Synergistic Effects of the Geriatric Nutritional Risk Index and the Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Calculation of Nutritional Indices and Patient Grouping
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Patients
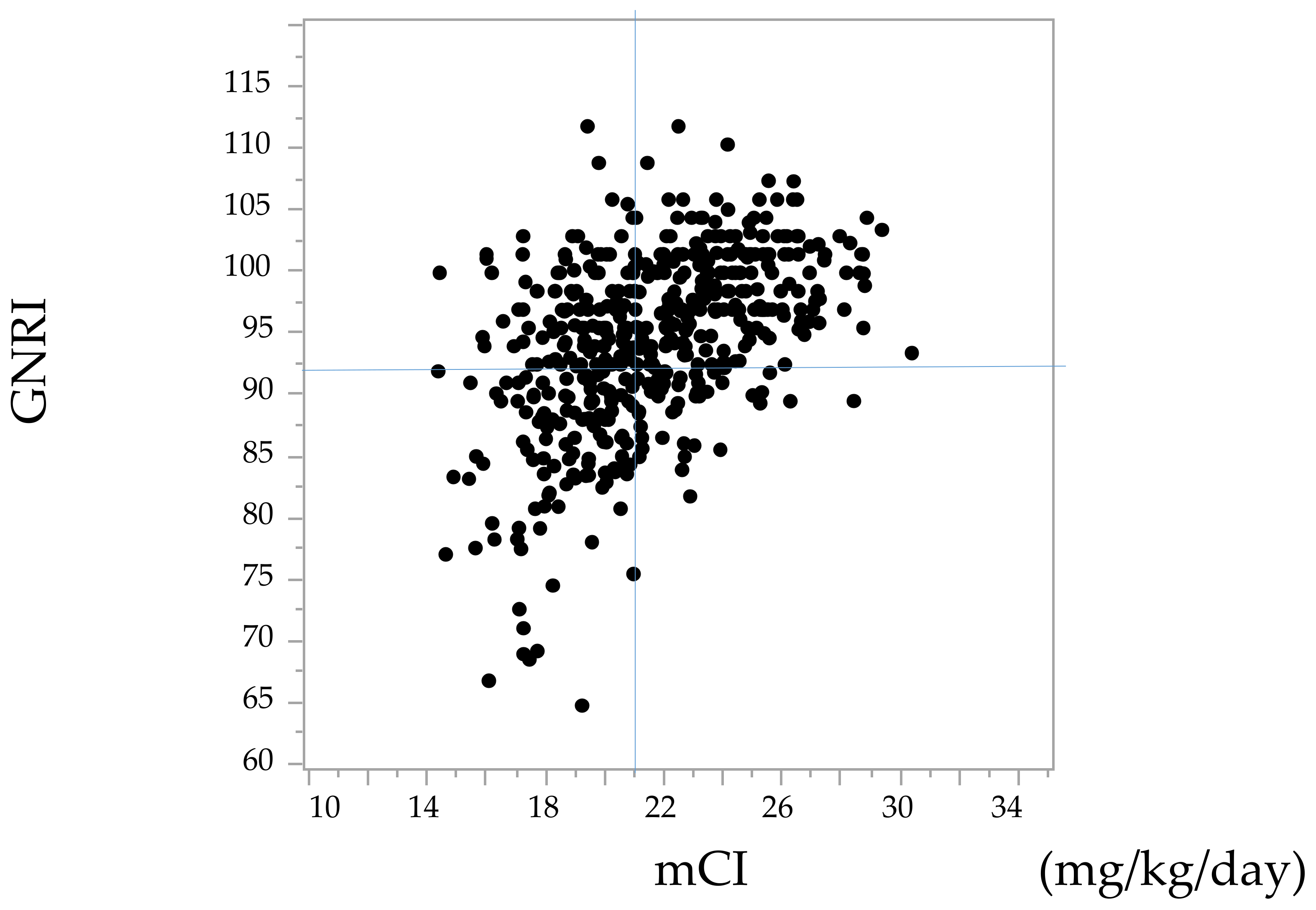
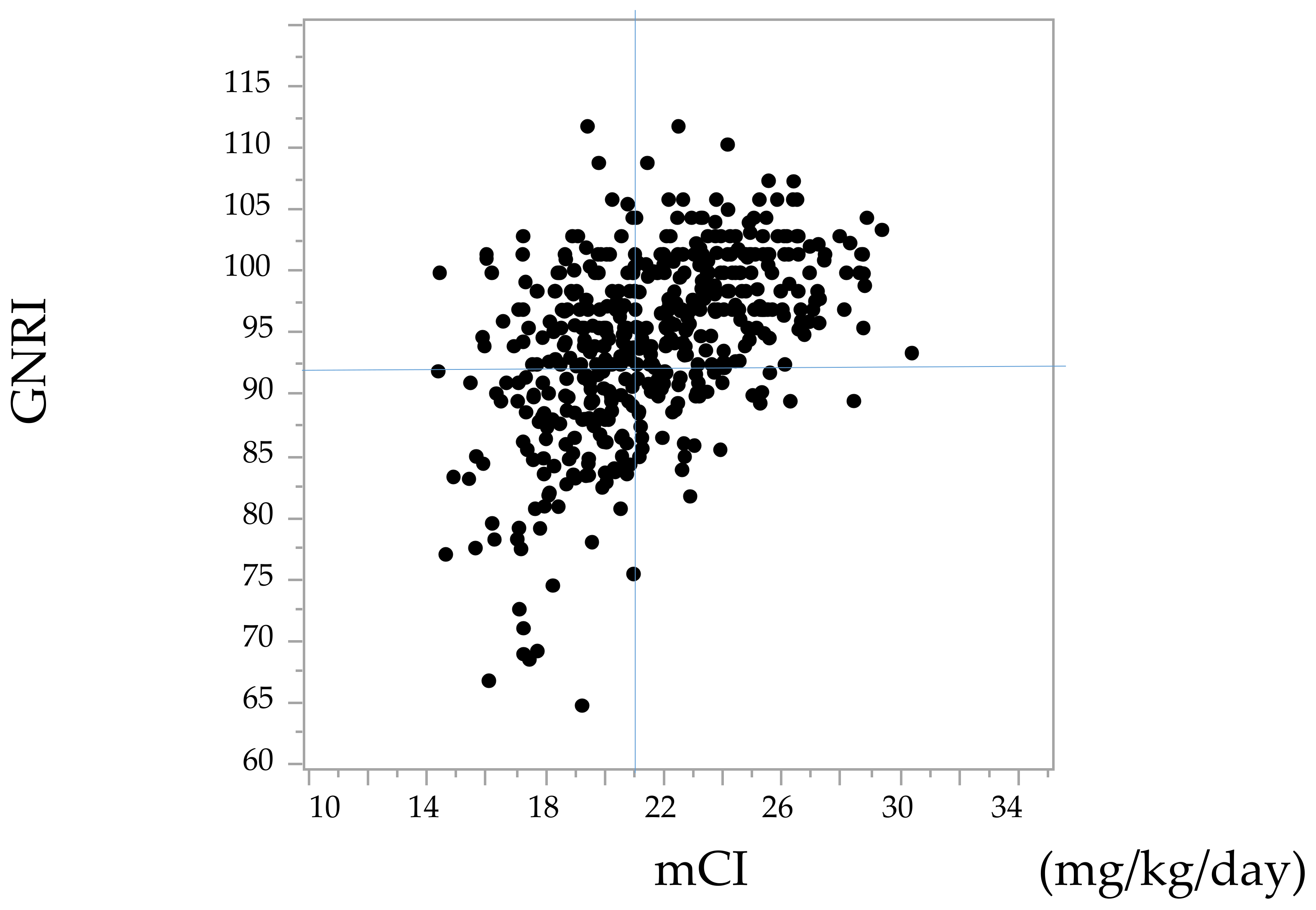
3.2. Correlation between the GNRI and the mCI
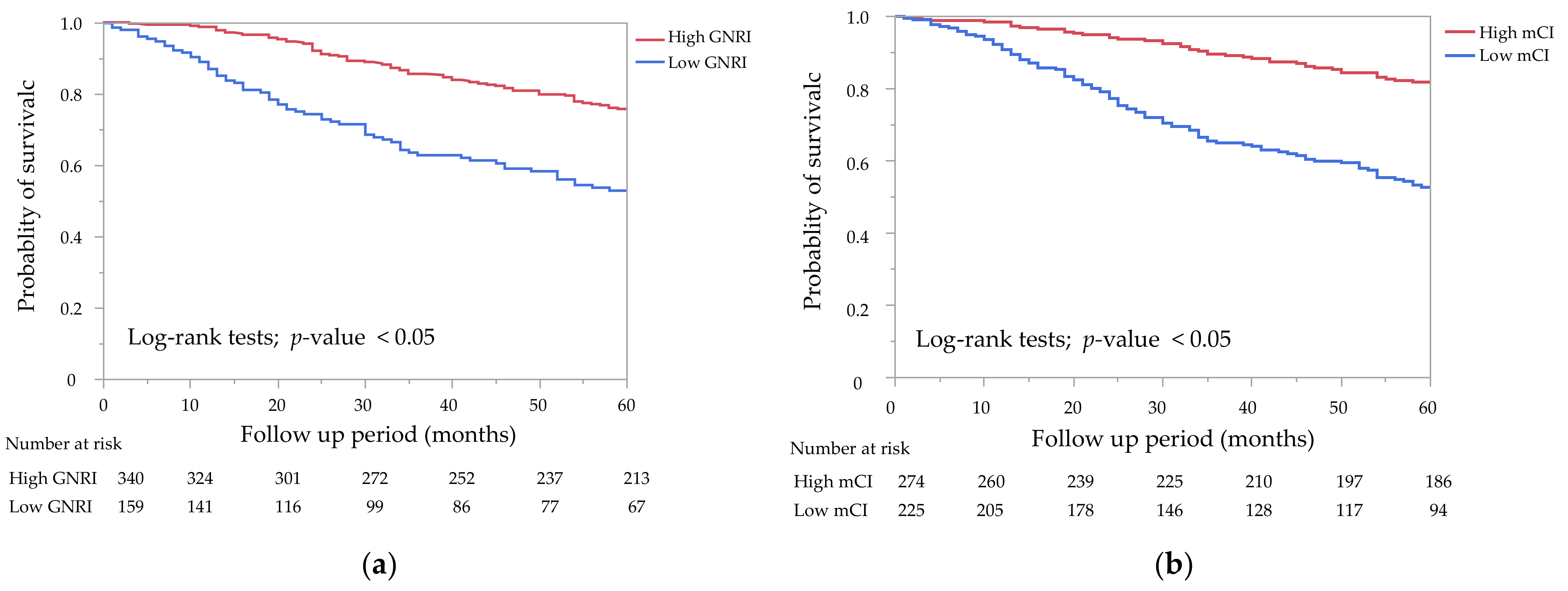
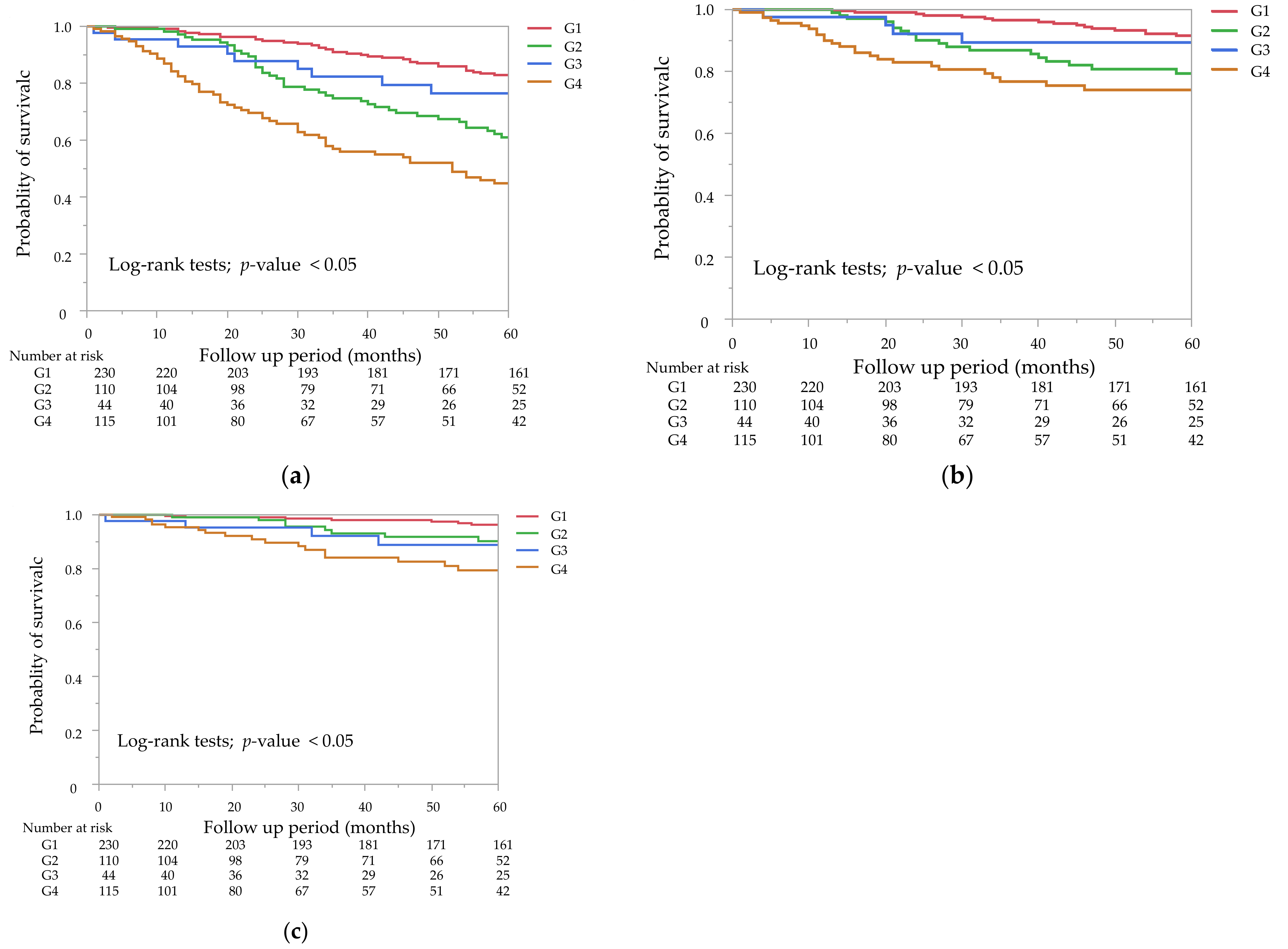
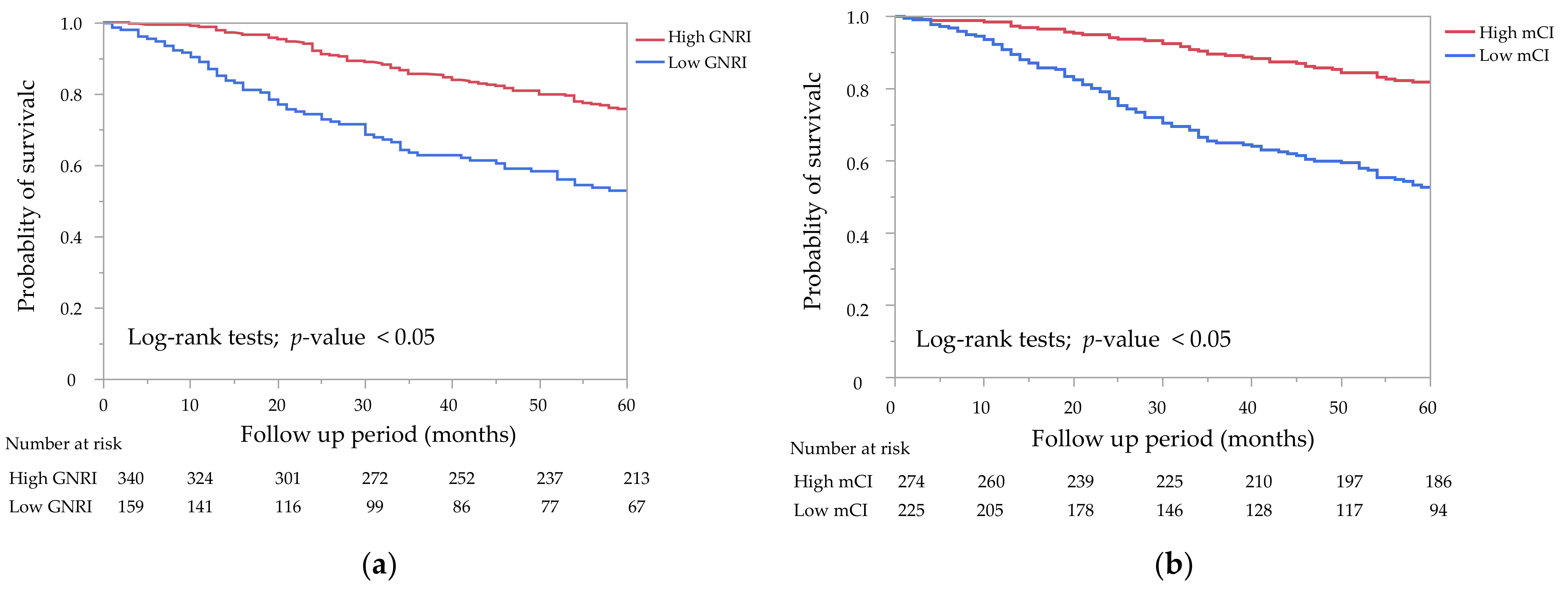
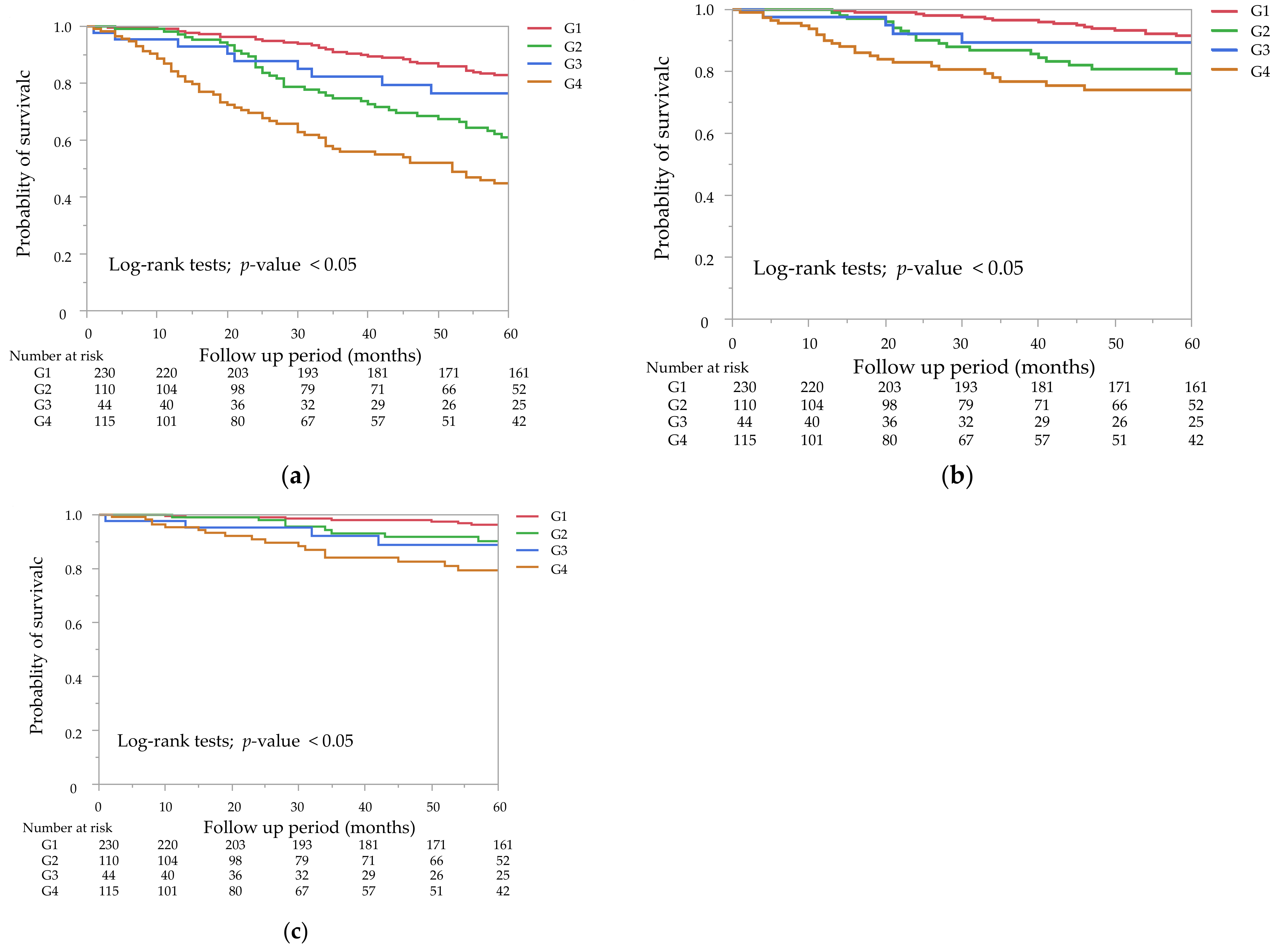
3.3. Clinical Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pifer, T.; McCullough, K.; Port, F.; Goodkin, D.; Maroni, B.; Held, P.; Young, E. Mortality risk in hemodialysis patients and changes in nutritional indicators: DOPPS. Kidney Int. 2002, 62, 2238–2245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalantar-Zadeh, K.; Kopple, J.; Block, G.; Humphreys, M. A malnutrition-inflammation score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 1251–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beberashvili, I.; Azar, A.; Sinuani, I.; Kadoshi, H.; Shapiro, G.; Feldman, L.; Averbukh, Z.; Weissgarten, J. Comparison analysis of nutritional scores for serial monitoring of nutritional status in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2013, 8, 443–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.-P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Yamada, K.; Furuya, R.; Takita, T.; Maruyama, Y.; Yamaguchi, Y.; Ohkawa, S.; Kumagai, H. Simplified nutritional screening tools for patients on maintenance hemodialysis. Am. J. Clin. Nutr. 2008, 87, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Qin, X.; Li, Y.; Yang, Y.; Yang, S.; Lu, Y.; Zhao, Y.; He, Y.; Li, Y.; Lei, Z.; et al. Comparison of three nutritional screening tools for predicting mortality in maintenance hemodialysis patients. Nutrition 2019, 67, 110532. [Google Scholar] [CrossRef]
- Canaud, B.; Garred, L.; Argiles, A.; Flavier, J.; Bouloux, C.; Mion, C. Creatinine kinetic modelling: A simple and reliable tool for the assessment of protein nutritional status in haemodialysis patients. Nephrol. Dial. Transplant. 1995, 10, 1405–1410. [Google Scholar]
- Canaud, B.; Vallée, G.A.; Molinari, N.; Chenine, L.; Leray-Moragues, H.; Rodriguez, A.; Chalabi, L.; Morena, M.; Cristol, J.-P. Creatinine index as a surrogate of lean body mass derived from urea Kt/V, pre-dialysis serum levels and anthropometric characteristics of haemodialysis patients. PLoS ONE 2014, 9, e93286. [Google Scholar] [CrossRef]
- Xiong, J.; Wang, M.; Zhang, Y.; Nie, L.; He, T.; Wang, Y.; Huang, Y.; Feng, B.; Zhang, J.; Zhao, J. Association of Geriatric Nutritional Risk Index with Mortality in Hemodialysis Patients: A Meta-Analysis of Cohort Studies. Kidney Blood Press. Res. 2018, 43, 1878–1889. [Google Scholar] [CrossRef]
- Arase, H.; Yamada, S.; Yotsueda, R.; Taniguchi, M.; Yoshida, H.; Tokumoto, M.; Nakano, T.; Tsuruya, K.; Kitazono, T. Modified creatinine index and risk for cardiovascular events and all-cause mortality in patients undergoing hemodialysis: The Q-Cohort study. Atherosclerosis 2018, 275, 115–123. [Google Scholar] [CrossRef]
- Huang, C.; Lee, S.; Yang, C.; Hung, S.; Chiang, C.; Huang, J.; Hung, K. A Simpler Creatinine Index Can Predict Long-Term Survival in Chinese Hemodialysis Patients. PLoS ONE 2016, 11, e0165164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arase, H.; Yamada, S.; Hiyamuta, H.; Taniguchi, M.; Tokumoto, M.; Tsuruya, K.; Nakano, T.; Kitazono, T. Modified creatinine index and risk for long-term infection-related mortality in hemodialysis patients: Ten-year outcomes of the Q-Cohort Study. Sci. Rep. 2020, 10, 1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, S.; Yamamoto, S.; Fukuma, S.; Nakano, T.; Tsuruya, K.; Inaba, M. Geriatric Nutritional Risk Index (GNRI) and Creatinine Index Equally Predict the Risk of Mortality in Hemodialysis Patients: J-DOPPS. Sci. Rep. 2020, 10, 5756. [Google Scholar] [CrossRef] [Green Version]
- Yajima, T.; Yajima, K.; Arao, M. Combined Evaluation of Geriatric Nutritional Risk Index and Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis. Nutrients 2022, 14, 752. [Google Scholar] [CrossRef] [PubMed]
- Fujioka, H.; Koike, T.; Imamura, T.; Tomoda, F.; Kakeshita, K.; Yamazaki, H.; Kinugawa, K. Impact of Geriatric Nutritional Risk Index and Modified Creatinine Index Combination on Mortality in Hemodialysis Patients. Nutrients 2022, 14, 801. [Google Scholar] [CrossRef]
- Satoh, A.; Doi, S.; Naito, T.; Nakashima, A.; Masaki, T. N-terminal pro brain natriuretic peptide predicts both all-cause and cardiovascular disease mortality in Japanese hemodialysis patients. Clin. Exp. Nephrol. 2021, 25, 1142–1150. [Google Scholar] [CrossRef]
- Takahashi, H.; Ito, Y.; Ishii, H.; Aoyama, T.; Kamoi, D.; Kasuga, H.; Yasuda, K.; Maruyama, S.; Matsuo, S.; Murohara, T.; et al. Geriatric nutritional risk index accurately predicts cardiovascular mortality in incident hemodialysis patients. J. Cardiol. 2014, 64, 32–36. [Google Scholar] [CrossRef] [Green Version]
- Matsukuma, Y.; Tanaka, S.; Taniguchi, M.; Nakano, T.; Masutani, K.; Hirakata, H.; Kitazono, T.; Tsuruya, K. Association of geriatric nutritional risk index with infection-related mortality in patients undergoing hemodialysis: The Q-Cohort Study. Clin. Nutr. 2019, 38, 279–287. [Google Scholar] [CrossRef]
- Hwang, W.; Cho, M.; Oh, J.; Lee, J.; Jeong, J.; Shin, G.; Kim, H.; Park, I. Comparison of creatinine index and geriatric nutritional risk index for nutritional evaluation of patients with hemodialysis. Hemodial. Int. 2018, 22, 507–514. [Google Scholar] [CrossRef]
- Suzuki, Y.; Matsuzawa, R.; Hoshi, K.; Koh, Y.; Yamamoto, S.; Harada, M.; Watanabe, T.; Imamura, K.; Kamiya, K.; Yoshida, A.; et al. Comparative Analysis of Simplified, Objective Nutrition-Associated Markers in Patients Undergoing Hemodialysis. J. Ren. Nutr. 2021, 21, S1051–S2276. [Google Scholar] [CrossRef]
- Panichi, V.; Cupisti, A.; Rosati, A.; Di Giorgio, A.; Scatena, A.; Menconi, O.; Bozzoli, L.; Bottai, A. Geriatric nutritional risk index is a strong predictor of mortality in hemodialysis patients: Data from the Riscavid cohort. J. Nephrol. 2014, 27, 193–201. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Total (N = 499) | G1 (N = 230) | G2 (N = 110) | G3 (N = 44) | G4 (N = 115) | p-Value | |
|---|---|---|---|---|---|---|
| Age, years | 65 (56–74) | 58 (49–65) | 72 (63–77) * | 64 (58–68) * | 73 (68–81) * | <0.05 |
| Male sex, n (%) | 334 (67) | 189 (82) | 58 (53) | 34 (77) | 53 (46) | <0.05 |
| Dialysis vintage, months | 64 (29–136) | 91 (45–154) | 38 (16–82) * | 93 (45–194) | 46 (18–106) * | <0.05 |
| Presence of diabetes, n (%) | 185 (37) | 77 (33) | 53 (48) | 9 (20) | 46 (40) | <0.05 |
| History of CVD, n (%) | 218 (44) | 84 (37) | 58 (53) | 17 (39) | 59 (51) | <0.05 |
| Never smokers, n (%) | 253 (51) | 109 (47) | 61 (55) | 18 (41) | 65 (57) | 0.15 |
| Presence of RKF, n (%) | 155 (31) | 58 (25) | 46 (42) | 7 (16) | 44 (38) | <0.05 |
| Type of vascular access—AVF, n (%) | 464 (93) | 218 (95) | 102 (93) | 43 (98) | 101 (88) | 0.06 |
| BMI, kg/m2 | 22 (19–24) | 23 (21–25) | 23 (21–24) | 19 (18–21) * | 19 (18–21) * | <0.05 |
| Systolic blood pressure, mmHg | 155 (139–168) | 156 (140–167) | 159 (141–172) | 150 (136–171) | 152 (136–164) | 0.07 |
| Single-pool Kt/V | 1.38 (1.25–1.53) | 1.37 (1.25–1.49) | 1.38 (1.23–1.54) | 1.39 (1.31–1.54) | 1.38 (1.24–1.57) | 0.61 |
| Use of Antihypertensive drugs, n (%) | 370 (74) | 176 (77) | 82 (75) | 31 (70) | 81 (70) | 0.61 |
| Use of RAS inhibitors, n (%) | 302 (61) | 148 (65) | 64 (58) | 28 (64) | 62 (54) | 0.25 |
| Use of ESAs, n (%) | 445 (89) | 200 (87) | 101 (92) | 38 (86) | 106 (92) | 0.32 |
| Use of P binders, n (%) | 407 (82) | 214 (93) | 75 (68) | 37 84) | 81 (70) | <0.05 |
| Use of VDRAs, n (%) | 257 (52) | 123 (53) | 56 (51) | 21 (48) | 57 (50) | 0.85 |
| Use of statins, n (%) | 59 (12) | 21 (9) | 22 (20) | 3 (7) | 13 (11) | <0.05 |
| Hemoglobin, g/dL | 11.0 (10.3–11.8) | 11.0 (10.3–11.9) | 11.1 (10.5–11.9) | 11.2 (10.5–11.8) | 10.8 (9.9–11.6) * | <0.05 |
| Serum albumin, g/dL | 3.7 (3.5–4.0) | 4.0 (3.7–4.1) | 3.8 (3.6–4.0) * | 3.5 (3.3–3.7) * | 3.3 (3.1–3.6) * | <0.05 |
| Serum urea nitrogen, mg/dL | 65 (56–74) | 69 (62–78) | 59 (51–68) * | 69 (57–79) | 59 (47–70) * | <0.05 |
| Serum creatinine, mg/dL | 10.8 (8.7–13.0) | 13.0 (11.8–14.5) | 8.6 (7.5–9.7) * | 12.1 (11.2–12.7) * | 8.2 (6.7–9.7) * | <0.05 |
| Serum total cholesterol, mg/dL | 153 (132–178) | 152 (130–174) | 164 (139–183) * | 145 (123–174) | 151 (133–181) | <0.05 |
| Corrected serum calcium, mg/dL | 9.4 (9.0–10.0) | 9.5 (9.0–9.9) | 9.2 (8.9–9.7) * | 9.7 (9.0–10.1) | 9.4 (9.0–10.2) | <0.05 |
| Serum phosphate, mg/dL | 5.2 (4.5–6.0) | 5.5 (4.6–6.1) | 5.1 (4.4–5.9) | 5.2 (4.4–6.1) | 4.7 (4.0–5.7) * | <0.05 |
| Serum intact PTH, pg/mL | 113 (48–191) | 134 (65–217) | 94 (51–182) * | 112 (30–169) | 86 (28–168) * | <0.05 |
| Serum C-reactive protein, mg/dL | 0.09 (0.03–0.29) | 0.06 (0.03–0.18) | 0.10 (0.04–0.25) | 0.12 (0.05–0.40) * | 0.19 (0.05–0.78) * | <0.05 |
| GNRI | 95 (90–100) | 98 (96–101) | 97 (94–100) * | 90 (86–91) * | 86 (83–89) * | <0.05 |
| mCI, mg/kg/day | 21 (19–24) | 24 (22–26) | 19 (18–20) * | 23 (22–23) * | 19 (18–20) * | <0.05 |
| Unadjusted Model | Multivariable Model 1 | Multivariable Model 2 | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| GNRI | ||||||
| High GNRI | 1.00 (reference) | - | 1.00 (reference) | - | 1.00 (reference) | - |
| Low GNRI | 2.48 (1.78–3.45) | <0.05 | 1.48 (1.02–2.15) | <0.05 | 1.51 (1.03–2.20) | <0.05 |
| mCI | ||||||
| High mCI | 1.00 (reference) | - | 1.00 (reference) | - | 1.00 (reference) | - |
| Low mCI | 3.28 (2.30–4.69) | <0.05 | 1.67 (1.09–2.58) | <0.05 | 1.82 (1.17–2.82) | <0.05 |
| Unadjusted Model | Multivariable Model 1 | Multivariable Model 2 | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95%CI) | p-Value | |
| All-cause mortality | ||||||
| G1 | 1.00 (reference) | - | 1.00 (reference) | - | 1.00 (reference) | - |
| G2 | 2.61 (1.65–4.12) | <0.05 | 1.39 (0.83–2.31) | 0.21 | 1.50 (0.89–2.51) | 0.13 |
| G3 | 1.55 (0.75–3.23) | 0.24 | 1.02 (0.48–2.16) | 0.96 | 1.01 (0.47–2.15) | 0.98 |
| G4 | 4.65 (3.06–7.07) | <0.05 | 2.10 (1.25–3.52) | <0.05 | 2.31 (1.36–3.89) | <0.05 |
| Cardiovascular mortality | ||||||
| G1 | 1.00 (reference) | - | 1.00 (reference) | - | 1.00 (reference) | - |
| G2 | 2.74 (1.41–5.32) | <0.05 | 1.45 (0.68–3.02) | 0.33 | 1.62 (0.76–3.46) | 0.21 |
| G3 | 1.49 (0.50–4.47) | 0.47 | 1.00 (0.33–3.80) | 1.00 | 1.00 (0.32–3.07) | 0.99 |
| G4 | 4.20 (2.24–7.88) | <0.05 | 1.83 (0.85–3.98) | 0.12 | 2.12 (0.96–4.68) | 0.06 |
| Infection-related mortality | ||||||
| G1 | 1.00 (reference) | - | 1.00 (reference) | - | 1.00 (reference) | - |
| G2 | 2.69 (0.97–7.41) | 0.06 | 1.10 (0.35–3.41) | 0.87 | 1.23 (0.39–3.89) | 0.72 |
| G3 | 3.46 (1.01–11.81) | 0.05 | 2.07 (0.57–7.52) | 0.27 | 2.00 (0.55–7.30) | 0.29 |
| G4 | 6.67 (2.76–16.11) | <0.05 | 2.67 (0.91–7.77) | 0.77 | 2.95 (1.00–8.70) | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naito, T.; Doi, T.; Morii, K.; Usui, K.; Arita, M.; Yamashita, K.; Shigemoto, K.; Nishizawa, Y.; Mizuiri, S.; Sasaki, K.; et al. Synergistic Effects of the Geriatric Nutritional Risk Index and the Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis. Nutrients 2022, 14, 2398. https://doi.org/10.3390/nu14122398
Naito T, Doi T, Morii K, Usui K, Arita M, Yamashita K, Shigemoto K, Nishizawa Y, Mizuiri S, Sasaki K, et al. Synergistic Effects of the Geriatric Nutritional Risk Index and the Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis. Nutrients. 2022; 14(12):2398. https://doi.org/10.3390/nu14122398
Chicago/Turabian StyleNaito, Takayuki, Toshiki Doi, Kenichi Morii, Koji Usui, Michiko Arita, Kazuomi Yamashita, Kenichiro Shigemoto, Yoshiko Nishizawa, Sonoo Mizuiri, Kensuke Sasaki, and et al. 2022. "Synergistic Effects of the Geriatric Nutritional Risk Index and the Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis" Nutrients 14, no. 12: 2398. https://doi.org/10.3390/nu14122398
APA StyleNaito, T., Doi, T., Morii, K., Usui, K., Arita, M., Yamashita, K., Shigemoto, K., Nishizawa, Y., Mizuiri, S., Sasaki, K., & Masaki, T. (2022). Synergistic Effects of the Geriatric Nutritional Risk Index and the Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis. Nutrients, 14(12), 2398. https://doi.org/10.3390/nu14122398