
Profile of Folate in Breast Milk from Chinese Women over 1–400 Days Postpartum

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants and Human Milk Sample Collection
2.2. Quantification of Folate
2.3. Statistical Analysis
3. Results
3.1. Basic Characteristics
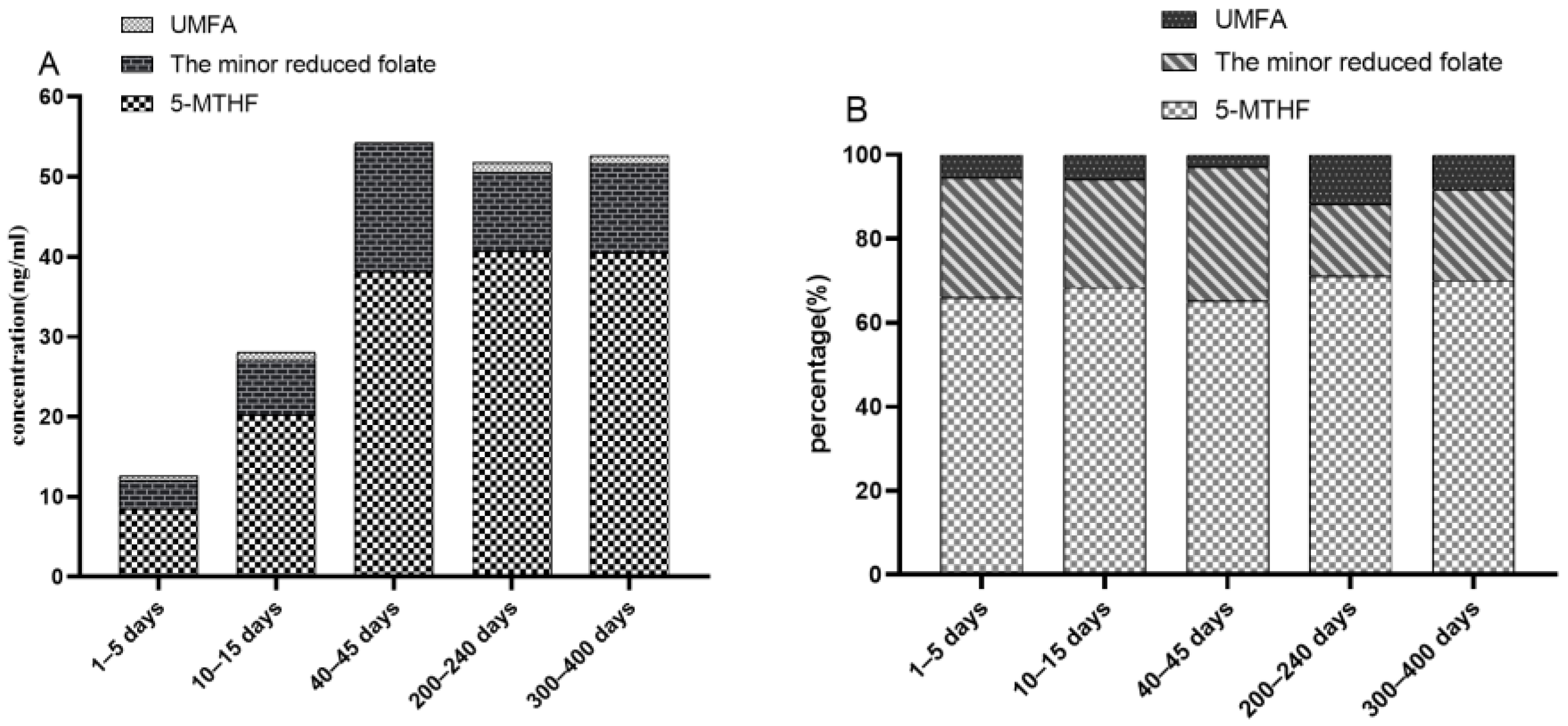
3.2. Milk Folate Levels over Lactational Periods
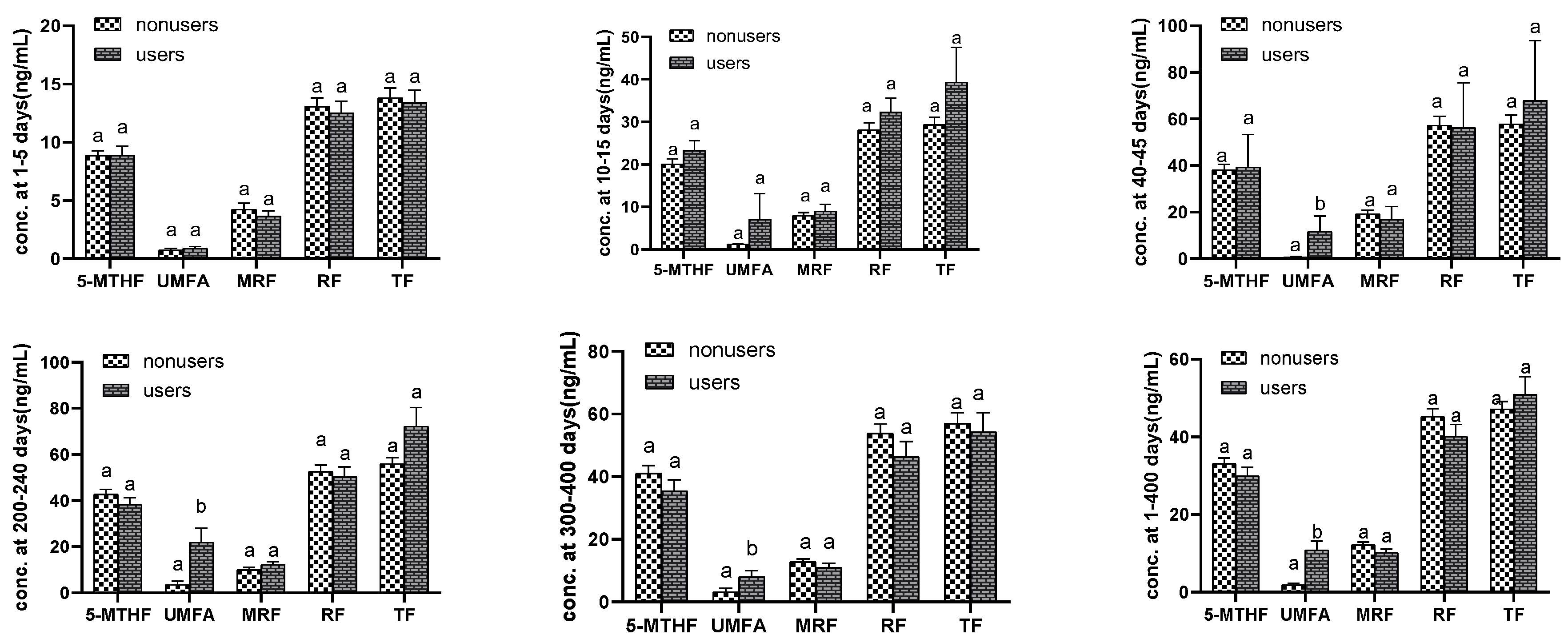
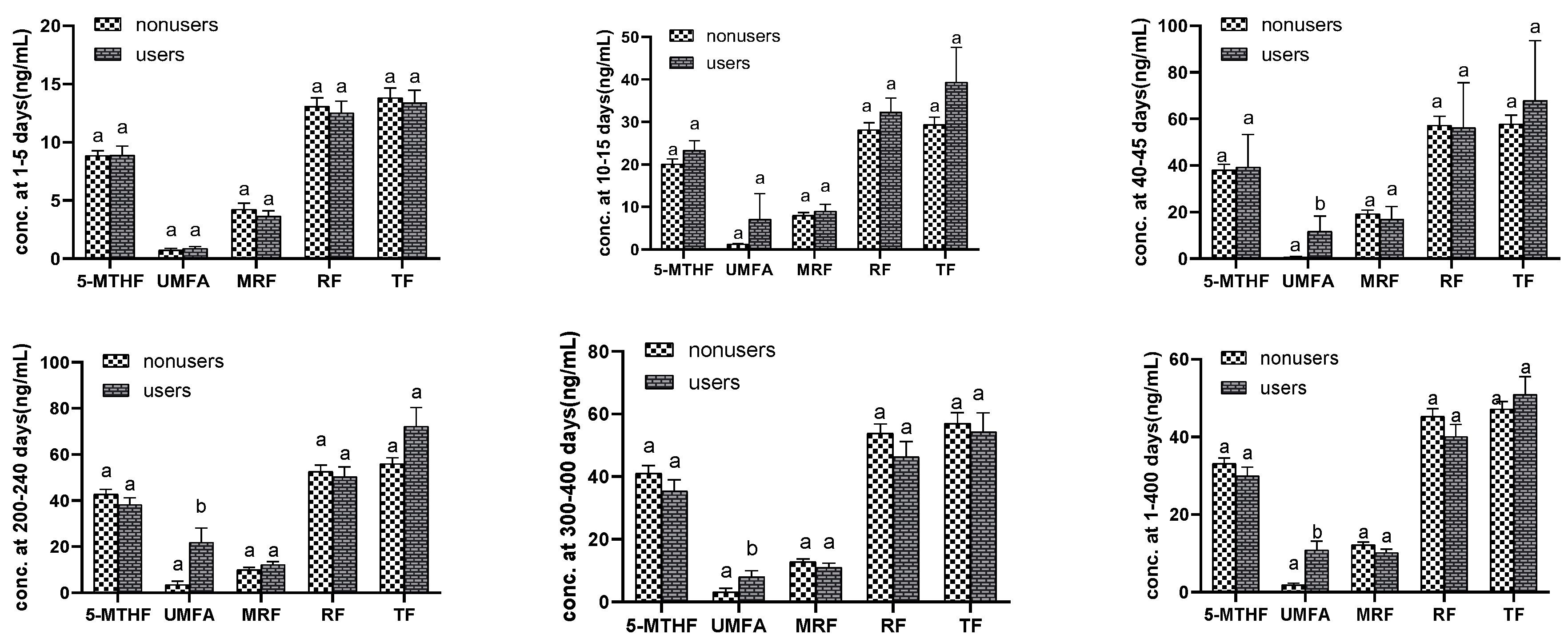
3.3. Supplement Users Compared with Nonusers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shamir, R. The Benefits of Breast Feeding. Nestle Nutr. Inst. Workshop Ser. 2016, 86, 67–76. [Google Scholar] [PubMed] [Green Version]
- ESPGHANCommittee on Nutrition; Agostoni, C.; Braegger, C.; Decsi, T.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; Mihatsch, W.; Moreno, L.A.; Puntis, J.; et al. Breast-feeding: A commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 112–125. [Google Scholar]
- Almeida, C.C.; Mendonça Pereira, B.F.; Leandro, K.C.; Costa, M.P.; Spisso, B.F.; Conte-Junior, C.A. Bioactive Compounds in Infant Formula and Their Effects on Infant Nutrition and Health: A Systematic Literature Review. Int. J. Food Sci. 2021, 2021, 8850080. [Google Scholar] [CrossRef]
- Scaglione, F.; Panzavolta, G. Folate, folic acid and 5-methyltetrahydrofolate are not the same thing. Xenobiotica 2014, 44, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Wang, Y.; Xin, X.; Zhang, Y.; Liu, D.; Peng, Z.; He, Y.; Xu, J.; Ma, X. Effect of folic acid supplementation on preterm delivery and small for gestational age births: A systematic review and meta-analysis. Reprod. Toxicol. 2017, 67, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Hodgetts, V.A.; Morris, K.; Francis, A.; Gardosi, J.; Ismail, K.M. Effectiveness of folic acid supplementation in pregnancy on reducing the risk of small-for-gestational age neonates: A population study, systematic review and meta-analysis. BJOG 2015, 122, 478–490. [Google Scholar] [CrossRef]
- De-Regil, L.M.; Peña-Rosas, J.P.; Fernández-Gaxiola, A.C.; Rayco-Solon, P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects. Cochrane Database Syst. Rev. 2015, 14, Cd007950. [Google Scholar] [CrossRef]
- Gatica-Domínguez, G.; Rothenberg, S.J.; Torres-Sánchez, L.; Schnaas, M.D.L.; Schmidt, R.; López-Carrillo, L. Child dietary intake of folate and vitamin B12 and their neurodevelopment at 24 and 30 months of age. Salud Publica Mex. 2018, 60, 388–394. [Google Scholar] [CrossRef] [Green Version]
- Deoni, S.; Dean, D., 3rd; Joelson, S.; O’Regan, J.; Schneider, N. Early nutrition influences developmental myelination and cognition in infants and young children. Neuroimage 2018, 178, 649–659. [Google Scholar] [CrossRef]
- Strand, T.; Taneja, S.; Ueland, P.M.; Refsum, H.; Bahl, R.; Schneede, J.; Sommerfelt, H.; Bhandari, N. Cobalamin and folate status predicts mental development scores in North Indian children 12–18 mo of age. Am. J. Clin. Nutr. 2013, 97, 310–317. [Google Scholar] [CrossRef] [Green Version]
- Shane, B. Folate and vitamin B12 metabolism: Overview and interaction with riboflavin, vitamin B6, and polymorphisms. Food Nutr. Bull. 2008, 29 (Suppl. 2), S5–S16, discussion S17–S19. [Google Scholar] [CrossRef] [PubMed]
- Page, R.; Robichaud, A.; Arbuckle, T.E.; Fraser, W.D.; Macfarlane, A.J. Total folate and unmetabolized folic acid in the breast milk of a cross-section of Canadian women. Am. J. Clin. Nutr. 2017, 105, 1101–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, D.L.; Tamura, T.; Picciano, M.F. Pteroylpolyglutamates in human milk. Am. J. Clin. Nutr. 1991, 53, 930–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patanwala, I.; King, M.J.; Barrett, D.A.; Rose, J.; Jackson, R.; Hudson, M.; Philo, M.; Dainty, J.R.; Wright, A.J.A.; Finglas, P.M.; et al. Folic acid handling by the human gut: Implications for food fortification and supplementation. Am. J. Clin. Nutr. 2014, 100, 593–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philip, D.; Buch, A.; Moorthy, D.; Scott, T.M.; Parnell, L.D.; Lai, C.-Q.; Ordovás, J.M.; Selhub, J.; Rosenberg, I.H.; Tucker, K.L.; et al. Dihydrofolate reductase 19-bp deletion polymorphism modifies the association of folate status with memory in a cross-sectional multi-ethnic study of adults. Am. J. Clin. Nutr. 2015, 102, 1279–1288. [Google Scholar] [CrossRef] [Green Version]
- Bailey, S.W.; Ayling, J.E. The extremely slow and variable activity of dihydrofolate reductase in human liver and its implications for high folic acid intake. Proc. Natl. Acad. Sci. USA 2009, 106, 15424–15429. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, C.M.; Sternberg, M.R.; Fazili, Z.; Yetley, E.A.; Lacher, D.A.; Bailey, R.L.; Johnson, C.L. Unmetabolized folic acid is detected in nearly all serum samples from US children, adolescents, and adults. J. Nutr. 2015, 145, 520–531. [Google Scholar] [CrossRef] [Green Version]
- Lamers, Y.; Macfarlane, A.J.; O’Connor, D.; Fontaine-Bisson, B. Periconceptional intake of folic acid among low-risk women in Canada: Summary of a workshop aiming to align prenatal folic acid supplement composition with current expert guidelines. Am. J. Clin. Nutr. 2018, 108, 1357–1368. [Google Scholar] [CrossRef] [Green Version]
- Huot, P.; Ly, A.; Szeto, I.M.; Reza-López, S.A.; Cho, D.; Kim, Y.-I.; Anderson, G.H. Maternal and postweaning folic acid supplementation interact to influence body weight, insulin resistance, and food intake regulatory gene expression in rat offspring in a sex-specific manner. Appl. Physiol. Nutr. Metab. 2016, 41, 411–420. [Google Scholar] [CrossRef] [Green Version]
- Raghavan, R.; Selhub, J.; Paul, L.; Ji, Y.; Wang, G.; Hong, X.; Zuckerman, B.; Fallin, M.D.; Wang, X. A prospective birth cohort study on cord blood folate subtypes and risk of autism spectrum disorder. Am. J. Clin. Nutr. 2020, 112, 1304–1317. [Google Scholar] [CrossRef]
- Ford, J.E.; Zechalko, A.; Murphy, J.; Brooke, O.G. Comparison of the B vitamin composition of milk from mothers of preterm and term babies. Arch. Dis. Child. 1983, 58, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Cooperman, J.M.; Dweck, H.S.; Newman, L.J.; Garbarino, C.; Lopez, R. The folate in human milk. Am. J. Clin. Nutr. 1982, 36, 576–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nygren-Babol, L.; Jägerstad, M. Folate-binding protein in milk: A review of biochemistry, physiology, and analytical methods. Crit. Rev. Food Sci. Nutr. 2012, 52, 410–425. [Google Scholar] [CrossRef]
- Chandra-Hioe, M.V.; Bucknall, M.P.; Arcot, J. Evaluating folate extraction from infant milk formulae and adult nutritionals: Enzymatic digestion versus enzyme-free heat treatment. Food Chem. 2017, 234, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Szpylka, J.; De Vries, J.; Cheney, A.; House, S. Determination of total folates in infant formula and adult nutritionals by trienzyme extraction and UPLC-MS/MS Quantitation: First Action 2011.06. J. AOAC Int. 2012, 95, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Xue, Y.; Redeuil, K.M.; Giménez, E.C.; Vinyes-Pares, G.; Zhao, A.; He, T.; Yang, X.; Zheng, Y.; Zhang, Y.; Wang, P.; et al. Regional, socioeconomic, and dietary factors influencing B-vitamins in human milk of urban Chinese lactating women at different lactation stages. BMC Nutr. 2017, 3, 22. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.-H.; Yon, M.; Han, H.-S.; Kim, K.-Y.; Tamura, T.; Hyun, T.H. Folate contents in human milk and casein-based and soya-based formulas, and folate status in Korean infants. Br. J. Nutr. 2009, 101, 1769–1774. [Google Scholar] [CrossRef] [Green Version]
- Hampel, D.; Allen, L.H. Analyzing B-vitamins in Human Milk: Methodological Approaches. Crit. Rev. Food Sci. Nutr. 2016, 56, 494–511. [Google Scholar] [CrossRef]
- Guignard, L.; Nembrini, C.; Moulin, J.; Meisser, K.; Silva-Zolezzi, I.; Kratzsch, J.; Vogel, M.; Kiess, W.; Eckhardt, E. A Rapid Chemiluminescence Assay for Measurement of Folate in Small Volumes of Breast Milk. Molecules 2019, 27, 2730. [Google Scholar] [CrossRef] [Green Version]
- Brown, C.M.; Smith, A.M.; Picciano, M.F. Forms of human milk folacin and variation patterns. J. Pediatr. Gastroenterol. Nutr. 1986, 5, 278–282. [Google Scholar] [CrossRef]
- Bank, M.R.; Kirksey, A.; West, K.; Giacoia, G. Effect of storage time and temperature on folacin and vitamin C levels in term and preterm human milk. Am. J. Clin. Nutr. 1985, 41, 235–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ek, J. Plasma, red cell, and breast milk folacin concentrations in lactating women. Am. J. Clin. Nutr. 1983, 38, 929–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, A.M.; Allen, C.E.; Audus, K.L. Efflux transporters of the human placenta. Adv. Drug. Deliv. Rev. 2003, 55, 125–132. [Google Scholar] [CrossRef]
- Kubo, Y.; Fukuoka, H.; Kawabata, T.; Shoji, K.; Mori, C.; Sakurai, K.; Nishikawa, M.; Ohkubo, T.; Oshida, K.; Yanagisawa, N.; et al. Distribution of 5-Methyltetrahydrofolate and Folic Acid Levels in Maternal and Cord Blood Serum: Longitudinal Evaluation of Japanese Pregnant Women. Nutrients 2020, 12, 1633. [Google Scholar] [CrossRef]
- Obeid, R.; Kasoha, M.; Kirsch, S.H.; Munz, W.; Herrmann, W. Concentrations of unmetabolized folic acid and primary folate forms in pregnant women at delivery and in umbilical cord blood. Am. J. Clin. Nutr. 2010, 92, 1416–1422. [Google Scholar] [CrossRef] [Green Version]
- Mackey, A.D.; Picciano, M.F. Maternal folate status during extended lactation and the effect of supplemental folic acid. Am. J. Clin. Nutr. 1999, 69, 285–292. [Google Scholar] [CrossRef] [Green Version]
- Troesch, B.; Demmelmair, J.; Gimpfl, M.; Hecht, C.; Lakovic, G.; Roehle, R.; Sipka, L.; Trisic, B.; Vusurovic, M.; Schoop, R.; et al. Suitability and safety of L-5-methyltetrahydrofolate as a folate source in infant formula: A randomized-controlled trial. PLoS ONE 2019, 14, e0216790. [Google Scholar] [CrossRef] [Green Version]
- EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA); Turck, D.; Castenmiller, J.; De Henauw, S.; Hirsch-Ernst, K.I.; Kearney, J.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; Naska, A.; et al. Calcium l-methylfolate as a source of folate added for nutritional purposes to infant and follow-on formula, baby food and processed cereal-based food. EFSA J. 2020, 18, e05947. [Google Scholar]
- Smulders, Y.M.; Stehouwer, C.D. Folate metabolism and cardiovascular disease. Semin. Vasc. Med. 2005, 5, 87–97. [Google Scholar] [CrossRef]
- Tymchuk, A.; Keltner, B. Advantage profiles: A tool for health care professionals working with parents with mental retardation. Issues Compr. Pediatr. Nurs. 1991, 14, 155–161. [Google Scholar] [CrossRef]
- Houghton, L.A.; Yang, J.; O’Connor, D.L. Unmetabolized folic acid and total folate concentrations in breast milk are unaffected by low-dose folate supplements. Am. J. Clin. Nutr. 2009, 89, 216–220. [Google Scholar] [CrossRef] [PubMed]
- West, A.A.; Yan, J.; Perry, C.A.; Jiang, X.; Malysheva, O.V.; Caudill, M.A. Folate-status response to a controlled folate intake in nonpregnant, pregnant, and lactating women. Am. J. Clin. Nutr. 2012, 96, 789–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, R.; Wong, A.; Arbuckle, T.E.; Macfarlane, A.J. The MTHFR 677C>T polymorphism is associated with unmetabolized folic acid in breast milk in a cohort of Canadian women. Am. J. Clin. Nutr. 2019, 110, 401–409. [Google Scholar] [CrossRef] [Green Version]
- Frosst, P.; Blom, H.J.; Milos, R.; Goyette, P.; Sheppard, C.A.; Matthews, R.G.; Boers, G.J.H.; den Heijer, M.; Kluijtmans, L.A.J.; van den Heuve, L.P.; et al. A candidate genetic risk factor for vascular disease: A common mutation in methylenetetrahydrofolate reductase. Nat. Genet. 1995, 10, 111–113. [Google Scholar] [CrossRef]
- Crider, K.S.; Zhu, J.H.; Hao, L.; Yang, Q.H.; Yang, T.P.; Gindler, J.; Maneval, D.R.; Quinlivan, E.P.; Li, Z.; Bailey, L.B.; et al. MTHFR 677C→T genotype is associated with folate and homocysteine concentrations in a large, population-based, double-blind trial of folic acid supplementation. Am. J. Clin. Nutr. 2011, 93, 1365–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashfield-Watt, P.A.L.; Pullin, C.H.; Whiting, J.M.; Clark, Z.E.; Moat, S.J.; Newcombe, R.G.; Burr, M.L.; Lewis, M.J.; Powers, H.J.; McDowell, I.F.W. Methylenetetrahydrofolate reductase 677C→T genotype modulates homocysteine responses to a folate-rich diet or a low-dose folic acid supplement: A randomized controlled trial. Am. J. Clin. Nutr. 2002, 76, 180–186. [Google Scholar] [CrossRef]
- Wilcken, B.; Bamforth, F.; Li, Z.; Zhu, H.; Ritvanen, A.; Redlund, M.; Stoll, C.; Alembik, Y.; Dott, B.; Czeizel, A.E.; et al. Geographical and ethnic variation of the 677C>T allele of 5,10 methylenetetrahydrofolate reductase (MTHFR): Findings from over 7000 newborns from 16 areas world wide. J. Med. Genet. 2003, 40, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Ding, Y.; Indayati, W.; Basnet, T.B.; Li, F.; Luo, H.; Pan, H.; Wang, Z. Dietary intake in lactating mothers in China 2018: Report of a survey. Nutr. J. 2020, 19, 72. [Google Scholar] [CrossRef]
- Sneed, S.M.; Zane, C.; Thomas, M.R. The effects of ascorbic acid, vitamin B6, vitamin B12, and folic acid supplementation on the breast milk and maternal nutritional status of low socioeconomic lactating women. Am. J. Clin. Nutr. 1981, 34, 1338–1346. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, M.T.T.; Kim, J.; Lee, H.; Won, S.; Kim, Y.; Jung, J.A.; Li, D.; To, X.H.M.; Huynh, K.T.N.; Van Le, T.; et al. A Comparison of Vitamin and Lutein Concentrations in Breast Milk from Four Asian Countries. Nutrients 2020, 12, 1794. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Days Postpartum (n) | p Value | |||||
|---|---|---|---|---|---|---|
| 1–5 Days (n = 30) | 10–15 Days (n = 30) | 40–45 Days (n = 48) | 200–240 Days (n = 51) | 300–400 Days (n = 46) | ||
| Age (years) | 28.3 ± 3.3 | 29.0 ± 2.2 | 29.6 ± 2.8 | 29.0 ± 3.8 | 29.3 ± 3.0 | 0.483 |
| Gestational age (weeks) | 39.3 ± 0.9 ab | 39.0 ± 1.2 ab | 38.9 ± 1.0 a | 40.0 ± 2.2 b | 40.0 ± 2.1 b | <0.05 |
| Prepregnancy BMI (kg/m2) | 20.5 ± 1.9 | 20.2 ± 2.1 | 20.9 ± 2.7 | 20.9 ± 3.1 | 20.2 ± 2.1 | 0.503 |
| Predelivery BMI (kg/m2) | 26.5 ± 2.5 | 25.4 ± 2.5 | 26.4 ± 2.7 | 26.9 ± 3.1 | 25.7 ± 2.6 | 0.115 |
| Gestational weight (kg) | 15.4 ± 5.1 | 13.3 ± 4.6 | 14.0 ± 4.3 | 15.1 ± 5.7 | 13.9 ± 4.5 | 0.343 |
| Vaginal delivery | 17 (56.7%) | 16 (53.3%) | 23 (47.9%) | 20 (39.2%) | 25 (54.3%) | 0.489 |
| Offspring gender | ||||||
| Male | 14 (46.7%) | 18 (60.0%) | 24 (50.0%) | 31 (60.8%) | 26 (56.5%) | 0.631 |
| Female | 16 (53.3%) | 12 (40.0%) | 24 (50.0%) | 20 (39.2%) | 20 (43.5%) | |
| Offspring weight (g) | 3372.7 ± 315.1 | 3331.0 ± 323.7 | 3416.8 ± 374.6 | 3531.1 ± 864.8 | 3379.1 ± 785.0 | 0.347 |
| Folate | Days Postpartum (n) | ||||
|---|---|---|---|---|---|
| 1–5 Days (n = 30) | 10–15 Days (n = 30) | 40–45 Days (n = 48) | 200–240 Days (n = 51) | 300–400 Days (n = 46) | |
| 5-MTHF | 8.52 (7.51,10.07) c | 20.24 (17.55,23.02) b | 38.06 (22.91,49.01) a | 40.65 (32.58,50.17) a | 40.49 (27.00,48.73) a |
| UMFA | 0.60 (0.51,0.71) b | 0.99 (0.81,1.27) a | 0.00 (0.00,0.66) c | 1.24 (0.94,2.99) a | 1.06 (0.82,8.25) a |
| The minor reduced folate | 3.48 (2.71,4.65) d | 6.83 (5.49,11.07) bc | 16.15 (11.39,24.71) a | 9.89 (5.80,14.05) b | 11.07 (7.81,15.71) b |
| Reduced folate | 12.09 (10.39,14.67) c | 27.52 (23.18,32.02) b | 54.65 (35.91,71.62) a | 51.29 (41.45,62.48) a | 52.71 (34.54,65.38) a |
| Total folate | 12.86 (10.91,15.58) c | 28.42 (26.09,32.97) b | 54.65 (37.42,71.94) a | 56.77 (44.83,73.92) a | 55.14 (35.78,70.58) a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, Y.; Mao, Y.; Tian, F.; Cai, X.; Chen, R.; Li, N.; Qian, C.; Li, X.; Zhao, Y.; Wang, Y. Profile of Folate in Breast Milk from Chinese Women over 1–400 Days Postpartum. Nutrients 2022, 14, 2962. https://doi.org/10.3390/nu14142962
Su Y, Mao Y, Tian F, Cai X, Chen R, Li N, Qian C, Li X, Zhao Y, Wang Y. Profile of Folate in Breast Milk from Chinese Women over 1–400 Days Postpartum. Nutrients. 2022; 14(14):2962. https://doi.org/10.3390/nu14142962
Chicago/Turabian StyleSu, Yanyan, Yingyi Mao, Fang Tian, Xiaokun Cai, Ruidi Chen, Na Li, Changli Qian, Xiang Li, Yanrong Zhao, and Yu Wang. 2022. "Profile of Folate in Breast Milk from Chinese Women over 1–400 Days Postpartum" Nutrients 14, no. 14: 2962. https://doi.org/10.3390/nu14142962
APA StyleSu, Y., Mao, Y., Tian, F., Cai, X., Chen, R., Li, N., Qian, C., Li, X., Zhao, Y., & Wang, Y. (2022). Profile of Folate in Breast Milk from Chinese Women over 1–400 Days Postpartum. Nutrients, 14(14), 2962. https://doi.org/10.3390/nu14142962