
Underreporting of Energy Intake Increases over Pregnancy: An Intensive Longitudinal Study of Women with Overweight and Obesity

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Measures
2.2.1. Demographic Characteristics
2.2.2. Weight and Physical Activity Measures
2.2.3. Psychosocial Measures
2.2.4. Self-Reported Energy Intake
2.3. Calculating Underreporting of Energy Intake
2.4. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Error in Reporting of Energy Intake
3.3. Change in Reporting Error across Pregnancy
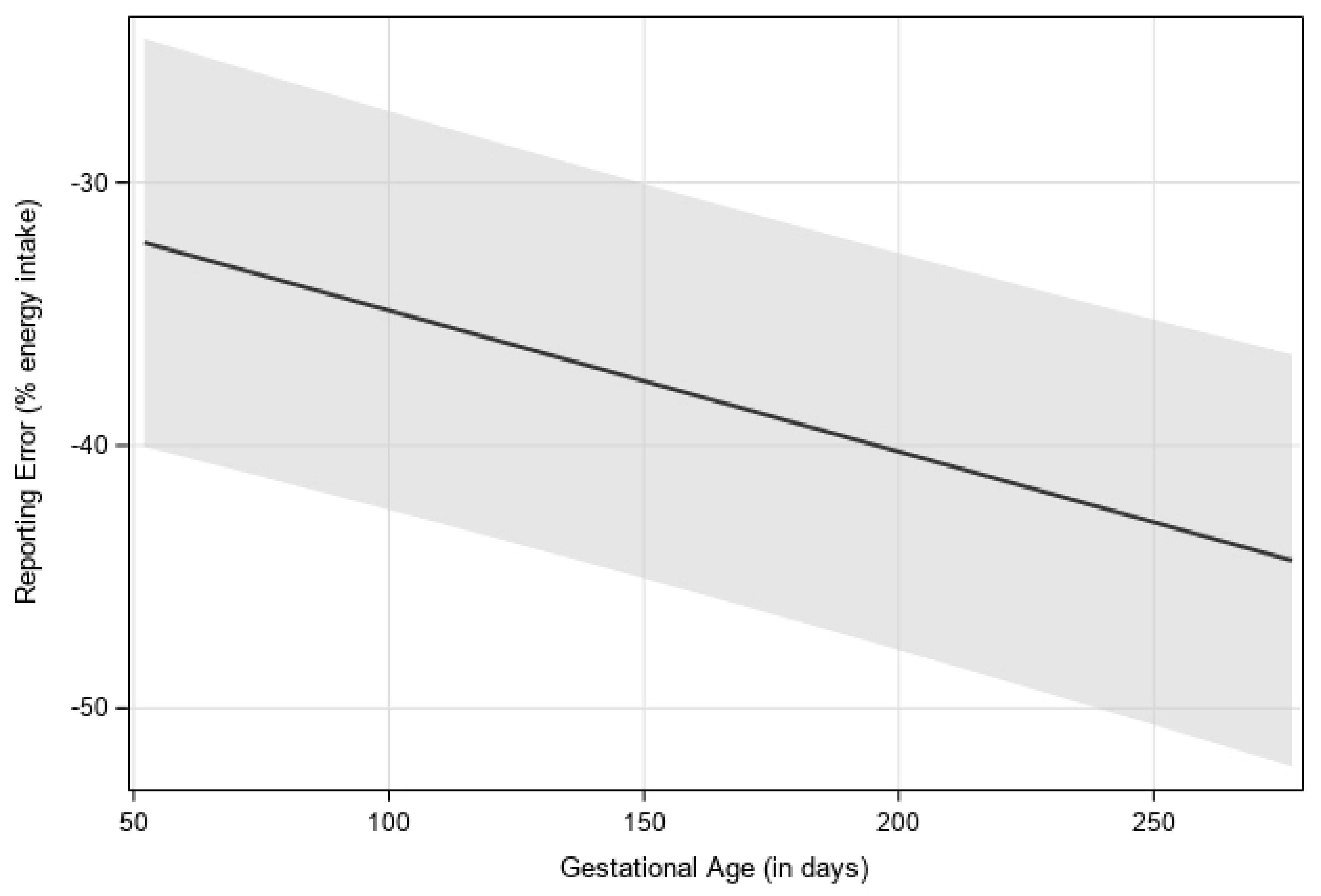
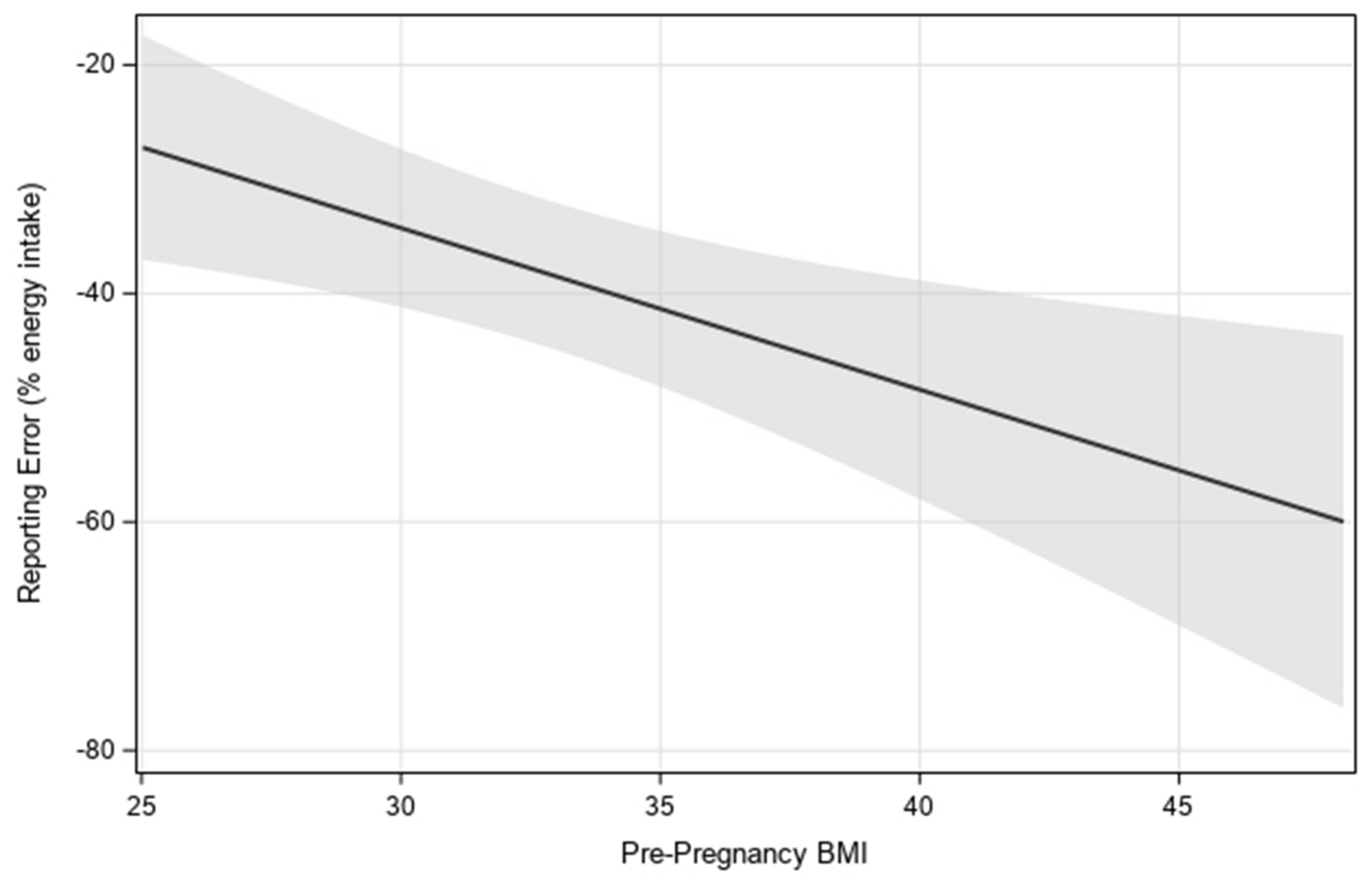
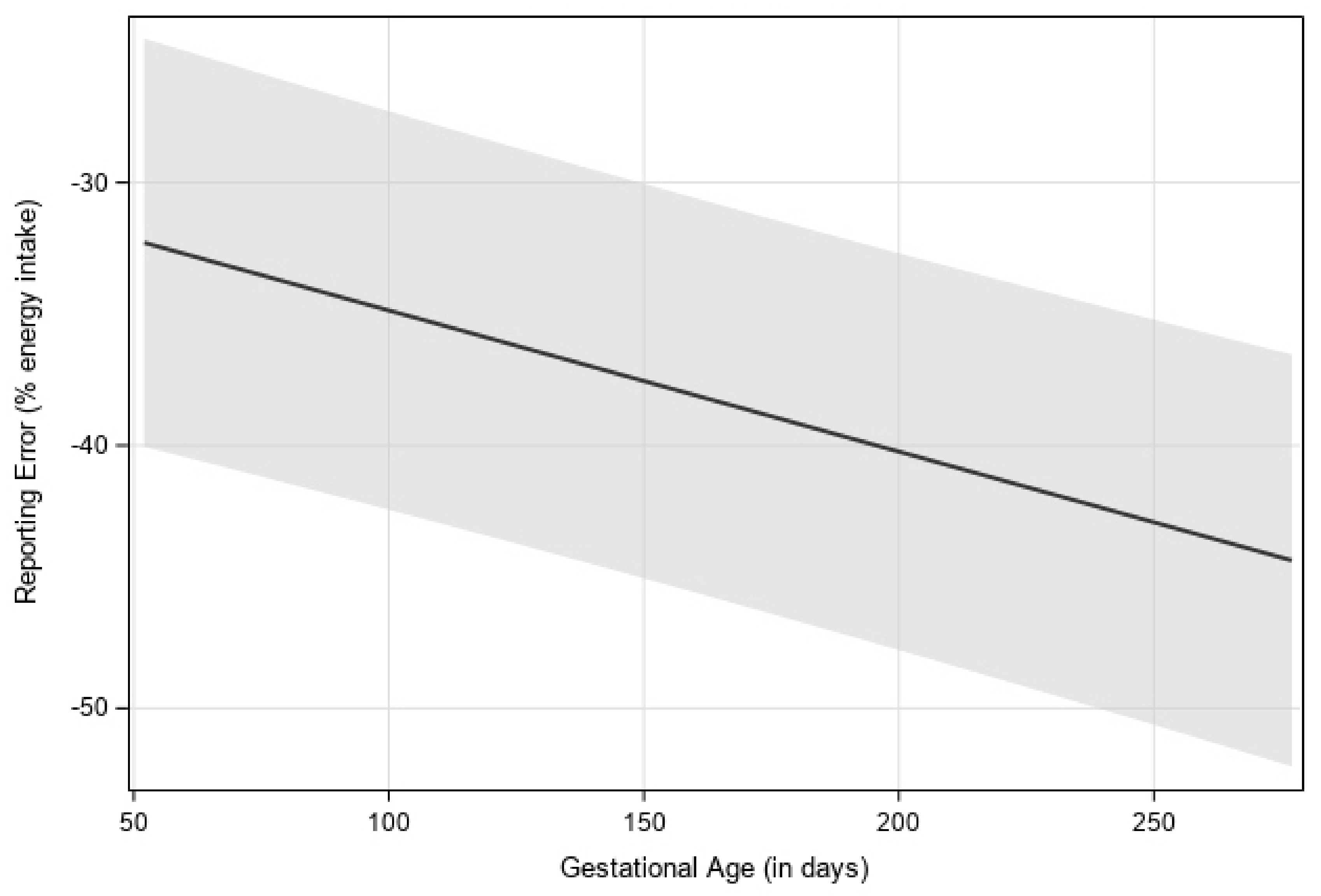
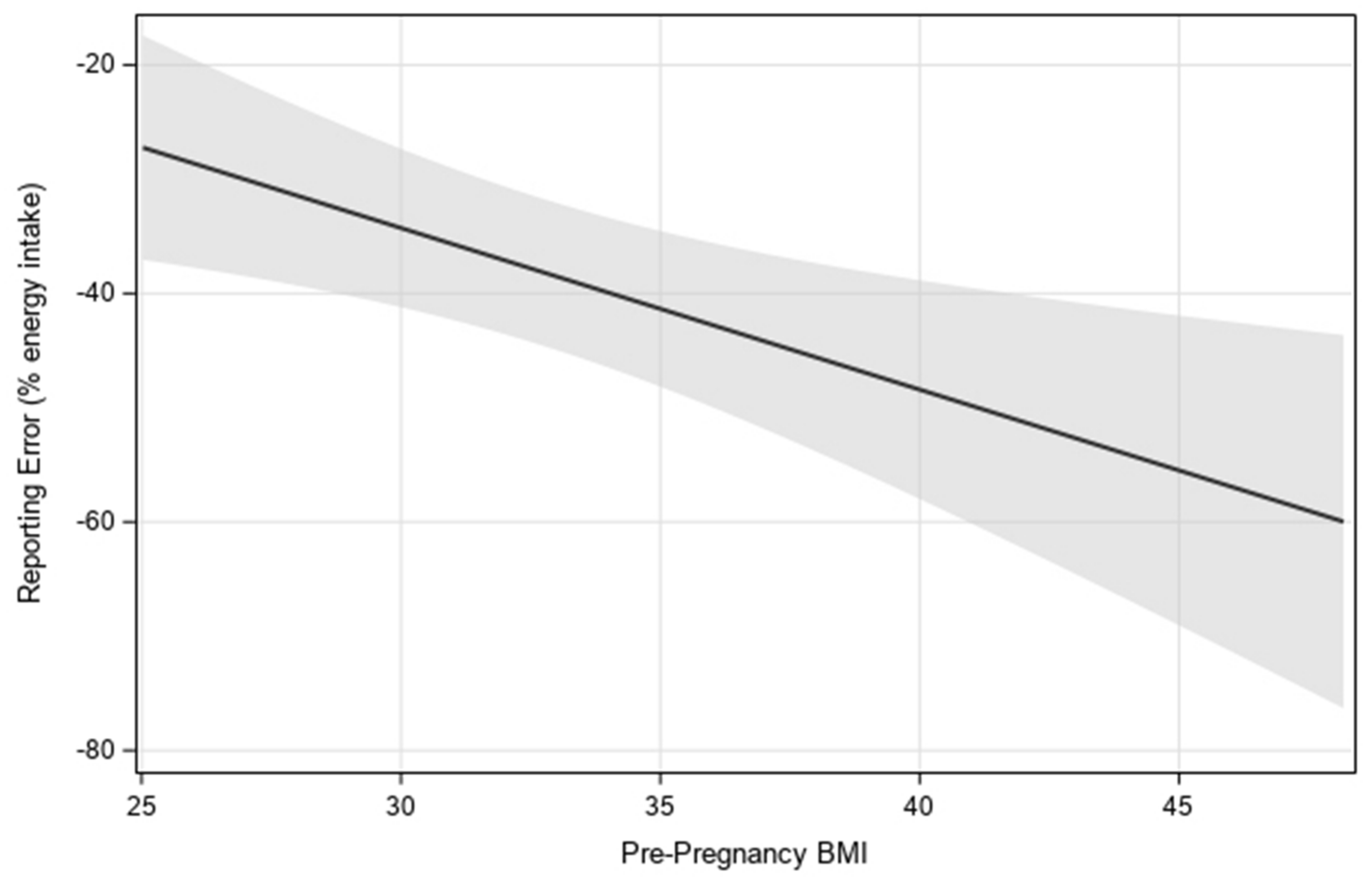
3.4. Independent Factors Associated with Reporting Error
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flegal, K.M.; Kruszon-Moran, D.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Trends in Obesity Among Adults in the United States, 2005 to 2014. JAMA 2016, 315, 2284–2291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugen, M.; Brantsaeter, A.L.; Winkvist, A.; Lissner, L.; Alexander, J.; Oftedal, B.; Magnus, P.; Meltzer, H.M. Associations of pre-pregnancy body mass index and gestational weight gain with pregnancy outcome and postpartum weight retention: A prospective observational cohort study. BMC Pregnancy Childbirth 2014, 14, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nehring, I.; Schmoll, S.; Beyerlein, A.; Hauner, H.; von Kries, R. Gestational weight gain and long-term postpartum weight retention: A meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Vesco, K.K.; Dietz, P.M.; Rizzo, J.; Stevens, V.J.; Perrin, N.A.; Bachman, D.J.; Callaghan, W.M.; Bruce, F.C.; Hornbrook, M.C. Excessive gestational weight gain and postpartum weight retention among obese women. Obstet. Gynecol. 2009, 114, 1069–1075. [Google Scholar] [CrossRef] [Green Version]
- Gunderson, E.P.; Sternfeld, B.; Wellons, M.F.; Whitmer, R.A.; Chiang, V.; Quesenberry, C.P., Jr.; Lewis, C.E.; Sidney, S. Childbearing may increase visceral adipose tissue independent of overall increase in body fat. Obesity 2008, 16, 1078–1084. [Google Scholar] [CrossRef] [Green Version]
- McDonald, S.D.; Han, Z.; Mulla, S.; Beyene, J. Overweight and obesity in mothers and risk of preterm birth and low birth weight infants: Systematic review and meta-analyses. BMJ 2010, 341, c3428. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.W.; Soh, S.E.; Tint, M.T.; Loy, S.L.; Yap, F.; Tan, K.H.; Lee, Y.S.; Shek, L.P.; Godfrey, K.M.; Gluckman, P.D.; et al. Combined analysis of gestational diabetes and maternal weight status from pre-pregnancy through post-delivery in future development of type 2 diabetes. Sci. Rep. 2021, 11, 5021. [Google Scholar] [CrossRef]
- Fu, Z.; Kelley, J.L.; Odunsi, K.; Edwards, R.P.; Moysich, K.; Modugno, F. Gestational weight gain and risk of epithelial ovarian cancer. Cancer Causes Control 2021, 32, 537–545. [Google Scholar] [CrossRef]
- Vesco, K.K.; Sharma, A.J.; Dietz, P.M.; Rizzo, J.H.; Callaghan, W.M.; England, L.; Bruce, F.C.; Bachman, D.J.; Stevens, V.J.; Hornbrook, M.C. Newborn size among obese women with weight gain outside the 2009 Institute of Medicine recommendation. Obstet. Gynecol. 2011, 117, 812–818. [Google Scholar] [CrossRef]
- Hillier, T.A.; Pedula, K.L.; Vesco, K.K.; Schmidt, M.M.; Mullen, J.A.; LeBlanc, E.S.; Pettitt, D.J. Excess gestational weight gain: Modifying fetal macrosomia risk associated with maternal glucose. Obstet. Gynecol. 2008, 112, 1007–1014. [Google Scholar] [CrossRef]
- Schack-Nielsen, L.; Michaelsen, K.F.; Gamborg, M.; Mortensen, E.L.; Sorensen, T.I. Gestational weight gain in relation to offspring body mass index and obesity from infancy through adulthood. Int. J. Obes. 2010, 34, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Bailey, R.L.; Pac, S.G.; Fulgoni, V.L.; Reidy, K.C.; Catalano, P.M. Estimation of Total Usual Dietary Intakes of Pregnant Women in the United States. JAMA Netw. Open 2019, 2, e195967. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine. Nutrition During Pregnancy: Part I Weight Gain: Part II Nutrient Supplements; The National Academies Press: Washington, DC, USA, 1990. [Google Scholar]
- Farpour-Lambert, N.J.; Ells, L.J.; Martinez de Tejada, B.; Scott, C. Obesity and Weight Gain in Pregnancy and Postpartum: An Evidence Review of Lifestyle Interventions to Inform Maternal and Child Health Policies. Front. Endocrinol. 2018, 9, 546. [Google Scholar] [CrossRef] [Green Version]
- Phelan, S.; Jankovitz, K.; Hagobian, T.; Abrams, B. Reducing excessive gestational weight gain: Lessons from the weight control literature and avenues for future research. Womens Health 2011, 7, 641–661. [Google Scholar] [CrossRef]
- Tooze, J.A.; Subar, A.F.; Thompson, F.E.; Troiano, R.; Schatzkin, A.; Kipnis, V. Psychosocial predictors of energy underreporting in a large doubly labeled water study. Am. J. Clin. Nutr. 2004, 79, 795–804. [Google Scholar] [CrossRef] [Green Version]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.; Jakubikova, M.; van’t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 hour recalls, control and adjustment methods in practice. Br. J. Nutr. 2009, 101, S73–S85. [Google Scholar] [CrossRef] [Green Version]
- Ventura, A.K.; Loken, E.; Mitchell, D.C.; Smiciklas-Wright, H.; Birch, L.L. Understanding reporting bias in the dietary recall data of 11-year-old girls. Obesity 2006, 14, 1073–1084. [Google Scholar] [CrossRef] [Green Version]
- Bathalon, G.P.; Tucker, K.L.; Hays, N.P.; Vinken, A.G.; Greenberg, A.S.; McCrory, M.A.; Roberts, S.B. Psychological measures of eating behavior and the accuracy of 3 common dietary assessment methods in healthy postmenopausal women. Am. J. Clin. Nutr. 2000, 71, 739–745. [Google Scholar] [CrossRef]
- Poppitt, S.D.; Swann, D.; Black, A.E.; Prentice, A.M. Assessment of selective under-reporting of food intake by both obese and non-obese women in a metabolic facility. Int. J. Obes. Relat. Metab. Disord. 1998, 22, 303–311. [Google Scholar] [CrossRef] [Green Version]
- Lutomski, J.E.; van den Broeck, J.; Harrington, J.; Shiely, F.; Perry, I.J. Sociodemographic, lifestyle, mental health and dietary factors associated with direction of misreporting of energy intake. Public Health Nutr. 2011, 14, 532–541. [Google Scholar] [CrossRef] [Green Version]
- Derbyshire, E.; Davies, G.J.; Costarelli, V.; Dettmar, P.W. Habitual micronutrient intake during and after pregnancy in Caucasian Londoners. Matern. Child Nutr. 2009, 5, 1–9. [Google Scholar] [CrossRef]
- Horan, M.K.; McGowan, C.A.; Gibney, E.R.; Byrne, J.; Donnelly, J.M.; McAuliffe, F.M. Maternal Nutrition and Glycaemic Index during Pregnancy Impacts on Offspring Adiposity at 6 Months of Age—Analysis from the ROLO Randomised Controlled Trial. Nutrients 2016, 8, 7. [Google Scholar] [CrossRef] [Green Version]
- Winkvist, A.; Persson, V.; Hartini, T.N. Underreporting of energy intake is less common among pregnant women in Indonesia. Public Health Nutr. 2002, 5, 523–529. [Google Scholar] [CrossRef]
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar]
- Ariens, S.; Ceulemans, E.; Adolf, J.K. Time series analysis of intensive longitudinal data in psychosomatic research: A methodological overview. J. Psychosom. Res. 2020, 137, 110191. [Google Scholar] [CrossRef]
- Moran, L.J.; McNaughton, S.A.; Sui, Z.; Cramp, C.; Deussen, A.R.; Grivell, R.M.; Dodd, J.M. The characterisation of overweight and obese women who are under reporting energy intake during pregnancy. BMC Pregnancy Childbirth 2018, 18, 204. [Google Scholar] [CrossRef]
- Thomas, D.M.; Bredlau, C.; Islam, S.; Armah, K.A.; Kunnipparampil, J.; Patel, K.; Redman, L.M.; Misra, D.; Salafia, C. Relationships between misreported energy intake and pregnancy in the pregnancy, infection and nutrition study: New insights from a dynamic energy balance model. Obes. Sci. Pract. 2016, 2, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Maurer, J.; Taren, D.L.; Teixeira, P.J.; Thomson, C.A.; Lohman, T.G.; Going, S.B.; Houtkooper, L.B. The psychosocial and behavioral characteristics related to energy misreporting. Nutr. Rev. 2006, 64, 53–66. [Google Scholar] [CrossRef] [PubMed]
- Downs, D.S.; Savage, J.S.; Rivera, D.E.; Pauley, A.M.; Leonard, K.S.; Hohman, E.E.; Guo, P.; McNitt, K.M.; Stetter, C.; Kunselman, A. Adaptive, behavioral intervention impact on weight gain, physical activity, energy intake, and motivational determinants: Results of a feasibility trial in pregnant women with overweight/obesity. J. Behav. Med. 2021, 44, 605–621. [Google Scholar] [CrossRef] [PubMed]
- Wilbur, J.; Kolanowski, A.M.; Collins, L.M. Utilizing MOST frameworks and SMART designs for intervention research. Nurs. Outlook 2016, 64, 287–289. [Google Scholar] [CrossRef] [PubMed]
- Symons Downs, D.; Savage, J.S.; Rivera, D.E.; Smyth, J.M.; Rolls, B.J.; Hohman, E.E.; McNitt, K.M.; Kunselman, A.R.; Stetter, C.; Pauley, A.M.; et al. Individually Tailored, Adaptive Intervention to Manage Gestational Weight Gain: Protocol for a Randomized Controlled Trial in Women with Overweight and Obesity. JMIR Res. Protoc. 2018, 7, e150. [Google Scholar] [CrossRef] [Green Version]
- Cappelleri, J.C.; Bushmakin, A.G.; Gerber, R.A.; Leidy, N.K.; Sexton, C.C.; Lowe, M.R.; Karlsson, J. Psychometric analysis of the Three-Factor Eating Questionnaire-R21: Results from a large diverse sample of obese and non-obese participants. Int. J. Obes. 2009, 33, 611–620. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Jimoh, F.; Lund, E.K.; Harvey, L.J.; Frost, C.; Lay, W.J.; Roe, M.A.; Berry, R.; Finglas, P.M. Comparing Diet and Exercise Monitoring Using Smartphone App and Paper Diary: A Two-Phase Intervention Study. JMIR mHealth uHealth 2018, 6, e17. [Google Scholar] [CrossRef] [Green Version]
- Butte, N.F.; Wong, W.W.; Treuth, M.S.; Ellis, K.J.; O’Brian Smith, E. Energy requirements during pregnancy based on total energy expenditure and energy deposition. Am. J. Clin. Nutr. 2004, 79, 1078–1087. [Google Scholar] [CrossRef]
- Guo, P.; Rivera, D.E.; Downs, D.S.; Savage, J.S. Semi-physical Identification and State Estimation of Energy Intake for Interventions to Manage Gestational Weight Gain. In Proceedings of the 2016 American Control Conference (ACC), Boston, MA, USA, 6–8 July 2016; Volume 2016, pp. 1271–1276. [Google Scholar] [CrossRef] [Green Version]
- Pauley, A.M.; Hohman, E.; Savage, J.S.; Rivera, D.E.; Guo, P.; Leonard, K.S.; Symons Downs, D. Gestational Weight Gain Intervention Impacts Determinants of Healthy Eating and Exercise in Overweight/Obese Pregnant Women. J. Obes. 2018, 2018, 6469170. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, T.; Rowlands, A.V.; Olds, T.; Maher, C. The validity of consumer-level, activity monitors in healthy adults worn in free-living conditions: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 42. [Google Scholar] [CrossRef] [Green Version]
- Storm, F.A.; Heller, B.W.; Mazzà, C. Step detection and activity recognition accuracy of seven physical activity monitors. PLoS ONE 2015, 10, e0118723. [Google Scholar] [CrossRef]
- Guo, P.; Rivera, D.E.; Pauley, A.M.; Leonard, K.S.; Savage, J.S.; Downs, D.S. A “Model-on-Demand” Methodology for Energy Intake Estimation to Improve Gestational Weight Control Interventions. In Proceedings of the IFAC World Congress. International Federation of Automatic Control World Congress, Stockholm, Sweden, 9–11 July 2018; Volume 51, pp. 144–149. [Google Scholar] [CrossRef]
- Black, A.E.; Prentice, A.M.; Goldberg, G.R.; Jebb, S.A.; Bingham, S.A.; Livingstone, M.B.; Coward, W.A. Measurements of total energy expenditure provide insights into the validity of dietary measurements of energy intake. J. Am. Diet. Assoc. 1993, 93, 572–579. [Google Scholar] [CrossRef]
- Cnaan, A.; Laird, N.M.; Slasor, P. Using the general linear mixed model to analyse unbalanced repeated measures and longitudinal data. Stat. Med. 1997, 16, 2349–2380. [Google Scholar] [CrossRef]
- McNeish, D.; Harring, J. Covariance pattern mixture models: Eliminating random effects to improve convergence and performance. Behav. Res. Methods 2020, 52, 947–979. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Cade, J.E.; Allman-Farinelli, M. The Most Popular Smartphone Apps for Weight Loss: A Quality Assessment. JMIR mHealth uHealth 2015, 3, e104. [Google Scholar] [CrossRef]
- Rebro, S.M.; Patterson, R.E.; Kristal, A.R.; Cheney, C.L. The effect of keeping food records on eating patterns. J. Am. Diet. Assoc. 1998, 98, 1163–1165. [Google Scholar] [CrossRef]
- Gemming, L.; Utter, J.; Ni Mhurchu, C. Image-assisted dietary assessment: A systematic review of the evidence. J. Acad. Nutr. Diet. 2015, 115, 64–77. [Google Scholar] [CrossRef]
- Lindsay, K.L.; Heneghan, C.; McNulty, B.; Brennan, L.; McAuliffe, F.M. Lifestyle and dietary habits of an obese pregnant cohort. Matern. Child Health J. 2015, 19, 25–32. [Google Scholar] [CrossRef]
- Mullaney, L.; O’Higgins, A.C.; Cawley, S.; Doolan, A.; McCartney, D.; Turner, M.J. An estimation of periconceptional under-reporting of dietary energy intake. J. Public Health 2015, 37, 728–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGowan, C.A.; McAuliffe, F.M. Maternal nutrient intakes and levels of energy underreporting during early pregnancy. Eur. J. Clin. Nutr. 2012, 66, 906–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiraishi, M.; Haruna, M.; Matsuzaki, M.; Murayama, R.; Sasaki, S. Pre-pregnancy BMI, gestational weight gain and body image are associated with dietary under-reporting in pregnant Japanese women. J. Nutr. Sci. 2018, 7, e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mather, M.; Sutherland, M.R. Arousal-Biased Competition in Perception and Memory. Perspect. Psychol. Sci. 2011, 6, 114–133. [Google Scholar] [CrossRef] [PubMed]
- Vansant, G.; Hulens, M. The assessment of dietary habits in obese women: Influence of eating behavior patterns. Eat. Disord. 2006, 14, 121–129. [Google Scholar] [CrossRef]
- Royal, J.D.; Kurtz, J.L. I ate what?! The effect of stress and dispositional eating style on food intake and behavioral awareness. Pers. Individ. Dif. 2010, 49, 565–569. [Google Scholar] [CrossRef]
- Wallis, D.J.; Hetherington, M.M. Emotions and eating. Self-reported and experimentally induced changes in food intake under stress. Appetite 2009, 52, 355–362. [Google Scholar] [CrossRef]
- Furber, C.M.; Garrod, D.; Maloney, E.; Lovell, K.; McGowan, L. A qualitative study of mild to moderate psychological distress during pregnancy. Int. J. Nurs. Stud. 2009, 46, 669–677. [Google Scholar] [CrossRef]
- Pasquali, R. The hypothalamic-pituitary-adrenal axis and sex hormones in chronic stress and obesity: Pathophysiological and clinical aspects. Ann. N. Y. Acad. Sci. 2012, 1264, 20–35. [Google Scholar] [CrossRef]
- Garden, L.; Clark, H.; Whybrow, S.; Stubbs, R.J. Is misreporting of dietary intake by weighed food records or 24-hour recalls food specific? Eur. J. Clin. Nutr. 2018, 72, 1026–1034. [Google Scholar] [CrossRef]
- Ricciardi, L.; Mostashari, F.; Murphy, J.; Daniel, J.G.; Siminerio, E.P. A national action plan to support consumer engagement via e-health. Health Aff. 2013, 32, 376–384. [Google Scholar] [CrossRef]
- Patel, M.L.; Hopkins, C.M.; Brooks, T.L.; Bennett, G.G. Comparing Self-Monitoring Strategies for Weight Loss in a Smartphone App: Randomized Controlled Trial. JMIR mHealth uHealth 2019, 7, e12209. [Google Scholar] [CrossRef]
- Carroll, R.J.; Midthune, D.; Subar, A.F.; Shumakovich, M.; Freedman, L.S.; Thompson, F.E.; Kipnis, V. Taking advantage of the strengths of 2 different dietary assessment instruments to improve intake estimates for nutritional epidemiology. Am. J. Epidemiol. 2012, 175, 340–347. [Google Scholar] [CrossRef] [Green Version]
- Natamba, B.K.; Sanchez, S.E.; Gelaye, B.; Williams, M.A. Concordance between self-reported pre-pregnancy body mass index (BMI) and BMI measured at the first prenatal study contact. BMC Pregnancy Childbirth 2016, 16, 187. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Characteristic | N(%) 1 |
|---|---|
| Maternal Age, years | 30.7 ± 3.0 |
| Preconception BMI, kg/m2 | 32.7 ± 6.8 |
| % BMI = 24.5–29.9 | 10 (48%) |
| % BMI ≥ 30 | 11 (52%) |
| Gestational Age at Baseline (Weeks) | 10.0 ± 1.7 |
| Gestational Weight Gain, kg | 21.5 ± 15.4 |
| Race | |
| White | 21 (100%) |
| Ethnicity | |
| Non-Hispanic | 21 (100%) |
| Marital Status | |
| Divorced | 1 (5%) |
| Married | 19 (90%) |
| Single | 1 (5%) |
| Maternal Education | |
| High School | 1 (5%) |
| College | 11 (52%) |
| Graduate/Professional School | 9 (43%) |
| Gravidity | |
| 1 | 11 (52%) |
| 2 | 8 (38%) |
| 3 | 2 (10%) |
| Parity | |
| 0 | 13 (62%) |
| 1 | 8 (38%) |
| Employment | |
| Full-Time | 17 (81%) |
| Part-Time | 2 (9%) |
| Self-Employed | 1 (5%) |
| Other | 1 (5%) |
| Household Income | |
| <$20,000 | 1 (5%) |
| $20,000–$40,000 | 4 (19%) |
| $40,000–100,000 | 8 (38%) |
| ≥$100,000 | 8 (38%) |
| Characteristic | Self-Reported EI (kcal/d) Mean ± SD | Back-Calculated EI, (kcal/d) Mean ± SD | Difference between Back-Calculated and Self-Reported EI, (kcal/d) Mean ± SD | % Underreporting Mean ± SD |
|---|---|---|---|---|
| Overall (n = 21) | 1696 ± 481 | 2950 ± 142 | 1263 ± 162 | 38% ± 4 |
| Gestational Age (Trimester) | ||||
| First Trimester | 1702 ± 70 a | 2688 ± 144 a | 986 ± 166 a | 32% ± 4 a |
| Second Trimester | 1681 ± 67 a | 2960 ± 141 b | 1280 ± 162 b | 39% ± 4 b |
| Third Trimester | 1692 ± 68 a | 3077 ± 142 c | 1386 ± 164 c | 40% ± 4 b |
| Pre-Pregnancy BMI | ||||
| BMI 25–29.9 (n = 10) | 1743 ± 97 a | 2537 ± 165 a | 794 ± 190 a | 28% ± 5 a |
| BMI ≥ 30 (n = 11) | 1637 ± 92 a | 3324 ± 157 b | 1688 ± 181 b | 47% ± 4 b |
| Total GWG Classified by Institute of Medicine Guidelines | ||||
| Not Exceeding (n = 12) | 1736 ± 88 a | 3006 ± 191 a | 1271 ± 220 a | 35% ± 5 a |
| Exceeding (n = 9) | 1622 ± 102 a | 2874 ± 221 a | 1253 ± 254 a | 41% ± 6 a |
| Parity | ||||
| 0 (n = 13) | 1672 ± 86 a | 3000 ± 184 a | 1329 ± 210 a | 40% ± 5 a |
| 1 (n = 8) | 1712 ± 110 a | 2867 ± 234 a | 1156 ± 340 a | 36% ± 6 a |
| Annual Household Income | ||||
| $10,000–$20,000 (n = 1) | 1465 ± 315 a | 4286 ± 613 a | 2821 ± 61 a | 65% ± 17 a |
| $20,000–$40,000 (n = 4) | 1689 ± 158 a | 2695 ± 307 b | 1007 ± 346 b | 32% ± 9 a |
| $40,000–$100,000 (n = 8) | 1624 ± 111 a | 2971 ± 216 b | 1348 ± 244 b | 41% ± 6 a |
| >$100,000 (n = 8) | 1778 ± 111 a | 2888 ± 217 b | 1111 ± 244 b | 35% ± 6 a |
| Treatment Group Assignment | ||||
| Intervention (n = 11) | 1689 ± 94 a | 2902 ± 200 a | 1213 ± 229 a | 37% ± 5 a |
| Control (n = 10) | 1686 ± 99 a | 3002 ± 210 a | 1318 ± 240 a | 40% ± 6 a |
| Variable | Model Estimate | Standard Error | p-Value |
|---|---|---|---|
| Gestational Age (days) | −0.05372 | 0.009664 | <0.0001 |
| Gestational Age (by trimester) (reference = Trimester 3) | <0.0001 | ||
| Trimester (1) | 8.0931 | 1.6027 | |
| Trimester (2) | 1.3743 | 1.1605 | |
| Pre-Pregnancy BMI (kg/m2) | −1.4144 | 0.4943 | 0.0100 |
| Pre-Pregnancy BMI classification (reference = BMI > 30) | 0.0075 | ||
| BMI = 25.0–29.9 | 19.3786 | 6.4793 | |
| Perceived Stress (within-person) | 0.2561 | 0.1033 | 0.0133 |
| Perceived Stress (between-person) | −0.1708 | 0.6372 | 0.7915 |
| Emotional Eating (within-person) | 7.3520 | 0.5073 | <0.0001 |
| Emotional Eating (between-person) | −0.1734 | 0.6583 | 0.7950 |
| Cognitive Restraint (within-person) | 0.6897 | 0.5186 | 0.1838 |
| Cognitive Restraint (between-person) | −2.7578 | 3.2976 | 0.4134 |
| Uncontrolled Eating (within-person) | −0.3294 | 0.2798 | 0.2393 |
| Uncontrolled Eating (between-person) | −1.3742 | 1.1126 | 0.2318 |
| Total GWG (in kg) (n = 19) | −0.5049 | 0.5856 | 0.4006 |
| Total GWG (meeting vs. exceeding Institute of Medicine guidelines) (reference = meeting guidelines) | −6.5364 | 8.3740 | 0.4458 |
| Weekly GWG (in kg) | −5.4802 | 0.9972 | <0.0001 |
| Weekly GWG (meeting vs. exceeding Institute of Medicine guidelines) (reference = meeting guidelines) | 0.0007 | ||
| Under | 5.0148 | 1.9283 | |
| Over | 0.5328 | 1.9144 | |
| Treatment group (reference = intervention) | 0.7294 | ||
| Control | −2.7539 | 7.28448 | |
| Maternal Age (yrs) | 0.3989 | 1.3283 | 0.7672 |
| Parity (reference = 1) | 0.6131 | ||
| Parity (0) | −4.1338 | 8.0404 | |
| Household Income (yearly) (reference ≥ $100,000) | 0.3396 | ||
| $10,000–$20,000 | −30.4517 | 18.3616 | |
| $20,000–$40,000 | 2.8334 | 10.6118 | |
| $40,000–100,000 | 6.9350 | 8.6440 |
| Predictor | Relationship with underreporting |
|---|---|
| Gestational age | Greater underreporting in later pregnancy |
| Pre-pregnancy BMI | Greater underreporting with higher BMI |
| Gestational weight gain | Greater underreporting with greater weekly weight gain |
| Maternal age | No association |
| Parity | No association |
| Household Income | No association |
| Perceived stress | Less underreporting during weeks when participant indicated higher stress than their usual stress level |
| Emotional eating | Less underreporting during months when participant indicated higher emotional eating than their usual level |
| Cognitive restraint | No association |
| Uncontrolled eating | No association |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McNitt, K.M.; Hohman, E.E.; Rivera, D.E.; Guo, P.; Pauley, A.M.; Gernand, A.D.; Symons Downs, D.; Savage, J.S. Underreporting of Energy Intake Increases over Pregnancy: An Intensive Longitudinal Study of Women with Overweight and Obesity. Nutrients 2022, 14, 2326. https://doi.org/10.3390/nu14112326
McNitt KM, Hohman EE, Rivera DE, Guo P, Pauley AM, Gernand AD, Symons Downs D, Savage JS. Underreporting of Energy Intake Increases over Pregnancy: An Intensive Longitudinal Study of Women with Overweight and Obesity. Nutrients. 2022; 14(11):2326. https://doi.org/10.3390/nu14112326
Chicago/Turabian StyleMcNitt, Katherine M., Emily E. Hohman, Daniel E. Rivera, Penghong Guo, Abigail M. Pauley, Alison D. Gernand, Danielle Symons Downs, and Jennifer S. Savage. 2022. "Underreporting of Energy Intake Increases over Pregnancy: An Intensive Longitudinal Study of Women with Overweight and Obesity" Nutrients 14, no. 11: 2326. https://doi.org/10.3390/nu14112326
APA StyleMcNitt, K. M., Hohman, E. E., Rivera, D. E., Guo, P., Pauley, A. M., Gernand, A. D., Symons Downs, D., & Savage, J. S. (2022). Underreporting of Energy Intake Increases over Pregnancy: An Intensive Longitudinal Study of Women with Overweight and Obesity. Nutrients, 14(11), 2326. https://doi.org/10.3390/nu14112326