
Long Term Physical Activity Improves Quality of Life Perception, Healthy Nutrition, and Daily Life Management in Elderly: A Randomized Controlled Trial

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
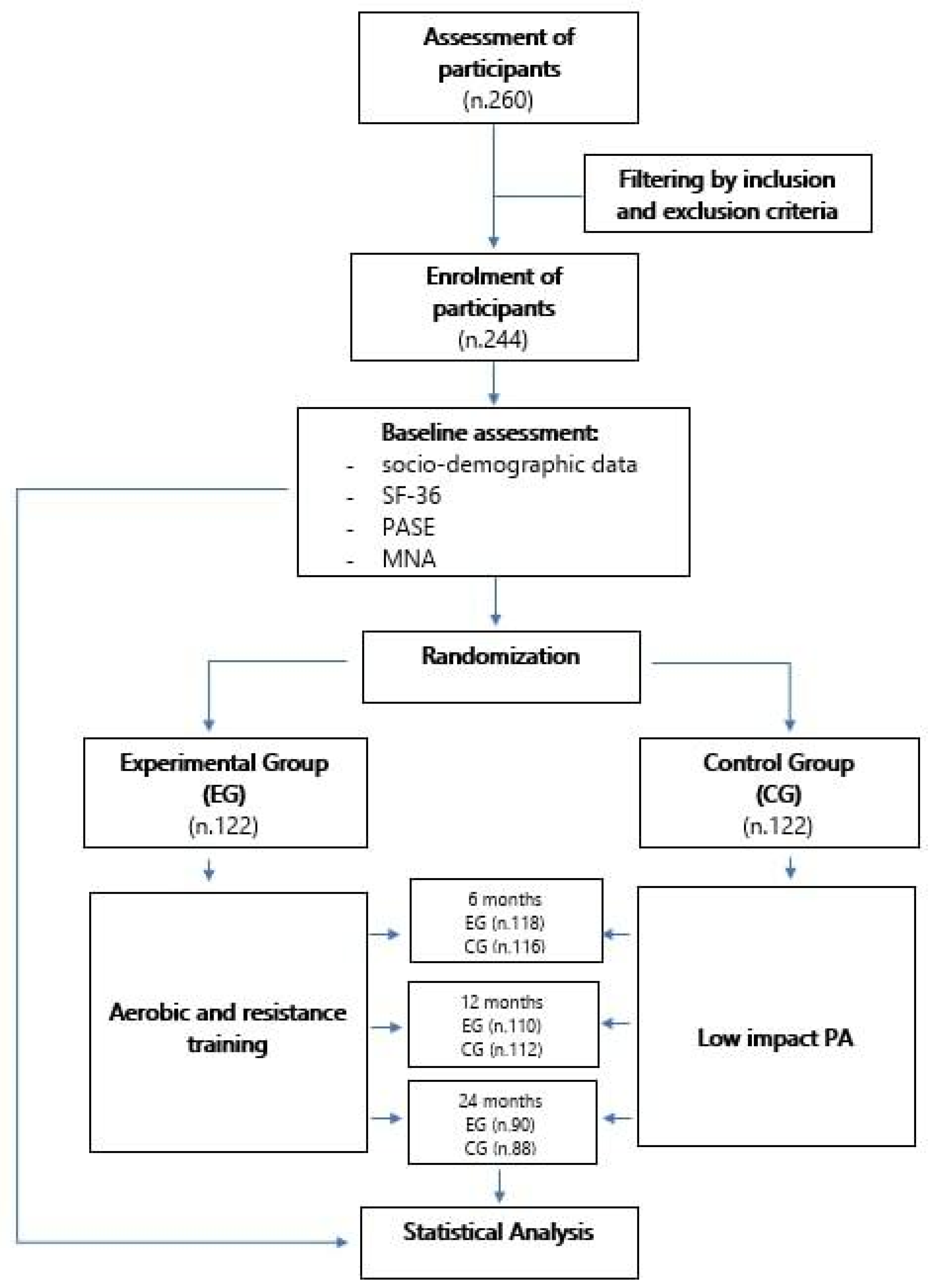
2.1. Participants
2.2. Procedures
2.2.1. Short Form 36-Item
2.2.2. Mini Nutritional Assessment (MNA)
2.2.3. Physical Activity Scale for the Elderly (PASE)
2.3. Intervention
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Campbell, E.; Petermann-Rocha, F.; Welsh, P.; Celis-Morales, C.; Pell, J.P.; Ho, F.K.; Gray, S.R. The effect of exercise on quality of life and activities of daily life in frail older adults: A systematic review of randomised control trials. Exp. Gerontol. 2021, 147, 111287. [Google Scholar] [CrossRef] [PubMed]
- Krawczyk-Suszek, M.; Kleinrok, A. Health-Related Quality of Life (HRQoL) of People over 65 Years of Age. Int. J. Environ. Res. Public Health 2022, 19, 625. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Park, S. A Meta-Analysis of the Correlates of Successful Aging in Older Adults. Res. Aging. 2017, 39, 657–677. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour: Web Annex: Evidence Profiles; World Health Organization: Geneva, Switzerland, 2022; Available online: https://apps.who.int/iris/handle/10665/336657 (accessed on 24 May 2022).
- Mora, F. Successful brain aging: Plasticity, environmental enrichment, and lifestyle. Dialogues Clin. Neurosci. 2013, 15, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Iuliano, E.; Di Cagno, A.; Aquino, G.; Pistone, M.P.; Tsopani, D.; Calcagno, G.; Fiorilli, G. Relationship between physical activity and cognitive decline in aging. Med. Sport. 2016, 69, 151–161. [Google Scholar]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Kivipelto, M. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]
- Leon, M.; Woo, C. Environmental Enrichment and Successful Aging. Front. Behav. Neurosci. 2018, 12, 155. [Google Scholar] [CrossRef] [Green Version]
- Choi, E. Social participation and depressive symptoms in community-dwelling older adults: Emotional social support as a mediator. J. Psychiatr. Res. 2021, 137, 589–596. [Google Scholar] [CrossRef]
- Młynarska, M.; Rudnicka-Drożak, E.; Nowicki, E.; Misztal-Okońska, P.; Dyndur, J.; Majcher, P. The concept of health in the opinion of people over 65 years of age. Gereontol Geriatr. 2015, 1, 11–18. [Google Scholar]
- the LIVSFORSK network; Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.J.; Lin, I.M.; Fan, S.Y. Methodological issues in measuring health-related quality of life. Tzu Chi Med. J. 2013, 25, 8–12. [Google Scholar] [CrossRef] [Green Version]
- The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [CrossRef]
- De Oliveira, L.F.S.; Wanderley, R.L.; de Medeiros, M.M.D.; de Figueredo, O.M.C.; Pinheiro, M.A.; Garcia, R.C.M.R.; De Fátima Dantas de Almeida, L. Health-related quality of life of institutionalized older adults: Influence of physical, nutritional and self-perceived health status. Arch. Gerontol Geriatr. 2021, 92, 104278. [Google Scholar] [CrossRef] [PubMed]
- Porter Starr, K.N.; Borack, M.S.; Rincker, J.C.; Bales, C.W. Nutrition and aging: Meeting the unique needs of older adults. In Nutrition Guide for Physicians and Related Healthcare Professions. Nutrition and Health; Wilson, T., Temple, N.J., Bray, G.A., Eds.; Humana Press: Totowa, NJ, USA, 2022; pp. 59–69. [Google Scholar] [CrossRef]
- Di Cagno, A.; Marchetti, M.; Battaglia, C.; Giombini, A.; Calcagno, G.; Fiorilli, G.; Piazza, M.; Pigozzi, F.; Borrione, P. Is menstrual delay a serious problem for elite rhythmic gymnasts? J. Sports Med. Phys. Fit. 2012, 52, 7. [Google Scholar]
- Zhou, Z.F.; Wang, D.; Li, X.M.; Zhang, C.L.; Wu, C.Y. Effects of enhanced external counterpulsation on exercise capacity and quality of life in patients with chronic heart failure: A meta-analysis. Medicine 2021, 100, e26536. [Google Scholar] [CrossRef]
- Chen, S.; Malete, L.; Ling, J. An examination of physical activity guidelines and health-related quality of life among U.S. older adults. Prev. Med. 2022, 156, 106986. [Google Scholar] [CrossRef]
- Pate, R.R.; O’Neill, J.R.; Lobelo, F. The Evolving Definition of “Sedentary”. Exerc. Sport Sci. Rev. 2008, 36, 173–178. [Google Scholar] [CrossRef]
- Enright, P.L. The Six-Minute Walk Test. Respir. Care 2003, 48, 3. [Google Scholar]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. In Medical Care; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1992; p. 12. [Google Scholar]
- Guigoz, Y.; Vellas, B. The mini nutritional assessment (MNA) for grading the nutritional state of elderly patients: Presentation of the MNA, history and validation. In Nestlè Nutrition Workshop Series: Clinical & Performance Program; Vellas, B., Garry, P.J., Guigoz, Y., Eds.; Karger Publishers: Basel, Switzerland; Nestlè Center, Nestec Ltd.: Basel, Switzerland, 1999; Volume 1, pp. 3–12. [Google Scholar] [CrossRef] [Green Version]
- Washburn, R.A.; Smith, K.W.; Jette, A.M.; Janney, C.A. The physical activity scale for the elderly (PASE): Development and evaluation. J. Clin. Epidemiol. 1993, 46, 153–162. [Google Scholar] [CrossRef]
- Eshaghi, S.R.; Arash Rame, M.; Shahsanaee, A.; Pooya, A. Validity and Reliability of the Short Form- 36 Items Questionnaire as a Measure of Quality of Life in Elderly Iranian Population. Am. J. Appl Sci. 2006, 3, 1763–1766. [Google Scholar] [CrossRef]
- Bleda, M.J.; Bolibar, I.; Pares, R.; Salva, A. Reliability of the mini nutritional assessment (MNA) in institutionalized elderly people. J. Nutr. 2002, 6, 134–137. [Google Scholar]
- Logan, S.; Gottlieb, B.; Maitland, S.; Meegan, D.; Spriet, L. The Physical Activity Scale for the Elderly (PASE) Questionnaire; Does It Predict Physical Health? Int. J. Environ. Res. Public Health 2013, 10, 3967–3986. [Google Scholar] [CrossRef] [PubMed]
- Washburn, R.A.; McAuley, E.; Katula, J.; Mihalko, S.L.; Boileau, R.A. The physical activity scale for the elderly (PASE): Evidence for validity. J. Clin. Epidemiol. 1999, 52, 643–651. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; David, C.; Swain, D.P. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Bigliassi, M.; Karageorghis, C.I.; Wright, M.J.; Orgs, G.; Nowicky, A.V. Effects of auditory stimuli on electrical activity in the brain during cycle ergometry. Physiol. Behav. 2017, 177, 135–147. [Google Scholar] [CrossRef]
- Pawłowska-Cyprysiak, K.; Konarska, M.; Żołnierczyk-Zreda, D. Self-Perceived Quality of Life of People with Physical Disabilities and Labour Force Participation. Int J. Occup. Saf. Ergon. 2013, 19, 185–194. [Google Scholar] [CrossRef]
- Borglin, G.; Jakobsson, U.; Edberg, A.K.; Hallberg, I.R. Self-reported health complaints and their prediction of overall and health-related quality of life among elderly people. Int. J. Nur. Stud. 2005, 42, 147–158. [Google Scholar] [CrossRef]
- Akosile, C.O.; Igwemmadu, C.K.; Okoye, E.C.; Odole, A.C.; Mgbeojedo, U.G.; Fabunmi, A.A.; Onwuakagba, I.U. Physical activity level, fear of falling and quality of life: A comparison between community-dwelling and assisted-living older adults. BMC Geriatr. 2021, 21, 12. [Google Scholar] [CrossRef]
- Iuliano, E.; di Cagno, A.; Cristofano, A.; Angiolillo, A.; D’Aversa, R.; Ciccotelli, S.; Corbi, G.; Fiorilli, G.; Calcagno, G.; Di Costanzo, A.; et al. Physical exercise for prevention of dementia (EPD) study: Background, design and methods. BMC Public Health 2019, 19, 659. [Google Scholar] [CrossRef]
- Demurtas, J.; Schoene, D.; Torbahn, G.; Marengoni, A.; Grande, G.; Zou, L.; Petrovic, M.; Maggi, S.; Cesari, M.; Lamb, S.; et al. Physical Activity and Exercise in Mild Cognitive Impairment and Dementia: An Umbrella Review of Intervention and Observational Studies. J. Am. Med. Dir. Assoc. 2020, 21, 1415–1422.e6. [Google Scholar] [CrossRef]
- Cupisti, A.; D’Alessandro, C.; Finato, V.; Del Corso, C.; Catania, B.; Caselli, G.M.; Egidi, M.F. Assessment of physical activity, capacity and nutritional status in elderly peritoneal dialysis patients. BMC Nephrol. 2017, 18, 180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, W.; Ik Suh, Y.; Ryu, J.; Heo, J. Physical Activity Levels and Well-Being in Older Adults. Psychol. Rep. 2017, 120, 192–205. [Google Scholar] [CrossRef] [PubMed]
- Costigan, S.A.; Lubans, D.R.; Lonsdale, C.; Sanders, T.; del Pozo Cruz, B. Associations between physical activity intensity and well-being in adolescents. Prev. Med. 2019, 125, 55–61. [Google Scholar] [CrossRef]
- Netz, Y.; Wu, M.J.; Becker, B.J.; Tenenbaum, G. Physical Activity and Psychological Well-Being in Advanced Age: A Meta-Analysis of Intervention Studies. Psychol. Aging 2005, 20, 272–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eime, R.; Harvey, J.; Payne, W. Dose-Response of Women’s Health-Related Quality of Life (HRQoL) and Life Satisfaction to Physical Activity. J. Phys. Act. Health 2014, 11, 330–338. [Google Scholar] [CrossRef]
- Abd El-Kader, S.M.; Al-Jiffri, O.H. Aerobic exercise improves quality of life, psychological well-being and systemic inflammation in subjects with Alzheimer’s disease. Afr. Health Sci. 2017, 16, 1045. [Google Scholar] [CrossRef] [PubMed]
- Amarantos, E.; Martinez, A.; Dwyer, J. Nutrition and Quality of Life in Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56 (Suppl. 2), 54–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buonsenso, A.; Fiorilli, G.; Mosca, C.; Centorbi, M.; Notarstefano, C.C.; Di Martino, G.; Calcagno, G.; Intrieri, M.; di Cagno, A. Exploring the Enjoyment of the Intergenerational Physical Activity. J. Funct. Morphol. Kinesiol. 2021, 6, 51. [Google Scholar] [CrossRef] [PubMed]
- Farrance, C.; Tsofliou, F.; Clark, C. Adherence to community based group exercise interventions for older people: A mixed-methods systematic review. Prev. Med. 2016, 87, 155–166. [Google Scholar] [CrossRef] [Green Version]
- Gabriel, K.P.; McClain, J.J.; Schmid, K.K.; Storti, K.L.; High, R.R.; Underwood, D.A.; Kuller, L.H.; Kriska, A.M. Issues in accelerometer methodology: The role of epoch length on estimates of physical activity and relationships with health outcomes in overweight, post-menopausal women. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 53. [Google Scholar] [CrossRef] [Green Version]
- Besson, H.; Brage, S.; Jakes, R.W.; Ekelund, U. Wareham NJ. Estimating physical activity energy expenditure, sedentary time, and physical activity intensity by self-report in adults. Am. J. Clin. Nutr. 2010, 91, 106–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delerue Matos, A.; Barbosa, F.; Cunha, C.; Voss, G.; Correia, F. Social isolation, physical inactivity and inadequate diet among European middle-aged and older adults. BMC Public Health 2021, 21, 924. [Google Scholar] [CrossRef] [PubMed]
- Bailly, N.; Maître, I.; Wymelbeke, V.V. Relationships between nutritional status, depression and pleasure of eating in aging men and women. Arch. Gerontol. Geriatr. 2015, 61, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Bennie, J.A.; De Cocker, K.; Duncan, M.J. Associations of muscle-strengthening and aerobic exercise with self-reported components of sleep health among a nationally representative sample of 47,564 US adults. Sleep Health 2021, 7, 281–288. [Google Scholar] [CrossRef]
- Awick, E.A.; Wójcicki, T.R.; Olson, E.A.; Fanning, J.; Chung, H.D.; Zuniga, K.; Mackenzie, M.; Kramer, A.F.; McAuley, E. Differential exercise effects on quality of life and health-related quality of life in older adults: A randomized controlled trial. Qual. Life Res. 2015, 24, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Rejeski, W.J.; Mihalko, S.L. Physical activity and quality of life in older adults. Gerontol. A Biol. Sci. Med. Sci. 2001, 56 (Suppl. 2), 23–35. [Google Scholar] [CrossRef] [Green Version]
- Charlton, K.; Walton, K.; Brumerskyj, K.; Halcomb, E.; Hull, A.; Comerford, T.; Do Rosario, V.A. Model of nutritional care in older adults: Improving the identification and management of malnutrition using the Mini Nutritional Assessment–Short Form (MNA®-SF) in general practice. Aust. J. Prim. Health 2021, 28, 23–32. [Google Scholar] [CrossRef]
- Buecker, S.; Horstmann, K.T.; Krasko, J.; Kritzler, S.; Terwiel, S.; Kaiser, T.; Luhmann, M. Changes in daily loneliness for German residents during the first four weeks of the COVID-19 pandemic. Soc. Sci. Med. 2020, 265, 113541. [Google Scholar] [CrossRef]
- Iuliano, E.; Fiorilli, G.; Aquino, G.; Di Costanzo, A.; Calcagno, G.; di Cagno, A. Twelve-Week Exercise Influences Memory Complaint but not Memory Performance in Older Adults: A Randomized Controlled Study. J. Aging Phys. Act. 2017, 25, 612–620. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n |
|---|---|
| Experimental group | 90 |
| Age (mean ± SD) | 62.12 ± 7.88 |
| Gender | |
| Male | 32 |
| Female | 58 |
| PASE | 108.48 ± 45.21 |
| Control group | 88 |
| Age (mean ± SD) | 65.64 ± 8.12 |
| Gender | |
| Male | 28 |
| Female | 62 |
| PASE | 108.22 ± 47.04 |
| Variable | Time | EG | CG | Significant Results |
|---|---|---|---|---|
| Means ± SD | Means ± SD | |||
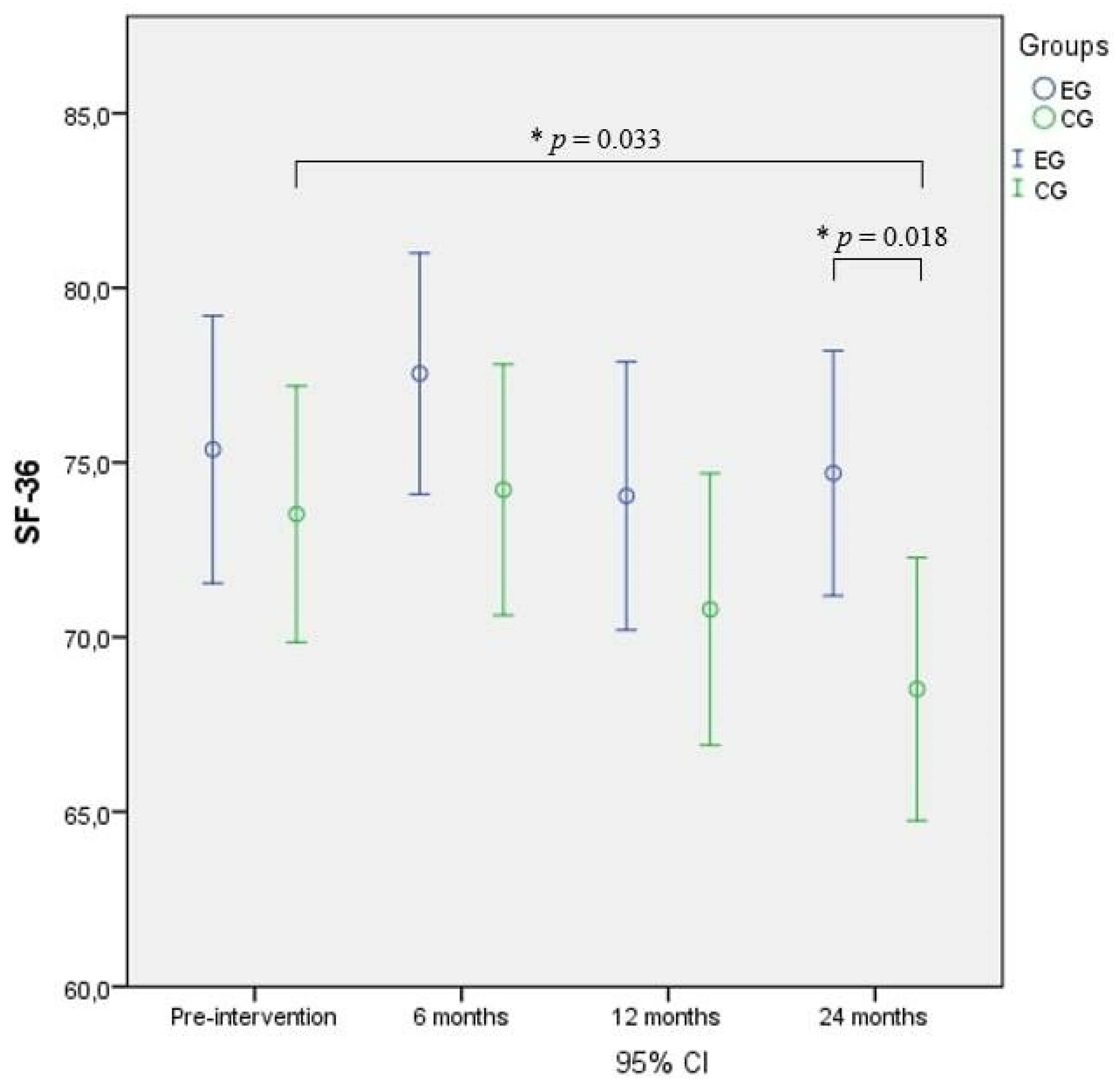
| SF-36 | Baseline | 75.37 ± 17.51 | 73.52 ± 16.80 a | a the score of CG at 24 months was significantly lower compared to the CG baseline score (p = 0.033), b the score of CG at 24 months was significantly lower compared with EG at 24 months (p = 0.018). |
| 6 months | 77.55 ± 15.80 | 74.22 ± 16.48 | ||
| 12 months | 74.04 ± 17.58 | 70.79 ± 17.82 | ||
| 24 months | 74.69 ± 16.06 b | 68.51 ± 17.25 a,b | ||
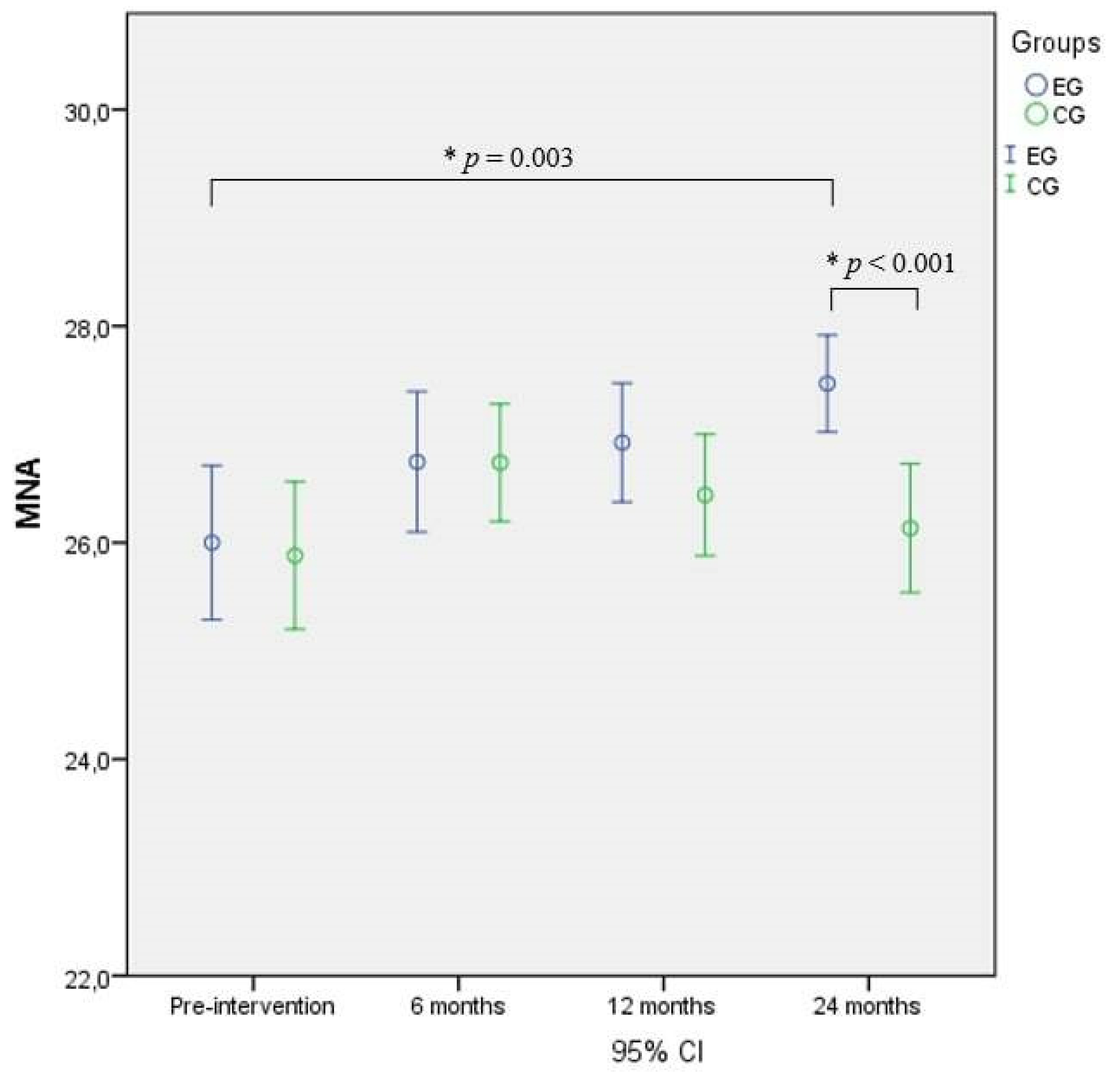
| MNA | Baseline | 26.00 ± 2.90 c | 25.88 ± 2.79 | c the score of EG at 24 months was significantly higher compared to the EG baseline score (p = 0.003), d the score of EG at 24 months was significantly higher compared with CG at 24 months (p < 0.001). |
| 6 months | 26.75 ± 2.64 | 26.74 ± 2.23 | ||
| 12 months | 26.92 ± 2.23 | 26.44 ± 2.30 | ||
| 24 months | 27.47 ± 1.82 c,d | 26.13 ± 2.44 d | ||
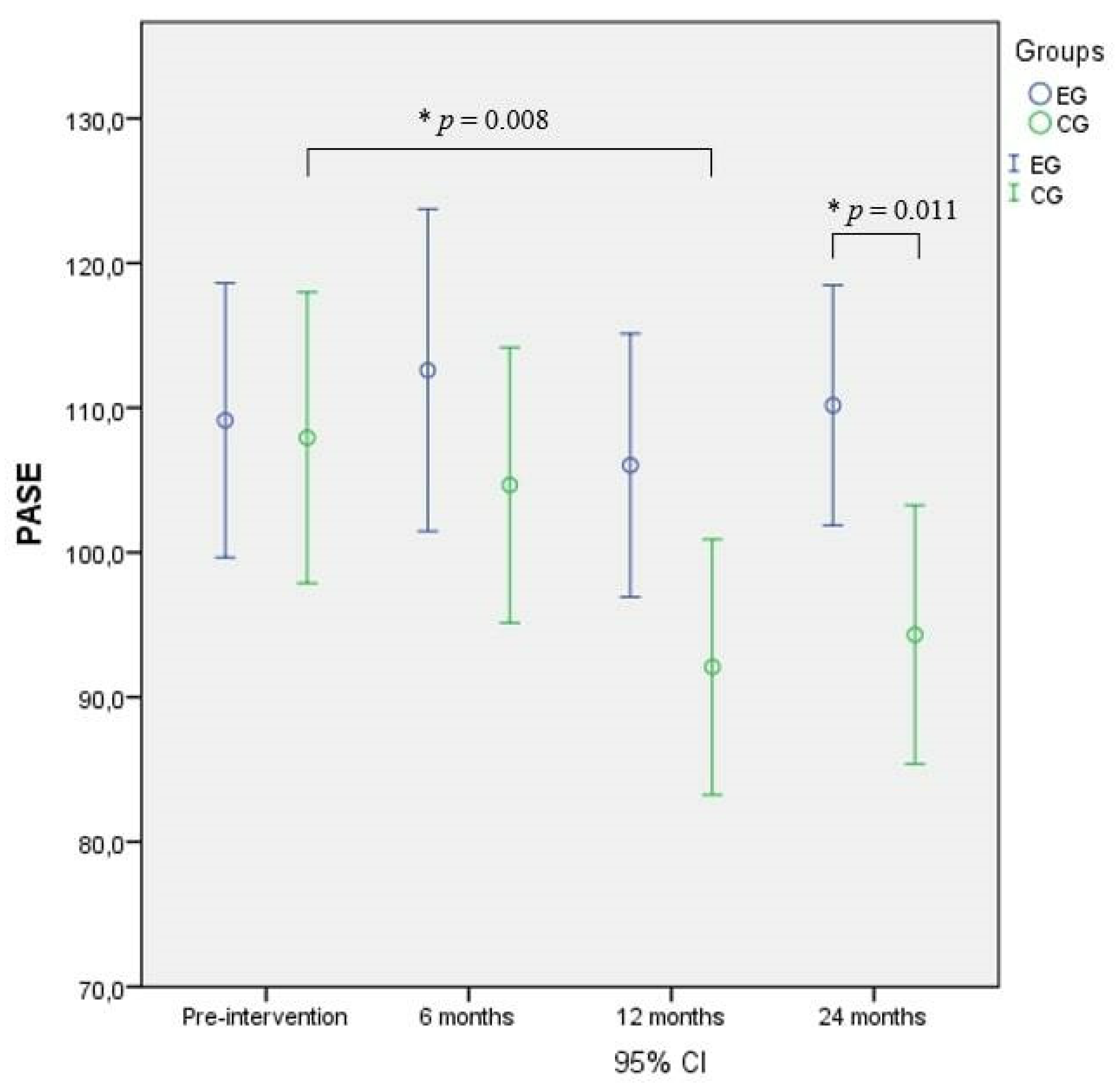
| PASE | Baseline | 109.13 ± 45.03 | 107.93 ± 47.23 e | e the score of EG at 24 months was significantly higher compared to the EG baseline score (p = 0.008), f the score of CG at 12 months was significantly lower compared with CG baseline score (p = 0.011). |
| 6 months | 112.59 ± 52.87 | 104.66 ± 44.65 | ||
| 12 months | 106.02 ± 43.21 | 92.08 ± 41.97 e | ||
| 24 months | 110.17 ± 39.40 f | 94.31 ± 41.97 f |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorilli, G.; Buonsenso, A.; Centorbi, M.; Calcagno, G.; Iuliano, E.; Angiolillo, A.; Ciccotelli, S.; di Cagno, A.; Di Costanzo, A. Long Term Physical Activity Improves Quality of Life Perception, Healthy Nutrition, and Daily Life Management in Elderly: A Randomized Controlled Trial. Nutrients 2022, 14, 2527. https://doi.org/10.3390/nu14122527
Fiorilli G, Buonsenso A, Centorbi M, Calcagno G, Iuliano E, Angiolillo A, Ciccotelli S, di Cagno A, Di Costanzo A. Long Term Physical Activity Improves Quality of Life Perception, Healthy Nutrition, and Daily Life Management in Elderly: A Randomized Controlled Trial. Nutrients. 2022; 14(12):2527. https://doi.org/10.3390/nu14122527
Chicago/Turabian StyleFiorilli, Giovanni, Andrea Buonsenso, Marco Centorbi, Giuseppe Calcagno, Enzo Iuliano, Antonella Angiolillo, Santina Ciccotelli, Alessandra di Cagno, and Alfonso Di Costanzo. 2022. "Long Term Physical Activity Improves Quality of Life Perception, Healthy Nutrition, and Daily Life Management in Elderly: A Randomized Controlled Trial" Nutrients 14, no. 12: 2527. https://doi.org/10.3390/nu14122527
APA StyleFiorilli, G., Buonsenso, A., Centorbi, M., Calcagno, G., Iuliano, E., Angiolillo, A., Ciccotelli, S., di Cagno, A., & Di Costanzo, A. (2022). Long Term Physical Activity Improves Quality of Life Perception, Healthy Nutrition, and Daily Life Management in Elderly: A Randomized Controlled Trial. Nutrients, 14(12), 2527. https://doi.org/10.3390/nu14122527