
Malnutrition Risk: Four Year Outcomes from the Health, Work and Retirement Study 2014 to 2018




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Recruitment
2.3. Measures
2.3.1. Demographic Characteristics
2.3.2. Physical and Mental Health
2.3.3. Depression
2.3.4. Hazardous Alcohol Use
2.3.5. Social Connectedness
2.3.6. Nutrition Status
2.4. Statistical Analysis
3. Results
3.1. Participants
3.2. Exploring the Baseline Differences
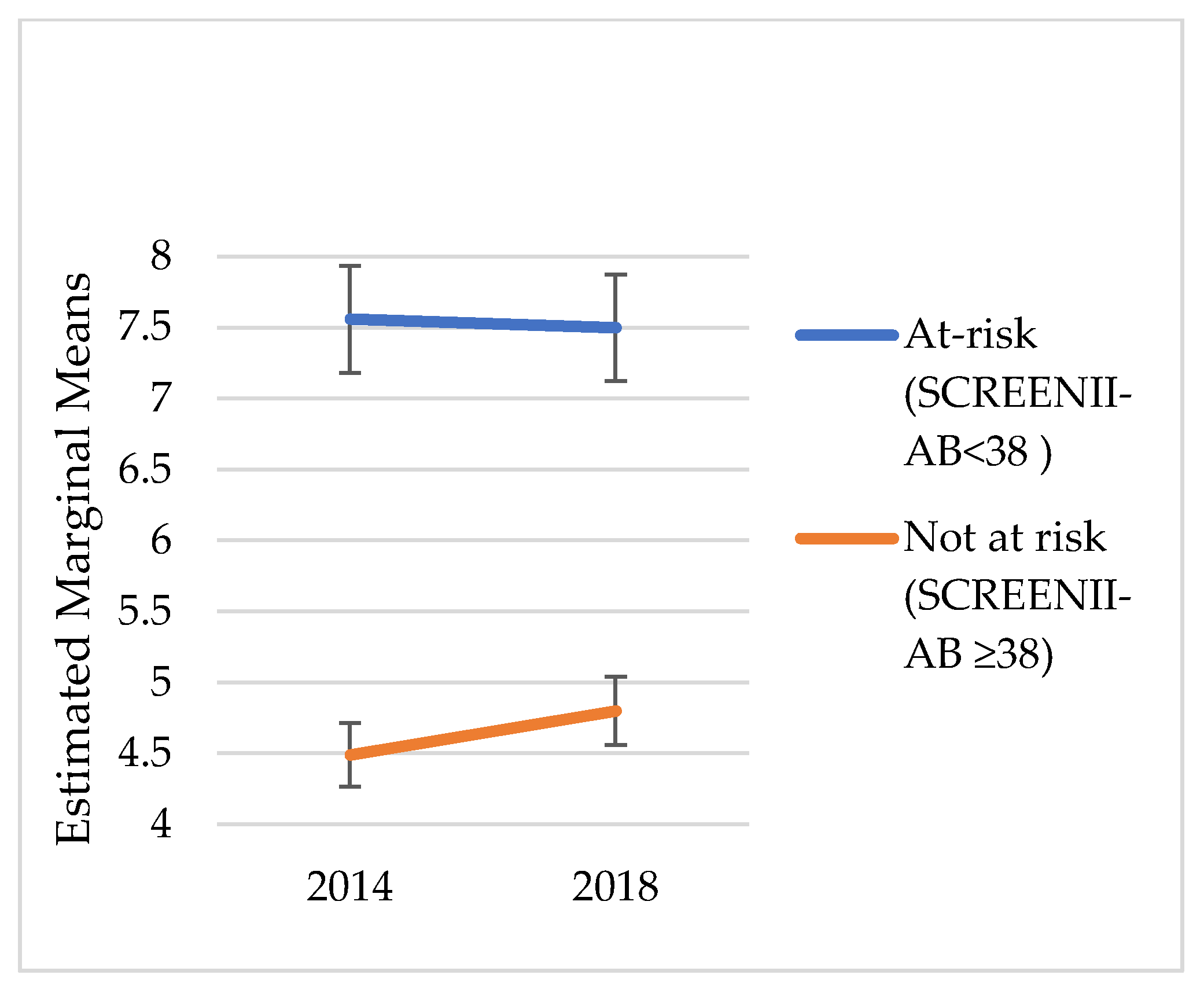
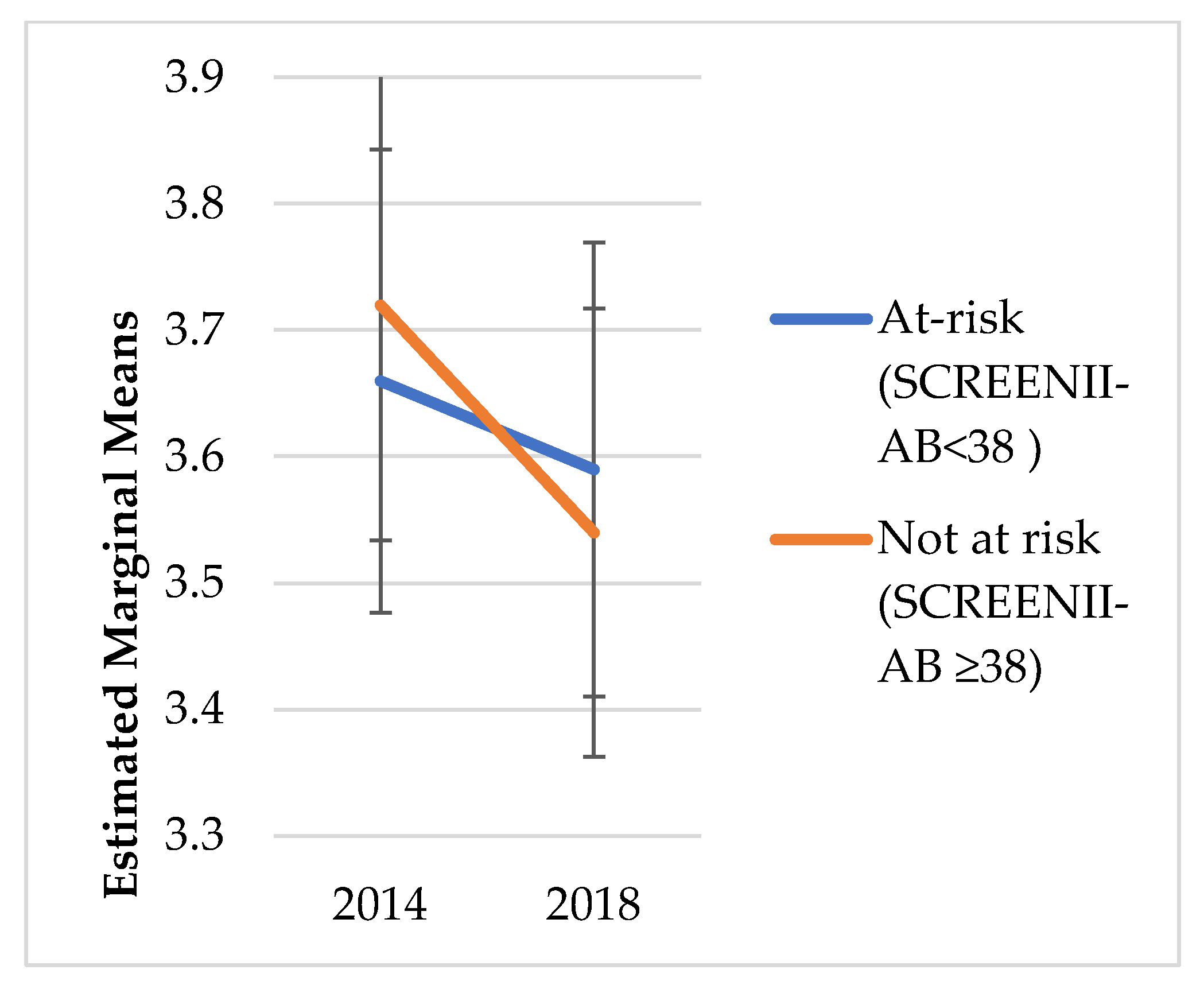
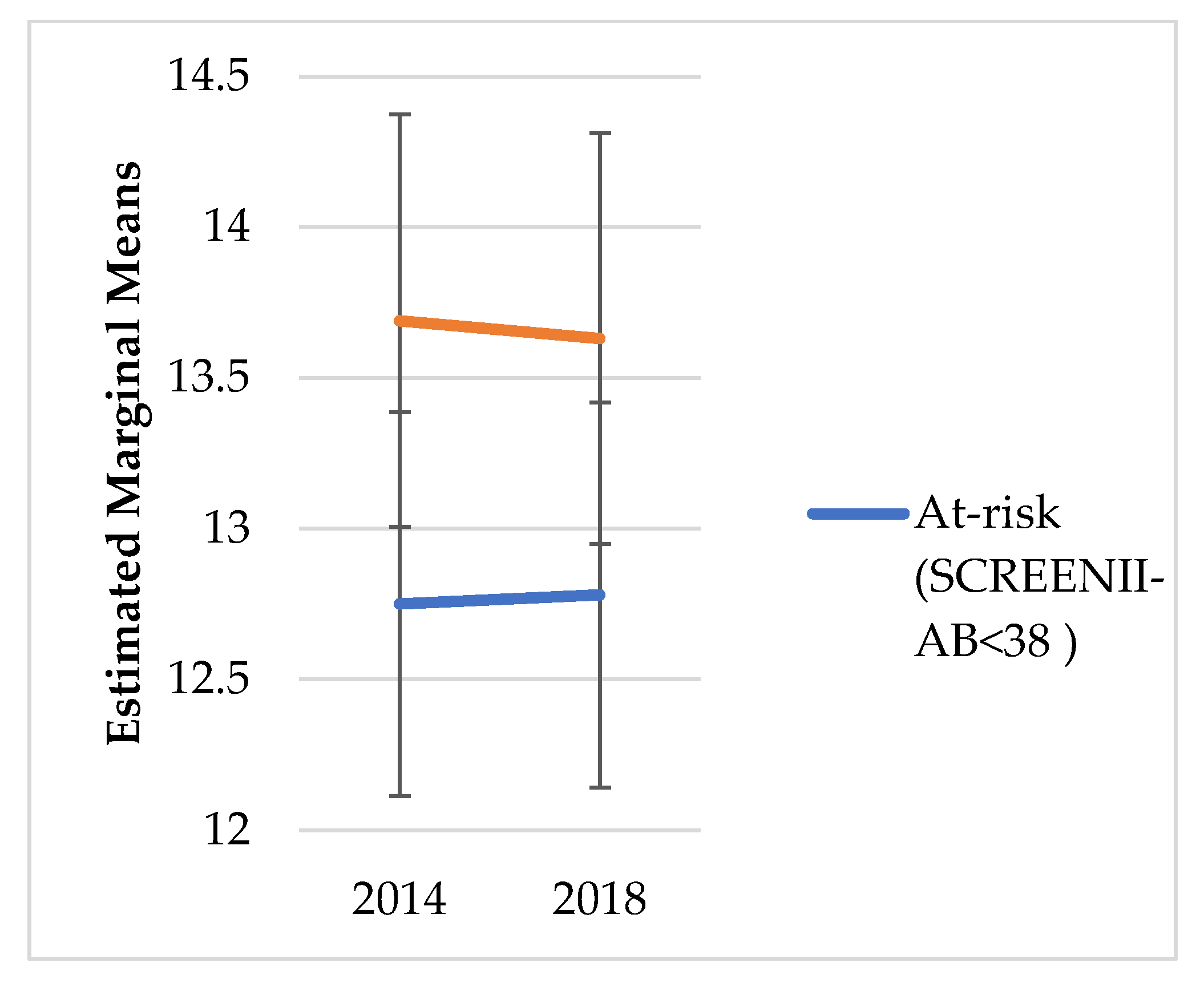
3.3. Exploring Differences between Baseline and Four-Year Follow-Up
3.4. Assessing Statistically Significant Change
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Number of People over 60 Years Set to Double by 2050; Major Societal Changes Required. Available online: http://www.who.int/mediacentre/news/releases/2015/older-persons-day/en/ (accessed on 3 August 2021).
- Organisation for Economic Co-operation and Development (OECD). Life Expectancy at Birth (Indicator). Available online: https://data.oecd.org/healthstat/life-expectancy-at-birth.htm#indicator-chart (accessed on 22 January 2018).
- Ministry of Health. Older People’s Health Data and Stats; Ministry of Health: Wellington, New Zealand, 2016. [Google Scholar]
- Kowal, P.; Towers, A.; Byles, J. Ageing across the Tasman Sea: The demographics and health of older adults in Australia and New Zealand. Aust. N. Z. J. Public Health 2014, 38, 377–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parr-Brownlie, L.C.; Waters, D.L.; Neville, S.; Neha, T.; Muramatsu, N. Aging in New Zealand: Ka haere ki te ao pakeketanga. Gerontologist 2020, 60, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.; Savina, C.; Rosano, A.; Cannella, C. Systematic review of nutritional status evaluation and screening tools in the elderly. J. Nutr. Health Aging 2007, 11, 421–432. [Google Scholar]
- Watterson, C.; Fraser, A.; Banks, M.; Iserning, E.; Miller, M.H.; Hoevenaars, R.; Bauer, J.; Vivanti, A.; Ferguson, M. Evidence based practice guidelines for the nutritional management of malnutrition in adult patients across the continuum of care. Nutr. Diet. 2009, 66, S1–S34. [Google Scholar]
- Australian & New Zealand Society for Geriatric Medicine. Position Statement No 6 Undernutrition and the Older Person; Australian & New Zealand Society for Geriatric Medicine: Sydney, Australia, 2019. [Google Scholar]
- Starr, K.N.P.; McDonald, S.R.; Bales, C.W. Nutritional vulnerability in older adults: A continuum of concerns. Curr. Nutr. Rep. 2015, 4, 176–184. [Google Scholar] [CrossRef] [Green Version]
- Keller, H.; Goy, R.; Kane, S.L. Validity and reliability of SCREEN II (Seniors in the Community: Risk evaluation for eating and nutrition, Version II). Eur. J. Clin. Nutr. 2005, 59, 1149–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tkatch, M.T.; Towers, A.J.; Keller, H.H.; Wham, C.A. Nutrition risk prevalence and associated health and social risk factors in Māori and non-Māori: Results from the New Zealand Health, Work and Retirement Study. Australas. J. Ageing 2021, 41, 59–69. [Google Scholar] [CrossRef]
- Watson, S.; Zhang, Z.K.; Wilkinson, T.J. Nutrition risk screening in community-living older people attending medical or falls prevention services. Nutr. Diet. 2010, 67, 84–89. [Google Scholar] [CrossRef]
- McElnay, C.; Marshall, B.; O’Sullivan, J.; Jones, L.; Ashworth, T.; Hicks, K.; Forrest, R.H. Nutritional risk amongst community-living Maori and non-Maori older people in Hawke’s Bay. J. Prim. Health Care 2012, 4, 299–305. [Google Scholar] [CrossRef]
- Wham, C.; Teh, R.; Moyes, S.; Dyall, L.; Kepa, M.; Hayman, K.; Kerse, N. Health and social factors associated with nutrition risk: Results from life and living in advanced age: A cohort study in New Zealand (LILACS NZ). J. Nutr. Health Aging 2015, 19, 637–645. [Google Scholar] [CrossRef]
- Allen, J.; Alpass, F.M.; Stephens, C.V. New Zealand Health, Work, and Retirement Longitudinal Study. In Encyclopedia of Gerontology and Population Aging; Gu, D., Dupre, M.E., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 1–7. [Google Scholar]
- Towers, A.; Stevenson, B.; Breheny, M.; Allen, J. Health, Work, and Retirement Longitudinal Study. In Encyclopedia of Geropsychology; Pachana, N.A., Ed.; Springer Singapore: Singapore, 2017; pp. 1025–1033. [Google Scholar]
- Shah, C.H.; Brown, J.D. Reliability and Validity of the Short-Form 12 Item Version 2 (SF-12v2) Health-Related Quality of Life Survey and Disutilities Associated with Relevant Conditions in the U.S. Older Adult Population. J. Clin. Med. 2020, 9, 661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for depression in well older adults: Evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef]
- Mohebbi, M.; Nguyen, V.; McNeil, J.J.; Woods, R.L.; Nelson, M.R.; Shah, R.C.; Storey, E.; Murray, A.M.; Reid, C.M.; Kirpach, B.; et al. Psychometric properties of a short form of the Center for Epidemiologic Studies Depression (CES-D-10) scale for screening depressive symptoms in healthy community dwelling older adults. Gen. Hosp. Psychiatry 2018, 51, 118–125. [Google Scholar] [CrossRef]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT alcohol consumption questions (AUDIT-C): An effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Towers, A.; Stephens, C.; Dulin, P.; Kostick, M.; Noone, J.; Alpass, F. Estimating older hazardous and binge drinking prevalence using AUDIT-C and AUDIT-3 thresholds specific to older adults. Drug Alcohol Depend. 2011, 117, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.; Hewitt, C.; McCambridge, J. Exploratory validation study of the individual AUDIT-C items among older people. Alcohol Alcohol. 2020, 56, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Cutrona, C.E.; Russell, D.W. The provisions of social relationships and adaptation to stress. Adv. Pers. Relatsh. 1987, 1, 37–67. [Google Scholar]
- Zaki, M.A. Reliability and validity of the Social Provision Scale (SPS) in the students of Isfahan University. Iran. J. Psychiatry Clin. Psychol. 2009, 14, 439–444. [Google Scholar]
- Craven, D.L.; Pelly, F.E.; Lovell, G.P.; Isenring, E. Nutrition Risk Measured Online in Community-Living Older Australians. J. Nutr. Gerontol. Geriatr. 2018, 37, 241–254. [Google Scholar] [CrossRef]
- Yap, K.B.; Niti, M.; Ng, T.P. Nutrition screening among community-dwelling older adults in Singapore. Singap. Med. J. 2007, 48, 911–916. [Google Scholar]
- Naseer, M.; Fagerström, C. Prevalence and association of undernutrition with quality of life among Swedish people aged 60 years and above: Results of the SNAC-B study. J. Nutr. Health Aging 2015, 19, 970. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-C.; Liang, C.-K.; Hsu, Y.-H.; Peng, L.-N.; Chu, C.-S.; Liao, M.-C.; Shen, H.-C.; Chou, M.-Y.; Lin, Y.-T. Synergistic effect of low handgrip strength and malnutrition on 4-year all-cause mortality in older males: A prospective longitudinal cohort study. Arch. Gerontol. Geriatr. 2019, 83, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Ghimire, S.; Baral, B.K.; Karmacharya, I.; Callahan, K.; Mishra, S.R. Life satisfaction among elderly patients in Nepal: Associations with nutritional and mental well-being. Health Qual. Life Outcomes 2018, 16, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulos, C.; Salameh, P.; Barberger-Gateau, P. Social isolation and risk for malnutrition among older people. Geriatr. Gerontol. Int. 2017, 17, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Schilp, J.; Wijnhoven, H.; Deeg, D.; Visser, M. Early determinants for the development of undernutrition in an older general population: Longitudinal Aging Study Amsterdam. Br. J. Nutr. 2011, 106, 708–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wham, C.A.; Teh, R.; Moyes, S.; Dyall, L.; Kepa, M.; Hayman, K.; Kerse, N. The Bright Trial: What are the factors associated with nutrition risk? J. Nutr. Health Aging 2014, 18, 692–697. [Google Scholar] [CrossRef]
- Bernstein, M.A.; Tucker, K.L.; Ryan, N.D.; O’Neill, E.F.; Clements, K.M.; Nelson, M.E.; Evans, W.J.; Singh, M.A.F. Higher dietary variety is associated with better nutritional status in frail elderly people. J. Am. Diet. Assoc. 2002, 102, 1096–1104. [Google Scholar] [CrossRef]
- Locher, J.; Robinson, C.; Roth, D.; Ritchie, C.; Burgio, K. The Effect of the Presence of Others on Caloric Intake in Homebound Older Adults. J. Gerontol. Med. Sci. 2005, 60, 1475–1478. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, K.; Yamada, M.; Kajiwara, Y.; Nishiguchi, S.; Aoyama, T. Relationship between depression and risk of malnutrition among community-dwelling young-old and old-old elderly people. Aging Ment. Health 2013, 17, 456–460. [Google Scholar] [CrossRef] [Green Version]
- Lyness, J.M.; Noel, T.K.; Cox, C.; King, D.A.; Conwell, Y.; Caine, E.D. Screening for depression in elderly primary care patients. A comparison of the Center for Epidemiologic Studies-Depression Scale and the Geriatric Depression Scale. Arch. Intern. Med. 1997, 157, 449–454. [Google Scholar] [CrossRef]
- Roberts, K.C.; Wolfson, C.; Payette, H. Predictors of nutritional risk in community-dwelling seniors. Can. J. Public Health 2007, 98, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, M.A.S.; Mesas, A.E.; Garcia, A.R.L.; de Andrade, S.M. Malnutrition and Depression among Community-dwelling Elderly People. J. Am. Med. Dir. Assoc. 2007, 8, 582–584. [Google Scholar] [CrossRef]
- Johansson, Y.; Bachrach-Lindström, M.; Carstensen, J.; Ek, A.C. Malnutrition in a home-living older population: Prevalence, incidence and risk factors. A prospective study. J. Clin. Nurs. 2009, 18, 1354–1364. [Google Scholar] [CrossRef] [PubMed]
- Durie, M. A Maori perspective of health. Soc. Sci. Med. 1985, 20, 483–486. [Google Scholar] [CrossRef]
- Ávila-Funes, J.A.; Gray-Donald, K.; Payette, H. Association of Nutritional Risk and Depressive Symptoms with Physical Performance in the Elderly: The Quebec Longitudinal Study of Nutrition as a Determinant of Successful Aging (NuAge). J. Am. Coll. Nutr. 2008, 27, 492–498. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, W.A.; Shifflett, P.A. Influence of Social Support Systems on Dietary Intake of the Elderly. J. Nutr. Elder. 1984, 4, 5–18. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 2405 | At-Risk n (%) SCREENII-AB < 38 782 (33.9) | Not at-Risk n (%) SCREENII-AB ≥ 38 1528 (66.1) | |
|---|---|---|---|
| Age (49–87) | |||
| Mean (SD) | 66 (6.2) | 65.8 (6.3) | 66.2 (6.1) |
| Sex | |||
| Male | 1066 (44.3) | 308 (39.4) | 713 (46.7) |
| Female | 1339 (55.7) | 474 (60.4) | 815 (53.3) |
| Ethnicity | |||
| NZ European | 1598 (71) | 459 (60.2) | 1139 (76.6) |
| Māori | 537 (23.9) | 252 (33) | 285 (19.1) |
| Other | 115 (5.1) | 52 (6.8) | 63 (4.2) |
| Marital status | |||
| Partnered | 1805 (76.2) | 486 (63.4) | 1249 (82.9) |
| Un-partnered | 564 (23.8) | 281 (36.6) | 258 (17.1) |
| Education | |||
| No qualifications | 500 (27.1) | 207 (27) | 257 (17) |
| Secondary school | 528 (28.6) | 169 (22.1) | 345 (22.9) |
| Post-secondary | 819 (44.3) | 390 (50.9) | 907 (60.1) |
| Household composition | |||
| Living alone | 546 (19.1) | 200 (26.2) | 218 (14.4) |
| Living with others | 2315 (80.9) | 563 (73.8) | 1291 (85.6) |
| Residence type | |||
| Standalone or detached | 2045 (87.2) | 641 (86.3) | 1332 (90.5) |
| Joined household | 207 (8.8) | 82 (11) | 112 (7.6) |
| Retirement village | 38 (1.6) | 12 (1.6) | 23 (1.9) |
| Other, including moveable dwelling, or rest home | 56 (2.3) | 8 (0.54) | 5 (0.3) |
| Hospital usage in last 12 months | |||
| Yes | 811 (36.1) | 315 (41.4) | 496 (33.3) |
| No | 1438 (63.9) | 445 (58.6) | 993 (66.7) |
| Scale Scores | |||
|---|---|---|---|
| At-Risk n (%) SCREENII-AB < 38 782 (33.9) | Not at-Risk n (%) SCREENII-AB ≥ 38 1528 (66.1) | Test for Significant Difference | |
| Mean (SD) | Mean (SD) | ||
| SF-12 Physical health | 42.94 (11.06) | 48.56 (8.27) | p ≤ 0.001; d = 0.61 |
| SF-12 Mental health | 46.25 (11.29) | 52.29 (8.05) | p ≤ 0.001; d = 0.65 |
| Depression | 8.05 (5.15) | 4.65 (3.80) | p ≤ 0.001; d = 0.79 |
| Hazardous alcohol use | 3.37 (2.42) | 3.57 (2.06) | p = 0.07; d = 0.09 |
| Social connections | |||
| Attachment | 12.67 (2.35) | 13.76 (2.09) | p ≤ 0.001; d = 0.50 |
| Social integration | 12.7 (1.92) | 13.6 (1.79) | p ≤ 0.001; d = 0.49 |
| Effect | Univariate Outcome | N | df | F | p * | η2p |
|---|---|---|---|---|---|---|
| Time | SF-12 Physical health | 1471 | 1, 1469 | 13.65 | <0.001 * | 0.009 |
| SF-12 Mental health | 1471 | 1, 1469 | 8.14 | 0.004 * | 0.006 | |
| Depression | 1471 | 1, 1469 | 1.195 | 0.275 | 0.001 | |
| Hazardous alcohol use | 1471 | 1, 1469 | 12.08 | 0.001 * | 0.008 | |
| Attachment | 1471 | 1, 1469 | 4.23 | 0.40 | 0.003 | |
| Social integration | 1471 | 1, 1469 | 0.14 | 0.712 | <0.001 | |
| Malnutrition risk | SF-12 Physical health | 1471 | 1, 1469 | 106.03 | <0.001 * | 0.67 |
| SF-12 Mental health | 1471 | 1, 1469 | 112.43 | <0.001 * | 0.71 | |
| Depression | 1471 | 1, 1469 | 174.36 | <0.001 * | 0.106 | |
| Hazardous alcohol use | 1471 | 1, 1469 | 0.004 | 0.952 | <0.001 | |
| Attachment | 1471 | 1, 1469 | 113.52 | <0.001 * | 0.072 | |
| Social integration | 1471 | 1, 1469 | 93.52 | <0.001 * | 0.06 | |
| Time*Malnutrition risk | SF-12 Physical health | 1471 | 1, 1469 | 1.26 | 0.263 | 0.001 |
| SF-12 Mental health | 1471 | 1, 1469 | 8.19 | 0.004 * | 0.006 | |
| Depression | 1471 | 1, 1469 | 2.65 | 0.104 | 0.002 | |
| Hazardous alcohol use | 1471 | 1, 1469 | 2.66 | 0.103 | 0.002 | |
| Attachment | 1471 | 1, 1469 | 0.008 | 0.929 | <0.001 | |
| Social integration | 1471 | 1, 1469 | 0.79 | 0.374 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wham, C.; Curnow, J.; Towers, A. Malnutrition Risk: Four Year Outcomes from the Health, Work and Retirement Study 2014 to 2018. Nutrients 2022, 14, 2205. https://doi.org/10.3390/nu14112205
Wham C, Curnow J, Towers A. Malnutrition Risk: Four Year Outcomes from the Health, Work and Retirement Study 2014 to 2018. Nutrients. 2022; 14(11):2205. https://doi.org/10.3390/nu14112205
Chicago/Turabian StyleWham, Carol, Jade Curnow, and Andy Towers. 2022. "Malnutrition Risk: Four Year Outcomes from the Health, Work and Retirement Study 2014 to 2018" Nutrients 14, no. 11: 2205. https://doi.org/10.3390/nu14112205
APA StyleWham, C., Curnow, J., & Towers, A. (2022). Malnutrition Risk: Four Year Outcomes from the Health, Work and Retirement Study 2014 to 2018. Nutrients, 14(11), 2205. https://doi.org/10.3390/nu14112205