
The Association of Dietary Fiber Intake in Three Meals with All-Cause and Disease-Specific Mortality among Adults: The U.S. National Health and Nutrition Examination Survey, 2003–2014

Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Dietary Assessment
2.3. Main Exposure
2.4. Main Outcomes
2.5. Confounding and Effect Modification Measurements
2.6. Statistical Analysis
2.7. Sensitivity Analysis
3. Results
3.1. Baseline Characteristics
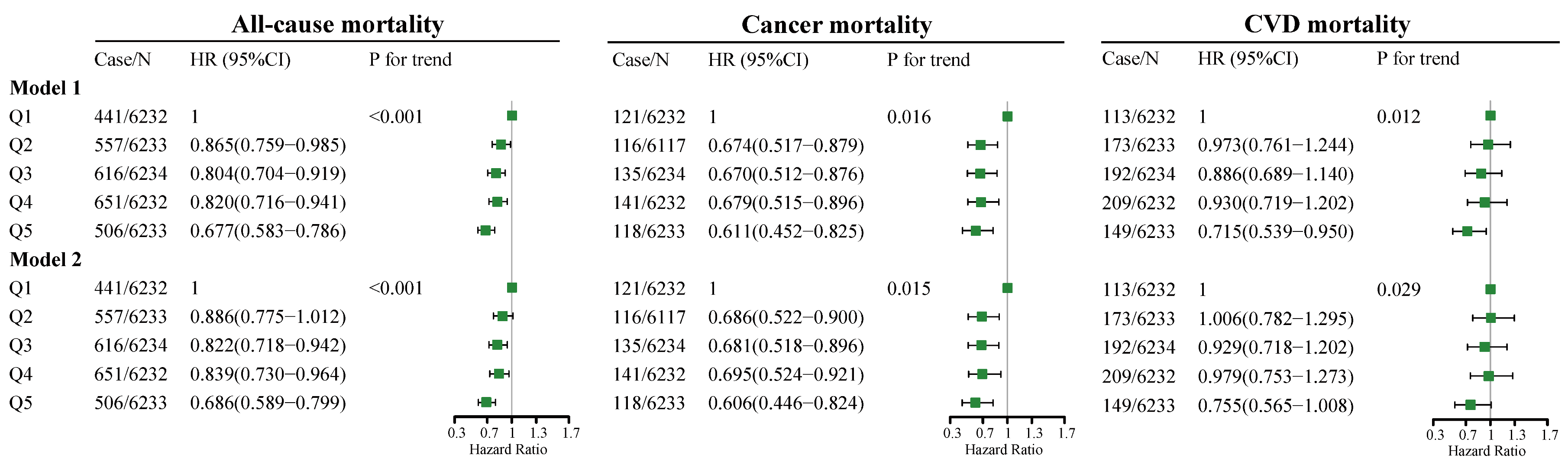
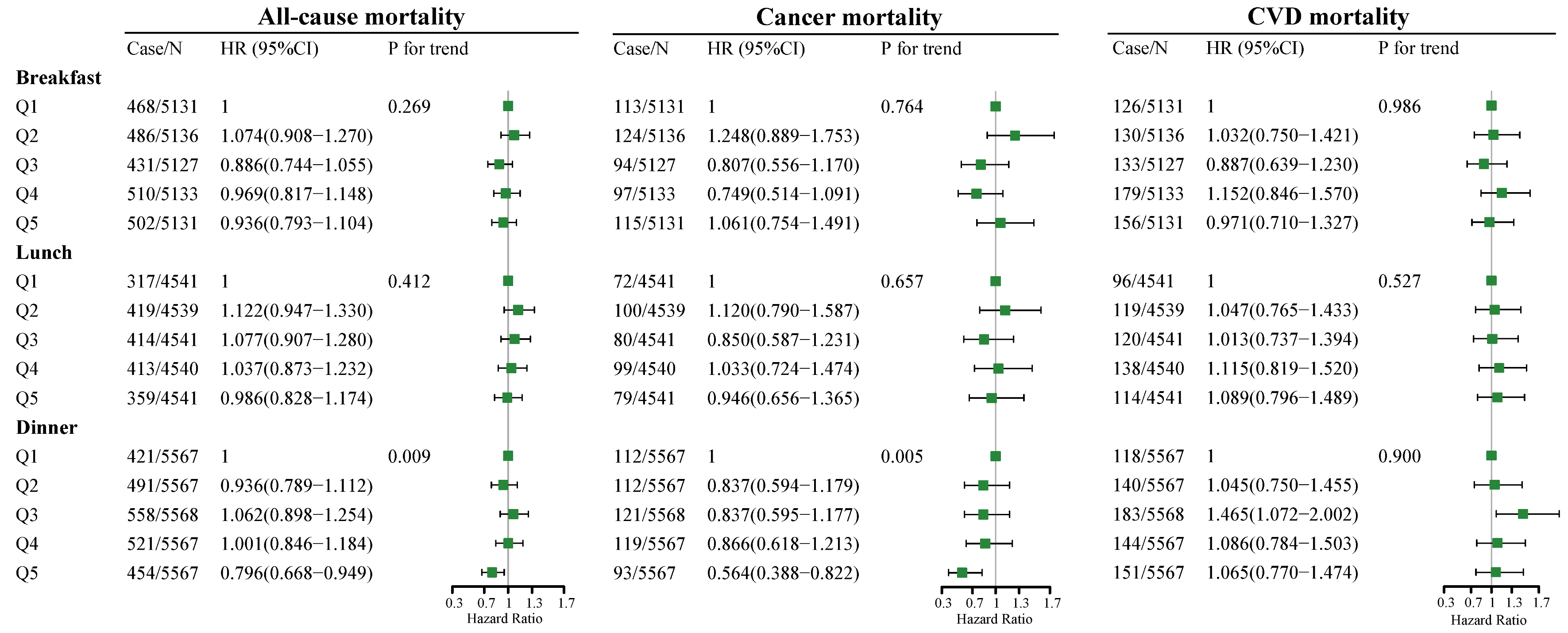
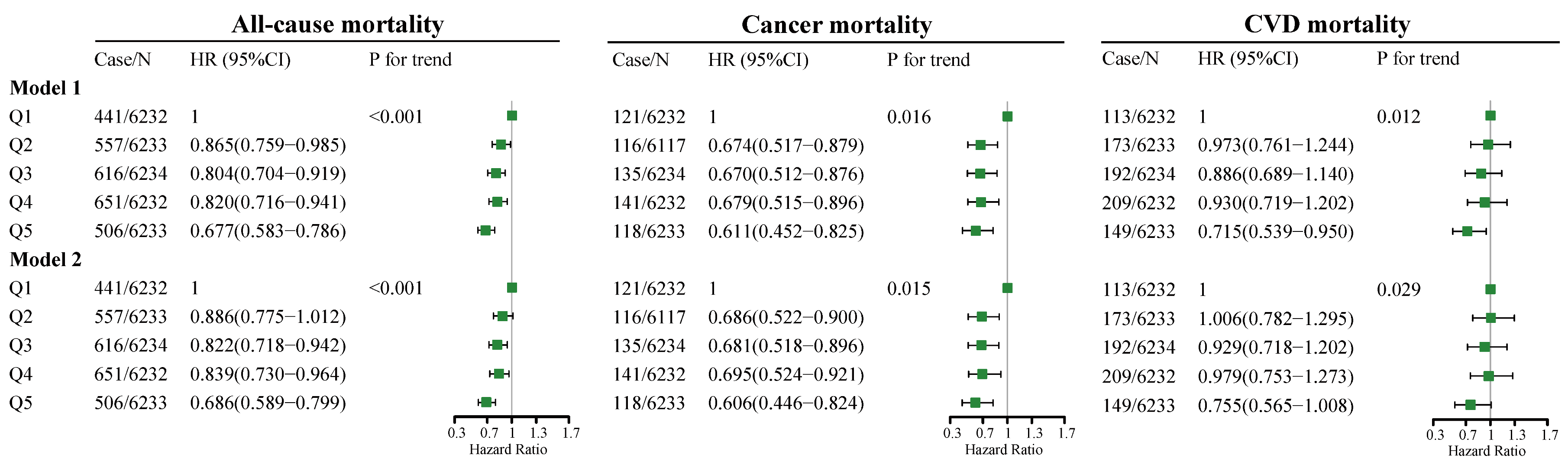
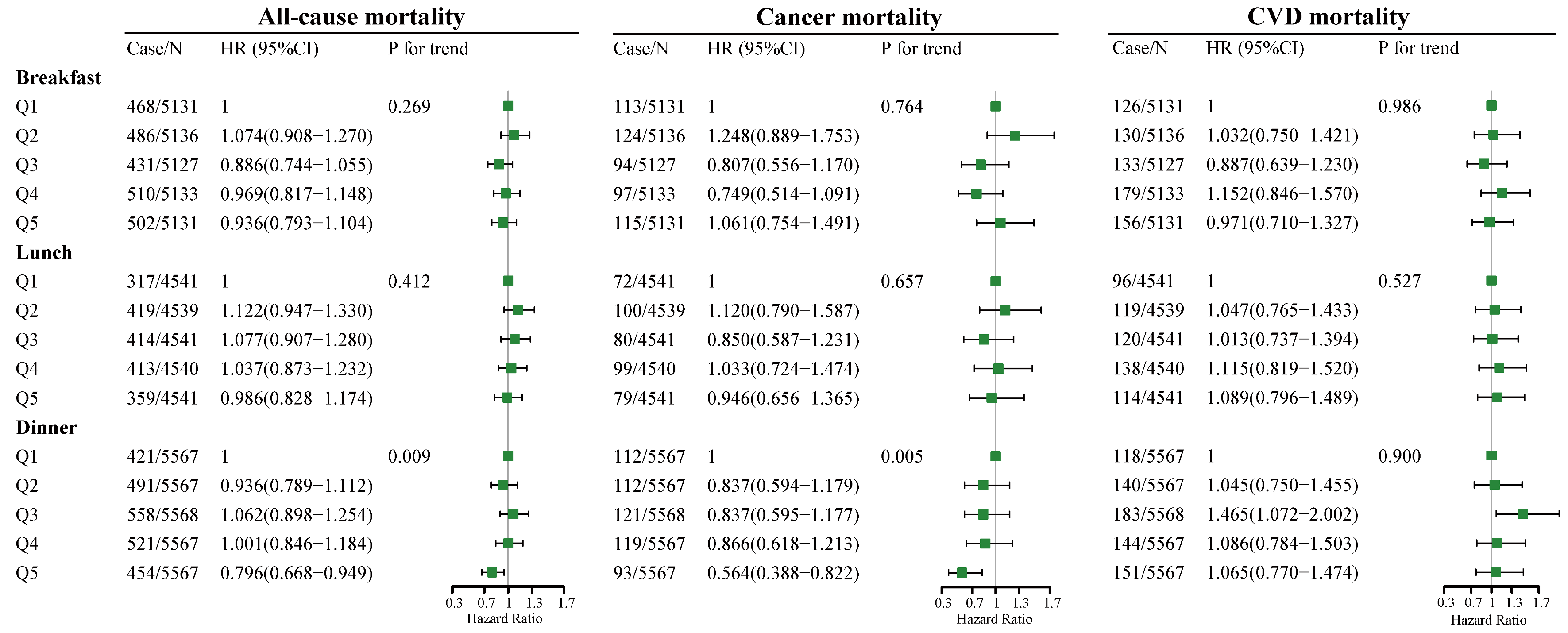
3.2. Cox Proportional Hazards Models
3.3. Equivalent Substitution Analysis
3.4. Sensitivity Analysis
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Asher, G.; Sassone-Corsi, P. Time for food: The intimate interplay between nutrition, metabolism, and the circadian clock. Cell 2015, 161, 84–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, K.; Pivovarova-Ramich, O. Meal Timing, Aging, and Metabolic Health. Int. J. Mol. Sci. 2019, 20, 1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, T.; Gao, J.; Wang, L.; Li, C.; Qi, L.; Sun, C.; Li, Y. The Association of Energy and Macronutrient Intake at Dinner Versus Breakfast With Disease-Specific and All-Cause Mortality Among People With Diabetes: The U.S. National Health and Nutrition Examination Survey, 2003–2014. Diabetes Care 2020, 43, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Shafi, A.A.; Knudsen, K.E. Cancer and the Circadian Clock. Cancer Res. 2019, 79, 3806–3814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.; Wei, W.; Xu, J.; Huang, J.; Li, L.; Han, T.; Qi, J.; Sun, C.; Li, Y.; Jiang, W. The association of minerals intake in three meals with cancer and all-cause mortality: The U.S. National Health and Nutrition Examination Survey, 2003–2014. BMC Cancer 2021, 21, 912. [Google Scholar] [CrossRef] [PubMed]
- Hatori, M.; Vollmers, C.; Zarrinpar, A.; DiTacchio, L.; Bushong, E.A.; Gill, S.; Leblanc, M.; Chaix, A.; Joens, M.; Fitzpatrick, J.A.; et al. Time-restricted feeding without reducing caloric intake prevents metabolic diseases in mice fed a high-fat diet. Cell Metab. 2012, 15, 848–860. [Google Scholar] [CrossRef] [Green Version]
- Srour, B.; Plancoulaine, S.; Andreeva, V.A.; Fassier, P.; Julia, C.; Galan, P.; Hercberg, S.; Deschasaux, M.; Latino-Martel, P.; Touvier, M. Circadian nutritional behaviours and cancer risk: New insights from the NutriNet-sante prospective cohort study: Disclaimers. Int. J. Cancer 2018, 143, 2369–2379. [Google Scholar] [CrossRef] [Green Version]
- DeVries, J.W. On defining dietary fibre. Proc. Nutr. Soc. 2003, 62, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Lattimer, J.M.; Haub, M.D. Effects of dietary fiber and its components on metabolic health. Nutrients 2010, 2, 1266–1289. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Wang, S.; Liu, J. Fiber consumption and all-cause, cardiovascular, and cancer mortalities: A systematic review and meta-analysis of cohort studies. Mol. Nutr. Food Res. 2015, 59, 139–146. [Google Scholar] [CrossRef]
- Sun, L.; Zhang, Z.; Xu, J.; Xu, G.; Liu, X. Dietary fiber intake reduces risk for Barrett’s esophagus and esophageal cancer. Crit. Rev. Food Sci. Nutr. 2017, 57, 2749–2757. [Google Scholar] [CrossRef] [PubMed]
- Farvid, M.S.; Spence, N.D.; Holmes, M.D.; Barnett, J.B. Fiber consumption and breast cancer incidence: A systematic review and meta-analysis of prospective studies. Cancer 2020, 126, 3061–3075. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Hunter, D.J.; Spiegelman, D.; Bergkvist, L.; Berrino, F.; van den Brandt, P.A.; Buring, J.E.; Colditz, G.A.; Freudenheim, J.L.; Fuchs, C.S.; et al. Dietary fiber intake and risk of colorectal cancer: A pooled analysis of prospective cohort studies. JAMA 2005, 294, 2849–2857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slavin, J.L. Dietary fiber and body weight. Nutrition 2005, 21, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.L. Position of the American Dietetic Association: Health implications of dietary fiber. J. Am. Diet. Assoc. 2008, 108, 1716–1731. [Google Scholar]
- Tucker, L.A.; Thomas, K.S. Increasing total fiber intake reduces risk of weight and fat gains in women. J. Nutr. 2009, 139, 576–581. [Google Scholar] [CrossRef] [Green Version]
- Lu, L.; Huang, Y.-F.; Wang, M.-Q.; Chen, D.-X.; Wan, H.; Wei, L.-B.; Xiao, W. Dietary fiber intake is associated with chronic kidney disease (CKD) progression and cardiovascular risk, but not protein nutritional status, in adults with CKD. Asia Pac. J. Clin. Nutr. 2017, 26, 598–605. [Google Scholar] [CrossRef]
- Hopping, B.N.; Erber, E.; Grandinetti, A.; Verheus, M.; Kolonel, L.N.; Maskarinec, G. Dietary fiber, magnesium, and glycemic load alter risk of type 2 diabetes in a multiethnic cohort in Hawaii. J. Nutr. 2010, 140, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Meyer, K.A.; Kushi, L.H.; Jacobs, D.R., Jr.; Slavin, J.; Sellers, T.A.; Folsom, A.R. Carbohydrates, dietary fiber, and incident type 2 diabetes in older women. Am. J. Clin. Nutr. 2000, 71, 921–930. [Google Scholar] [CrossRef] [Green Version]
- Zheng, B.; Shen, H.; Han, H.; Han, T.; Qin, Y. Dietary fiber intake and reduced risk of ovarian cancer: A meta-analysis. Nutr. J. 2018, 17, 99. [Google Scholar] [CrossRef]
- Sivaprakasam, S.; Prasad, P.D.; Singh, N. Benefits of short-chain fatty acids and their receptors in inflammation and carcinogenesis. Pharmacol. Ther. 2016, 164, 144–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Dong, A.; Xie, K.; Yu, Y. Dietary Supplementation With High Fiber Alleviates Oxidative Stress and Inflammatory Responses Caused by Severe Sepsis in Mice Without Altering Microbiome Diversity. Front. Physiol. 2018, 9, 1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, M.S.; Seekatz, A.M.; Koropatkin, N.M.; Kamada, N.; Hickey, C.A.; Wolter, M.; Pudlo, N.A.; Kitamoto, S.; Terrapon, N.; Muller, A.; et al. A Dietary Fiber-Deprived Gut Microbiota Degrades the Colonic Mucus Barrier and Enhances Pathogen Susceptibility. Cell 2016, 167, 1339–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarrinpar, A.; Chaix, A.; Yooseph, S.; Panda, S. Diet and feeding pattern affect the diurnal dynamics of the gut microbiome. Cell Metab. 2014, 20, 1006–1017. [Google Scholar] [CrossRef] [Green Version]
- Tahara, Y.; Yamazaki, M.; Sukigara, H.; Motohashi, H.; Sasaki, H.; Miyakawa, H.; Haraguchi, A.; Ikeda, Y.; Fukuda, S.; Shibata, S. Gut Microbiota-Derived Short Chain Fatty Acids Induce Circadian Clock Entrainment in Mouse Peripheral Tissue. Sci. Rep. 2018, 8, 1395. [Google Scholar] [CrossRef]
- Choi, H.; Rao, M.C.; Chang, E.B. Gut microbiota as a transducer of dietary cues to regulate host circadian rhythms and metabolism. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 679–689. [Google Scholar] [CrossRef]
- Shan, Z.; Rehm, C.D.; Rogers, G.; Ruan, M.; Wang, D.D.; Hu, F.B.; Mozaffarian, D.; Zhang, F.F.; Bhupathiraju, S.N. Trends in Dietary Carbohydrate, Protein, and Fat Intake and Diet Quality Among US Adults, 1999–2016. JAMA 2019, 322, 1178–1187. [Google Scholar] [CrossRef] [Green Version]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef]
- Wang, D.D.; Leung, C.W.; Li, Y.; Ding, E.L.; Chiuve, S.E.; Hu, F.B.; Willett, W.C. Trends in dietary quality among adults in the United States, 1999 through 2010. JAMA Intern. Med. 2014, 174, 1587–1595. [Google Scholar] [CrossRef]
- Ibsen, D.B.; Laursen, A.S.D.; Wurtz, A.M.L.; Dahm, C.C.; Rimm, E.B.; Parner, E.T.; Overvad, K.; Jakobsen, M.U. Food substitution models for nutritional epidemiology. Am. J. Clin. Nutr. 2021, 113, 294–303. [Google Scholar] [CrossRef]
- Moslehi, N.; Ehsani, B.; Mirmiran, P.; Hojjat, P.; Azizi, F. Association of Dietary Proportions of Macronutrients with Visceral Adiposity Index: Non-Substitution and Iso-Energetic Substitution Models in a Prospective Study. Nutrients 2015, 7, 8859–8870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Brandt, P.A. Coffee or Tea? A prospective cohort study on the associations of coffee and tea intake with overall and cause-specific mortality in men versus women. Eur. J. Epidemiol. 2018, 33, 183–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaczmarczyk, M.M.; Miller, M.J.; Freund, G.G. The health benefits of dietary fiber: Beyond the usual suspects of type 2 diabetes mellitus, cardiovascular disease and colon cancer. Metabolism 2012, 61, 1058–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St-Onge, M.P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P.; Varady, K.; American Heart Association Obesity Committee of the Council on Lifestyle; Cardiometabolic Health; Council on Cardiovascular Disease in the Young; et al. Meal Timing and Frequency: Implications for Cardiovascular Disease Prevention: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [CrossRef] [PubMed]
- King, D.E.; Xiang, J. A Relationship Between Mortality and Eating Breakfast and Fiber. J. Am. Board Fam. Med. 2021, 34, 678–687. [Google Scholar] [CrossRef] [PubMed]
- Bishehsari, F.; Levi, F.; Turek, F.W.; Keshavarzian, A. Circadian Rhythms in Gastrointestinal Health and Diseases. Gastroenterology 2016, 151, e1–e5. [Google Scholar] [CrossRef] [Green Version]
- Goo, R.H.; Moore, J.G.; Greenberg, E.; Alazraki, N.P. Circadian variation in gastric emptying of meals in humans. Gastroenterology 1987, 93, 515–518. [Google Scholar] [CrossRef]
- Kim, H.K.; Nanba, T.; Ozaki, M.; Chijiki, H.; Takahashi, M.; Fukazawa, M.; Okubo, J.; Shibata, S. Effect of the Intake of a Snack Containing Dietary Fiber on Postprandial Glucose Levels. Foods 2020, 9, 1500. [Google Scholar] [CrossRef]
- Meng, H.; Matthan, N.R.; Ausman, L.M.; Lichtenstein, A.H. Effect of prior meal macronutrient composition on postprandial glycemic responses and glycemic index and glycemic load value determinations. Am. J. Clin. Nutr. 2017, 106, 1246–1256. [Google Scholar] [CrossRef] [Green Version]
- Diederichs, T.; Herder, C.; Rossbach, S.; Roden, M.; Wudy, S.A.; Nothlings, U.; Alexy, U.; Buyken, A.E. Carbohydrates from Sources with a Higher Glycemic Index during Adolescence: Is Evening Rather than Morning Intake Relevant for Risk Markers of Type 2 Diabetes in Young Adulthood? Nutrients 2017, 9, 591. [Google Scholar] [CrossRef] [Green Version]
- Suh, S.; Kim, K.W. Diabetes and Cancer: Cancer Should Be Screened in Routine Diabetes Assessment. Diabetes Metab. J. 2019, 43, 733–743. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.M.; Howitt, M.R.; Panikov, N.; Michaud, M.; Gallini, C.A.; Bohlooly, Y.M.; Glickman, J.N.; Garrett, W.S. The microbial metabolites, short-chain fatty acids, regulate colonic Treg cell homeostasis. Science 2013, 341, 569–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zmora, N.; Suez, J.; Elinav, E. You are what you eat: Diet, health and the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 35–56. [Google Scholar] [CrossRef]
- Qin, J.; Li, R.; Raes, J.; Arumugam, M.; Burgdorf, K.S.; Manichanh, C.; Nielsen, T.; Pons, N.; Levenez, F.; Yamada, T.; et al. A human gut microbial gene catalogue established by metagenomic sequencing. Nature 2010, 464, 59–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, A.C.; Hoffmann, C.; Mota, J.F. The human gut microbiota: Metabolism and perspective in obesity. Gut Microbes 2018, 9, 308–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stojanov, S.; Berlec, A.; Strukelj, B. The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease. Microorganisms 2020, 8, 1715. [Google Scholar] [CrossRef]
- Thaiss, C.A.; Zeevi, D.; Levy, M.; Zilberman-Schapira, G.; Suez, J.; Tengeler, A.C.; Abramson, L.; Katz, M.N.; Korem, T.; Zmora, N.; et al. Transkingdom control of microbiota diurnal oscillations promotes metabolic homeostasis. Cell 2014, 159, 514–529. [Google Scholar] [CrossRef] [Green Version]
- Liang, X.; Bushman, F.D.; FitzGerald, G.A. Rhythmicity of the intestinal microbiota is regulated by gender and the host circadian clock. Proc. Natl. Acad. Sci. USA 2015, 112, 10479–10484. [Google Scholar] [CrossRef] [Green Version]
- Turnbaugh, P.J.; Ridaura, V.K.; Faith, J.J.; Rey, F.E.; Knight, R.; Gordon, J.I. The effect of diet on the human gut microbiome: A metagenomic analysis in humanized gnotobiotic mice. Sci. Transl. Med. 2009, 1, 6ra14. [Google Scholar] [CrossRef] [Green Version]
- De Filippo, C.; Cavalieri, D.; Di Paola, M.; Ramazzotti, M.; Poullet, J.B.; Massart, S.; Collini, S.; Pieraccini, G.; Lionetti, P. Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proc. Natl. Acad. Sci. USA 2010, 107, 14691–14696. [Google Scholar] [CrossRef] [Green Version]
- Sandberg, J.C.; Bjorck, I.M.; Nilsson, A.C. Rye-Based Evening Meals Favorably Affected Glucose Regulation and Appetite Variables at the Following Breakfast; A Randomized Controlled Study in Healthy Subjects. PLoS ONE 2016, 11, e0151985. [Google Scholar] [CrossRef] [PubMed]
- Swann, O.G.; Kilpatrick, M.; Breslin, M.; Oddy, W.H. Dietary fiber and its associations with depression and inflammation. Nutr. Rev. 2020, 78, 394–411. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.J.; Chen, X.; Kwan, T.K.; Loh, Y.W.; Singer, J.; Liu, Y.; Ma, J.; Tan, J.; Macia, L.; Mackay, C.R.; et al. Dietary Fiber Protects against Diabetic Nephropathy through Short-Chain Fatty Acid-Mediated Activation of G Protein-Coupled Receptors GPR43 and GPR109A. J. Am. Soc. Nephrol. 2020, 31, 1267–1281. [Google Scholar] [CrossRef] [PubMed]
- Steffens, S.; Winter, C.; Schloss, M.J.; Hidalgo, A.; Weber, C.; Soehnlein, O. Circadian Control of Inflammatory Processes in Atherosclerosis and Its Complications. Arter. Thromb Vasc. Biol 2017, 37, 1022–1028. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | Quintile 1 (n = 6232) | Quintile 2 (n = 6233) | Quintile 3 (n = 6234) | Quintile 4 (n = 6232) | Quintile 5 (n = 6233) | p-Value |
|---|---|---|---|---|---|---|
| Age, years | 39.51 (16.97) | 45.25 (19.47) | 48.99 (19.43) | 51.29 (19.00) | 51.39 (18.10) | <0.001 |
| Female, % | 2506 (40.21) | 3477 (55.78) | 3604 (57.81) | 3511 (56.34) | 3051 (48.95) | <0.001 |
| Non-Hispanic White, % | 2807 (45.04) | 2832 (45.44) | 2986 (47.90) | 2920 (46.85) | 2691 (43.17) | <0.001 |
| BMI, kg/m2 | 28.95 (7.45) | 29.04 (7.12) | 28.97 (6.91) | 28.72 (6.45) | 28.12 (6.08) | <0.001 |
| College graduate or above, % | 652 (10.46) | 943 (15.13) | 1235 (19.81) | 1545 (24.79) | 1928 (30.93) | <0.001 |
| >USD 100,000 annual household income, % | 418 (6.71) | 544 (8.73) | 624 (10.01) | 729 (11.70) | 912 (14.63) | 0.002 |
| Exercise regularly, % | 1379 (22.13) | 1399 (22.45) | 1421 (22.79) | 1436 (23.04) | 1657 (26.58) | <0.001 |
| Current smoker, % | 2663 (42.73) | 1771 (28.41) | 1290 (20.69) | 928 (14.89) | 718 (11.52) | <0.001 |
| Current drinker, % | 4192 (67.27) | 3863 (61.98) | 3885 (62.32) | 3852 (61.81) | 3976 (63.79) | <0.001 |
| Dietary supplements use, % | 2020 (32.41) | 2693 (43.21) | 3143 (50.42) | 3467 (55.63) | 3665 (58.80) | <0.001 |
| Diabetes, % | 571 (9.28) | 865 (14.08) | 964 (15.72) | 1119 (18.20) | 1005 (16.40) | <0.001 |
| Hypertension, % | 2851 (45.76) | 3100 (49.75) | 3207 (51.44) | 3266 (52.42) | 3153 (50.59) | <0.001 |
| Dyslipidemia, % | 2008 (32.22) | 2316 (37.16) | 2565 (41.15) | 2696 (43.26) | 2751 (44.14) | <0.001 |
| Medicine use for lower blood sugar, % | 1321 (21.20) | 1448 (23.23) | 1615 (25.91) | 1676 (26.89) | 1506 (24.16) | <0.001 |
| Medicine use for hypertension, % | 1114 (17.88) | 1561 (25.04) | 1770 (28.39) | 1805 (28.96) | 1712 (27.47) | <0.001 |
| Medicine use for lower cholesterol, % | 874 (14.02) | 1263 (20.26) | 1585 (25.43) | 1694 (27.18) | 1651 (26.49) | <0.001 |
| Total energy, kcal/day | 2306.22 (826.46) | 1883.70 (740.46) | 1858.92 (718.60) | 1930.49 (706.57) | 2161.03 (737.03) | <0.001 |
| Total fat, % of energy | 33.92 (8.33) | 34.47 (7.28) | 33.53 (7.22) | 32.65 (7.14) | 30.92 (7.45) | <0.001 |
| Carbohydrate, % of energy | 46.76 (11.31) | 48.29 (9.32) | 49.71 (8.76) | 50.80 (8.48) | 53.59 (8.69) | <0.001 |
| Protein, % of energy | 15.13 (4.71) | 15.78 (4.39) | 16.12 (4.23 | 16.40 (4.19) | 16.36 (3.91) | <0.001 |
| Total dietary fiber, g/day | 9.18 (4.17) | 11.16 (4.22) | 13.99 (4.14) | 18.08 (4.23) | 28.12 (8.63) | <0.001 |
| AHEI | 51.82 (13.70) | 48.91 (13.90) | 50.42 (13.26) | 53.06 (12.81) | 56.84 (12.42) | <0.001 |
| Three meals a day, % | 2588 (42.25) | 3098 (50.41) | 3525 (56.95) | 3930 (63.45) | 4165 (67.10) | <0.001 |
| Only breakfast skipping, % | 916 (14.96) | 738 (12.01) | 572 (9.24) | 386 (6.23) | 283 (4.56) | <0.001 |
| Only lunch skipping, % | 1255 (20.49) | 1223 (19.90) | 1214 (19.61) | 1129 (18.23) | 1093 (17.61) | <0.001 |
| Only dinner skipping, % | 356 (5.81) | 389 (6.33) | 379 (6.12) | 379 (6.12) | 379 (6.12) | <0.001 |
| Only eat breakfast, % | 138 (2.25) | 121 (1.97) | 109 (1.76) | 81 (1.31) | 82 (1.32) | <0.001 |
| Only eat lunch, % | 230 (3.76) | 156 (2.54) | 102(1.65) | 83 (1.34) | 48 (0.77) | <0.001 |
| Only eat dinner, % | 642 (10.48) | 421 (6.85) | 289(4.67) | 206 (3.33) | 157 (2.53) | <0.001 |
| Variables | Total Dietary Fiber Intake per Meal | Residual Dietary Fiber Intake per Meal | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | p-Value | ||||||||
| n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | ||
| Fiber intake at breakfast, g/day | 25,881 | 3.88 (3.49) | 5131 | 2.40 (1.97) | 5136 | 1.98 (1.78) | 5127 | 2.53 (1.97) | 5133 | 4.12 (2.06) | 5131 | 8.40 (4.21) | <0.001 |
| Fiber intake at lunch, g/day | 22,714 | 5.13 (3.95) | 4541 | 3.60 (2.51) | 4539 | 3.07 (2.25) | 4541 | 3.65 (2.38) | 4540 | 5.25 (2.43 | 4541 | 10.08 (2.65) | <0.001 |
| Fiber intake at dinner, g/day | 28,072 | 6.36 (4.68) | 5567 | 4.17 (2.95) | 5567 | 3.824 (2.78) | 5568 | 4.87 (2.86) | 5567 | 6.82 (2.91) | 5567 | 12.18 (5.36) | <0.001 |
| Residual fiber intake at breakfast, g/day | 25,658 | 4.11 (2.65) | 5131 | 1.27 (1.09) | 5136 | 2.85 (0.26) | 5127 | 3.68 (0.25) | 5133 | 4.80 (0.41) | 5131 | 7.97 (2.92) | <0.001 |
| Residual fiber intake at lunch, g/day | 22,702 | 5.06 (2.84) | 4541 | 1.98 (1.20) | 4539 | 3.69 (0.28) | 4541 | 4.59 (0.27) | 4540 | 5.77 (0.45) | 4541 | 9.29 (2.93) | <0.001 |
| Residual fiber intake at dinner, g/day | 27,836 | 6.53 (3.39) | 5567 | 2.80 (1.52) | 5567 | 4.85 (0.33) | 5568 | 5.98 (0.35) | 5567 | 7.47 (0.56) | 5567 | 11.53 (3.43) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, J.; Gao, J.; Zhang, Y.; Hou, W.; Han, T.; Sun, C. The Association of Dietary Fiber Intake in Three Meals with All-Cause and Disease-Specific Mortality among Adults: The U.S. National Health and Nutrition Examination Survey, 2003–2014. Nutrients 2022, 14, 2521. https://doi.org/10.3390/nu14122521
Qi J, Gao J, Zhang Y, Hou W, Han T, Sun C. The Association of Dietary Fiber Intake in Three Meals with All-Cause and Disease-Specific Mortality among Adults: The U.S. National Health and Nutrition Examination Survey, 2003–2014. Nutrients. 2022; 14(12):2521. https://doi.org/10.3390/nu14122521
Chicago/Turabian StyleQi, Jiayue, Jian Gao, Yuntao Zhang, Wanying Hou, Tianshu Han, and Changhao Sun. 2022. "The Association of Dietary Fiber Intake in Three Meals with All-Cause and Disease-Specific Mortality among Adults: The U.S. National Health and Nutrition Examination Survey, 2003–2014" Nutrients 14, no. 12: 2521. https://doi.org/10.3390/nu14122521
APA StyleQi, J., Gao, J., Zhang, Y., Hou, W., Han, T., & Sun, C. (2022). The Association of Dietary Fiber Intake in Three Meals with All-Cause and Disease-Specific Mortality among Adults: The U.S. National Health and Nutrition Examination Survey, 2003–2014. Nutrients, 14(12), 2521. https://doi.org/10.3390/nu14122521