
The Efficacy of Ginseng (Panax) on Human Prediabetes and Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis

 ,
,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection and Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis and Meta-Analysis
3. Results
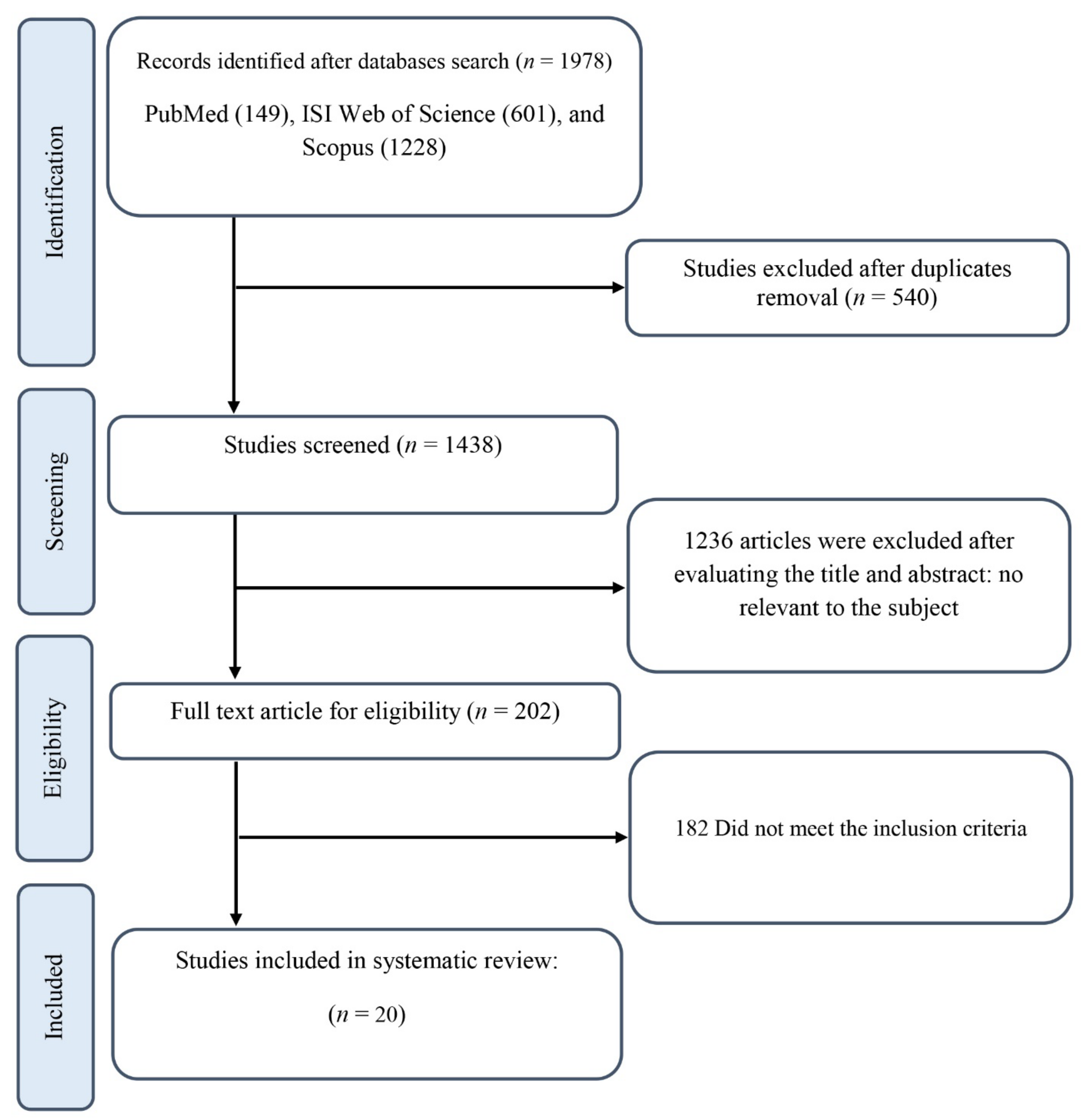
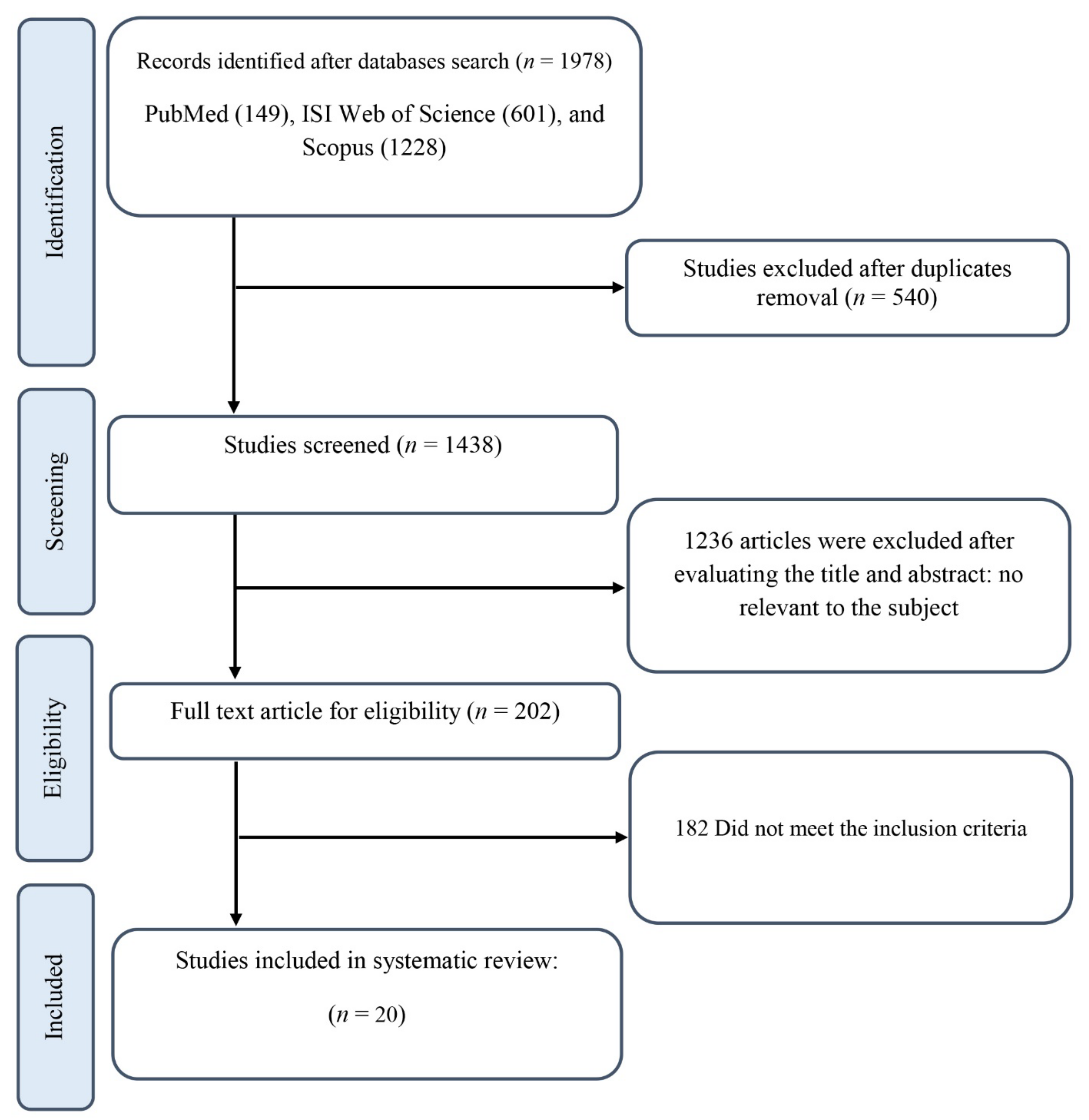
3.1. Study Selection
3.2. Study Characteristics
3.3. Effects of Ginseng Supplementation on Cardiometabolic Parameters
3.3.1. Anthropometric Measurements
3.3.2. Measures of Glucose Homeostasis
Glycemic Control
Insulin Resistance and Secretion
3.3.3. Cardiovascular Risk Factors
Lipid Profile
Blood Pressure and Heart Rate
3.3.4. Inflammatory Markers and Adipocytokines
3.3.5. Liver Function Tests
3.4. Sensitivity Analysis
3.5. Publication Bias
3.6. Non-Linear Dose-Response between Dose and Duration of Ginseng Supplementation on Cardiometabolic Indicators
3.7. Meta-Regression Analysis
3.8. GRADE Assessment
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bessell, E.; Fuller, N.R.; Markovic, T.P.; Lau, N.S.; Burk, J.; Hendy, C.; Picone, T.; Li, A.; Caterson, I.D. Effects of α-cyclodextrin on cholesterol control and hydrolyzed ginseng extract on glycemic control in people with prediabetes: A randomized clinical trial. JAMA Netw. Open 2020, 3, e2023491. [Google Scholar] [CrossRef] [PubMed]
- Woldeamlak, B.; Yirdaw, K.; Biadgo, B. Role of gut microbiota in type 2 diabetes mellitus and its complications: Novel insights and potential intervention strategies. Korean J. Gastroenterol. 2019, 74, 314–320. [Google Scholar] [CrossRef]
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of cardiovascular disease in type 2 diabetes: A systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc. Diabetol. 2018, 17, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- RISE Consortium. Metabolic contrasts between youth and adults with impaired glucose tolerance or recently diagnosed type 2 diabetes: II. Observations using the oral glucose tolerance test. Diabetes Care 2018, 41, 1707–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuksan, V.; Xu, Z.Z.; Jovanovski, E.; Jenkins, A.L.; Beljan-Zdravkovic, U.; Sievenpiper, J.L.; Mark Stavro, P.; Zurbau, A.; Duvnjak, L.; Li, M.Z. Efficacy and safety of American ginseng (Panax quinquefolius L.) extract on glycemic control and cardiovascular risk factors in individuals with type 2 diabetes: A double-blind, randomized, cross-over clinical trial. Eur. J. Nutr. 2019, 58, 1237–1245. [Google Scholar] [CrossRef]
- Shishtar, E.; Sievenpiper, J.L.; Djedovic, V.; Cozma, A.I.; Ha, V.; Jayalath, V.H.; Jenkins, D.J.; Meija, S.B.; de Souza, R.J.; Jovanovski, E. The effect of ginseng (the genus Panax) on glycemic control: A systematic review and meta-analysis of randomized controlled clinical trials. PLoS ONE 2014, 9, e107391. [Google Scholar] [CrossRef] [Green Version]
- Tackett, K.L.; Jones, M.C. Complementary and alternative medicines for the treatment of diabetes. J. Pharm. Pract. 2009, 22, 546–552. [Google Scholar] [CrossRef]
- Manya, K.; Champion, B.; Dunning, T. The use of complementary and alternative medicine among people living with diabetes in Sydney. BMC Complement. Altern. Med. 2012, 12, 2. [Google Scholar] [CrossRef] [Green Version]
- Rao, M.U.; Sreenivasulu, M.; Chengaiah, B.; Reddy, K.J.; Chetty, C.M. Herbal medicines for diabetes mellitus: A review. Int J PharmTech Res 2010, 2, 1883–1892. [Google Scholar]
- Xie, J.-T.; Mehendale, S.; Yuan, C.-S. Ginseng and diabetes. Am. J. Chin. Med. 2005, 33, 397–404. [Google Scholar] [CrossRef] [Green Version]
- Yuan, H.-D.; Kim, J.T.; Kim, S.H.; Chung, S.H. Ginseng and diabetes: The evidences from in vitro, animal and human studies. J. Ginseng Res. 2012, 36, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuksan, V.; Sung, M.-K.; Sievenpiper, J.L.; Stavro, P.M.; Jenkins, A.L.; Di Buono, M.; Lee, K.-S.; Leiter, L.A.; Nam, K.Y.; Arnason, J.T. Korean red ginseng (Panax ginseng) improves glucose and insulin regulation in well-controlled, type 2 diabetes: Results of a randomized, double-blind, placebo-controlled study of efficacy and safety. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Shin, B.-C.; Lee, M.S.; Lee, H.; Ernst, E. Red ginseng for type 2 diabetes mellitus: A systematic review of randomized controlled trials. Chin. J. Integr. Med. 2011, 17, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Sievenpiper, J.L.; Arnason, J.T.; Vidgen, E.; Leiter, L.A.; Vuksan, V. a systematic quantitative analysis of the literature of the high variability in ginseng (Panax spp.) should ginseng be trusted in diabetes? Diabetes Care 2004, 27, 839–840. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Yi, Y.S.; Kim, M.Y.; Cho, J.Y. Role of ginsenosides, the main active components of Panax ginseng, in inflammatory responses and diseases. J. Ginseng Res. 2017, 41, 435–443. [Google Scholar] [CrossRef] [Green Version]
- Parlakpınar, H.; Özhan, O.; Ermiş, N.; Acet, A. Cardiovascular effects of Panax ginseng. J. Turgut Ozal Med. Cent. 2016, 23, 482–487. [Google Scholar] [CrossRef]
- Baek, K.S.; Yi, Y.S.; Son, Y.J.; Yoo, S.; Sung, N.Y.; Kim, Y.; Hong, S.; Aravinthan, A.; Kim, J.H.; Cho, J.Y. In vitro and in vivo anti-inflammatory activities of Korean Red Ginseng-derived components. J. Ginseng Res. 2016, 40, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Hong, M.; Lee, Y.H.; Kim, S.; Suk, K.T.; Bang, C.S.; Yoon, J.H.; Baik, G.H.; Kim, D.J.; Kim, M.J. Anti-inflammatory and antifatigue effect of Korean Red Ginseng in patients with nonalcoholic fatty liver disease. J. Ginseng Res. 2016, 40, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Miraghajani, M.; Hadi, A.; Hajishafiee, M.; Arab, A.; Ghaedi, E.; Moodi, V. The effects of ginseng supplementation on anthropometric indices and body composition: A systematic review and meta-analysis. J. Herb. Med. 2020, 23, 100379. [Google Scholar] [CrossRef]
- Yoon, M.; Lee, H.; Jeong, S.; Kim, J.J.; Nicol, C.J.; Nam, K.W.; Kim, M.; Cho, B.G.; Oh, G.T. Peroxisome proliferator-activated receptor alpha is involved in the regulation of lipid metabolism by ginseng. Br. J. Pharmacol. 2003, 138, 1295–1302. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, S.A.; Alipour, M.; Ghadiry, A.; Zakerkish, M. The effects of standardized extract of ginseng (G115) on blood sugar control and inflammatory factors in patients with type 2 diabetes: A double-blind clinical trial. Int. J. Pharm. Res. Allied Sci. 2016, 5, 55–59. [Google Scholar]
- Jovanovski, E.; Smircic-Duvnjak, L.; Komishon, A.; Au-Yeung, F.R.; Sievenpiper, J.L.; Zurbau, A.; Jenkins, A.L.; Sung, M.K.; Josse, R.; Li, D.; et al. Effect of coadministration of enriched Korean Red Ginseng (Panax ginseng) and American ginseng (Panax quinquefolius L.) on cardiometabolic outcomes in type-2 diabetes: A randomized controlled trial. J. Ginseng Res. 2021, 45, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Mucalo, I.; Jovanovski, E.; Vuksan, V.; Božikov, V.; Romić, Z.; Rahelić, D. American ginseng extract (Panax quinquefolius L.) is safe in long-term use in type 2 diabetic patients. Evid.-Based Complement. Altern. Med. Ecam 2014, 2014, 969168. [Google Scholar] [CrossRef] [Green Version]
- Park, K.; Ahn, C.W.; Kim, Y.; Nam, J.S. The effect of Korean Red Ginseng on sarcopenia biomarkers in type 2 diabetes patients. Arch. Gerontol. Geriatr. 2020, 90, 104108. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Kim, Y.; Kim, J.; Kang, S.; Park, J.S.; Ahn, C.W.; Nam, J.S. Supplementation with Korean red ginseng improves current perception threshold in Korean type 2 diabetes patients: A randomized, double-blind, placebo-controlled trial. J. Diabetes Res. 2020, 2020, 5295328. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.S.; Kim, S.; Kim, M.J.; Kim, M.S.; Kim, J.; Park, C.W.; Seo, D.; Shin, S.S.; Oh, S.W. Efficacy and safety of Panax ginseng berry extract on glycemic control: A 12-wk randomized, double-blind, and placebo-controlled clinical trial. J. Ginseng Res. 2018, 42, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Oh, M.R.; Park, S.H.; Kim, S.Y.; Back, H.I.; Kim, M.G.; Jeon, J.Y.; Ha, K.C.; Na, W.T.; Cha, Y.S.; Park, B.H.; et al. Postprandial glucose-lowering effects of fermented red ginseng in subjects with impaired fasting glucose or type 2 diabetes: A randomized, double-blind, placebo-controlled clinical trial. BMC Complement. Altern. Med. 2014, 14, 237. [Google Scholar] [CrossRef] [Green Version]
- Mucalo, I.; Jovanovski, E.; Rahelić, D.; Božikov, V.; Romić, Z.; Vuksan, V. Effect of American ginseng (Panax quinquefolius L.) on arterial stiffness in subjects with type-2 diabetes and concomitant hypertension. J. Ethnopharmacol. 2013, 150, 148–153. [Google Scholar] [CrossRef]
- Hosseini, S.A.; Ghaedi, E.; Zakerkish, M.; Ghadiri, A.; Ashtary-larky, D.; Safari, M.; Parsanahad, M.; Alipour, M. Effects of ginseng extract on chemerin, apelin and glycemic biomarkers in type 2 diabetic patients. Indian J. Physiol. Pharm. 2017, 61, 152–158. [Google Scholar]
- Yoon, J.W.; Kang, S.M.; Vassy, J.L.; Shin, H.; Lee, Y.H.; Ahn, H.Y.; Choi, S.H.; Park, K.S.; Jang, H.C.; Lim, S. Efficacy and safety of ginsam, a vinegar extract from Panax ginseng, in type 2 diabetic patients: Results of a double-blind, placebo-controlled study. J. Diabetes Investig. 2012, 3, 309–317. [Google Scholar] [CrossRef] [Green Version]
- Ghavami, A.; Ziaei, R.; Foshati, S.; Hojati Kermani, M.A.; Zare, M.; Amani, R. Benefits and harms of ginseng supplementation on liver function? a systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2020, 39, 101173. [Google Scholar] [CrossRef] [PubMed]
- Hernández-García, D.; Granado-Serrano, A.B.; Martín-Gari, M.; Naudí, A.; Serrano, J.C. Efficacy of Panax ginseng supplementation on blood lipid profile: A meta-analysis and systematic review of clinical randomized trials. J. Ethnopharmacol. 2019, 243, 112090. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, H.; Hadi, A.; Kord-Varkaneh, H.; Arab, A.; Afshari, M.; Ferguson, A.J.R.; Ghaedi, E. Effects of ginseng supplementation on selected markers of inflammation: A systematic review and meta-analysis. Phytother. Res. PTR 2019, 33, 1991–2001. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Chung, S.; Chung, M.-Y.; Choi, H.-K.; Hwang, J.-T.; Park, J.H. Effects of Panax ginseng on hyperglycemia, hypertension, and hyperlipidemia: A systematic review and meta-analysis. J. Ginseng Res. 2022, 46, 188–205. [Google Scholar] [CrossRef] [PubMed]
- Saboori, S.; Falahi, E.; Yousefi Rad, E.; Asbaghi, O.; Khosroshahi, M.Z. Effects of ginseng on C-reactive protein level: A systematic review and meta-analysis of clinical trials. Complement. Ther. Med. 2019, 45, 98–103. [Google Scholar] [CrossRef]
- Ziaei, R.; Ghavami, A.; Ghaedi, E.; Hadi, A.; Javadian, P.; Clark, C.C.T. The efficacy of ginseng supplementation on plasma lipid concentration in adults: A systematic review and meta-analysis. Complement. Ther. Med. 2020, 48, 102239. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Brondani, L.A.; Assmann, T.S.; de Souza, B.M.; Bouças, A.P.; Canani, L.H.; Crispim, D. Meta-analysis reveals the association of common variants in the uncoupling protein (UCP) 1-3 genes with body mass index variability. PLoS ONE 2014, 9, e96411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menon, K.; Marquina, C.; Hoj, P.; Liew, D.; Mousa, A.; de Courten, B. Carnosine and histidine-containing dipeptides improve dyslipidemia: A systematic review and meta-analysis of randomized controlled trials. Nutr. Rev. 2020, 78, 939–951. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, A.L.; Morgan, L.M.; Bishop, J.; Jovanovski, E.; Jenkins, D.J.A.; Vuksan, V. Co-administration of a konjac-based fibre blend and American ginseng (Panax quinquefolius L.) on glycaemic control and serum lipids in type 2 diabetes: A randomized controlled, cross-over clinical trial. Eur. J. Nutr. 2018, 57, 2217–2225. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Yoon, K.H.; Kang, M.J.; Yim, H.W.; Lee, K.S.; Vuksan, V.; Sung, M.K. A six-month supplementation of mulberry, korean red ginseng, and banaba decreases biomarkers of systemic low-grade inflammation in subjects with impaired glucose tolerance and type 2 diabetes. Evid.-Based Complement. Altern. Med. 2012, 2012, 735191. [Google Scholar] [CrossRef]
- Mohammad-Saeed, B.; Mohammad-Ali, A.; Mahmoud, R.-k. Effect of diabetan on blood glucose, glycosylated hemoglobin, lipid profile, liver and kidney function tests of diabetic patients: A clinical, double blind, randomized trial. Afr. J. Pharm. Pharmacol. 2013, 7, 50–53. [Google Scholar] [CrossRef]
- Park, S.; Kim, C.J.; Ha, K.C.; Baek, H.I.; Yang, H.J.; Kim, M.J.; Park, S.J. Efficacy and safety of aronia, red ginseng, shiitake mushroom, and nattokinase mixture on insulin resistance in prediabetic adults: A randomized, double-blinded, placebo-controlled trial. Foods 2021, 10, 1558. [Google Scholar] [CrossRef]
- Shin, S.K.; Kwon, J.H.; Jeong, Y.J.; Jeon, S.M.; Choi, J.Y.; Choi, M.S. Supplementation of cheonggukjang and red ginseng cheonggukjang can improve plasma lipid profile and fasting blood glucose concentration in subjects with impaired fasting glucose. J. Med. Food 2011, 14, 108–113. [Google Scholar] [CrossRef]
- Zurbau, A.; Smircic Duvnjak, L.; Magas, S.; Jovanovski, E.; Miocic, J.; Jenkins, A.L.; Jenkins, D.J.A.; Josse, R.G.; Leiter, L.A.; Sievenpiper, J.L.; et al. Co-administration of viscous fiber, Salba-chia and ginseng on glycemic management in type 2 diabetes: A double-blind randomized controlled trial. Eur. J. Nutr. 2021, 60, 3071–3083. [Google Scholar] [CrossRef]
- Choi, K.M.; Lee, E.J.; Kim, Y.H.; Baik, S.H.; Kim, Y.K.; Choi, D.S. Erythrocyte and antioxidant superoxide dismutase (SOI) activity in NIDDM patients. Korean J. Ginseng Sci. 1997, 21, 153–159. [Google Scholar]
- Kim, H.-O.; Park, M.-J.; Han, J.-S. Effects of fermented red ginseng supplementation on blood glucose and insulin resistance in type 2 diabetic patients. J. Korean Soc. Food Sci. Nutr. 2011, 40, 696–703. [Google Scholar] [CrossRef]
- Hosseini, S.A.; Alipour, M.; Zakerish, M.; Haghighizadeh, M.H. Effects of standardized extract of ginseng [G115] on biomarkers of systemic low-grade inflammation in patients with type 2 diabetes: A double-blind clinical trial. Iran. J. Endocrinol. Metab. 2014, 16, 175–182. [Google Scholar]
- Jovanovski, E.; Jenkins, A.; Vuksan, V. Effects of Korean White Ginseng (Panax ginseng CA Meyer) on vascular and glycemic health in type 2 diabetes: Results of a randomized, double blind, placebo-controlled, multiple-crossover, acute dose escalation trial. Clin. Nutr. Res. 2014, 3, 89–97. [Google Scholar]
- Bang, H.; Kwak, J.H.; Ahn, H.Y.; Shin, D.Y.; Lee, J.H. Korean red ginseng improves glucose control in subjects with impaired fasting glucose, impaired glucose tolerance, or newly diagnosed type 2 diabetes mellitus. J. Med. Food 2014, 17, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseini, S.A.; Ehsanpour, A.; Asgari, M.; Malihi, R. Evaluation of standardized ginseng extract Panax (G115®) effect on fasting blood glucose levels, glycated hemoglobin and lipid profile in patients with diabetes type 2. Jundishapur J. Chronic Dis. Care 2013, 2, 26–32. [Google Scholar]
- Jovanovski, E.; Lea Duvnjak, S.; Komishon, A.; Au-Yeung, F.; Zurbau, A.; Jenkins, A.L.; Sung, M.K.; Josse, R.; Vuksan, V. Vascular effects of combined enriched Korean Red ginseng (Panax ginseng) and American ginseng (Panax quinquefolius) administration in individuals with hypertension and type 2 diabetes: A randomized controlled trial. Complement. Ther. Med. 2020, 49, 102338. [Google Scholar] [CrossRef]
- Park, S.H.; Oh, M.R.; Choi, E.K.; Kim, M.G.; Ha, K.C.; Lee, S.K.; Kim, Y.G.; Park, B.H.; Kim, D.S.; Chae, S.W. An 8-wk, randomized, double-blind, placebo-controlled clinical trial for the antidiabetic effects of hydrolyzed ginseng extract. J. Ginseng Res. 2014, 38, 239–243. [Google Scholar] [CrossRef] [Green Version]
- Reeds, D.N.; Patterson, B.W.; Okunade, A.; Holloszy, J.O.; Polonsky, K.S.; Klein, S. Ginseng and ginsenoside Re do not improve β-cell function or insulin sensitivity in overweight and obese subjects with impaired glucose tolerance or diabetes. Diabetes Care 2011, 34, 1071–1076. [Google Scholar] [CrossRef] [Green Version]
- Sotaniemi, E.A.; Haapakoski, E.; Rautio, A. Ginseng therapy in non-insulin-dependent diabetic patients. Diabetes Care 1995, 18, 1373–1375. [Google Scholar] [CrossRef]
- Ma, S.W.; Benzie, I.F.; Chu, T.T.; Fok, B.S.; Tomlinson, B.; Critchley, L.A. Effect of Panax ginseng supplementation on biomarkers of glucose tolerance, antioxidant status and oxidative stress in type 2 diabetic subjects: Results of a placebo-controlled human intervention trial. Diabetes Obes. Metab. 2008, 10, 1125–1127. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Qu, C.-Y.; Li, J.-X.; Wang, Y.-F.; Li, W.; Wang, C.-Z.; Wang, D.-S.; Song, J.; Sun, G.-Z.; Yuan, C.-S. Hypoglycemic and hypolipidemic effects of malonyl ginsenoides from American ginseng (Panax quinquefolius L.) on type 2 diabetic mice. ACS Omega 2021, 6, 33652–33664. [Google Scholar] [CrossRef] [PubMed]
- Gui, Q.-f.; Xu, Z.-r.; Xu, K.-y.; Yang, Y.-m. The efficacy of ginseng-related therapies in type 2 diabetes mellitus: An updated systematic review and meta-analysis. Medicine 2016, 95, e2584. [Google Scholar] [CrossRef]
- Ma, C.; Yu, H.; Xiao, Y.; Wang, H. Momordica charantia extracts ameliorate insulin resistance by regulating the expression of SOCS-3 and JNK in type 2 diabetes mellitus rats. Pharm. Biol. 2017, 55, 2170–2177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, T.; Nguyen, T.T.; Zimmerman, B.R. Hyperlipidemia and diabetes mellitus. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 1998; pp. 969–976. [Google Scholar]
- Oza, M.J.; Kulkarni, Y.A. Biochanin A improves insulin sensitivity and controls hyperglycemia in type 2 diabetes. Biomed. Pharmacother. 2018, 107, 1119–1127. [Google Scholar] [CrossRef]
- Wang, D.-S.; Wang, J.-M.; Zhang, F.-R.; Lei, F.-J.; Wen, X.; Song, J.; Sun, G.-Z.; Liu, Z. Ameliorative effects of malonyl ginsenoide from Panax ginseng on glucose-lipid metabolism and insulin resistance via IRS1/PI3K/Akt and AMPK signaling pathways in type 2 diabetic mice. Am. J. Chin. Med. 2022, 50, 863–882. [Google Scholar] [CrossRef]
- Kim, S.-H.; Park, K.-S. Effects of Panax ginseng extract on lipid metabolism in humans. Pharmacol. Res. 2003, 48, 511–513. [Google Scholar] [CrossRef]
- Song, Y.B.; An, Y.R.; Kim, S.J.; Park, H.W.; Jung, J.W.; Kyung, J.S.; Hwang, S.Y.; Kim, Y.S. Lipid metabolic effect of Korean red ginseng extract in mice fed on a high-fat diet. J. Sci. Food Agric. 2012, 92, 388–396. [Google Scholar] [CrossRef]
- Gandhi, G.R.; Vasconcelos, A.B.S.; Wu, D.-T.; Li, H.-B.; Antony, P.J.; Li, H.; Geng, F.; Gurgel, R.Q.; Narain, N.; Gan, R.-Y. Citrus flavonoids as promising phytochemicals targeting diabetes and related complications: A systematic review of in vitro and in vivo studies. Nutrients 2020, 12, 2907. [Google Scholar] [CrossRef]
- Burgos-Morón, E.; Abad-Jiménez, Z.; Martinez de Maranon, A.; Iannantuoni, F.; Escribano-López, I.; López-Domènech, S.; Salom, C.; Jover, A.; Mora, V.; Roldan, I. Relationship between oxidative stress, ER stress, and inflammation in type 2 diabetes: The battle continues. J. Clin. Med. 2019, 8, 1385. [Google Scholar] [CrossRef] [Green Version]
- Alzamil, H. Elevated serum TNF-α is related to obesity in type 2 diabetes mellitus and is associated with glycemic control and insulin resistance. J. Obes. 2020, 2020, 5076858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alolga, R.N.; Nuer-Allornuvor, G.F.; Kuugbee, E.D.; Yin, X.; Ma, G. Ginsenoside Rg1 and the control of inflammation implications for the therapy of type 2 diabetes: A review of scientific findings and call for further research. Pharmacol. Res. 2020, 152, 104630. [Google Scholar] [CrossRef] [PubMed]
- Hong, B.N.; Ji, M.G.; Kang, T.H. The efficacy of red ginseng in type 1 and type 2 diabetes in animals. Evid.-Based Complement. Altern. Med. 2013, 2013, 593181. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Liu, W.; Ding, C.; Zhao, Y.; Chen, X.; Khatoon, S.; Zheng, Y.; Cheng, Z.; Xi, G. Antidiabetic effects of arginyl-fructosyl-glucose, a nanosaponin fraction from ginseng processing in streptozotocin-induced type 2 diabetic mice through regulating the PI3K/AKT/GSK-3β and Bcl-2/Bax Signaling pathways. Evid.-Based Complement. Altern. Med. 2020, 2020, 3707904. [Google Scholar] [CrossRef]
- Park, S.J.; Nam, J.; Ahn, C.W.; Kim, Y. Anti-diabetic properties of different fractions of Korean red ginseng. J. Ethnopharmacol. 2019, 236, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Malone, J.I.; Hansen, B.C. Does obesity cause type 2 diabetes mellitus (T2DM)? Or is it the opposite? Pediatr. Diabetes 2019, 20, 5–9. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.S.; Yoon, M. Korean red ginseng (Panax ginseng) inhibits obesity and improves lipid metabolism in high fat diet-fed castrated mice. J. Ethnopharmacol. 2018, 210, 80–87. [Google Scholar] [CrossRef]
- Nagar, H.; Kang, S.K.; Choi, S.W.; Song, H.-J.; Choi, S.-J.; Piao, S.; Kim, S.; Lee, I.; Kim, C.-S. Antihypertensive effects of Rg3-enriched Korean vitamin ginseng in spontaneously hypertensive rats. Nat. Prod. Commun. 2020, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ran, X.; Dou, D.; Chen, H.; Ren, G. The correlations of adverse effect and tonifying effect of ginseng medicines. J. Ethnopharmacol. 2022, 291, 115113. [Google Scholar] [CrossRef] [PubMed]
- Hur, M.-H.; Lee, M.-S.; Yang, H.-J.; Kim, C.; Bae, I.-L.; Ernst, E. Ginseng for reducing the blood pressure in patients with hypertension: A systematic review and meta-analysis. J. Ginseng Res. 2010, 34, 342–347. [Google Scholar] [CrossRef] [Green Version]
- Komishon, A.; Shishtar, E.; Ha, V.; Sievenpiper, J.; de Souza, R.; Jovanovski, E.; Ho, H.; Duvnjak, L.; Vuksan, V. The effect of ginseng (genus Panax) on blood pressure: A systematic review and meta-analysis of randomized controlled clinical trials. J. Hum. Hypertens. 2016, 30, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Park, T.Y.; Hong, M.; Sung, H.; Kim, S.; Suk, K.T. Effect of Korean red ginseng in chronic liver disease. J. Ginseng Res. 2017, 41, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Gwak, S.R.; Joo, J.C.; Song, B.K.; Cha, S.W.; Song, Y.U.; Pyo, M.K.; Park, S.J. Effectiveness and safety of Panax ginseng extract on hepatic dysfunction: A randomized, double-blind, placebo-controlled clinical trial. Evid.-Based Complement. Altern. Med. 2020, 2020, 2689565. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Inclusion Criteria |
|---|---|
| Population | Individuals older than 18 years and with physician’s diagnosis of impaired glucose tolerance or prediabetes or T2DM |
| Intervention | Administration of ginseng in different chemical forms including capsule, tablet, and powder |
| Comparator | Comparison with placebo, usual care, or any pharmacological or non-pharmacological intervention(s) |
| Outcome | Those which reported mean changes and their standard deviations (SDs) of anthropometric indices (weight, BMI, and WC), glycemic control parameters (FPG, insulin, HbA1c, OGTT, and HOMA-IR), lipid profile components (TG, TC, LDL-C, and HDL-C), blood pressure (SBP and DBP), HR, inflammatory biomarkers and adipokines (CRP, IL-6, TNF-α, adiponectin, and leptin), and liver function tests (ALT, AST, and GGT) throughout the trial for both intervention and control groups or those presenting the required information to calculate these effect sizes |
| Study design | Being an RCT in either parallel or cross-over design |
| Studies | Country | Study Design | Participant | Sex | Sample Size | Trial Duration (Week) | Means Age | Means BMI | Intervention | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IG | CG | IG | CG | IG | CG | Ginseng Dose | Ginseng Type | Control Group | ||||||
| Sotaniemi et al., 1995 (A) [58] | Finland | paralell, R, PC, DB | T2DM | M/F (8, 10) | 12 | 6 | 8 | 59 ± 7 | 60 ± 6 | NR | NR | 0.1 | Ginseng extract | Placebo |
| Finland | paralell, R, PC, DB | T2DM | M/F (8, 10) | 12 | 6 | 8 | 57 ± 9 | 60 ± 6 | NR | NR | 0.2 | Ginseng extract | Placebo | |
| Sotaniemi et al., 1995 (B) [58] | Canada | cross-over, R, PC, DB | T2DM | M/F (11, 8) | 9 | 10 | 12 | 64 ± 6 | 64 ± 6.32 | 28.9 ± 4.2 | 28.9 ± 4.42 | 6 | Panax ginseng | Placebo |
| Hong Kong | cross-over, R, PC, DB | T2DM | M/F | 10 | 10 | 4 | 51.5 ± 6 | 51.5 ± 6 | 28.5 ± 4.11 | 28.5 ± 4.11 | 2.214 | Panax ginseng | Placebo | |
| Vuksan et al., 2008 [12] | USA | paralell, R, PC, DB | T2DM | M/F (7, 1) | 5 | 3 | 4 | 46 ± 6.7 | 46 ± 5.19 | 31 ± 2.23 | 36 ± 3.46 | 8 | Panax ginseng | Placebo |
| USA | paralell, R, PC, DB | T2DM | M (7) | 5 | 2 | 4 | 46 ± 6.7 | 46 ± 4.24 | 35 ± 6.70 | 36 ± 2.82 | 0.35 | Panax ginseng | Placebo | |
| Ma et al., 2008 [59] | South Korea | paralell, R, PC, DB | T2DM | M/F (13, 11) | 18 | 6 | 8 | 52.7 ± 11 | 54.8 ± 10 | 26.3 ± 4.8 | 25.3 ± 1.9 | 1.5 | Panax ginseng | Placebo |
| South Korea | paralell, R, PC, DB | T2DM | M/F (15, 9) | 18 | 6 | 8 | 52.7 ± 10 | 54.8 ± 10 | 24 ± 2.6 | 25.3 ± 1.9 | 2 | Panax ginseng | Placebo | |
| Reedes et al., 2011 (A) [57] | South Korea | paralell, R, PC, DB | T2DM | M/F (16, 8) | 18 | 6 | 8 | 51.1 ± 8.6 | 54.8 ± 10 | 25.4 ± 2.7 | 25.3 ± 1.9 | 3 | Panax ginseng | Placebo |
| Iran | paralell, R, PC, DB | T2DM | M/F (14, 16) | 15 | 15 | 8 | 48.1 ± 5.7 | 46 ± 4.5 | 29.9 ± 3 | 30.6 ± 2.8 | 0.3 | Panax ginseng | Placebo | |
| Reedes et al., 2011 (B) [57] | Croatia | paralell, R, PC, DB | T2DM & HTN | M/F (22, 42) | 30 | 34 | 12 | 62.1 ± 8.8 | 63.9 ± 10.93 | 33.4 ± 5.6 | 29.9 ± 4.95 | 3 | Panax quinquefolius | Placebo |
| South Korea | paralell, R, PC, DB | Impaired fasting glucose | M/F (10, 10) | 11 | 9 | 8 | 50.45 ± 12.36 | 44.56 ± 10.48 | NR | NR | 0.96 | Panax ginseng | Placebo | |
| Yoon et al., 2012 (A) [30] | South Korea | paralell, R, PC, DB | T2DM | M/F (28, 13) | 21 | 20 | 12 | 58.81 ± 1.72 | 56.1 ± 2.18 | 23.52 ± 0.48 | 23.8 ± 0.61 | 5 | Panax ginseng | Placebo |
| South Korea | paralell, R, PC, DB | Impaired fasting glucose/T2DM | M/F (28, 14) | 21 | 21 | 4 | 53.2 ± 1.8 | 53.5 ± 1.9 | 24.9 ± 0.7 | 24.9 ± 0.8 | 2.7 | Panax ginseng | Placebo | |
| Yoon et al., 2012 (B) [30] | Croatia | paralell, R, PC, DB | T2DM | M/F (28, 46) | 35 | 39 | 12 | 61.9 ± 8.59 | 63.7 ± 10.28 | 33 ± 5.53 | 30.1 ± 4.68 | 3 | Panax quinquefolius | Placebo |
| Iran | paralell, R, PC, DB | T2DM | M/F (12, 28) | 20 | 20 | 8 | 47.9 ± 4.7 | 47.3 ± 6.4 | 29.29 ± 3.61 | 27.19 ± 4.71 | 0.3 | Panax ginseng | Placebo | |
| Yoon et al., 2012 (C) [30] | Iran | paralell, R, PC, DB | T2DM | M/F (11, 34) | 23 | 22 | 6 | 47.9 ± 4.7 | 47.3 ± 6.4 | 29.29 ± 3.61 | 27.19 ± 4.71 | 0.3 | Ginseng extract | Placebo |
| South Korea | paralell, R, PC, DB | T2DM | M/F (42, 30) | 34 | 38 | 12 | 52.76 ± 10.24 | 51.89 ± 9.46 | 25.52 ± 2.87 | 25.61 ± 3.05 | 1 | Panax ginseng | Placebo | |
| Hosseini et al., 2013 [54] | Canada | cross-over, R, PC, DB | T2DM | M/F (13, 11) | 12 | 12 | 8 | 64 ± 7 | 64 ± 7 | 27.8 ± 4.6 | 27.8 ± 4.6 | 3 | Panax quinquefolius | Placebo |
| Australia | paralell, R, PC, DB | Prediabetes | M/F (153, 248) | 202 | 199 | 24 | 53.4 ± 10 | 53.65 ± 10.4 | 34.7 ± 6.5 | 34.6 ± 6.0 | 0.32 | Panax ginseng | Placebo | |
| Mucalo et al., 2013 [28] | South Korea | paralell, R, PC, DB | T2DM | M/F (35, 24) | 28 | 31 | 24 | 61.2 ± 8.45 | 60.9 ± 7.23 | 24.5 ± 2.90 | 24.8 ± 2.82 | 1 | Panax ginseng | Placebo |
| South Korea | paralell, R, PC, DB | T2DM nephropathy | M/F (36, 25) | 30 | 31 | 24 | 59.3 ± 8.79 | 59.7 ± 7.22 | 24.7 ± 2.93 | 24.8 ± 2.82 | 3 | Panax ginseng | Placebo | |
| Park et al., 2014 [56] | Canada and Croatia | paralell, R, PC, DB | T2DM & HTN | M/F (49, 31) | 43 | 37 | 12 | 59.44 ± 7.4 | 60.58 ± 6.9 | 28.62 ± 3.4 | 29.66 ± 4.3 | 6.75 | Panax ginseng and Panax quinquefolius | Placebo |
| Canada and Croatia | paralell, R, PC, DB | T2DM & HTN | M/F (49, 31) | 43 | 37 | 12 | 59.44 ± 7.4 | 60.58 ± 6.9 | 28.62 ± 3.4 | 29.66 ± 4.3 | 2.25 | Panax ginseng and Panax quinquefolius | Placebo | |
| Number of Studies | WMD (95% CI) | p-Value | Heterogeneity | ||
|---|---|---|---|---|---|
| p Heterogeneity | I2 | ||||
| Subgroup analyses of ginseng supplementation on BW | |||||
| Overall effect | 5 | −0.54 (−2.54, 1.46) | 0.598 | 0.998 | 0.0% |
| Subgroup analyses of ginseng supplementation on BMI | |||||
| Overall effect | 9 | 0.05 (−0.26, 0.38) | 0.717 | 0.963 | 0.0% |
| Baseline BMI (kg/m2) | |||||
| Normal (18.5–24.9) | 3 | 0.118 (−0.37, 0.60) | 0.639 | 0.605 | 0.0% |
| Overweight (25–29.9) | 3 | 0.17 (−0.34, 0.69) | 0.501 | 0.961 | 0.0% |
| Obese (>30) | 3 | −0.31 (−1.05, 0.42) | 0.405 | 0.931 | 0.0% |
| Trial duration (week) | |||||
| ≤8 | 6 | 0.10 (−0.31, 0.53) | 0.617 | 0.991 | 0.0% |
| >8 | 3 | −0.00 (−0.49, 0.48) | 0.983 | 0.404 | 0.0% |
| Supplementation dose (g/day) | |||||
| <2 | 5 | 0.08 (−0.36, 0.52) | 0.713 | 0.694 | 0.0% |
| ≥2 | 4 | 0.03 (−0.43, 0.49) | 0.888 | 0.976 | 0.0% |
| Subgroup analyses of ginseng supplementation on WC | |||||
| Overall effect | 3 | 0.05 (−1.16, 1.27) | 0.929 | 0.729 | 0.0% |
| Subgroup analyses of ginseng supplementation on FPG | |||||
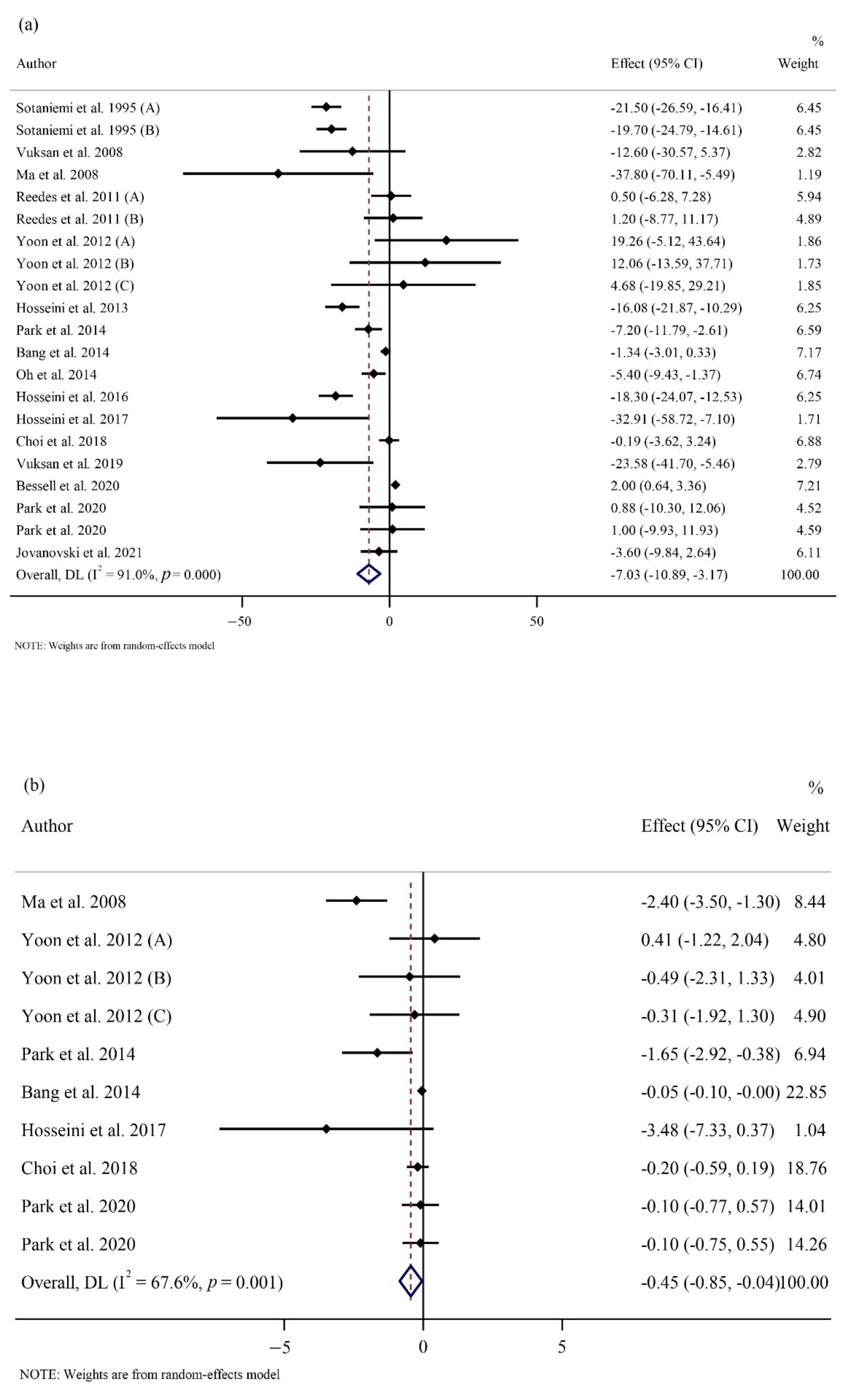
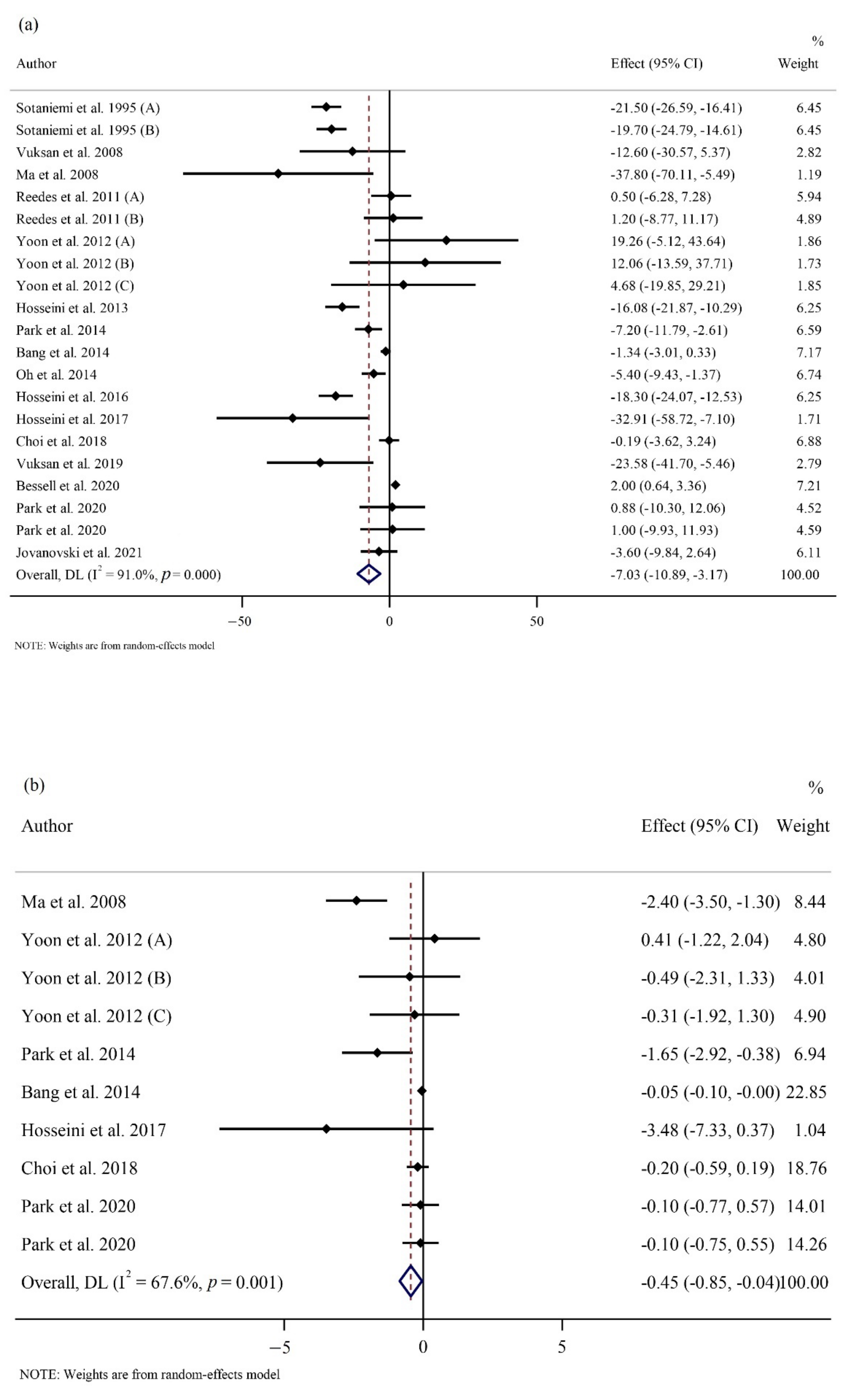
| Overall effect | 21 | −7.03 (−10.89, −3.17) | <0.001 | <0.001 | 91.0% |
| Baseline FPG (mg/dL) | |||||
| ≥126 | 11 | −9.69 (−16.70, −2.69) | 0.007 | <0.001 | 73.9% |
| <126 | 7 | −1.51 (−4.06, 1.04) | 0.247 | <0.001 | 77.9% |
| Trial duration (week) | |||||
| ≤8 | 14 | −10.71 (−16.23, −5.18) | <0.001 | <0.001 | 83.9% |
| >8 | 7 | −0.21 (−2.33, 1.90) | 0.842 | 0.040 | 54.6% |
| Supplementation dose (g/day) | |||||
| <2 | 11 | −8.72 (−15.53, −1.90) | 0.012 | <0.001 | 95.1% |
| ≥2 | 10 | −3.32 (−6.81, 0.17) | 0.063 | 0.044 | 48.1% |
| Subgroup analyses of ginseng supplementation on OGTT | |||||
| Overall effect | 10 | −6.81 (−16.77, 3.14) | 0.180 | 0.002 | 66.3% |
| Trial duration (week) | |||||
| ≤8 | 6 | −7.17 (−22.60, 8.25) | 0.362 | 0.009 | 67.3% |
| >8 | 4 | −3.63 (−10.00, 2.74) | 0.264 | 0.865 | 0.0% |
| Supplementation dose (g/day) | |||||
| <2 | 3 | −5.75 (−31.60, 20.10) | 0.663 | 0.001 | 85.6% |
| ≥2 | 7 | −6.20 (−12.55, 0.14) | 0.055 | 0.402 | 3.0% |
| Subgroup analyses of ginseng supplementation on HbA1c | |||||
| Overall effect | 15 | −0.04 (−0.16, 0.07) | 0.449 | <0.001 | 82.9% |
| Baseline HbA1c (%) | |||||
| <6.5 | 6 | 0.04 (−0.01, 0.09) | 0.117 | 0.278 | 20.6% |
| ≥6.5 | 9 | −0.08 (−0.28, 0.11) | 0.417 | <0.001 | 78.5% |
| Trial duration (week) | |||||
| ≤8 | 8 | 0.03 (−0.30, 0.37) | 0.838 | <0.001 | 80.8% |
| >8 | 7 | −0.04 (−0.14, 0.05) | 0.397 | <0.001 | 75.2% |
| Supplementation dose (g/day) | |||||
| <2 | 7 | −0.07 (−0.27, 0.12) | 0.476 | <0.001 | 88.4% |
| ≥2 | 8 | −0.00 (−0.19, 0.18) | 0.962 | 0.001 | 71.2% |
| Subgroup analyses of ginseng supplementation on fasting insulin | |||||
| Overall effect | 16 | −0.13 (−1.18, 0.90) | 0.796 | <0.001 | 89.8% |
| Trial duration (week) | |||||
| ≤8 | 10 | 0.49 (−1.12, 2.11) | 0.547 | 0.023 | 53.4% |
| >8 | 6 | −0.74 (−1.72, 0.24) | 0.140 | 0.003 | 71.6% |
| Supplementation dose (g/day) | |||||
| <2 | 6 | −0.38 (−1.83, 1.06) | 0.601 | 0.154 | <0.001 |
| ≥2 | 10 | 0.02 (−1.31, 1.36) | 0.974 | <0.001 | 93.4% |
| Subgroup analyses of ginseng supplementation on HOMA-IR | |||||
| Overall effect | 10 | −0.44 (−0.84, −0.04) | 0.030 | 0.001 | 67.6% |
| Trial duration (week) | |||||
| ≤8 | 6 | −1.15 (−2.17, −0.13) | 0.027 | 0.037 | 57.7% |
| >8 | 4 | −0.05 (−0.09, −0.00) | 0.022 | 0.899 | 0.0% |
| Supplementation dose (g/day) | |||||
| <2 | 5 | −0.41 (−1.05, 0.21) | 0.196 | 0.084 | 51.3% |
| ≥2 | 5 | −0.59 (−1.34, 0.16) | 0.126 | 0.001 | 77.6% |
| Subgroup analyses of ginseng supplementation on TG | |||||
| Overall effect | 12 | 6.05 (−4.37, 16.48) | 0.255 | <0.001 | 73.5% |
| Baseline TG (mg/dL) | |||||
| <150 | 6 | 17.23 (12.25, 22.21) | <0.001 | 0.479 | 0.0% |
| ≥150 | 6 | −2.68 (−22.50, 17.14) | 0.791 | 0.010 | 67.0% |
| Trial duration (week) | |||||
| ≤8 | 7 | 9.69 (−3.36, 22.75) | 0.146 | 0.002 | 71.9% |
| >8 | 5 | −4.45 (−29.17, 20.25) | 0.724 | 0.001 | 78.9% |
| Supplementation dose (g/day) | |||||
| <2 | 5 | 6.61 (−7.46, 20.68) | 0.357 | 0.157 | 39.6% |
| ≥2 | 7 | 4.76 (−9.14, 18.67) | 0.502 | 0.001 | 72.1%d |
| Subgroup analyses of ginseng supplementation on TC | |||||
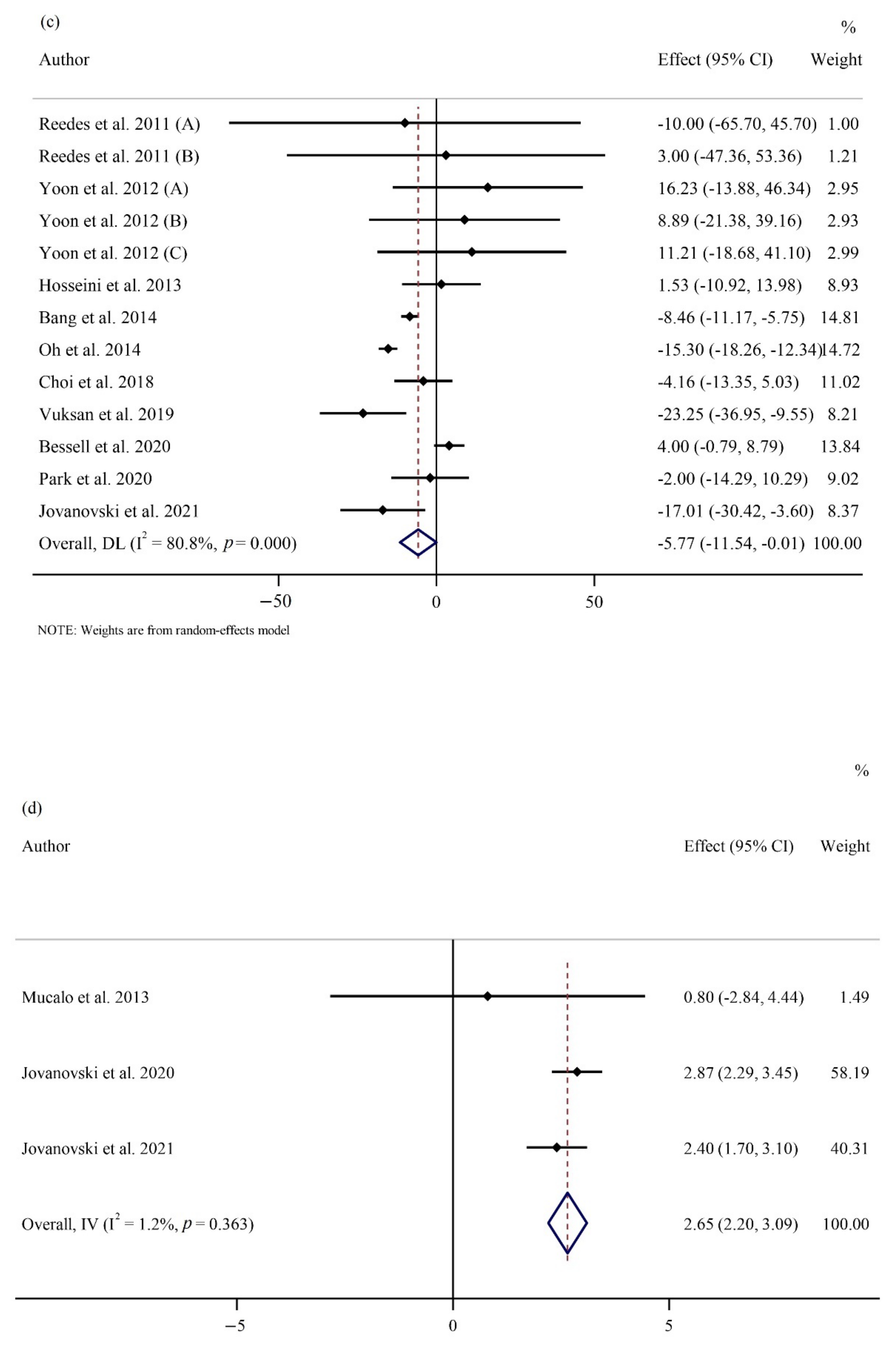
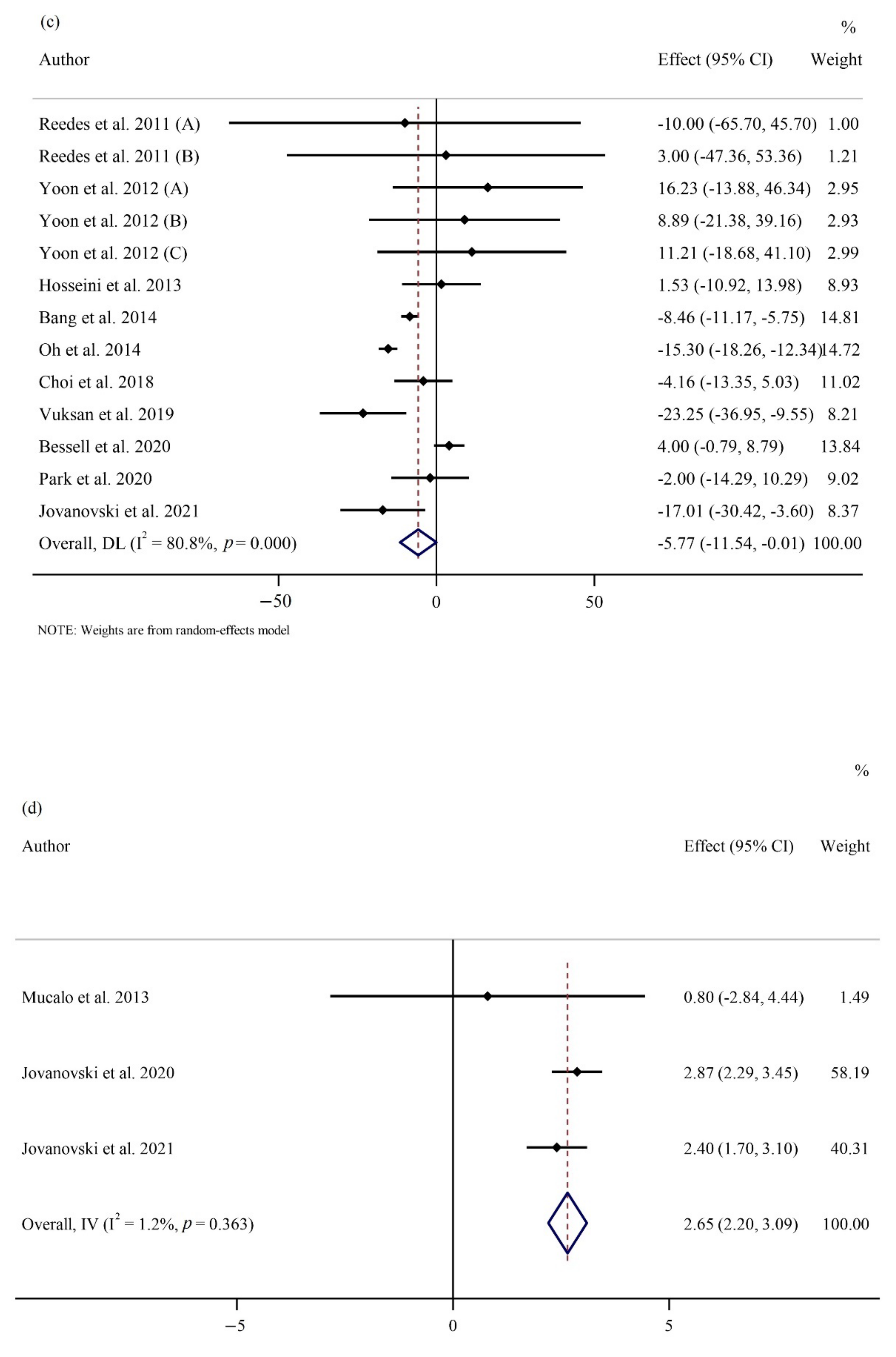
| Overall effect | 13 | −5.77 (−11.53, −0.01) | 0.049 | <0.001 | 80.8% |
| Baseline TC (mg/dL) | |||||
| ≥200 | 7 | −3.84 (−16.26, 8.57) | 0.544 | <0.001 | 89.1% |
| <200 | 6 | −7.04 (−10.78, −3.31) | <0.001 | 0.323 | 14.2% |
| Trial duration (week) | |||||
| ≤8 | 8 | −5.64 (−15.98, 4.69) | 0.285 | 0.013 | 60.5% |
| >8 | 5 | −4.77 (−11.94, 2.39) | 0.192 | <0.001 | 82.5% |
| Supplementation dose (g/day) | |||||
| <2 | 5 | 2.42 (−1.54, 6.40) | 0.231 | 0.523 | 0.0% |
| ≥2 | 8 | −11.10 (−16.53, −5.68) | <0.001 | 0.004 | 66.5% |
| Subgroup analyses of ginseng supplementation on LDL-C | |||||
| Overall effect | 13 | −4.16 (−8.98, 0.65) | 0.090 | <0.001 | 78.2% |
| Baseline LDL (mg/dL) | |||||
| ≥130 | 2 | 0.09 (−4.03, 4.22) | 0.965 | 0.666 | 0.0% |
| <130 | 11 | −5.04 (−10.22, 0.14) | 0.057 | <0.001 | 76.2% |
| Trial duration (week) | |||||
| ≤8 | 8 | −0.12 (−8.54, 8.29) | 0.977 | 0.025 | 56.3% |
| >8 | 5 | −6.59 (−13.37, 0.19) | 0.057 | <0.001 | 86.6% |
| Supplementation dose (g/day) | |||||
| <2 | 5 | −0.40 (−5.55, 4.74) | 0.877 | 0.281 | 21.0% |
| ≥2 | 8 | −6.81 (−12.73, −0.88) | 0.024 | <0.001 | 79.5% |
| Subgroup analyses of ginseng supplementation on HDL-C | |||||
| Overall effect | 13 | −1.28 (−5.58, 3.01) | 0.557 | <0.001 | 96.9% |
| Baseline HDL (mg/dL) | |||||
| <50 | 7 | 0.95 (−0.74, 2.64) | 0.273 | 0.949 | 0.0% |
| ≥50 | 6 | −3.05 (−9.53, 3.42) | 0.355 | <0.001 | 98.4% |
| Trial duration (week) | |||||
| ≤8 | 8 | −0.14 (−1.41, 1.12) | 0.822 | 0.998 | 0.0% |
| >8 | 5 | −2.53 (−10.04, 4.98) | 0.509 | <0.001 | 98.6% |
| Supplementation dose (g/day) | |||||
| <2 | 5 | −0.20 (−1.53, 1.12) | 0.762 | 0.876 | 0.0% |
| ≥2 | 8 | −1.60 (−7.61, 4.40) | 0.600 | <0.001 | 97.7% |
| Subgroup analyses of ginseng supplementation on SBP | |||||
| Overall effect | 10 | −2.78 (−6.97, 1.40) | 0.193 | <0.001 | 87.4% |
| Baseline SBP (mmHg) | |||||
| ≥130 | 5 | −4.51 (−14.18, 5.15) | 0.360 | <0.001 | 92.8% |
| <130 | 5 | −0.96 (−2.06, 0.13) | 0.086 | 0.704 | 0.0% |
| Trial duration (week) | |||||
| ≤8 | −3.22 (−10.68, 4.23) | 0.397 | 0.079 | 55.8% | |
| >8 | −2.59 (−7.79, 2.60) | 0.328 | <0.001 | 92.0% | |
| Supplementation dose (g/day) | |||||
| <2 | 2 | 2.75 (−2.15, 7.67) | 0.271 | 0.845 | 0.0% |
| ≥2 | 8 | −3.92 (−8.77, 0.91) | 0.112 | <0.001 | 89.7% |
| Subgroup analyses of ginseng supplementation on DBP | |||||
| Overall effect | 10 | −0.24 (−1.88, 1.39) | 0.770 | 0.003 | 63.4% |
| Baseline SBP (mmHg) | |||||
| ≥80 | 8 | 0.56 (−1.43, 2.56) | 0.582 | 0.004 | 66.8% |
| <80 | 2 | −2.63 (−6.54, 1.27) | 0.186 | 0.081 | 67.2% |
| Trial duration (week) | |||||
| ≤8 | 4 | 0.04 (−4.88, 4.96) | 0.987 | 0.024 | 68.1% |
| >8 | 6 | −0.20 (−1.96, 1.56) | 0.821 | 0.010 | 67.0% |
| Supplementation dose (g/day) | |||||
| <2 | 2 | 3.00 (−0.13, 6.14) | 0.061 | 0.998 | 0.0% |
| ≥2 | 8 | −0.93 (−2.50, 0.64) | 0.247 | 0.024 | 56.6% |
| Subgroup analyses of ginseng supplementation on HR | |||||
| Overall effect | 3 | 2.65 (2.20, 3.09) | <0.001 | 0.363 | 1.2% |
| Subgroup analyses of ginseng supplementation on CRP | |||||
| Overall effect | 6 | −0.10 (−0.61, 0.41) | 0.696 | 0.046 | 55.8% |
| Subgroup analyses of ginseng supplementation on IL−6 | |||||
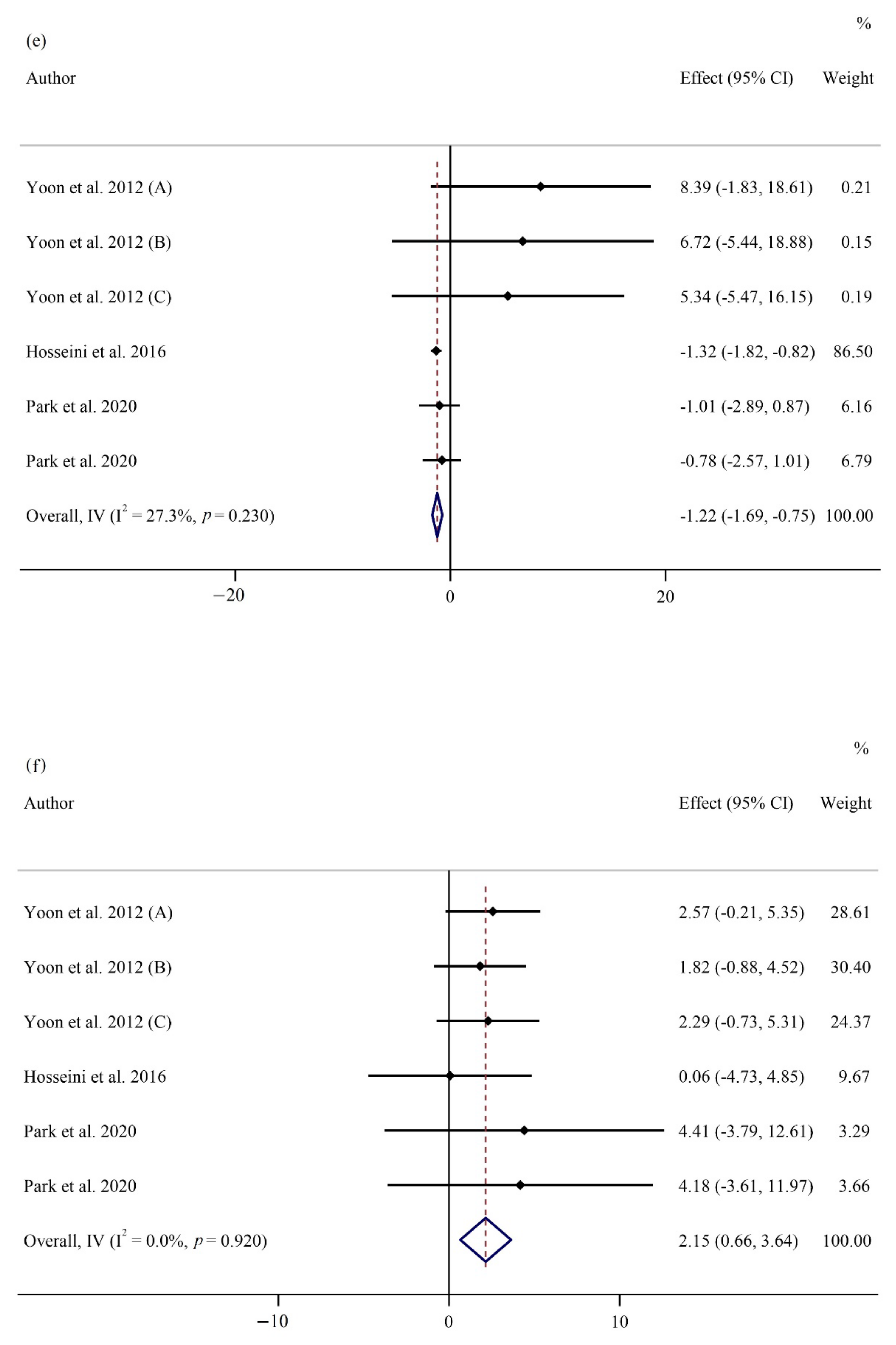
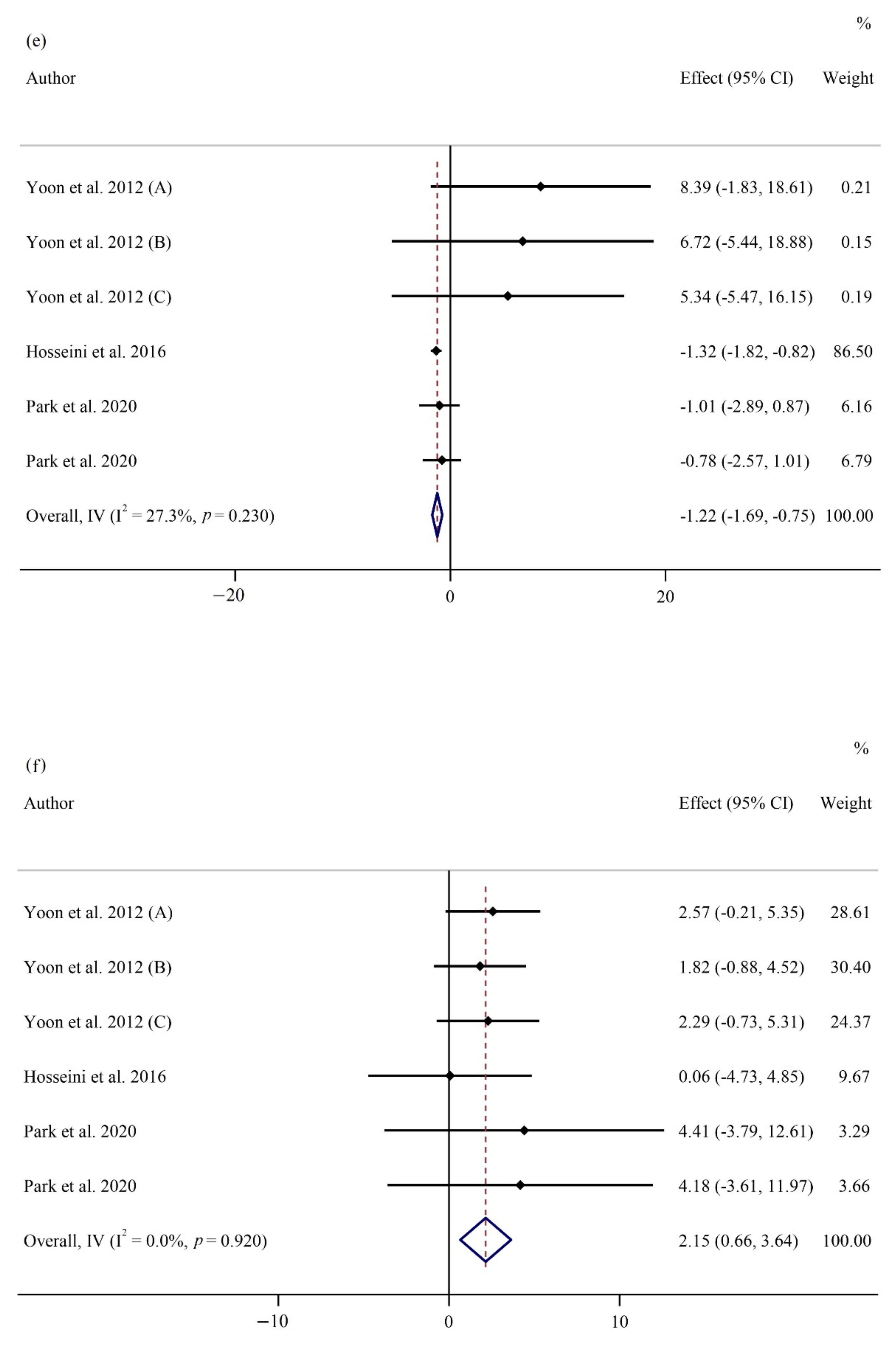
| Overall effect | 6 | −1.22 (−1.68, −0.75) | <0.001 | 0.230 | 27.3% |
| Subgroup analyses of ginseng supplementation on TNF-α | |||||
| Overall effect | 6 | 2.15 (0.66, 3.63) | 0.005 | 0.920 | 0.0% |
| Subgroup analyses of ginseng supplementation on adiponectin | |||||
| Overall effect | 3 | −0.27 (−1.41, 0.86) | 0.639 | 0.906 | 0.0% |
| Subgroup analyses of ginseng supplementation on leptin | |||||
| Overall effect | 3 | −0.67 (−2.01, 0.65) | 0.320 | 0.847 | 0.0% |
| Subgroup analyses of ginseng supplementation on ALT | |||||
| Overall effect | 7 | 0.62 (−1.90, 3.15) | 0.630 | 0.085 | 46.0% |
| Subgroup analyses of ginseng supplementation on AST | |||||
| Overall effect | 5 | −0.28 (−1.77, 1.19) | 0.704 | 0.272 | 22.3% |
| Subgroup analyses of ginseng supplementation on GGT | |||||
| Overall effect | 3 | 2.03 (−6.22, 10.28) | 0.630 | 0.285 | 20.3% |
| Biomarkers | Regression | Dose-Response | ||||||
|---|---|---|---|---|---|---|---|---|
| Dose | Duration | Dose | Duration | |||||
| Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | |
| FPG | 0.0806575 | 0.374 | 0.2427767 | 0.124 | −1.755688 | 0.180 | −13.6688 | 0.161 |
| OGTT | 0.075122 | 0.708 | 0.1427608 | 0.482 | 13.68284 | 0.356 | 7.016837 | 0.720 |
| HbA1c | 1.311766 | 0.588 | −6.340935 | 0.382 | 0.129185 | 0.499 | −0.5456897 | 0.468 |
| Insulin | −0.1057443 | 0.699 | 0.1184111 | 0.853 | 2.118513 | 0.204 | −1.431268 | 0.570 |
| HOMA-IR | 0.4107144 | 0.420 | 2.930911 | 0.132 | −0.2646978 | 0.028 | 7.189052 | 0.042 |
| TG | 0.0786231 | 0.623 | −0.0360899 | 0.829 | 0.3341626 | 0.750 | 38.14975 | 0.143 |
| TC | −0.1032192 | 0.480 | 0.4331759 | 0.081 | −2.04802 | 0.262 | 5.883329 | 0.606 |
| LDL-C | −0.2034715 | 0.160 | 0.0470388 | 0.861 | −2.107334 | 0.111 | −16.61938 | 0.048 |
| HDL-C | −0.2342807 | 0.020 | 0.021285 | 0.970 | −0.319954 | 0.009 | −3.99029 | 0.100 |
| SBP | 0.0292994 | 0.832 | 0.3400391 | 0.251 | −11.49681 | 0.132 | −17.22758 | 0.233 |
| DBP | −0.2617145 | 0.317 | 0.8746015 | 0.226 | −1.137181 | 0.077 | −8.580873 | 0.157 |
| Outcomes | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Number of Intervention/Control | Quality of Evidence |
|---|---|---|---|---|---|---|---|
| BW | No serious limitation | No serious limitation | No serious limitation | Serious limitation 2 | No serious limitation | 480 (244/236) | ⊕⊕⊕◯ 4 Moderate |
| BMI | No serious limitation | No serious limitation | No serious limitation | Serious limitation 2 | No serious limitation | 648 (344/304) | ⊕⊕⊕◯ Moderate |
| WC | No serious limitation | No serious limitation | No serious limitation | Serious limitation 2 | No serious limitation | 72 (54/18) | ⊕⊕⊕◯ Moderate |
| FPG | No serious limitation | Serious limitation 1 | No serious limitation | No serious limitation | Serious limitation 3 | 1077 (567/510) | ⊕⊕◯◯ Low |
| OGTT | No serious limitation | Serious limitation 1 | No serious limitation | Serious limitation 2 | No serious limitation | 347 (190/157) | ⊕⊕◯◯ Low |
| HbA1c | No serious limitation | Serious limitation 1 | No serious limitation | Serious limitation 2 | No serious limitation | 914 (478/436) | ⊕⊕◯◯ Low |
| Insulin | No serious limitation | Serious limitation 1 | No serious limitation | Serious limitation 2 | No serious limitation | 570 (306/264) | ⊕⊕◯◯ Low |
| HOMA | No serious limitation | Serious limitation 1 | No serious limitation | No serious limitation | No serious limitation | 390 (211/179) | ⊕⊕⊕◯ Moderate |
| TG | No serious limitation | Serious limitation 1 | No serious limitation | Serious limitation 2 | No serious limitation | 814 (430/ 384) | ⊕⊕◯◯ Low |
| TC | No serious limitation | Serious limitation 1 | No serious limitation | No serious limitation | No serious limitation | 838 (442/ 396) | ⊕⊕⊕◯ Moderate |
| LDL-C | No serious limitation | Serious limitation 1 | No serious limitation | Serious limitation 2 | No serious limitation | 838 (442/ 396) | ⊕⊕◯◯ Low |
| HDL-C | No serious limitation | Serious limitation 1 | No serious limitation | Serious limitation 2 | No serious limitation | 838 (442/ 396) | ⊕⊕◯◯ Low |
| SBP | No serious limitation | Serious limitation 1 | No serious limitation | Serious limitation 2 | No serious limitation | 420 (227/193) | ⊕⊕◯◯ Low |
| DBP | No serious limitation | Serious limitation 1 | No serious limitation | Serious limitation 2 | No serious limitation | 420 (227/193) | ⊕⊕◯◯ Low |
| HR | No serious limitation | No serious limitation | No serious limitation | No serious limitation | No serious limitation | 224 (116/108) | ⊕⊕⊕⊕ High |
| CRP | No serious limitation | Serious limitation 1 | No serious limitation | Serious limitation 2 | No serious limitation | 232 (132/100) | ⊕⊕◯◯ Low |
| IL6 | No serious limitation | No serious limitation | No serious limitation | No serious limitation | Serious limitation 3 | 232 (132/100) | ⊕⊕⊕◯ Moderate |
| TNF-α | No serious limitation | No serious limitation | No serious limitation | No serious limitation | No serious limitation | 232 (132/100) | ⊕⊕⊕⊕ High |
| Adiponectin | No serious limitation | No serious limitation | No serious limitation | Serious limitation 2 | No serious limitation | 72 (54/18) | ⊕⊕⊕◯ Moderate |
| Leptin | No serious limitation | No serious limitation | No serious limitation | Serious limitation 2 | No serious limitation | 72 (54/18) | ⊕⊕⊕◯ Moderate |
| ALT | No serious limitation | No serious limitation | No serious limitation | Serious limitation 2 | No serious limitation | 269 (153/116) | ⊕⊕⊕◯ Moderate |
| AST | No serious limitation | No serious limitation | No serious limitation | Serious limitation 2 | No serious limitation | 165 (98/67) | ⊕⊕⊕◯ Moderate |
| GGT | No serious limitation | No serious limitation | No serious limitation | Serious limitation 2 | No serious limitation | 72 (54/18) | ⊕⊕⊕◯ Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naseri, K.; Saadati, S.; Sadeghi, A.; Asbaghi, O.; Ghaemi, F.; Zafarani, F.; Li, H.-B.; Gan, R.-Y. The Efficacy of Ginseng (Panax) on Human Prediabetes and Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 2401. https://doi.org/10.3390/nu14122401
Naseri K, Saadati S, Sadeghi A, Asbaghi O, Ghaemi F, Zafarani F, Li H-B, Gan R-Y. The Efficacy of Ginseng (Panax) on Human Prediabetes and Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients. 2022; 14(12):2401. https://doi.org/10.3390/nu14122401
Chicago/Turabian StyleNaseri, Kaveh, Saeede Saadati, Amir Sadeghi, Omid Asbaghi, Fatemeh Ghaemi, Fatemeh Zafarani, Hua-Bin Li, and Ren-You Gan. 2022. "The Efficacy of Ginseng (Panax) on Human Prediabetes and Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis" Nutrients 14, no. 12: 2401. https://doi.org/10.3390/nu14122401
APA StyleNaseri, K., Saadati, S., Sadeghi, A., Asbaghi, O., Ghaemi, F., Zafarani, F., Li, H.-B., & Gan, R.-Y. (2022). The Efficacy of Ginseng (Panax) on Human Prediabetes and Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients, 14(12), 2401. https://doi.org/10.3390/nu14122401