
Attention Should Be Paid to Adolescent Girl Anemia in China: Based on China Nutrition and Health Surveillance (2015–2017)



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Survey Method
2.3. Anemia Definition
2.4. Influencing Factor Variables
2.5. Statistical Analysis Method
2.6. Mapping Method
2.7. Ethical Approval
3. Results
3.1. Adolescent Girl Hemoglobin and Anemia Status
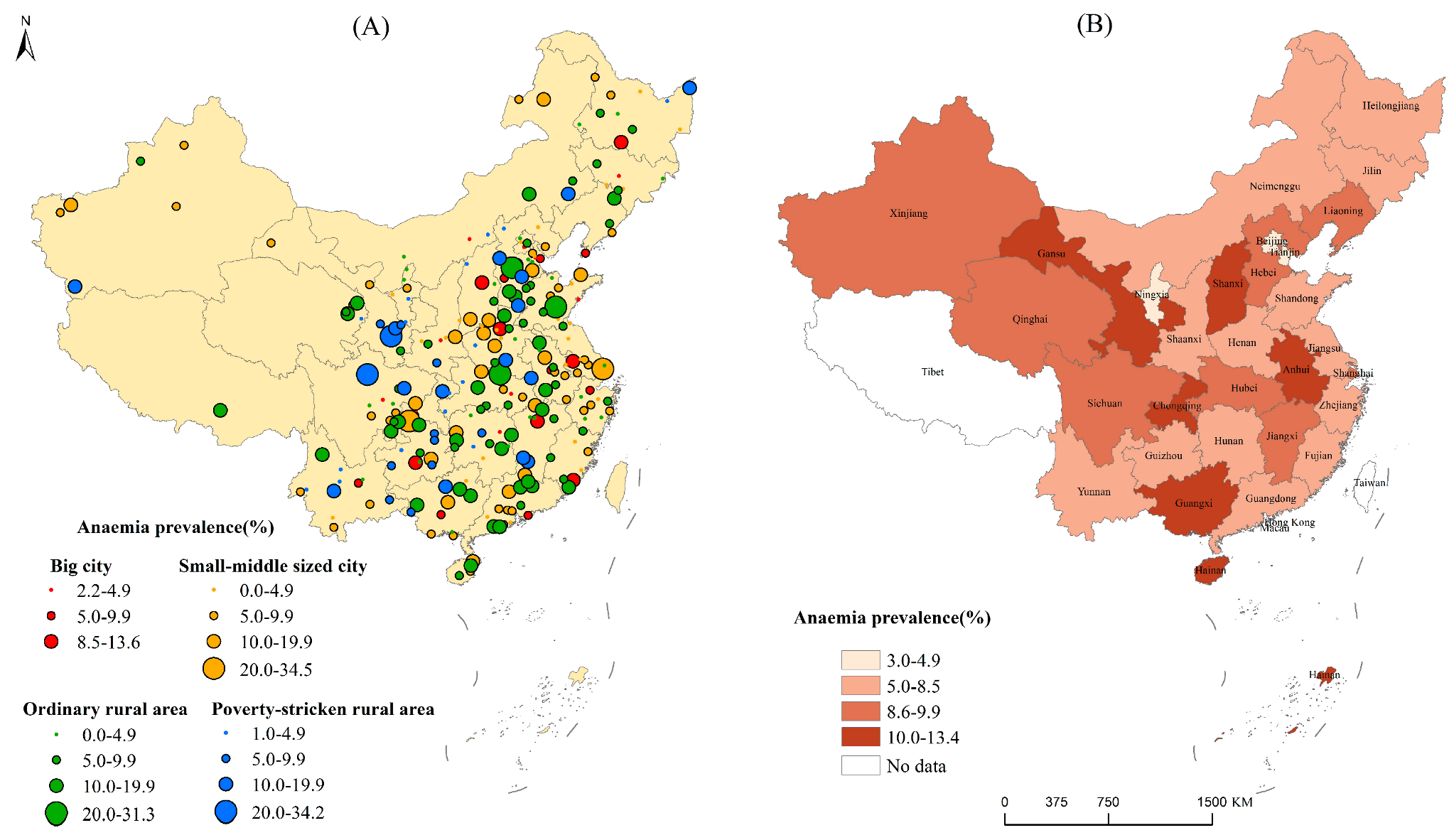
3.2. Regional Disparities of Adolescent Girl Anemia
3.3. Influencing Factors of Anemia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Characteristic | All | Urban | Rural | ||||||
|---|---|---|---|---|---|---|---|---|---|
| % | Anemia% | OR (95%CI) | % | Anemia% | OR (95%CI) | % | Anemia% | OR (95%CI) | |
| Having started menstruating | |||||||||
| Yes | 61.4 | 10.3 | 2.46 (2.18–2.77) ** | 64.2 | 9.0 | 2.08 (1.74–2.50) ** | 58.9 | 11.6 | 2.83 (2.41–3.31) ** |
| No | 38.6 | 4.5 | 1.00 (ref) | 35.8 | 4.5 | 1.00 (ref) | 41.1 | 4.4 | 1.00 (ref) |
| Nutrition status | |||||||||
| Underweight | 6.1 | 7.5 | 0.92 (0.74–1.13) | 5.2 | 6.8 | 0.92 (0.65–1.29) | 6.8 | 8.0 | 0.90 (0.69–1.17) |
| Normal | 80.2 | 8.2 | 1.00 (ref) | 78.6 | 7.4 | 1.00 (ref) | 81.6 | 8.9 | 1.00 (ref) |
| Overweight | 9.4 | 8.3 | 1.02 (0.86–1.20) | 10.9 | 8.1 | 1.11 (0.88–1.40) | 8.1 | 8.6 | 0.97 (0.76–1.23) |
| Obesity | 4.3 | 5.6 | 0.66 (0.50–0.88) ** | 5.2 | 6.1 | 0.82 (0.57–1.17) | 3.5 | 4.9 | 0.52 (0.33–0.83) ** |
| Father’s education level | |||||||||
| Low | 70.6 | 8.3 | 1.00 (ref) | 54.6 | 7.6 | 1.00 (ref) | 84.8 | 8.6 | 1.00 (ref) |
| High | 29.4 | 7.2 | 0.87 (0.78–0.97) * | 45.4 | 6.8 | 0.88 (0.76–1.02) | 15.2 | 8.5 | 0.98 (0.82–1.17) |
| Mother’s educational level | |||||||||
| Low | 74.5 | 8.3 | 1.00 (ref) | 59.0 | 7.6 | 1.00 (ref) | 88.4 | 8.7 | 1.00 (ref) |
| High | 25.5 | 6.9 | 0.82 (0.73–0.92) ** | 41.0 | 6.7 | 0.87 (0.75–1.02) | 11.6 | 7.7 | 0.87 (0.70–1.07) |
| Primary caregiver | |||||||||
| Mother and father | 81.9 | 7.9 | 1.00 (ref) | 88.2 | 7.2 | 1.00 (ref) | 76.2 | 8.6 | 1.00 (ref) |
| Grand parents | 15.6 | 8.1 | 1.03 (0.91–1.18) | 9.8 | 7.6 | 1.07 (0.84–1.37) | 20.8 | 8.3 | 0.96 (0.82–1.13) |
| Other relatives | 2.5 | 11.7 | 1.56 (1.20–2.02) ** | 1.9 | 10.2 | 1.48 (0.94–2.35) | 3.0 | 12.5 | 1.53 (1.11–2.11) ** |
| Father out-migrating | |||||||||
| Yes | 28.1 | 9.1 | 1.22 (1.10–1.36) ** | 15.9 | 8.4 | 1.22 (1.01–1.47) * | 38.9 | 9.3 | 1.15 (1.01–1.31) * |
| No | 70.5 | 7.6 | 1.00 (ref) | 82.4 | 7.0 | 1.00 (ref) | 59.9 | 8.2 | 1.00 (ref) |
| Not clear | 1.5 | 8.1 | 1.07 (0.72–1.60) | 1.7 | 8.7 | 1.27 (0.76–2.14) | 1.3 | 7.2 | 0.87 (0.47–1.62) |
| Mother out-migrating | |||||||||
| Yes | 14.6 | 9.1 | 1.19 (1.04–1.36) ** | 6.4 | 8.3 | 1.18 (0.90–1.56) | 21.8 | 9.3 | 1.12 (0.96–1.30) |
| No | 84.2 | 7.8 | 1.00 (ref) | 92.3 | 7.2 | 1.00 (ref) | 76.9 | 8.4 | 1.00 (ref) |
| Not clear | 1.3 | 9.4 | 1.24 (0.83–1.85) | 1.2 | 9.9 | 1.42 (0.80–2.53) | 1.3 | 9.1 | 1.09 (0.63–1.90) |
| Regions | |||||||||
| East | 33.8 | 7.5 | 1.00 (ref) | 43.0 | 6.6 | 1.00 (ref) | 25.7 | 9.0 | 1.00 (ref) |
| Middle | 30.1 | 8.2 | 1.10 (0.97–1.24) | 25.0 | 8.1 | 1.26 (1.05–1.52) * | 34.6 | 8.2 | 0.91 (0.77–1.08) |
| West | 36.1 | 8.2 | 1.10 (0.98–1.24) | 32.0 | 7.5 | 1.16 (0.97-1.37) | 39.6 | 8.8 | 0.98 (0.83–1.15) |
| Food intake | |||||||||
| Meat intake times | |||||||||
| <2 times/d | 94.2 | 8.0 | 1.00 (ref) | 93.2 | 7.2 | 1.00 (ref) | 95.1 | 8.7 | 1.00 (ref) |
| ≥2 times/d | 5.8 | 7.2 | 0.90 (0.72–1.12) | 6.8 | 6.8 | 0.94 (0.69–1.27) | 4.9 | 7.8 | 0.89 (0.65–1.22) |
| Meat intake weight | |||||||||
| <35 g/d | 53.2 | 8.1 | 1.00 (ref) | 44.6 | 7.7 | 1.00 (ref) | 60.8 | 8.4 | 1.00 (ref) |
| ≥35 g/d | 46.8 | 7.8 | 0.95 (0.86–1.05) | 55.4 | 6.8 | 0.87 (0.75–1.01) | 39.2 | 9.0 | 1.07 (0.94–1.22) |
| Vegetable intake times | |||||||||
| <3 times/d | 92.0 | 8.1 | 1.00 (ref) | 92.4 | 7.3 | 1.00 (ref) | 91.7 | 8.8 | 1.00 (ref) |
| ≥3 times/d | 8.0 | 6.4 | 0.78 (0.64–0.94) * | 7.6 | 6.0 | 0.80 (0.59–1.09) | 8.3 | 6.7 | 0.75 (0.58–0.97) * |
| Vegetable intake weight | |||||||||
| <400 g/d | 85.9 | 7.8 | 1.00 (ref) | 82.3 | 7.0 | 1.00 (ref) | 89.2 | 8.4 | 1.00 (ref) |
| ≥400 g/d | 14.1 | 9.1 | 1.19 (1.04–1.36) * | 17.7 | 8.1 | 1.17 (0.97–1.42) | 10.8 | 10.6 | 1.29 (1.06–1.56) * |
References
- Kassebaum, N.J. The Global Burden of Anemia. Hematol. Oncol. Clin. N. Am. 2016, 30, 247–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: A systematic analysis of population-representative data. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar] [CrossRef] [Green Version]
- Balarajan, Y.; Ramakrishnan, U.; Ozaltin, E.; Shankar, A.H.; Subramanian, S.V. Anaemia in low-income and middle-income countries. Lancet 2011, 378, 2123–2135. [Google Scholar] [CrossRef]
- Haas, J.D.; Brownlie, T., IV. Iron Deficiency and Reduced Work Capacity: A Critical Review of the Research to Determine a Causal Relationship. J. Nutr. 2001, 131, 676S–688S. [Google Scholar] [CrossRef] [Green Version]
- Second International Conference on Nutrition. Conference Outcome Document: Framework for Action. Available online: https://www.fao.org/3/mm215e/mm215e.pdf (accessed on 5 June 2022).
- Bureau of Disease Control and Prevention; National Health and Family Planning Commission of the People’s Republic of China. Report on Chinese Residents’ Chronic Diseases and Nutrition (2015); People’s Medical Publishing House: Beijing, China, 2016; p. 25.
- Bureau of Disease Control and Prevention; National Health Commission of the People’s Republic of China. Report on Chinese Residents' Chronic Diseases and Nutrition (2020); People’s Medical Publishing House: Beijing, China, 2021; p. 39.
- Liu, F.; Zhang, X.; Wu, J. Analysis of correlation between prevalence rate of anemia among Chinese children and adolescents and physical factors. Chin. J. Sch. Health 2017, 38, 3. [Google Scholar]
- Wang, J.Y.; Hu, P.J.; Luo, D.M.; Dong, B.; Ma, Y.; Dai, J.; Song, Y.; Ma, J.; Lau, P.W.C. Reducing Anemia Among School-Aged Children in China by Eliminating the Geographic Disparity and Ameliorating Stunting: Evidence from a National Survey. Front. Pediatr. 2020, 8, 193. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Jasrasaria, R.; Naghavi, M.; Wulf, S.K.; Murray, C.J.L. A systematic analysis of global anemia burden from 1990 to 2010. Blood 2013, 123, 615. [Google Scholar] [CrossRef]
- Ji, Y. Modern Children and Adolescent Health; People’s Medical Publishing House: Beijing, China, 2010. [Google Scholar]
- Zou, Y.; Zhang, R.H.; Xia, S.C.; Huang, L.C.; Fang, Y.Q.; Meng, J.; Chen, J.; Zhang, H.X.; Zhou, B.; Ding, G.Q. The Rural-Urban Difference in BMI and Anemia among Children and Adolescents. Int. J. Environ. Res. Public Health 2016, 13, 1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.X.; Chen, J.; Liu, X.H. Profiles of anemia among school-aged children categorized by body mass index and waist circumference in Shandong, China. Pediatr. Neonatol. 2021, 62, 165–171. [Google Scholar] [CrossRef]
- Yang, Z.; Li, Y.; Hu, P.; Ma, J.; Song, Y. Prevalence of Anemia and its Associated Factors among Chinese 9-, 12-, and 14-Year-Old Children: Results from 2014 Chinese National Survey on Students Constitution and Health. Int. J. Environ. Res. Public Health 2020, 17, 1474. [Google Scholar] [CrossRef] [Green Version]
- Gao, C.; Hu, X.; Zhang, Q.; Xu, P.; Li, L.; Yang, T.; Cao, W.; Gan, Q.; Pan, H.; Xu, J. Anemia status and related factors among left-behind children in poverty-sticken rural areas in China, 2016. Chin. J. Epidemiol. 2019, 40, 6. [Google Scholar]
- Wu, J.; Hu, Y.; Li, M.; Chen, J.; Mao, D.; Li, W.; Wang, R.; Yang, Y.; Piao, J.; Yang, L.; et al. Prevalence of Anemia in Chinese Children and Adolescents and Its Associated Factors. Int. J. Environ. Res. Public Health 2019, 16, 1416. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Zhao, L.; Zhang, J.; Yang, Z.; Yang, L.; Huang, J.; Fang, H.; Guo, Q.; Xu, X.; Ju, L.; et al. China Nutrition and Health Surveys (1982–2017). China CDC Wkly. 2021, 3, 3. [Google Scholar] [CrossRef] [PubMed]
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information System; WHO/NMH/NHD/MNM/11.1; World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/bitstream/handle/10665/85839/WHO_NMH_NHD_MNM_11.1_eng.pdf?sequence=22&isAllowed=y (accessed on 5 June 2022).
- Society, C.N. Dietary Guidelines for School-Aged Children in China (2022); People’s Medical Publishing House Co., Ltd.: Beijing, China, 2022; pp. 74–77. [Google Scholar]
- De Andrade Cairo, R.C.; Rodrigues Silva, L.; Carneiro Bustani, N.; Ferreira Marques, C.D. Iron deficiency anemia in adolescents; a literature review. Nutr. Hosp. 2014, 29, 1240–1249. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Shin, S.; Han, K.; Lee, K.C.; Kim, J.H.; Choi, Y.S.; Kim, D.H.; Nam, G.E.; Yeo, H.D.; Lee, H.G.; et al. Relationship between socioeconomic status and anemia prevalence in adolescent girls based on the fourth and fifth Korea National Health and Nutrition Examination Surveys. Eur. J. Clin. Nutr. 2014, 68, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Syed, S.; Addo, O.Y.; De la Cruz-Gongora, V.; Ashour, F.A.; Ziegler, T.R.; Suchdev, P.S. Determinants of Anemia among School-Aged Children in Mexico, the United States and Colombia. Nutrients 2016, 8, 387. [Google Scholar] [CrossRef]
- Luo, D.; Xu, R.; Ma, J.; Yan, X.; Hu, P.; Song, Y.; Jan, C.; Raat, H.; Patton, G.C. The associations of economic growth and anaemia for school-aged children in China. Matern. Child Nutr. 2020, 16, e12936. [Google Scholar] [CrossRef]
- Luo, D.; Yan, X.; Hu, P.; Zhang, J.; Lei, Y.; Song, Y.; Ma, J. Subnational disparity of anemia among Chinese Han students aged 7–14 years in 2014. Chin. J. Sch. Health 2019, 40, 6. [Google Scholar]
- Hehua, R.; Mao, H.; Wang, H.; Cao, M. Research Progress on Influencing Factors of menarche age. Matern. Child Health Care China 2018, 33, 3. [Google Scholar]
- WHO. Guideline: Intermittent Iron and Folic Acid Supplementation in Menstruating Women; World Health Organization: Geneva, Switzerland, 2011; Available online: https://www.who.int/publications/i/item/9789241502023 (accessed on 5 June 2022).
- Gayawan, E.; Arogundade, E.D.; Adebayo, S.B. Possible determinants and spatial patterns of anaemia among young children in Nigeria: A Bayesian semi-parametric modelling. Int. Health 2014, 6, 35–45. [Google Scholar] [CrossRef]
- Luo, R.; Zhang, L.; Liu, C.; Zhao, Q.; Shi, Y.; Miller, G.; Yu, E.; Sharbono, B.; Medina, A.; Rozelle, S. Anaemia among students of rural China’s elementary schools: Prevalence and correlates in Ningxia and Qinghai’s poor counties. J. Health Popul. Nutr. 2011, 29, 471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, M.B.; Hurrell, R.F. Nutritional iron deficiency. Lancet 2007, 370, 511–520. [Google Scholar] [CrossRef]
- Bentley, M.E.; Griffiths, P.L. The burden of anemia among women in India. Eur. J. Clin. Nutr. 2003, 57, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinhas-Hamiel, O.; Newfield, R.S.; Koren, I.; Agmon, A.; Lilos, P.; Phillip, M. Greater prevalence of iron deficiency in overweight and obese children and adolescent. Int. J. Obes. 2003, 27, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Zhang, X.; Shen, Y.; Fang, X.; Wang, Y.; Wang, F. Obesity and iron deficiency: A quantitative meta-analysis. Obes. Rev. 2015, 16, 1081–1093. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, C. A review of iron studies in overweight and obese children and adolescents: A double burden in the young? Eur. J. Nutr. 2016, 55, 2179–2197. [Google Scholar] [CrossRef]
- Yu, Q.; Melse-Boonstra, A.; Pan, X.; Yuan, B.; Dai, Y.; Zhao, J.; Zimmermann, M.B.; Kok, F.J.; Zhou, M.; Shi, Z. Anemia in relation to body mass index and waist circumference among chinese women. Nutr. J. 2013, 12, 10. [Google Scholar]
- Li, S.; Mengyao, L.; Xiaolu, L.; Mengting, Q.; Ziyan, H. Prevalence of iron deficiency anemia and the association with dietary nutrition fact of preschool children in rural Anhui Province. Chin. J. Sch. Health 2021, 42, 1793–1797. [Google Scholar] [CrossRef]

| Characteristic | N | Hb(g/L) | Anemia% | |||||
|---|---|---|---|---|---|---|---|---|
| All (95%CI) | Mild | Moderate | Severe | Urban | Rural | |||
| Total | 22,810 | 134.68 ± 12.13 | 8.5 (7.4–9.7) | 5.6 | 2.7 | 0.2 | 7.6 ** | 9.4 ** |
| Child’s age (in year) | ||||||||
| 10 | 3533 | 134.46 ± 10.65 | 4.0 (1.3–6.7) | 2.1 | 1.8 | 0.1 | 5.5 | 3.0 |
| 11 | 3564 | 136.02 ± 10.46 | 2.8 (1.3–4.3) | 1.6 | 1.2 | 0.0 | 2.9 | 2.8 |
| 12 | 3646 | 136.08 ± 11.28 | 6.0 (4.4–7.7) | 4.8 | 1.1 | 0.2 | 4.5 | 7.4 |
| 13 | 3234 | 134.86 ± 12.32 | 10.3 (7.8–12.7) | 7.1 | 3.1 | 0.1 | 8.5 | 11.8 |
| 14 | 1830 | 134.73 ± 13.02 | 9.7 (7.3–12.1) | 7.0 | 2.4 | 0.3 | 10.9 | 8.9 |
| 15 | 2426 | 132.92 ± 12.95 | 11.6 (9.3–13.8) | 7.2 | 4.2 | 0.2 | 9.4 ** | 13.9 ** |
| 16 | 3205 | 133.42 ± 13.71 | 11.5 (9.4–13.7) | 7.8 | 3.4 | 0.4 | 9.2 | 14.5 |
| 17 | 1372 | 133.57 ± 13.92 | 12.7 (9.9–15.4) | 8.1 | 4.5 | 0.1 | 10.3 ** | 15.2 ** |
| Model | Influencing Factors | Reference | OR(95%CI) | p |
|---|---|---|---|---|
| All girls | Urban/Rural | |||
| Rural | Urban | 1.18 (1.05–1.31) | 0.04 | |
| Having started menstruating | ||||
| Yes | No | 2.58 (2.28–2.92) | <0.01 | |
| Mother’s educational level | ||||
| High | Low | 0.87 (0.76–0.99) | 0.03 | |
| Meat intake weight | ||||
| ≥35 g/d | <35 g/d | 0.90 (0.81–1.00) | 0.04 | |
| Vegetable intake weight | ||||
| ≥400 g/d | <400 g/d | 1.24 (1.07–1.43) | <0.01 | |
| Vegetable intake frequency | ||||
| ≥3 times/d | <3 times/d | 0.72 (0.58–0.89) | <0.01 | |
| Urban girls | Having started menstruating | |||
| Yes | No | 2.28 (1.89–2.76) | <0.01 | |
| Distribution | ||||
| Middle | East | 1.34 (1.11–1.62) | <0.01 | |
| West | East | 1.17 (0.97–1.41) | 0.11 | |
| Meat intake weight | ||||
| ≥35 g/d | <35 g/d | 0.85 (0.73–1.00) | 0.04 | |
| Rural girls | Having started menstruating | |||
| Yes | No | 2.85 (2.42–3.36) | <0.01 | |
| Nutrition status | ||||
| Underweight | Normal | 1.15 (0.86–1.52) | 0.34 | |
| Overweight | Normal | 0.84 (0.65–1.08) | 0.16 | |
| Obesity | Normal | 0.58 (0.36–0.92) | 0.02 | |
| Vegetable intake weight | ||||
| ≥400 g/d | <400 g/d | 1.28 (1.04–1.57) | 0.02 | |
| Vegetable intake frequency | ||||
| ≥3 times/d | <3 times/d | 0.70 (0.53–0.92) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.; Zhao, L.; Yu, D.; Ren, H. Attention Should Be Paid to Adolescent Girl Anemia in China: Based on China Nutrition and Health Surveillance (2015–2017). Nutrients 2022, 14, 2449. https://doi.org/10.3390/nu14122449
Li S, Zhao L, Yu D, Ren H. Attention Should Be Paid to Adolescent Girl Anemia in China: Based on China Nutrition and Health Surveillance (2015–2017). Nutrients. 2022; 14(12):2449. https://doi.org/10.3390/nu14122449
Chicago/Turabian StyleLi, Shujuan, Liyun Zhao, Dongmei Yu, and Hongyan Ren. 2022. "Attention Should Be Paid to Adolescent Girl Anemia in China: Based on China Nutrition and Health Surveillance (2015–2017)" Nutrients 14, no. 12: 2449. https://doi.org/10.3390/nu14122449
APA StyleLi, S., Zhao, L., Yu, D., & Ren, H. (2022). Attention Should Be Paid to Adolescent Girl Anemia in China: Based on China Nutrition and Health Surveillance (2015–2017). Nutrients, 14(12), 2449. https://doi.org/10.3390/nu14122449