
Mixed Milk Feeding: A New Approach to Describe Feeding Patterns in the First Year of Life Based on Individual Participant Data from Two Randomised Controlled Trials

 ,
,  , , ,
, , ,  , , ,
, , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Tempo Study Description
- The daily feeding status variables were deduced from the start–stop ages for BF and FF. If for a given day a subject figured as neither FF nor BF (and before the start of complementary feeding), then the daily feeding status variables were set to “missing”. This was the case for approximately 2.4% of the data;
- The estimated daily study product volume intake was determined either by having it set to 0 for the days where subjects were not FF or by the average daily intake for all the days that corresponded to an e-diary entry. When the study product intake was not reported for an interval between time intervals with known study product intake, the average daily volume was filled in by interpolating between the closes known values. This was the case for 12% of the data;
- If study product volume intake was missing completely before a given age, first observation carried backward imputation was used. If the study product volume intake was missing completely after a given age, the last observation carried forward was used. This was the case for 8% of the data.
2.2. Venus Study Description
3. Results
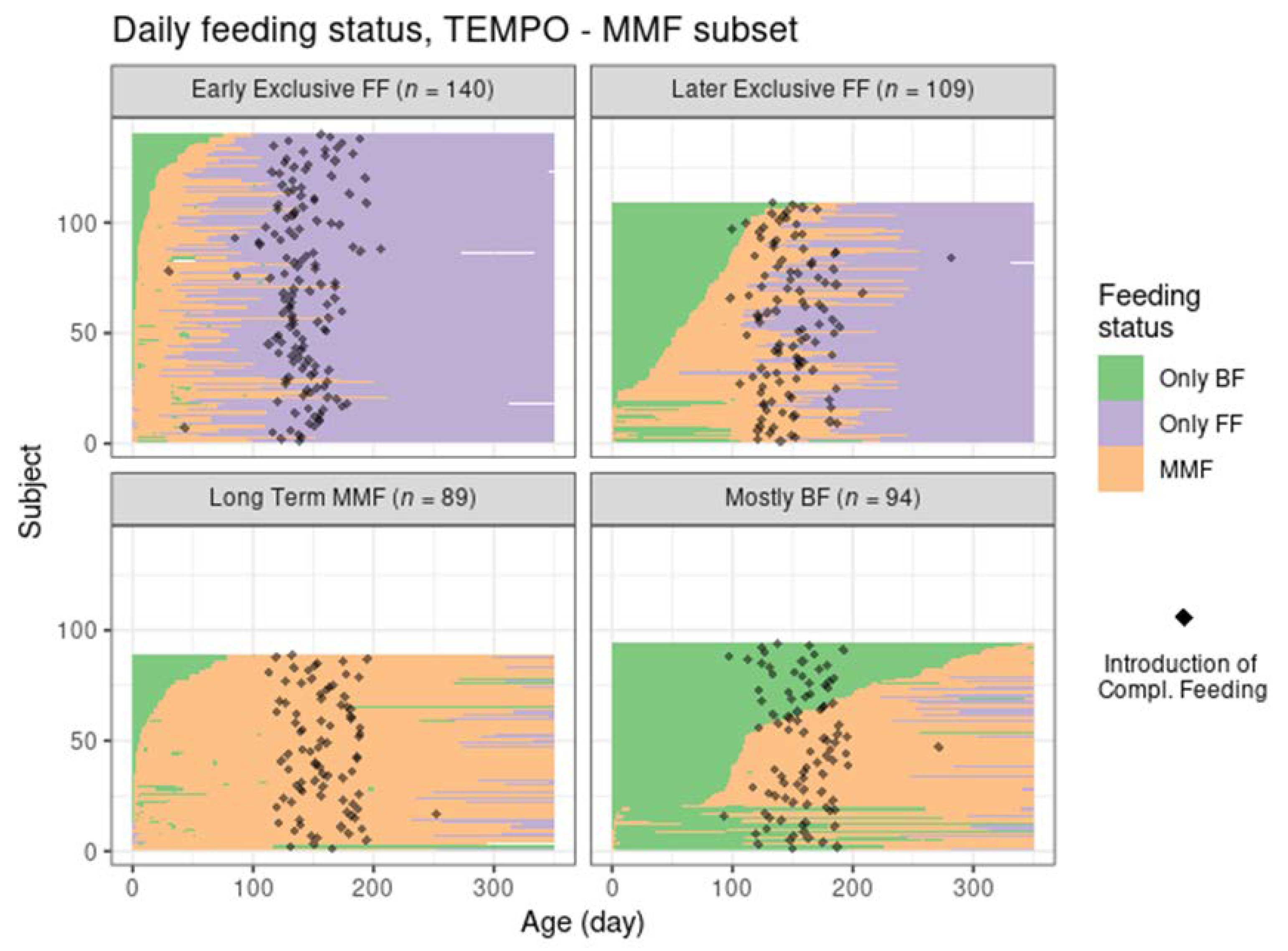
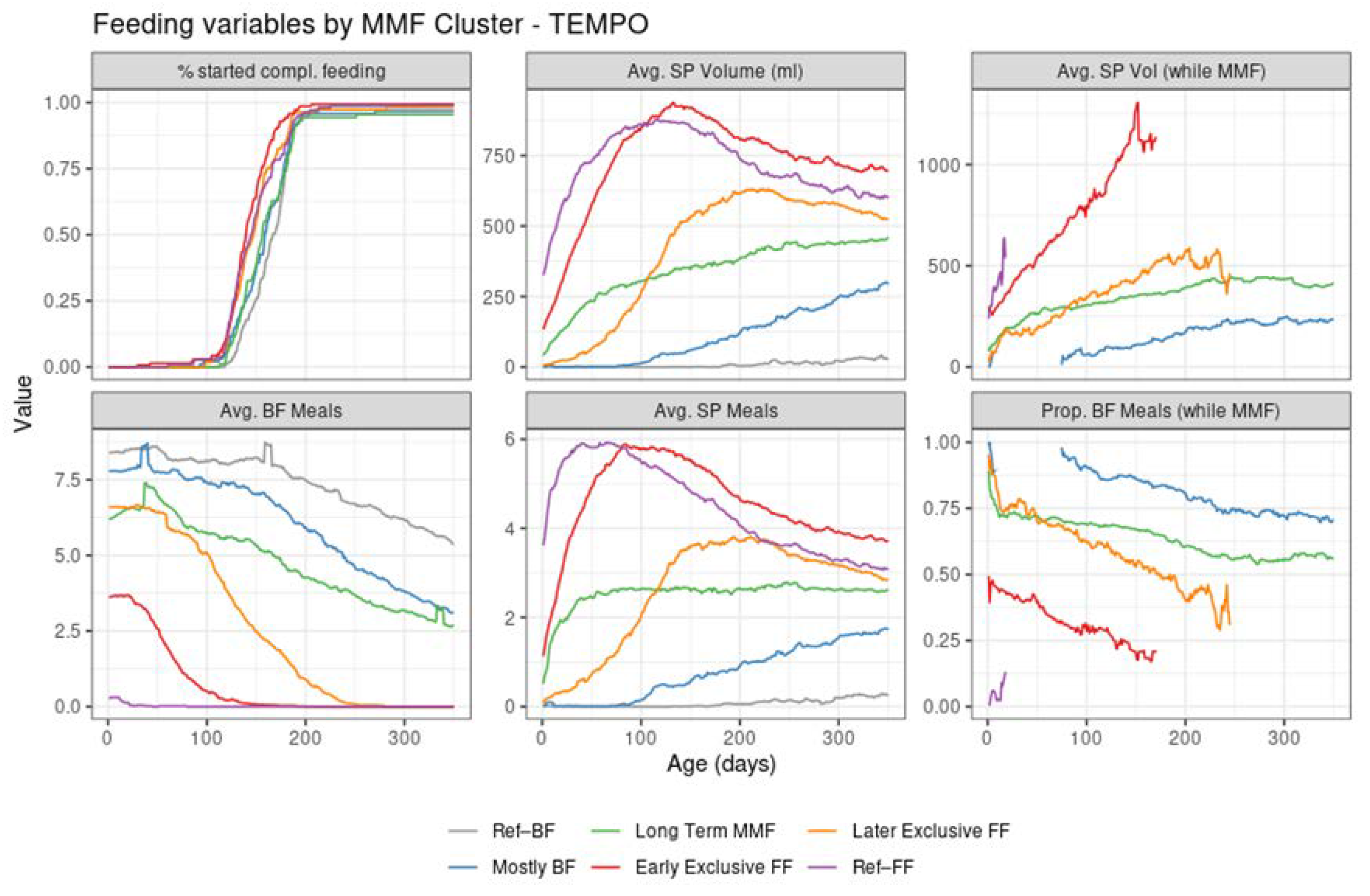
3.1. MMF Clusters in the TEMPO Study
- Cluster 1: Early exclusive FF (early transition to exclusive FF) are subjects that have an early episode of mixed milk feeding, followed by exclusive FF after approximately 80 days of age. Typically, by the time of introducing complementary foods, the babies are not BF anymore. In terms of formula intake, the quantity is very similar to the subjects in Ref–FF;
- Cluster 2: Later exclusive FF (later transition to exclusive FF) represents a feeding pattern where a mixed milk feeding episode is usually observed as a starting before 150 days of age (and, overall, later compared to early exclusive FF), with stopping of BF close to the age of introducing complementary feeding;
- Cluster 3: Long-term MMF are MMF subjects who are characterised by the introduction of formula quite early and continuing both FF and BF until 1 year of age;
- Cluster 4: Mostly BF are MMF subjects that have a prolonged period of exclusive BF, usually later introduction of formula, and in smaller amounts. The daily number of BF meals is close to that in the Ref–BF group.
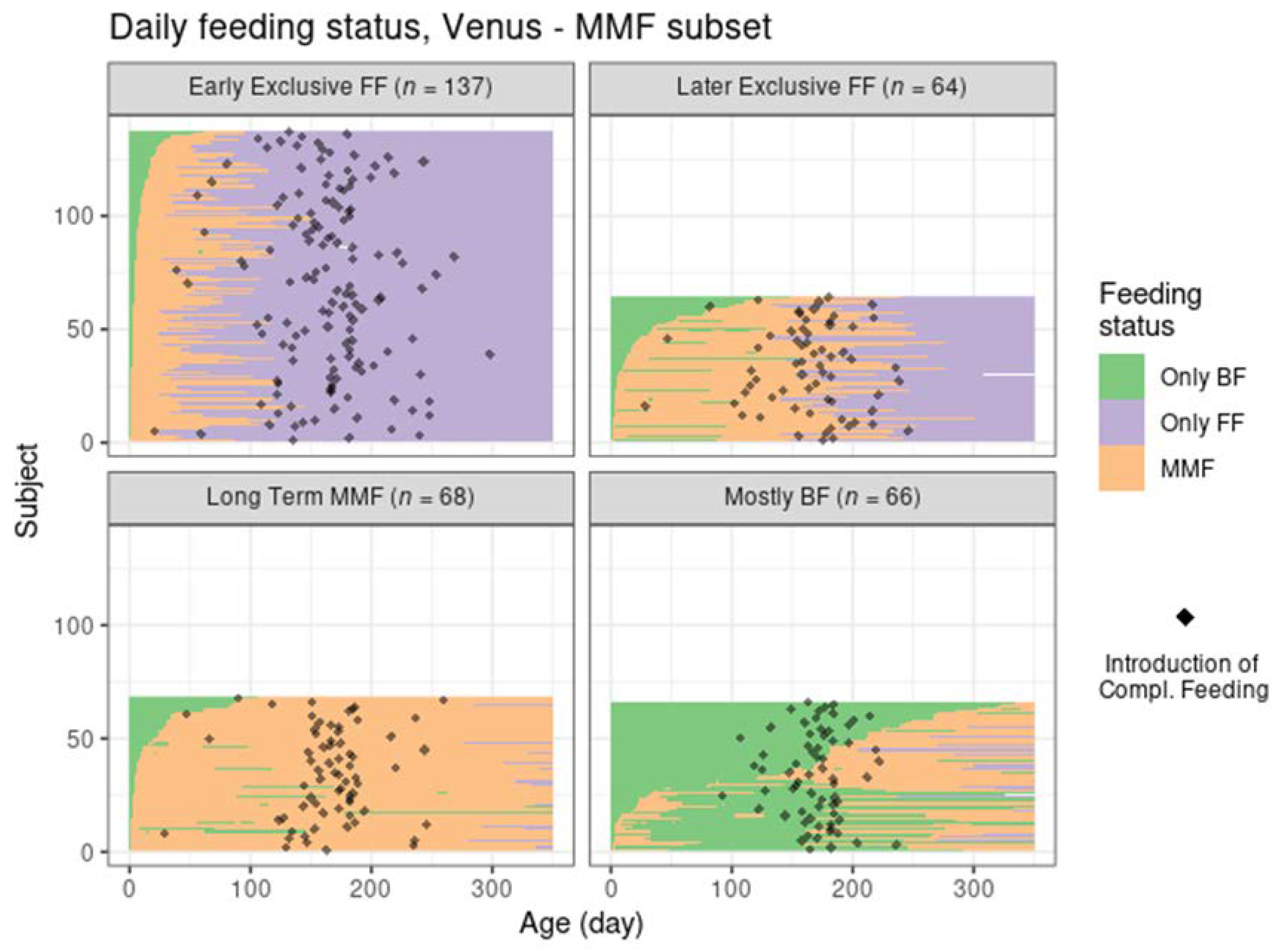
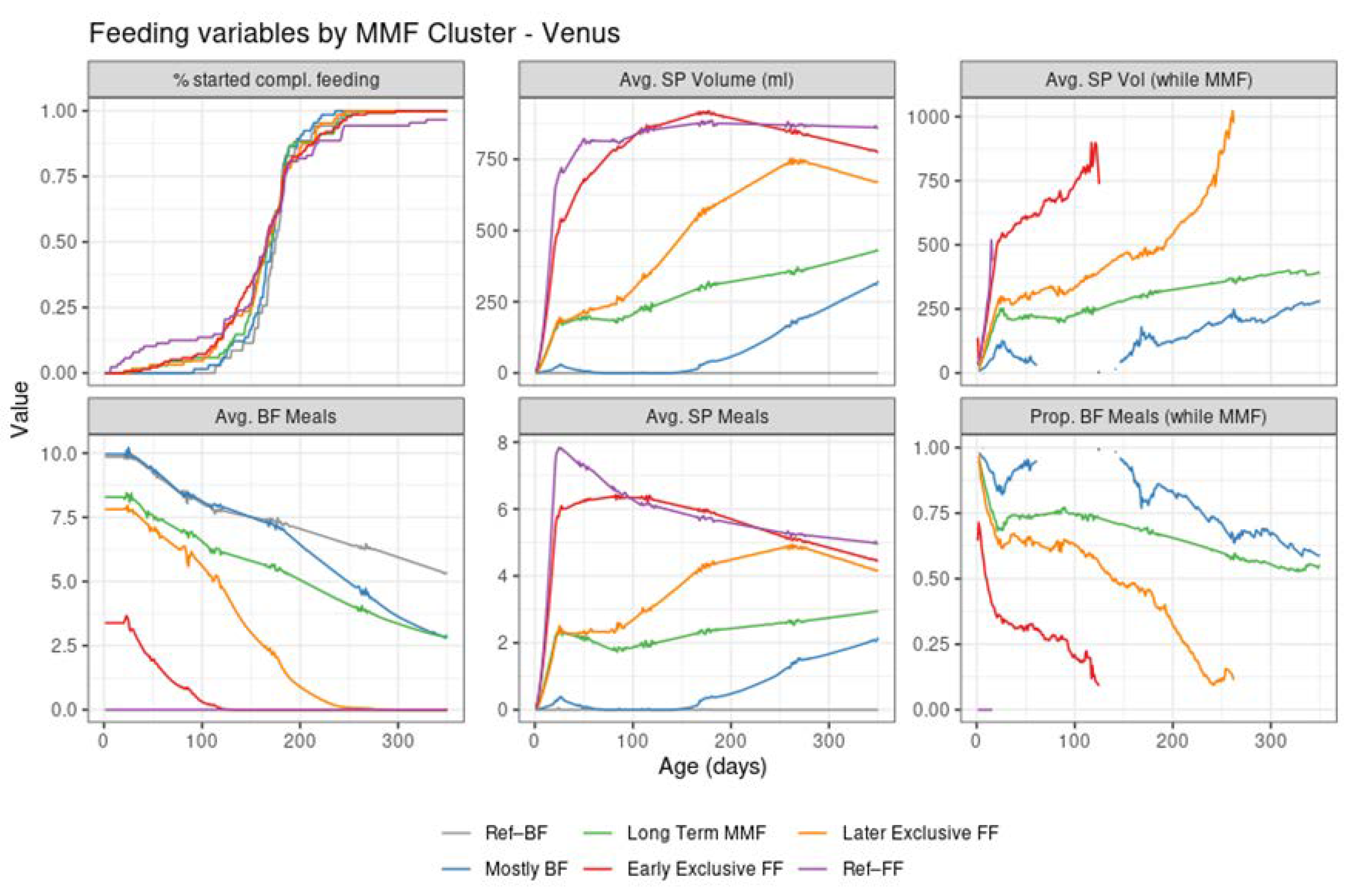
3.2. Replications of Findings in an Asian Population—Mixed Milk Feeding Patterns in the Venus Study
- In Venus, subjects in the early exclusive FF cluster had a later median age of introducing complementary feeding, a slightly higher average number of study product meals, and a higher study product intake;
- In Venus, the subjects in the later exclusive FF cluster introduced FF earlier and stopped BF later compared to TEMPO;
- In Venus, more subjects from the mostly BF cluster had some FF in the first 100 days compared to TEMPO. The mixed feeding episodes in this cluster tended to start later in Venus (at approximately 150–200 days of age) compared to TEMPO (at approximately 100 days of age)
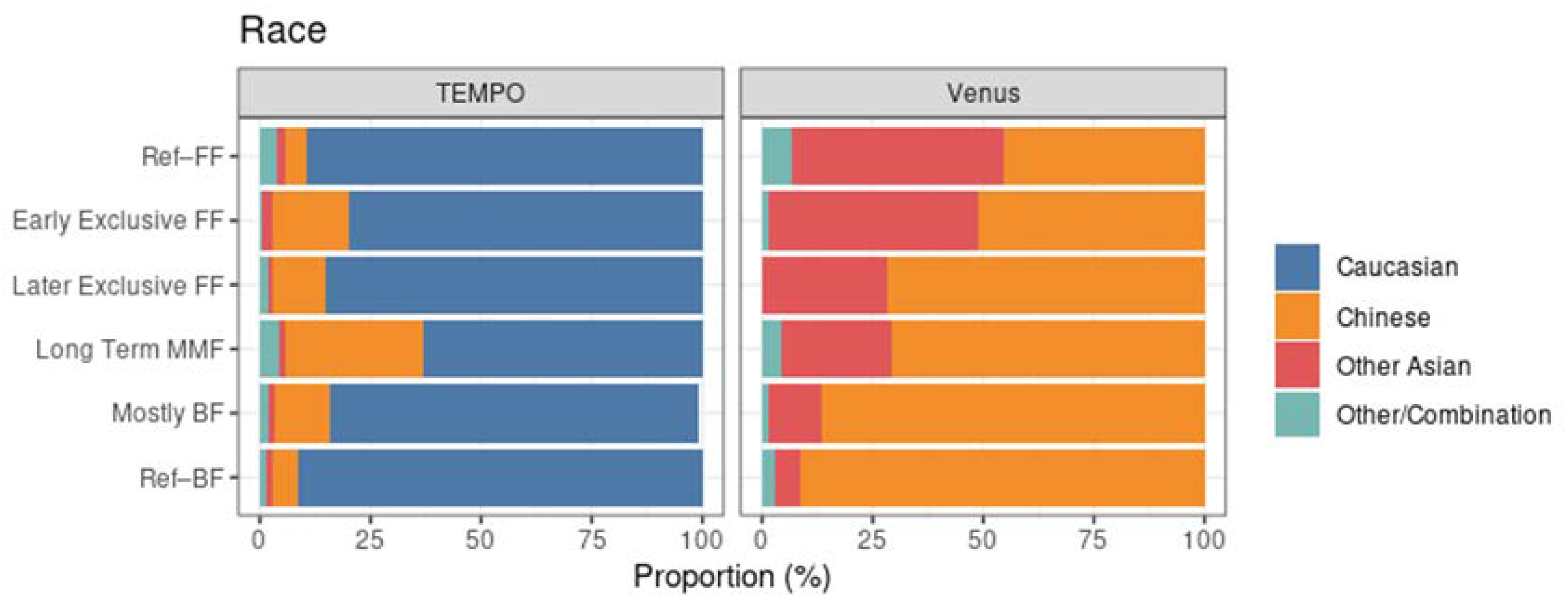
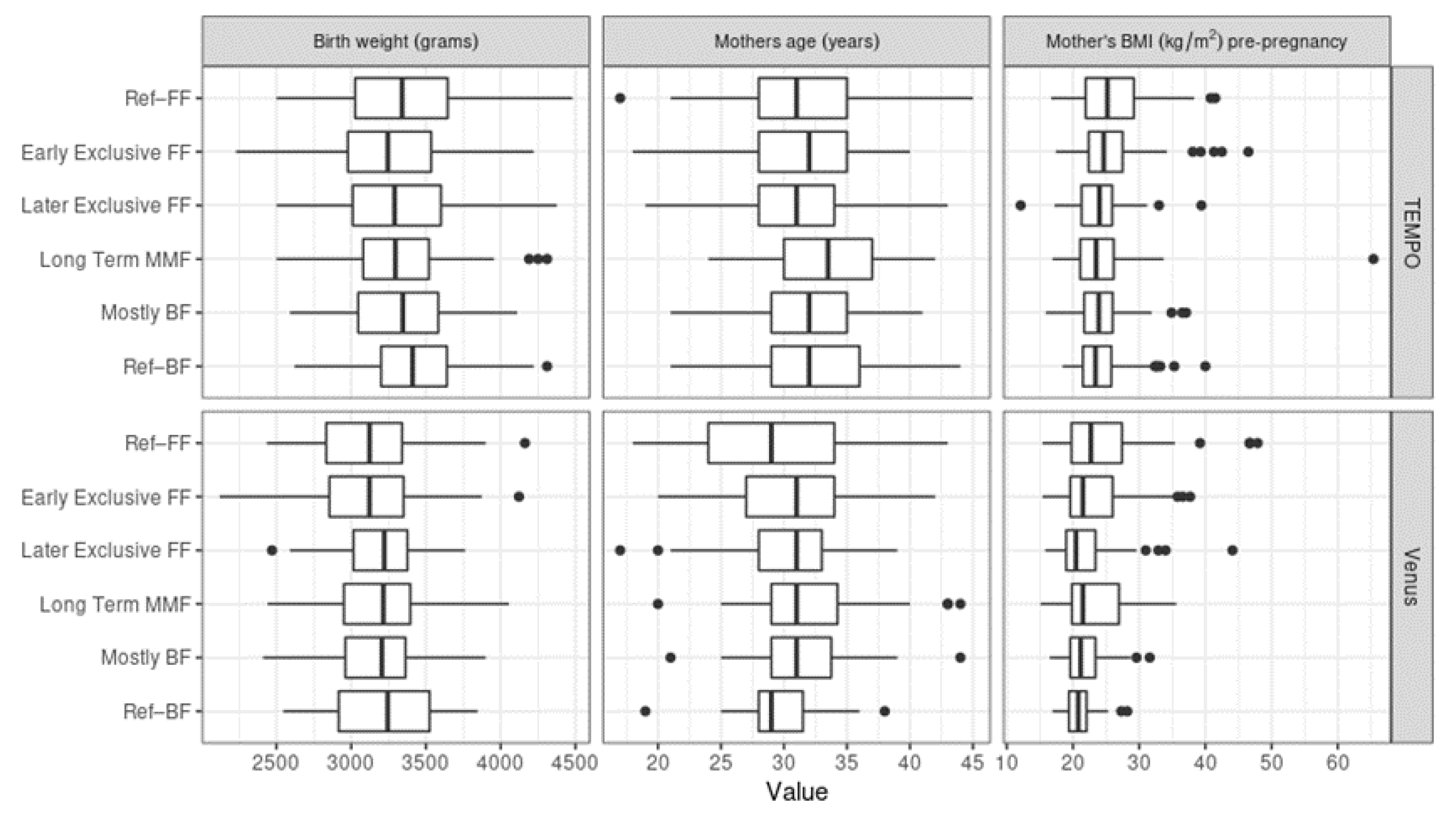
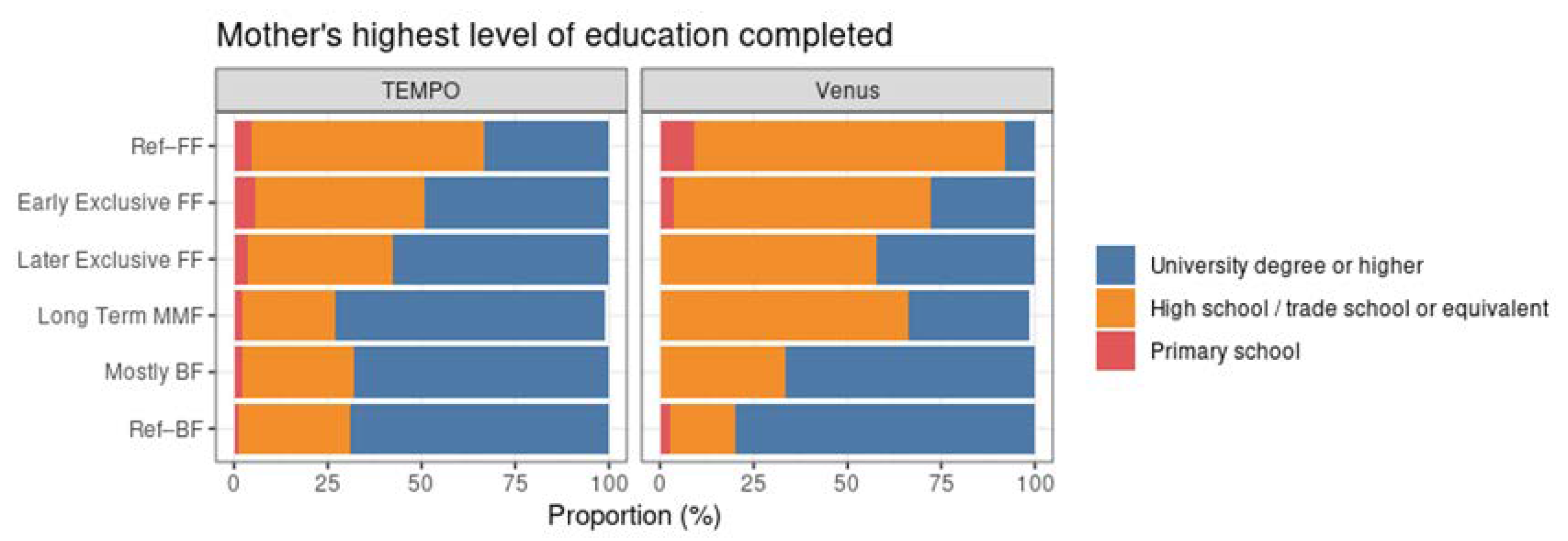
3.3. Baseline Variables and Their Association with MMF Clusters
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BF | Breastfeeding/breastfed |
| FF | formula feeding |
| MMF | Mixed milk Feeding |
| SP | Study product |
References
- Monge-Montero, C.; Van Der Merwe, L.F.; Papadimitropoulou, K.; Agostoni, C.; Vitaglione, P. Mixed milk feeding: A systematic review and meta-analysis of its prevalence and drivers. Nutr. Rev. 2020, 78, 914–927. [Google Scholar] [CrossRef]
- Indicators for Assessing Infant and Young Child Feeding Practices: Definitions and Measurement Methods. World Health Organization: Geneva, Switzerland. Available online: https://www.who.int/publications/i/item/9789240018389 (accessed on 30 April 2022).
- Thulier, D. A Call for Clarity in Infant Breast and Bottle-Feeding Definitions for Research. J. Obstet. Gynecol. Neonatal Nurs. 2010, 39, 627–634. [Google Scholar] [CrossRef]
- Holmes, A.V.; Auinger, P.; Howard, C.R. Combination Feeding of Breast Milk and Formula: Evidence for Shorter Breast-Feeding Duration from the National Health and Nutrition Examination Survey. J. Pediatr. 2011, 159, 186–191. [Google Scholar] [CrossRef]
- Neves, P.A.R.; Vaz, J.S.; Maia, F.S.; Baker, P.; Gatica-Domínguez, G.; Piwoz, E.; Rollins, N.; Victora, C.G. Rates and time trends in the consumption of breastmilk, formula, and animal milk by children younger than 2 years from 2000 to 2019: Analysis of 113 countries. Lancet Child Adolesc. Health 2021, 5, 619–630. [Google Scholar] [CrossRef]
- Neves, P.A.R.; Barros, A.J.D.; Gatica-Domínguez, G.; Vaz, J.S.; Baker, P.; Lutter, C.K. Maternal education and equity in breastfeeding: Trends and patterns in 81 low- and middle-income countries between 2000 and 2019. Int. J. Equity Health 2021, 20, 20. [Google Scholar] [CrossRef]
- Chung, S.-H.; Kim, H.-R.; Choi, Y.-S.; Bae, C.-W. Trends of Breastfeeding Rate in Korea (1994–2012): Comparison with OECD and Other Countries. J. Korean Med Sci. 2013, 28, 1573–1580. [Google Scholar] [CrossRef] [Green Version]
- The Optimal Duration of Exclusive Breastfeeding; Report of an Expert Consultation; World Health Organization: Geneva, Switzerland, 2001.
- Bowatte, G.; Tham, R.; Allen, K.J.; Tan, D.J.; Lau, M.; Dai, X.; Lodge, C.J. Breastfeeding and childhood acute otitis media: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Fisk, C.M.; Crozier, S.R.; Inskip, H.M.; Godfrey, K.M.; Cooper, C.; Roberts, G.C.; Robinson, S.M.; Southampton Women’s Survey Study Group. Breastfeeding and reported morbidity during infancy: Findings from the Southampton Women’s Survey. Matern. Child Nutr. 2011, 7, 61–70. [Google Scholar] [CrossRef]
- Grube, M.M.; von der Lippe, E.; Schlaud, M.; Brettschneider, A.K. Does breastfeeding help to reduce the risk of childhood overweight and obesity? A propensity score analysis of data from the KiGGS study. PLoS ONE 2015, 10, e0122534. [Google Scholar]
- Ip, S.; Chung, M.; Raman, G.; Chew, P.; Magula, N.; Devine, D.; Trikalinos, T.; Lau, J. Breastfeeding and maternal and infant health outcomes in developed countries. Évid. Rep. Technol. Assess. 2007, 153, 1–186. [Google Scholar]
- Lamberti, L.M.; Walker, C.L.F.; Noiman, A.; Victora, C.; Black, R.E. Breastfeeding and the risk for diarrhea morbidity and mortality. BMC Public Health 2011, 11, S15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sankar, M.J.; Sinha, B.; Chowdhury, R.; Bhandari, N.; Taneja, S.; Martines, J.C.; Bahl, R. Optimal breastfeeding practices and infant and child mortality: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Amitay, E.L.; Keinan-Boker, L. Breastfeeding and Childhood Leukemia Incidence: A Meta-analysis and Systematic Review. JAMA Pediatr. 2015, 169, e151025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, M.; Cameron, A.J.; Birken, C.S.; Keown-Stoneman, C.; Laws, R.; Wen, L.M.; Campbell, K.J. Early Infant Feeding and BMI Trajectories in the First 5 Years of Life. Obesity 2020, 28, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; Franca, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Norat, T.; Romundstad, P.R.; Vatten, L. Breastfeeding and the maternal risk of type 2 diabetes: A systematic review and dose–response meta-analysis of cohort studies. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 107–115. [Google Scholar] [CrossRef]
- Pinho-Gomes, A.; Morelli, G.; Jones, A.; Woodward, M. Association of lactation with maternal risk of type 2 diabetes: A systematic review and meta-analysis of observational studies. Diabetes, Obes. Metab. 2021, 23, 1902–1916. [Google Scholar] [CrossRef]
- Mezzacappa, E.S.; Katlin, E.S. Breast-feeding is associated with reduced perceived stress and negative mood in mothers. Health Psychol. 2002, 21, 187–193. [Google Scholar] [CrossRef]
- Papp, L.M. Longitudinal associations between breastfeeding and observed mother-child interaction qualities in early childhood. Child Care Health Dev. 2013, 40, 740–746. [Google Scholar] [CrossRef] [Green Version]
- Kramer, M.S.; Kakuma, R. Optimal Duration of Exclusive Breastfeeding. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2012. [Google Scholar] [CrossRef]
- Halken, S.; Muraro, A.; de Silva, D.; Khaleva, E.; Angier, E.; Arasi, S.; Arshad, H.; Bahnson, H.T.; Beyer, K.; Boyle, R.; et al. EAACI guideline: Preventing the development of food allergy in infants and young children (2020 update). Pediatr. Allergy Immunol. 2021, 32, 843–858. [Google Scholar] [CrossRef]
- United Nations Children’s Fund Organization UK. Guide to the Baby Friendly Initiative Standards. Available online: https://www.unicef.org.uk/babyfriendly/wp-content/uploads/sites/2/2014/02/Guide-to-the-Unicef-UK-Baby-Friendly-Initiative-Standards.pdf (accessed on 30 April 2022).
- Flaherman, V.J.; Aby, J.; Burgos, A.E.; Lee, K.A.; Cabana, M.D.; Newman, T.B. Effect of Early Limited Formula on Duration and Exclusivity of Breastfeeding in At-Risk Infants: An RCT. Pediatrics 2013, 131, 1059–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shek, L.P.; Chong, Y.S.; Winokan, A.; Abrahamse-Berkeveld, M.; Van Der Beek, E.M.; Teoh, O.H.; on behalf of the VENUS. Working Group Evaluation of an Infant Formula with Large, Milk-Phospholipid Coated Lipid Droplets on Long-Term Growth and Development of Singaporean Infants: Randomized Controlled Trial Protocol. Nutrients 2021, 13, 2865. [Google Scholar] [CrossRef] [PubMed]
- Genolini, C.; Pingault, J.; Driss, T.; Côté, S.; Tremblay, R.; Vitaro, F.; Arnaud, C.; Falissard, B. KmL3D: A non-parametric algorithm for clustering joint trajectories. Comput. Methods Programs Biomed. 2012, 109, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Genolini, C.; Alacoque, X.; Sentenac, M.; Arnaud, C. kml and kml3d: R packages to cluster longitudinal data. J. Stat. Softw. 2015, 65, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Janssen, P.A.; Thiessen, P.; Klein, M.C.; Whitfield, M.F.; MacNab, Y.C.; Cullis-Kuhl, S.C. Standards for the measurement of birth weight, length and head circumference at term in neonates of European, Chinese and South Asian ancestry. Open Med. 2007, 1, e74–e88. [Google Scholar]
- Madan, A.; Holland, S.; Humbert, J.E.; Benitz, W.E. Racial differences in birth weight of term infants in a northern California population. J. Perinatol. 2002, 22, 230–235. [Google Scholar] [CrossRef] [Green Version]
- Hanley, G.; Janssen, P.A. Ethnicity-Specific Growth Distributions for Prediction of Newborn Morbidity. J. Obstet. Gynaecol. Can. 2012, 34, 826–829. [Google Scholar] [CrossRef]
- Sarki, M.; Parlesak, A.; Robertson, A. Comparison of national cross-sectional breast-feeding surveys by maternal education in Europe (2006–2016). Public Health Nutr. 2018, 22, 848–861. [Google Scholar] [CrossRef] [Green Version]
- Pang, W.W.; Aris, I.M.; Fok, D.; Soh, S.E.; Chua, M.C.; Lim, S.B.; Saw, S.M.; Kwek, K.; Gluckman, P.D.; Godfrey, K.M.; et al. Determinants of breastfeeding practices and success in a multi-ethnic asian population. Birth 2016, 43, 68–77. [Google Scholar] [CrossRef]
- Whaley, S.E.; Meehan, K.; Lange, L.; Slusser, W.; Jenks, E. Predictors of breastfeeding duration for employees of the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). J. Am. Diet. Assoc. 2002, 102, 1290–1293. [Google Scholar] [CrossRef]
- HÖrnell, A.; Hofvander, Y.; Kylberg, E. Solids and Formula: Association with Pattern and Duration of Breastfeeding. Pediatrics 2001, 107, e38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howel, D.; Ball, H.L. Association between Length of Exclusive Breastfeeding and Subsequent Breastfeeding Continuation. J. Hum. Lact. 2013, 29, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Benn, C.S.; Wohlfahrt, J.; Aaby, P.; Westergaard, T.; Benfeldt, E.; Michaelsen, K.F.; Björkstén, B.; Melbye, M. Breastfeeding and Risk of Atopic Dermatitis, by Parental History of Allergy, during the First 18 Months of Life. Am. J. Epidemiol. 2004, 160, 217–223. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feeding Group | n | Percentage |
|---|---|---|
| Ref–BF | 141 | 16.5% |
| Ref–FF | 102 | 11.9% |
| MMF (>21 days MMF) | 432 | 50.5% |
| Short transition (<21 days MMF) | 92 | 10.8% |
| Follow up < 300 days | 88 | 10.3% |
| Total | 855 | 100% |
| Feeding Group | n | Percentage |
|---|---|---|
| Ref–BF | 35 | 6.5% |
| Ref–FF | 88 | 16.3% |
| MMF (>21 days MMF) | 335 | 62.2% |
| Short transition (<21 days MMF) | 30 | 5.6% |
| Follow up < 300 days | 16 | 3% |
| No feeding records | 35 | 6.5% |
| Total | 539 | 100% |
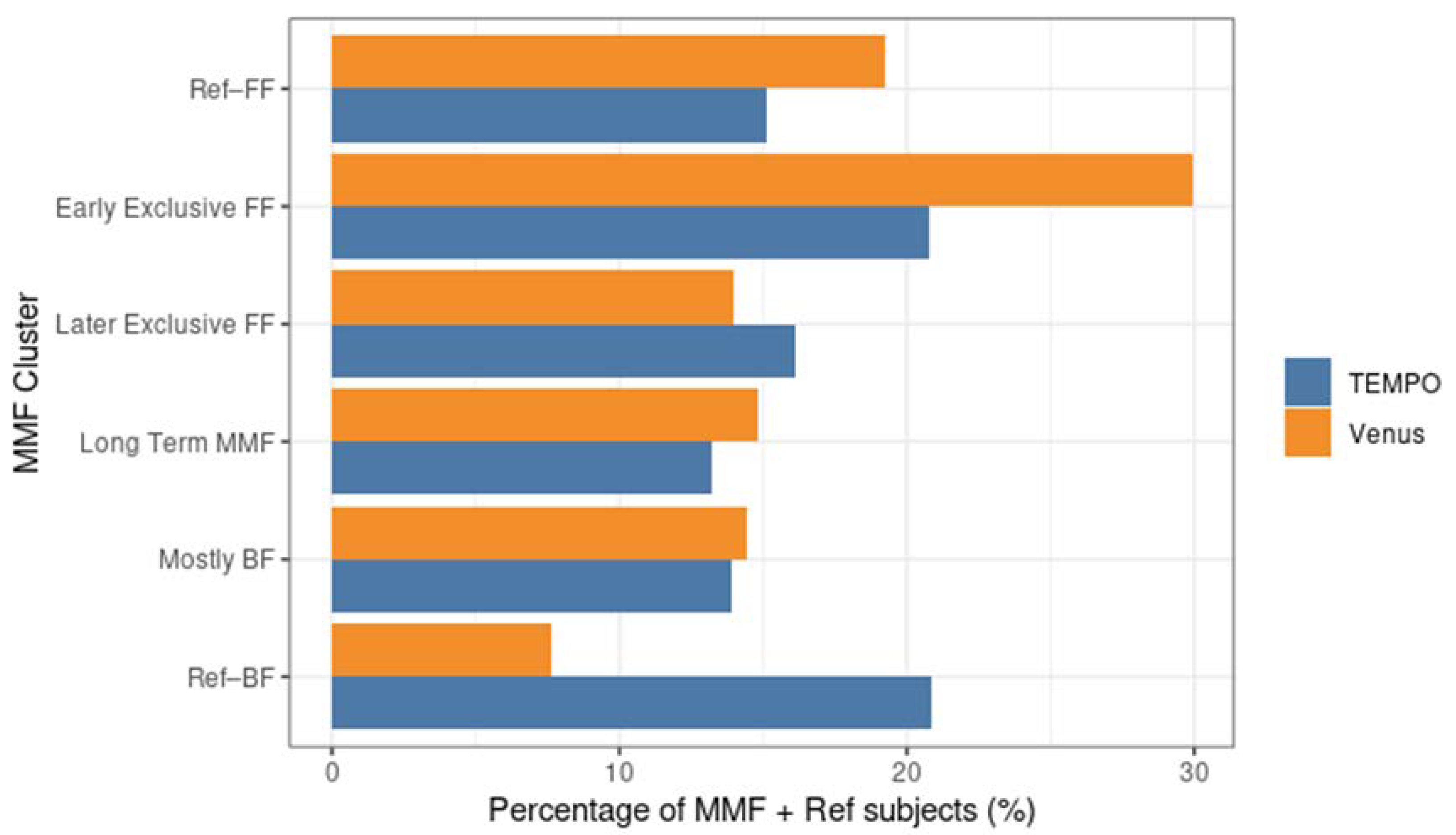
| MMF Cluster | n (TEMPO) | Percentage (TEMPO) | n (Venus) | Percentage (Venus) |
|---|---|---|---|---|
| Ref–BF | 141 | 20.9% | 35 | 7.6% |
| Mostly BF | 94 | 13.9% | 66 | 14.4% |
| Long-term MMF | 89 | 13.2% | 68 | 14.8% |
| Later exclusive FF | 109 | 16.1% | 64 | 14% |
| Early exclusive FF | 140 | 20.7% | 137 | 29.9% |
| Ref–FF | 102 | 15.1% | 88 | 19.2% |
| Total | 675 | 100% | 458 | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadopoulos, N.G.; Balan, T.A.; van der Merwe, L.F.; Pang, W.W.; Michaelis, L.J.; Shek, L.P.; Vandenplas, Y.; Teoh, O.H.; Fiocchi, A.G.; Chong, Y.S.; et al. Mixed Milk Feeding: A New Approach to Describe Feeding Patterns in the First Year of Life Based on Individual Participant Data from Two Randomised Controlled Trials. Nutrients 2022, 14, 2190. https://doi.org/10.3390/nu14112190
Papadopoulos NG, Balan TA, van der Merwe LF, Pang WW, Michaelis LJ, Shek LP, Vandenplas Y, Teoh OH, Fiocchi AG, Chong YS, et al. Mixed Milk Feeding: A New Approach to Describe Feeding Patterns in the First Year of Life Based on Individual Participant Data from Two Randomised Controlled Trials. Nutrients. 2022; 14(11):2190. https://doi.org/10.3390/nu14112190
Chicago/Turabian StylePapadopoulos, Nikolaos G., Theodor A. Balan, Liandre F. van der Merwe, Wei Wei Pang, Louise J. Michaelis, Lynette P. Shek, Yvan Vandenplas, Oon Hoe Teoh, Alessandro G. Fiocchi, Yap Seng Chong, and et al. 2022. "Mixed Milk Feeding: A New Approach to Describe Feeding Patterns in the First Year of Life Based on Individual Participant Data from Two Randomised Controlled Trials" Nutrients 14, no. 11: 2190. https://doi.org/10.3390/nu14112190
APA StylePapadopoulos, N. G., Balan, T. A., van der Merwe, L. F., Pang, W. W., Michaelis, L. J., Shek, L. P., Vandenplas, Y., Teoh, O. H., Fiocchi, A. G., Chong, Y. S., on behalf of the TEMPO Study Group, & on behalf of the Venus Study Group. (2022). Mixed Milk Feeding: A New Approach to Describe Feeding Patterns in the First Year of Life Based on Individual Participant Data from Two Randomised Controlled Trials. Nutrients, 14(11), 2190. https://doi.org/10.3390/nu14112190