J. Prev. Med. Public Health 2014, 47, 158–168. [Google Scholar] [CrossRef]
- Spear, B.A. Adolescent Growth and Development. J. Am. Diet. Assoc. 2002, 102, S23–S29. [Google Scholar] [CrossRef]
- Rees, J.M.; Neumark-Sztainer, D.; Kohn, M.; Jacobson, M. Improving the nutritional health of adolescents-position statement-society for adolescent medicine. J. Adolesc. Health 1999, 24, 461–462. [Google Scholar] [CrossRef]
- Kemm, J.R. Eating Patterns in Childhood and Adult Health. Nutr. Health 1987, 4, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Nicklas, T.A.; Farris, R.P.; Smoak, C.G.; Frank, G.C.; Srinivasan, S.R.; Webber, L.S.; Berenson, G.S. Dietary factors relate to cardiovascular risk factors in early life. Bogalusa Heart Study. Arterioscler. Off. J. Am. Heart Assoc. Inc. 1988, 8, 193–199. [Google Scholar]
- Rosenheck, R. Fast food consumption and increased caloric intake: A systematic review of a trajectory towards weight gain and obesity risk. Obes. Rev. 2008, 9, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Baek, Y.J. Family Structure and Diet of Children and Adolescents: Analysis of Data from the Fifth Korea National Health and Nutrition Examination Survey(KNHANES V) 2010–2011. Master’s Thesis, Seoul National University, Seoul, Korea, 2014. [Google Scholar]
- Korea National Statistical Office. Accual Statistic Information Report on Population and Housing Census of Korea; Statistics Korea: Sejong, Korea, 2020. [Google Scholar]
- Qin, X.; Zhang, W.; Hua, L.; Zhu, Z.; Ye, T. Influence of family dietary environment on children’s dietary behaviours. Chin. Nurs. Res. 2014, 2014, 4228–4230. [Google Scholar]
- Korea Centers for Disease Control and Prevention. The Report of the Korea Youth Risk Behavior Web-Based Survey in 2017; Korea Centers for Disease Control and Prevention: Cheongju, Korea, 2017. [Google Scholar]
- Jeong, W.; Kim, Y.K.; Lee, H.J.; Jang, J.; Kim, S.; Park, E.-C.; Jang, S.-I. Association of Bedtime with both Suicidal Ideation and Suicide Planning among Korean Adolescents. Int. J. Environ. Res. Public Health 2019, 16, 3817. [Google Scholar] [CrossRef] [PubMed]
- Korea Centers for Disease Control and Prevention. The Statistics of 16th Korea Youth Risk Behavior Web-Based Survey; Korea Centers for Disease Control and Prevention: Cheongju, Korea, 2021. [Google Scholar]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Bae, J.-S.; Joung, H.-J.; Kim, J.-Y.; Kwon, K.-N.; Kim, Y.-T.; Park, S.-W. Test-retest reliability of a questionnaire for the Korea Youth Risk Behavior Web-based Survey. J. Prev. Med. Public Health 2010, 43, 403–410. [Google Scholar] [CrossRef]
- Bae, J.-S.; Joung, H.-J.; Kim, J.-Y.; Kwon, K.-N.; Kim, Y.-J.; Park, S.-W. Validity of self-reported height, weight, and body mass index of the Korea Youth Risk Behavior Web-based Survey questionnaire. J. Prev. Med. Public Health 2010, 43, 396–402. [Google Scholar] [CrossRef]
- Li Wen, M.; Simpson, J.M.; Baur, L.A.; Rissel, C.; Flood, V.M. Family Functioning and Obesity Risk Behaviors: Implications for Early Obesity Intervention. Obesity 2011, 19, 1252–1258. [Google Scholar] [CrossRef]
- Berge, J.M.; MacLehose, R.F.; Larson, N.; Laska, M.; Neumark-Sztainer, D. Family Food Preparation and Its Effects on Adolescent Dietary Quality and Eating Patterns. J. Adolesc. Health 2016, 59, 530–536. [Google Scholar] [CrossRef]
- Bell, L.K.; Perry, R.A.; Prichard, I. Exploring Grandparents’ Roles in Young Children’s Lifestyle Behaviors and the Prevention of Childhood Obesity: An Australian Perspective. J. Nutr. Educ. Behav. 2018, 50, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Ryu, H.K. Analysis of the Dietary Life of Adolescents by Household Types in Korea using the Korea National Health and Nutrition Examination Survey. Korean J. Community Living Sci. 2021, 32, 285–304. [Google Scholar] [CrossRef]
- Markert, J.; Herke, M.; Bartels, A.; Gosse, K.; Roick, J.; Herz-Jakoby, A.; Täubig, V.; Schröer, W.; Richter, M. Food practices and nutrition of children and adolescents in residential care: A scoping review. Appetite 2021, 167, 105640. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Tucker, P.; Gilliland, J.; Irwin, J.D.; Larsen, K.; Hess, P. The Influence of Local Food Environments on Adolescents’ Food Purchasing Behaviors. Int. J. Environ. Res. Public Health 2012, 9, 1458–1471. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.C.; Gordon-Larsen, P.; North, K.E.; Adair, L.S. Body Mass Index Gain, Fast Food, and Physical Activity: Effects of Shared Environments over Time. Obesity 2006, 14, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Jeon, H.J. A proposal for improvement of the business supporting poorly-fed children using mobile payment and information delivery platform. In Proceedings of the Korea Information Processing Society Conference, Seoul, Korea, 2020; pp. 37–40. [Google Scholar] [CrossRef]
- Kim, S.H.; Jeong, S.H.; Park, E.-C.; Jang, S.-I. Association of Cigarette Type Initially Smoked With Suicidal Behaviors Among Adolescents in Korea From 2015 to 2018. JAMA Netw. Open 2021, 4, e218803. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Frequent Fast-Food Intake | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | ||||||||||||||
| Total | Yes | No | p-Value | Total | Yes | No | p-Value | ||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | ||||
| Total 186,277 | 89,280 | 100.0 | 3992 | 4.5 | 85,288 | 95.5 | 96,997 | 100.0 | 3505 | 3.6 | 93,492 | 96.4 | |||
| Type of Household | |||||||||||||||
| Living with both parents | 74,992 | 85.6 | 3243 | 4.3 | 71,749 | 95.7 | <0.0001 | 81,917 | 85.3 | 2865 | 3.5 | 79,052 | 96.5 | <0.0001 | |
| Living with single parent | 12,016 | 13.7 | 602 | 5.0 | 11,414 | 95.0 | 13,004 | 13.5 | 532 | 4.1 | 12,472 | 95.9 | |||
| Living apart from parents | 1477 | 1.7 | 75 | 5.1 | 1402 | 94.9 | 1554 | 1.6 | 70 | 4.5 | 1484 | 95.5 | |||
| No parents | 795 | 0.9 | 72 | 9.1 | 723 | 90.9 | 522 | 0.5 | 38 | 7.3 | 484 | 92.7 | |||
| Grade | |||||||||||||||
| Middle school 1st | 15,932 | 18.2 | 605 | 3.8 | 15,327 | 96.2 | <0.0001 | 17,049 | 17.8 | 499 | 2.9 | 16,550 | 97.1 | <0.0001 | |
| Middle school 2nd | 15,251 | 17.4 | 664 | 4.4 | 14,587 | 95.6 | 16,743 | 17.4 | 595 | 3.6 | 16,148 | 96.4 | |||
| Middle school 3rd | 14,906 | 17.0 | 726 | 4.9 | 14,180 | 95.1 | 16,558 | 17.2 | 633 | 3.8 | 15,925 | 96.2 | |||
| High school 1st | 14,233 | 16.2 | 667 | 4.7 | 13,566 | 95.3 | 15,441 | 16.1 | 537 | 3.5 | 14,904 | 96.5 | |||
| High school 2nd | 14,617 | 16.7 | 639 | 4.4 | 13,978 | 95.6 | 15,648 | 16.3 | 619 | 4.0 | 15,029 | 96.0 | |||
| High school 3rd | 14,341 | 16.4 | 691 | 4.8 | 13,650 | 95.2 | 15,558 | 16.2 | 622 | 4.0 | 14,936 | 96.0 | |||
| Income | |||||||||||||||
| High | 37,724 | 43.1 | 1742 | 4.6 | 35,982 | 95.4 | <0.0001 | 35,883 | 37.4 | 1263 | 3.5 | 34,620 | 96.5 | <0.0001 | |
| Middle | 40,058 | 45.7 | 1658 | 4.1 | 38,400 | 95.9 | 48,021 | 50.0 | 1639 | 3.4 | 46,382 | 96.6 | |||
| Low | 11,498 | 13.1 | 592 | 5.1 | 10,906 | 94.9 | 13,093 | 13.6 | 603 | 4.6 | 12,490 | 95.4 | |||
| Region | |||||||||||||||
| Capital area | 45,228 | 51.6 | 2009 | 4.4 | 43,219 | 95.6 | 0.4119 | 49,825 | 51.9 | 1790 | 3.6 | 48,035 | 96.4 | 0.2392 | |
| City area | 38,908 | 44.4 | 1769 | 4.5 | 37,139 | 95.5 | 41,253 | 43.0 | 1522 | 3.7 | 39,731 | 96.3 | |||
| Rural | 5144 | 5.9 | 214 | 4.2 | 4930 | 95.8 | 5919 | 6.2 | 193 | 3.3 | 5726 | 96.7 | |||
| Smoking | |||||||||||||||
| Yes | 7415 | 8.5 | 600 | 8.1 | 6815 | 91.9 | <0.0001 | 3025 | 3.1 | 254 | 8.4 | 2771 | 91.6 | <0.0001 | |
| No | 81,865 | 93.4 | 3392 | 4.1 | 78,473 | 95.9 | 93,972 | 97.9 | 3,251 | 3.5 | 90,721 | 96.5 | |||
| Alcohol use | |||||||||||||||
| Yes | 13,821 | 15.8 | 866 | 6.3 | 12,955 | 93.7 | <0.0001 | 11,832 | 12.3 | 672 | 5.7 | 11,160 | 94.3 | <0.0001 | |
| No | 75,459 | 86.1 | 3126 | 4.1 | 72,333 | 95.9 | 85,165 | 88.7 | 2833 | 3.3 | 82,332 | 96.7 | |||
| BMI | |||||||||||||||
| Obese | 17,695 | 20.2 | 854 | 4.8 | 16,841 | 95.2 | 0.0016 | 23,272 | 24.2 | 979 | 4.2 | 22,293 | 95.8 | <0.0001 | |
| Normal | 52,852 | 60.3 | 2378 | 4.5 | 50,474 | 95.5 | 64,531 | 67.2 | 2207 | 3.4 | 62,324 | 96.6 | |||
| Underweight | 18,733 | 21.4 | 760 | 4.1 | 17,973 | 95.9 | 9194 | 9.6 | 319 | 3.5 | 8875 | 96.5 | |||
| Physical activity | |||||||||||||||
| Yes | 77,940 | 89.0 | 3468 | 4.4 | 74,472 | 95.6 | 0.4237 | 68,451 | 71.3 | 2414 | 3.5 | 66,037 | 96.5 | 0.026 | |
| No | 11,340 | 12.9 | 524 | 4.6 | 10,816 | 95.4 | 28,546 | 29.7 | 1091 | 3.8 | 27,455 | 96.2 | |||
| Depressive symptom | |||||||||||||||
| Yes | 17,488 | 19.6 | 1121 | 6.4 | 16,367 | 93.6 | <0.0001 | 30,751 | 31.6 | 1614 | 5.2 | 29,137 | 94.8 | <0.0001 | |
| No | 71,792 | 81.9 | 2871 | 4.0 | 68,921 | 96.0 | 66,246 | 69.0 | 1891 | 2.9 | 64,355 | 97.1 | |||
| Year | |||||||||||||||
| 2017 | 27,916 | 31.9 | 1113 | 4.0 | 26,803 | 96.0 | <0.0001 | 28,851 | 30.0 | 890 | 3.1 | 27,961 | 96.9 | <0.0001 | |
| 2018 | 27,130 | 31.0 | 1089 | 4.0 | 26,041 | 96.0 | 27,994 | 29.2 | 1012 | 3.6 | 26,982 | 96.4 | |||
| 2019 | 15,840 | 18.1 | 847 | 5.3 | 14,993 | 94.7 | 19,150 | 19.9 | 794 | 4.1 | 18,356 | 95.9 | |||
| 2020 | 18,394 | 21.0 | 943 | 5.1 | 17,451 | 94.9 | 21,002 | 21.9 | 809 | 3.9 | 20,193 | 96.1 | |||
| Variables | Frequent Fast-Food Intake | ||||
|---|---|---|---|---|---|
| Boys | Girls | ||||
| OR | 95% CI | OR | 95% CI | ||
| Type of household | |||||
| Living with both parents | 1.00 | 1.00 | |||
| Living with single parent | 1.08 | (0.98–1.19) | 1.03 | (0.93–1.15) | |
| Living apart from parents | 1.04 | (0.80–1.35) | 1.18 | (0.89–1.62) | |
| No parents | 2.00 | (1.52–2.62) | 1.58 | (1.09–2.30) | |
| Grade | |||||
| Middle school | 1st | 0.89 | (0.78–1.01) | 0.83 | (0.72–0.95) |
| 2nd | 1.00 | (0.87–1.14) | 0.96 | (0.84–1.10) | |
| 3rd | 1.10 | (0.97–1.25) | 1.04 | (0.91–1.18) | |
| High school | 1st | 1.06 | (0.94–1.20) | 0.92 | (0.81–1.05) |
| 2nd | 0.96 | (0.85–1.08) | 1.07 | (0.95–1.22) | |
| 3rd | 1.00 | 1.00 | |||
| Income | |||||
| High | 1.00 | 1.00 | |||
| Middle | 0.90 | (0.90–0.97) | 0.96 | (0.88–1.05) | |
| Low | 1.01 | (1.01–1.13) | 1.16 | (1.03–1.30) | |
| Region | |||||
| Capital area | 1.00 | 1.00 | |||
| City area | 1.03 | (0.95–1.11) | 0.99 | (0.92–1.08) | |
| Rural | 1.00 | (0.85–1.19) | 0.86 | (0.72–1.02) | |
| Smoking | |||||
| Yes | 1.69 | (1.52–1.89) | 1.61 | (1.36–1.90) | |
| No | 1.00 | 1.00 | |||
| Alcohol use | |||||
| Yes | 1.24 | (1.12–1.37) | 1.37 | (1.22–1.53) | |
| No | 1.00 | 1.00 | |||
| BMI | |||||
| Obese | 1.14 | (1.05–1.25) | 1.32 | (1.21–1.44) | |
| Normal | 1.00 | 1.00 | |||
| Underweight | 0.89 | (0.81–0.97) | 0.99 | (0.87–1.13) | |
| Physical activity | |||||
| Yes | 1.00 | 1.00 | |||
| No | 1.03 | (0.93–1.15) | 1.07 | (0.98–1.16) | |
| Depressive symptom | |||||
| Yes | 1.49 | (1.37–1.61) | 1.74 | (1.61–1.88) | |
| No | 1.00 | 1.00 | |||
| Year | |||||
| 2017 | 1.00 | 1.00 | |||
| 2018 | 1.04 | (0.94–1.15) | 1.17 | (1.05–1.30) | |
| 2019 | 1.36 | (1.22–1.51) | 1.31 | (1.17–1.47) | |
| 2020 | 1.37 | (1.23–1.52) | 1.26 | (1.12–1.41) | |
| Variables | Frequent Fast Food Intake | ||||||
|---|---|---|---|---|---|---|---|
| Living with Both Parents | Living with Single Parent | Living Apart from Parents | No-Parents | ||||
| OR | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Boys | |||||||
| Income | |||||||
| High | 1.00 | 1.22 | (1.02–1.46) | 1.10 | (0.65–1.87) | 1.81 | (1.16–2.83) |
| Middle | 1.00 | 1.01 | (0.87–1.18) | 0.92 | (0.61–1.38) | 1.64 | (0.96–2.78) |
| Low | 1.00 | 1.04 | (0.85–1.27) | 1.18 | (0.75–1.85) | 2.60 | (1.67–4.07) |
| Year | |||||||
| 2017 | 1.00 | 1.07 | (0.89–1.27) | 1.29 | (0.81–2.06) | 2.35 | (1.50–3.70) |
| 2018 | 1.00 | 0.93 | (0.75–1.15) | 0.74 | (0.42–1.30) | 2.26 | (1.47–3.47) |
| 2019 | 1.00 | 1.18 | (0.95–1.47) | 1.19 | (0.74–1.92) | 1.89 | (0.93–3.83) |
| 2020 | 1.00 | 1.20 | (1.00–1.45) | 0.90 | (0.51–1.59) | 0.71 | (0.25–2.04) |
| Girls | |||||||
| Income | |||||||
| High | 1.00 | 1.22 | (0.99–1.51) | 1.61 | (0.94–2.74) | 2.30 | (1.11–4.80) |
| Middle | 1.00 | 0.97 | (0.83–1.13) | 0.99 | (0.64–1.52) | 0.62 | (0.31–1.23) |
| Low | 1.00 | 0.99 | (0.82–1.21) | 1.13 | (0.69–1.84) | 2.13 | (1.24–3.64) |
| Year | |||||||
| 2017 | 1.00 | 0.90 | (0.72–1.12) | 1.07 | (0.62–1.84) | 1.21 | (0.53–2.77) |
| 2018 | 1.00 | 0.90 | (0.74–1.10) | 0.94 | (0.56–1.59) | 1.93 | (0.98–3.82) |
| 2019 | 1.00 | 1.23 | (0.99–1.51) | 1.07 | (0.56–2.05) | 1.54 | (0.85–2.79) |
| 2020 | 1.00 | 1.18 | (0.95–1.46) | 1.90 | (1.11–3.25) | 1.52 | (0.63–3.67) |
| Variables | Frequent Fast Food Intake | |||
|---|---|---|---|---|
| Boys | Girls | |||
| OR | 95% CI | OR | 95% CI | |
| Type of household | ||||
| Living with both parents | 1.00 | 1.00 | ||
| Living with single parent | 1.08 | (0.98–1.19) | 1.03 | (0.93–1.15) |
| Living apart from parents | ||||
| Living with family or relative | 0.93 | (0.66–1.30) | 1.23 | (0.88–1.71) |
| Living in dormitory or boarding house | 1.15 | (0.74–1.78) | 1.15 | (0.70–1.89) |
| Living in orphanage | 2.07 | (0.84–5.12) | 0.69 | (0.27–1.73) |
| No parents | ||||
| Living with family or relative | 1.85 | (1.36–2.53) | 1.17 | (0.73–1.88) |
| Living in dormitory or boarding house | 4.58 | (2.27–9.23) | 4.40 | (1.75–11.08) |
| Living in orphanage | 1.20 | (0.49–2.99) | 2.17 | (0.94–4.99) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, H.S.; Kang, S.H.; Park, Y.S.; Kang, J.G.; Park, E.C. Association of Household Type and Fast-Food Consumption in Korean Adolescents. Nutrients 2022, 14, 3024. https://doi.org/10.3390/nu14153024
Kwon HS, Kang SH, Park YS, Kang JG, Park EC. Association of Household Type and Fast-Food Consumption in Korean Adolescents. Nutrients. 2022; 14(15):3024. https://doi.org/10.3390/nu14153024
Chicago/Turabian StyleKwon, Hwa Sook, Soo Hyun Kang, Yu Shin Park, Jung Gu Kang, and Eun Cheol Park. 2022. "Association of Household Type and Fast-Food Consumption in Korean Adolescents" Nutrients 14, no. 15: 3024. https://doi.org/10.3390/nu14153024
APA StyleKwon, H. S., Kang, S. H., Park, Y. S., Kang, J. G., & Park, E. C. (2022). Association of Household Type and Fast-Food Consumption in Korean Adolescents. Nutrients, 14(15), 3024. https://doi.org/10.3390/nu14153024