
Cannabidiol and Cannabidiol Metabolites: Pharmacokinetics, Interaction with Food, and Influence on Liver Function

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
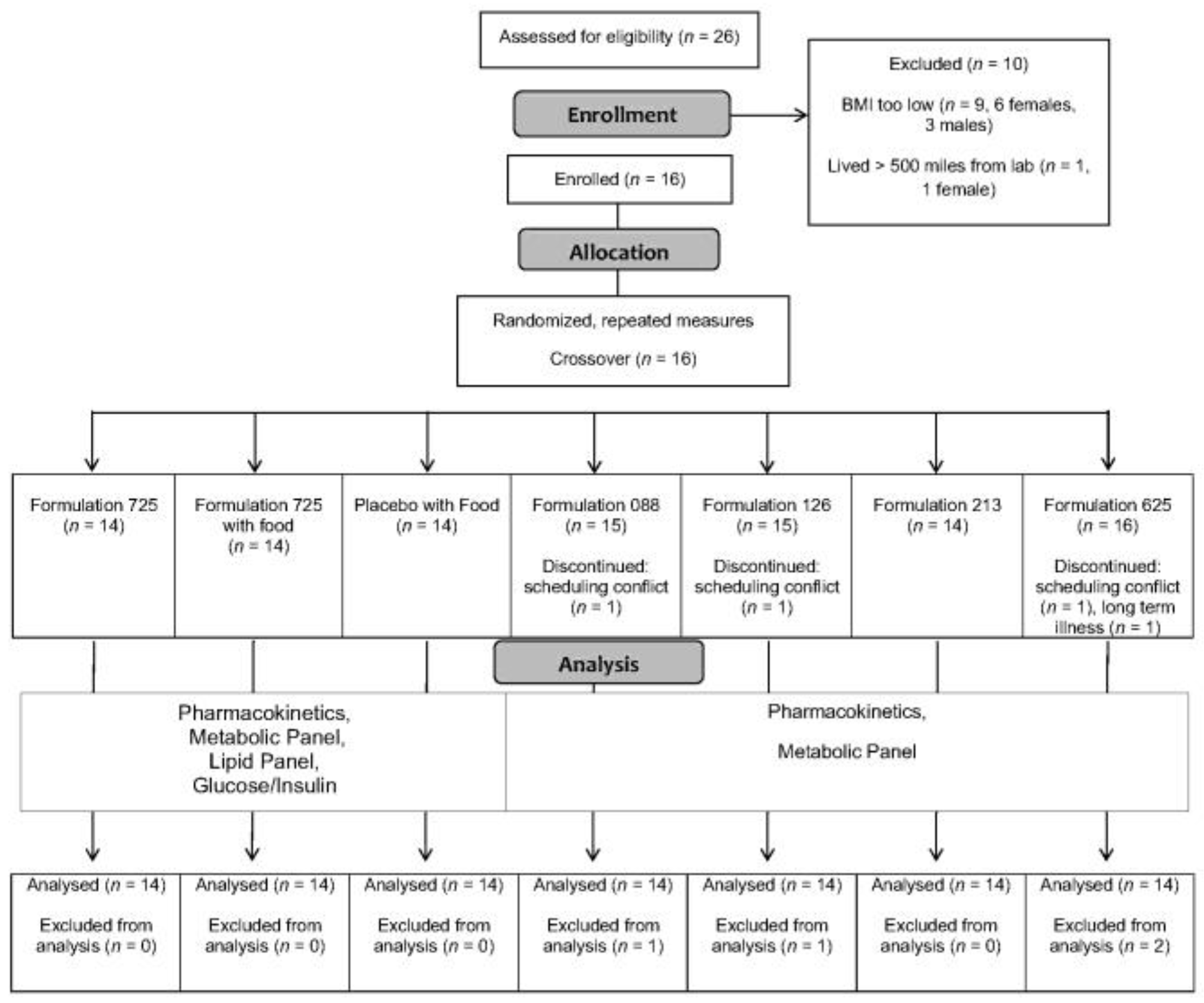
2.1. Participants
2.2. Protocol Overview
2.3. Procedures
2.4. CBD Preparations
2.5. Blood Handling and Analysis
2.6. CBD Reagents and Supplies
2.7. Calibrators, Quality Controls, and Internal Standard Preparation
2.8. CBD Analysis by Liquid Chromatography Tandem Mass Spectrometry (LC-MS/MS)
2.9. Pharmacokinetic Analysis
2.10. Statistical Analysis
3. Results
3.1. Participants
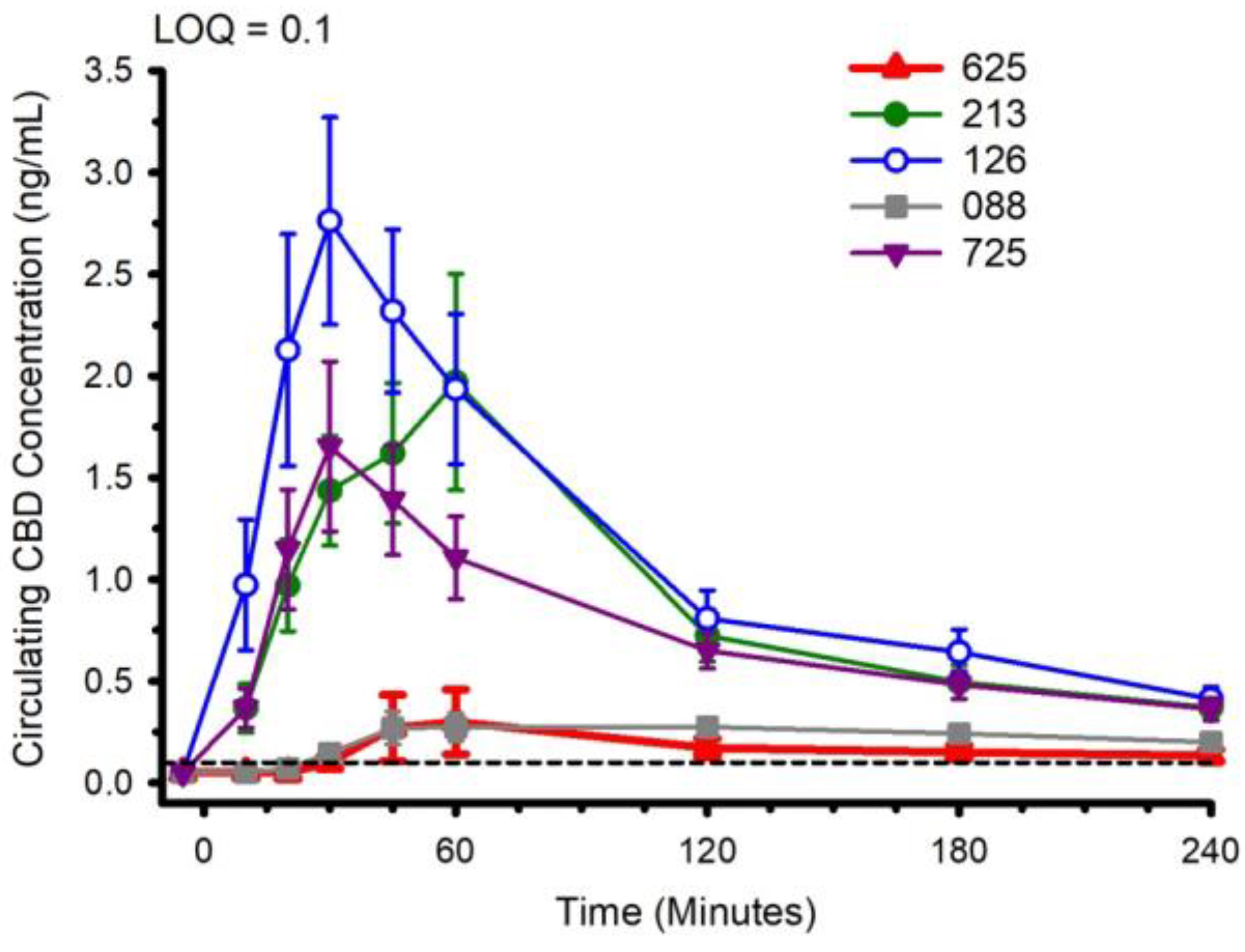
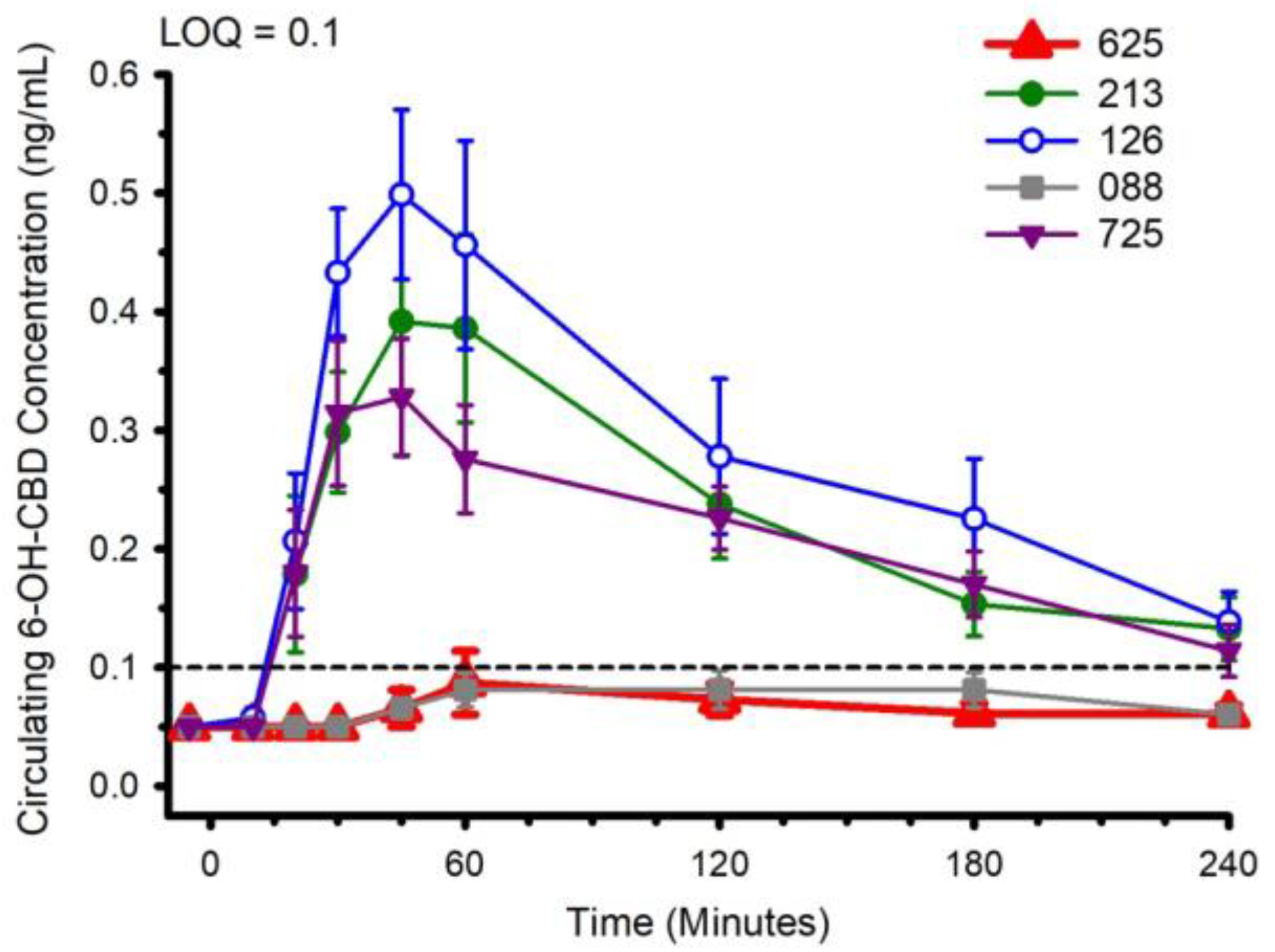
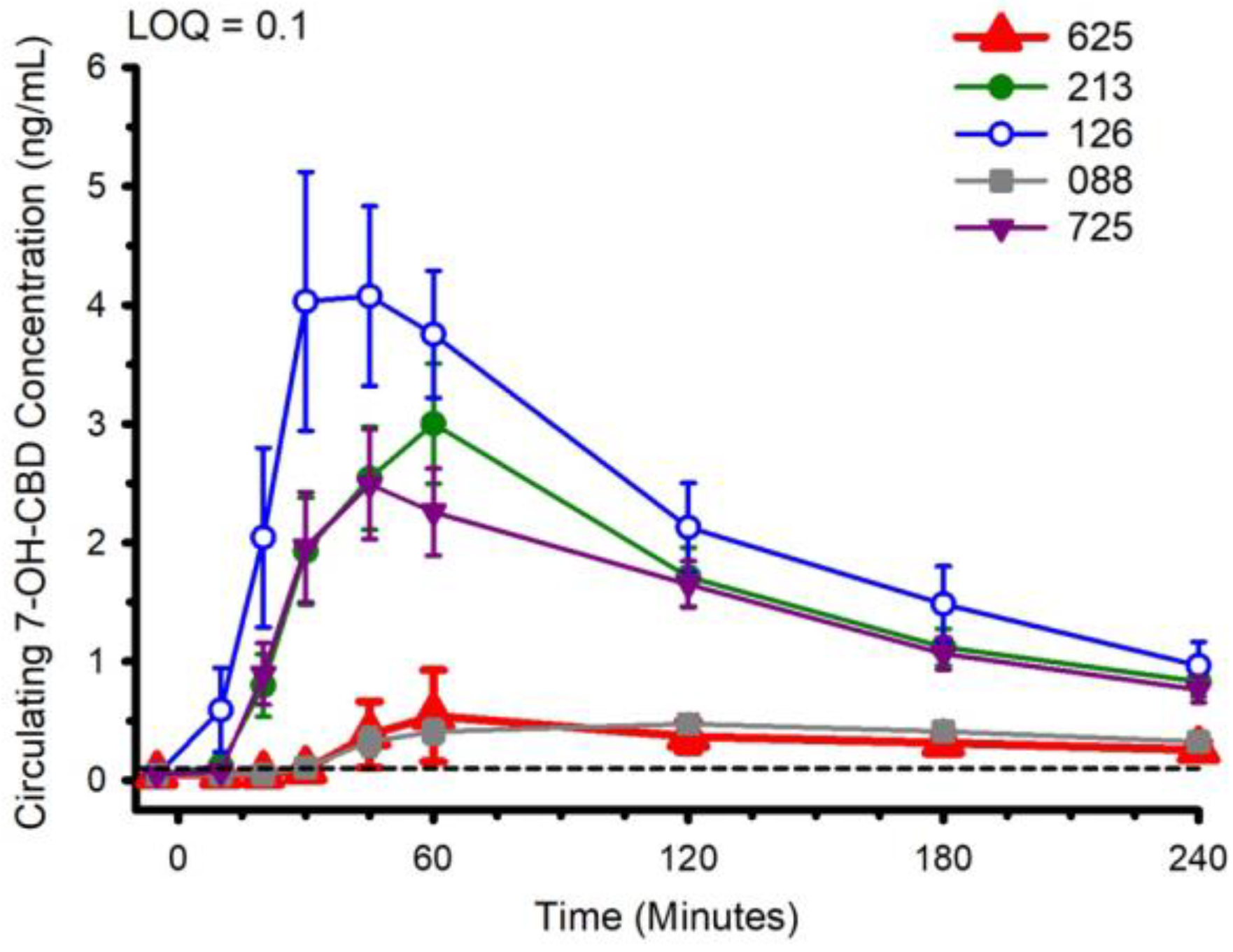
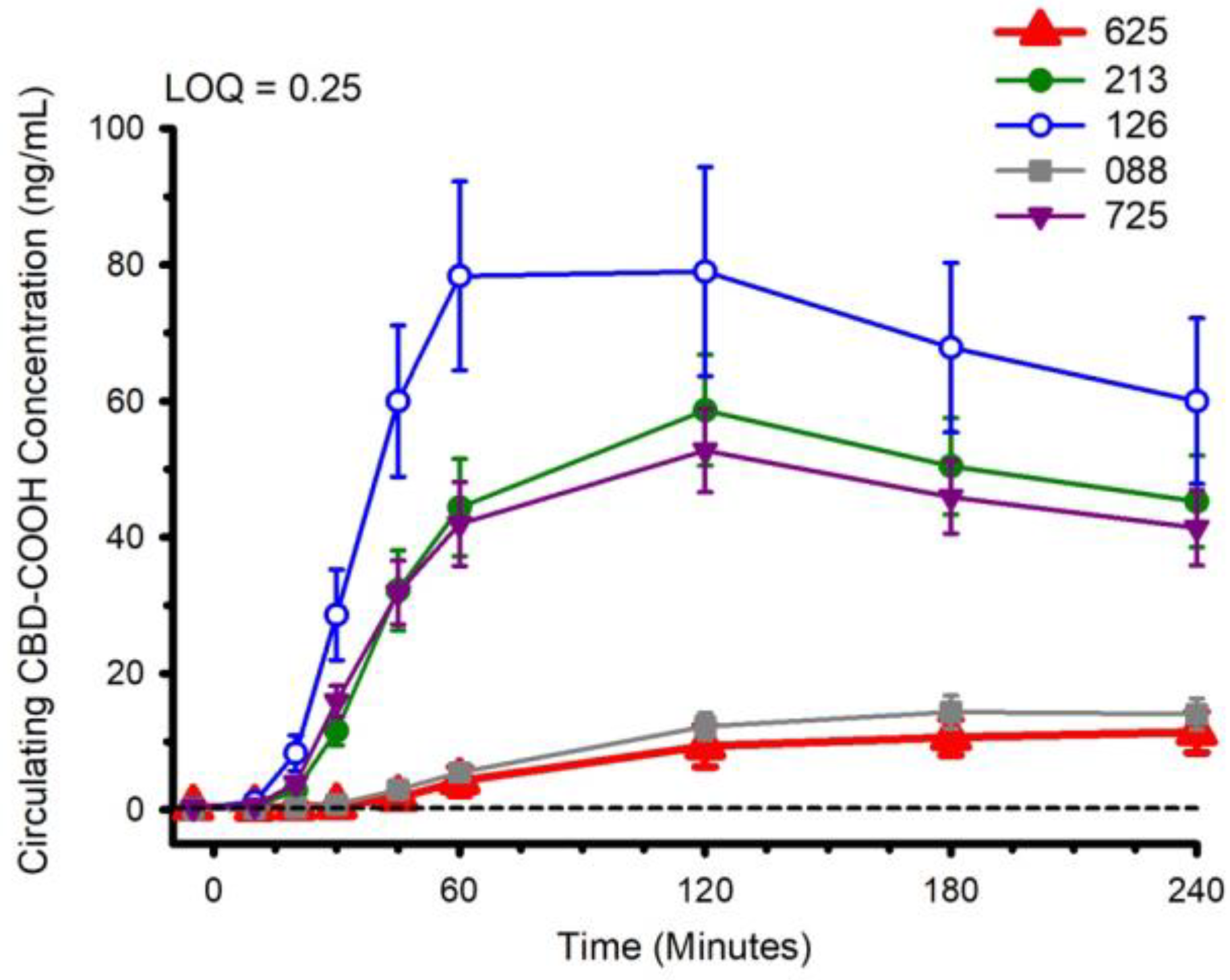
3.2. CBD, CBD Metabolites and Pharmacokinetics
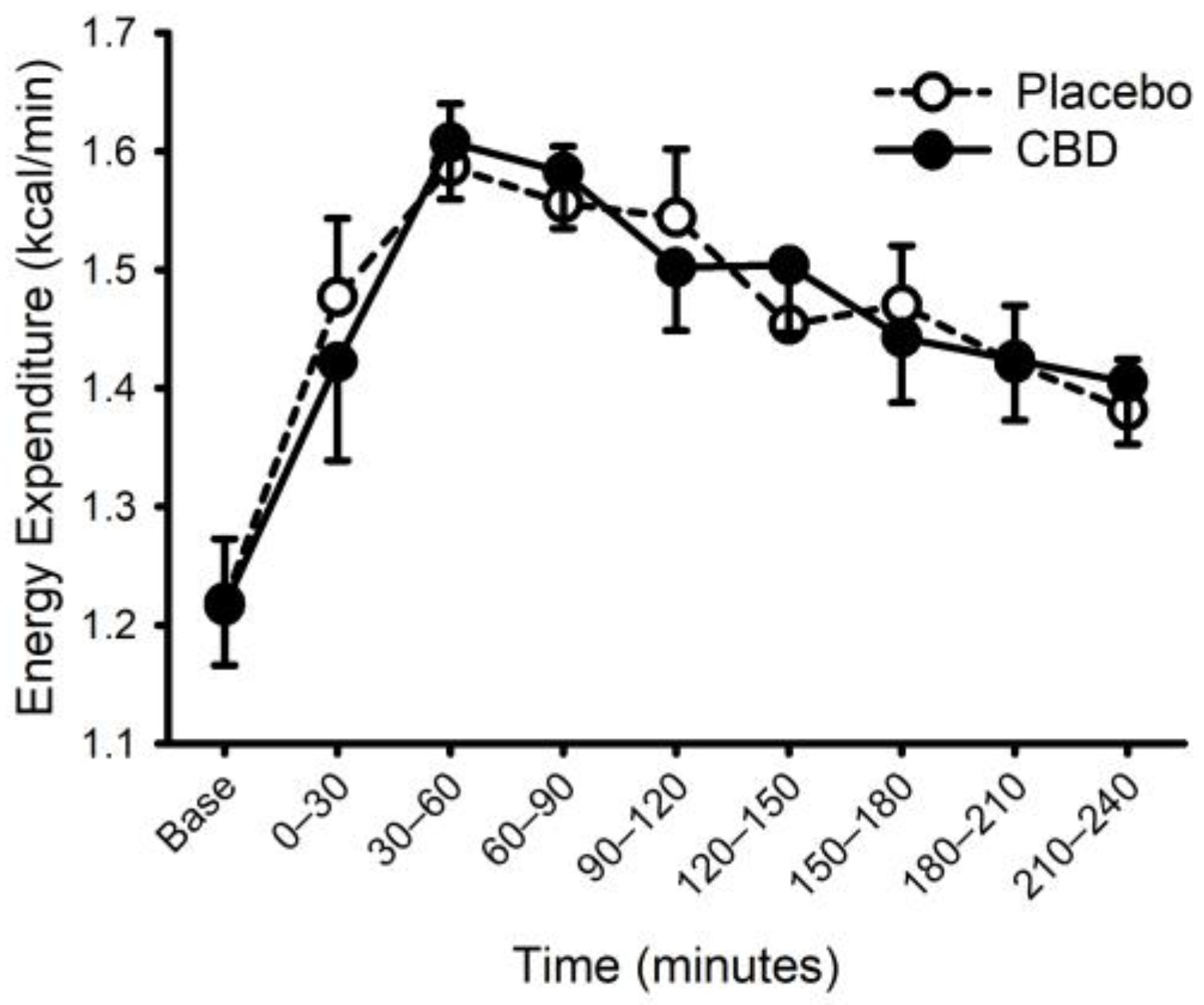
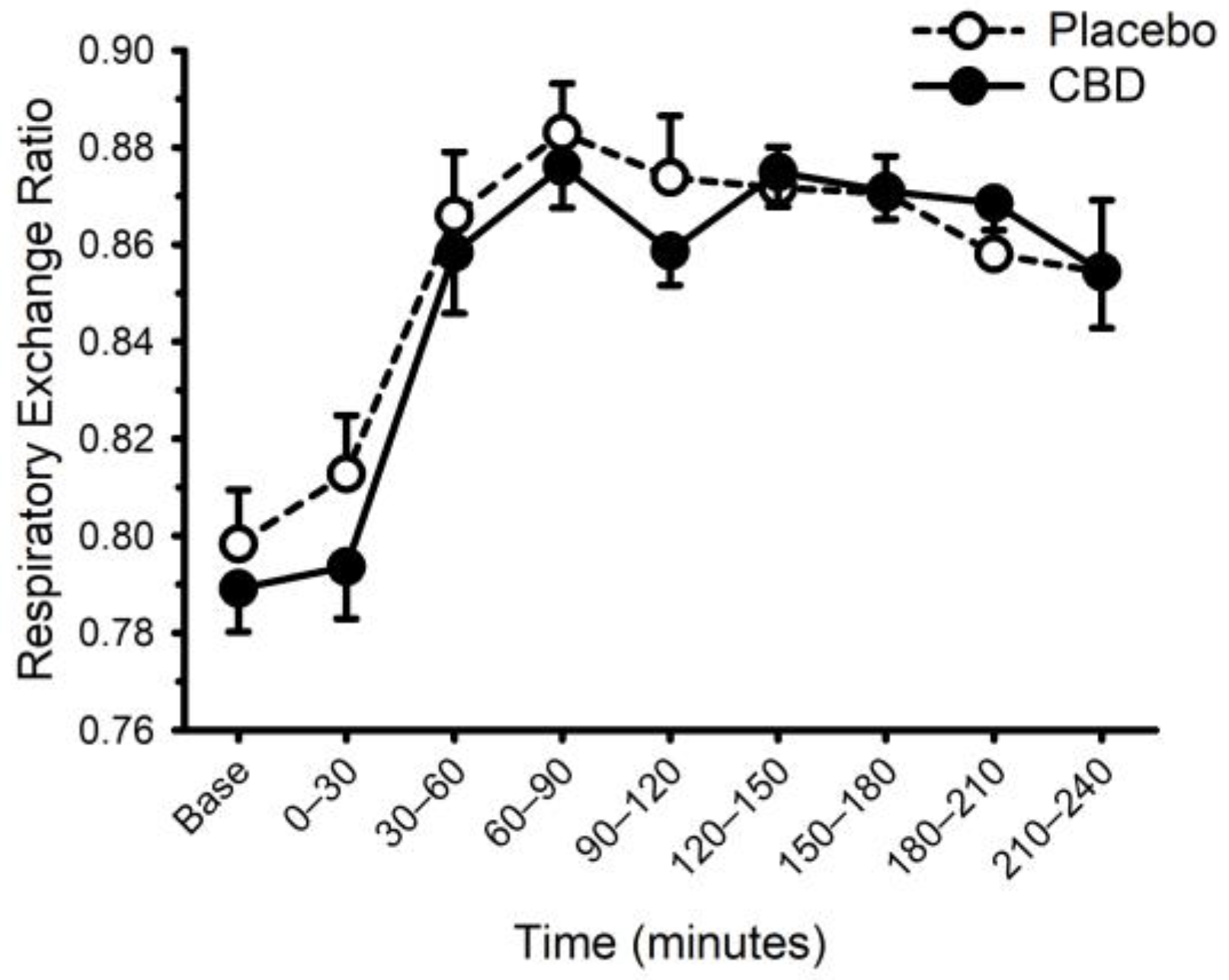
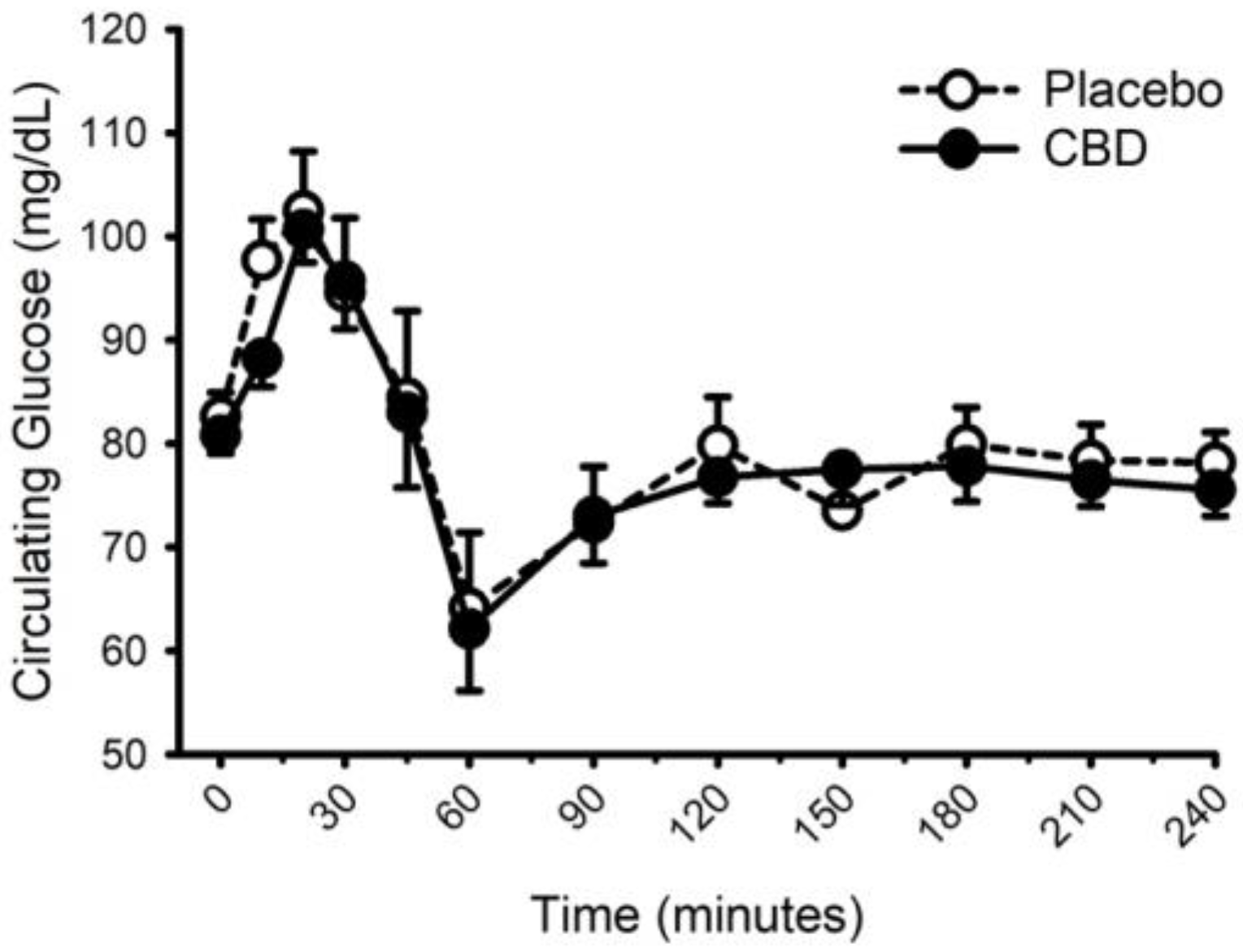
3.3. CBD and The Thermic Effect of Food
3.4. Influence of Food on the CBD Pharmacokinetics
3.5. Liver Function
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soleymanpour, M.; Saderholm, S.; Kavuluru, R. Therapeutic Claims in Cannabidiol (CBD) Marketing Messages on Twitter. In Proceedings of the 2021 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Houston, TX, USA, 9–12 December 2021; Volume 2021, pp. 3083–3088. [Google Scholar] [CrossRef]
- Sholler, D.J.; Schoene, L.; Spindle, T.R. Therapeutic Efficacy of Cannabidiol (CBD): A Review of the Evidence from Clinical Trials and Human Laboratory Studies. Curr. Addict. Rep. 2020, 7, 405–412. [Google Scholar] [CrossRef]
- Chesney, E.; McGuire, P.; Freeman, T.P.; Strang, J.; Englund, A. Lack of evidence for the effectiveness or safety of over-the-counter cannabidiol products. Ther. Adv. Psychopharmacol. 2020, 10, 2045125320954992. [Google Scholar] [CrossRef]
- Bruni, N.; Della Pepa, C.; Oliaro-Bosso, S.; Pessione, E.; Gastaldi, D.; Dosio, F. Cannabinoid Delivery Systems for Pain and Inflammation Treatment. Molecules 2018, 23, 2478. [Google Scholar] [CrossRef]
- Williams, N.N.B.; Ewell, T.R.; Abbotts, K.S.S.; Harms, K.J.; Woelfel, K.A.; Dooley, G.P.; Weir, T.L.; Bell, C. Comparison of Five Oral Cannabidiol Preparations in Adult Humans: Pharmacokinetics, Body Composition, and Heart Rate Variability. Pharmaceuticals 2021, 14, 35. [Google Scholar] [CrossRef]
- Millar, S.A.; Stone, N.L.; Yates, A.S.; O’Sullivan, S.E. A Systematic Review on the Pharmacokinetics of Cannabidiol in Humans. Front. Pharmacol. 2018, 9, 1365. [Google Scholar] [CrossRef]
- De Pra, M.A.A.; Vardanega, R.; Loss, C.G. Lipid-based formulations to increase cannabidiol bioavailability: In vitro digestion tests, pre-clinical assessment and clinical trial. Int. J. Pharm. 2021, 609, 121159. [Google Scholar] [CrossRef]
- Taylor, L.; Gidal, B.; Blakey, G.; Tayo, B.; Morrison, G. A Phase I, Randomized, Double-Blind, Placebo-Controlled, Single Ascending Dose, Multiple Dose, and Food Effect Trial of the Safety, Tolerability and Pharmacokinetics of Highly Purified Cannabidiol in Healthy Subjects. CNS Drugs 2018, 32, 1053–1067, Correction in CNS Drugs 2019, 33, 397. [Google Scholar] [CrossRef]
- Crockett, J.; Critchley, D.; Tayo, B.; Berwaerts, J.; Morrison, G. A phase 1, randomized, pharmacokinetic trial of the effect of different meal compositions, whole milk, and alcohol on cannabidiol exposure and safety in healthy subjects. Epilepsia 2020, 61, 267–277. [Google Scholar] [CrossRef]
- Abuhelwa, A.Y.; Williams, D.B.; Upton, R.N.; Foster, D.J. Food, gastrointestinal pH, and models of oral drug absorption. Eur. J. Pharm. Biopharm. 2017, 112, 234–248. [Google Scholar] [CrossRef]
- Franco, V.; Gershkovich, P.; Perucca, E.; Bialer, M. The Interplay Between Liver First-Pass Effect and Lymphatic Absorption of Cannabidiol and Its Implications for Cannabidiol Oral Formulations. Clin. Pharmacokinet. 2020, 59, 1493–1500. [Google Scholar] [CrossRef]
- Zgair, A.; Wong, J.C.; Lee, J.B.; Mistry, J.; Sivak, O.; Wasan, K.M.; Hennig, I.M.; Barrett, D.A.; Constantinescu, C.S.; Fischer, P.M.; et al. Dietary fats and pharmaceutical lipid excipients increase systemic exposure to orally administered cannabis and cannabis-based medicines. Am. J. Transl. Res. 2016, 8, 3448–3459. [Google Scholar]
- Collaboration, N.C.D.R.F. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Gammone, M.A.; D’Orazio, N. COVID-19 and Obesity: Overlapping of Two Pandemics. Obes. Facts 2021, 14, 579–585. [Google Scholar] [CrossRef]
- Rana, M.N.; Neeland, I.J. Adipose Tissue Inflammation and Cardiovascular Disease: An Update. Curr. Diab. Rep. 2022, 22, 27–37. [Google Scholar] [CrossRef]
- Bielawiec, P.; Harasim-Symbor, E.; Chabowski, A. Phytocannabinoids: Useful Drugs for the Treatment of Obesity? Special Focus on Cannabidiol. Front. Endocrinol. 2020, 11, 114. [Google Scholar] [CrossRef]
- Gruden, G.; Barutta, F.; Kunos, G.; Pacher, P. Role of the endocannabinoid system in diabetes and diabetic complications. Br. J. Pharmacol. 2016, 173, 1116–1127. [Google Scholar] [CrossRef]
- Schulz, P.; Hryhorowicz, S.; Rychter, A.M.; Zawada, A.; Slomski, R.; Dobrowolska, A.; Krela-Kazmierczak, I. What Role Does the Endocannabinoid System Play in the Pathogenesis of Obesity? Nutrients 2021, 13, 373. [Google Scholar] [CrossRef]
- Di Marzo, V. The endocannabinoid system in obesity and type 2 diabetes. Diabetologia 2008, 51, 1356–1367. [Google Scholar] [CrossRef]
- Thomas, A.; Baillie, G.L.; Phillips, A.M.; Razdan, R.K.; Ross, R.A.; Pertwee, R.G. Cannabidiol displays unexpectedly high potency as an antagonist of CB1 and CB2 receptor agonists in vitro. Br. J. Pharmacol. 2007, 150, 613–623. [Google Scholar] [CrossRef]
- Pertwee, R.G. The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: Δ9-tetrahydrocannabinol, cannabidiol and Δ9-tetrahydrocannabivarin. Br. J. Pharmacol. 2008, 153, 199–215. [Google Scholar] [CrossRef]
- Calcagno, M.; Kahleova, H.; Alwarith, J.; Burgess, N.N.; Flores, R.A.; Busta, M.L.; Barnard, N.D. The Thermic Effect of Food: A Review. J. Am. Coll. Nutr. 2019, 38, 547–551. [Google Scholar] [CrossRef]
- Goyal, H.; Rahman, M.R.; Perisetti, A.; Shah, N.; Chhabra, R. Cannabis in liver disorders: A friend or a foe? Eur. J. Gastroenterol. Hepatol. 2018, 30, 1283–1290. [Google Scholar] [CrossRef]
- Berk, K.; Bzdega, W.; Konstantynowicz-Nowicka, K.; Charytoniuk, T.; Zywno, H.; Chabowski, A. Phytocannabinoids-A Green Approach toward Non-Alcoholic Fatty Liver Disease Treatment. J. Clin. Med. 2021, 10, 393. [Google Scholar] [CrossRef] [PubMed]
- Watkins, P.B.; Church, R.J.; Li, J.; Knappertz, V. Cannabidiol and Abnormal Liver Chemistries in Healthy Adults: Results of a Phase I Clinical Trial. Clin. Pharmacol. Ther. 2021, 109, 1224–1231. [Google Scholar] [CrossRef]
- Hobbs, J.M.; Vazquez, A.R.; Remijan, N.D.; Trotter, R.E.; McMillan, T.V.; Freedman, K.E.; Wei, Y.; Woelfel, K.A.; Arnold, O.R.; Wolfe, L.M.; et al. Evaluation of pharmacokinetics and acute anti-inflammatory potential of two oral cannabidiol preparations in healthy adults. Phytother. Res. 2020, 34, 1696–1703. [Google Scholar] [CrossRef]
- Ewell, T.R.; Abbotts, K.S.S.; Williams, N.N.B.; Butterklee, H.M.; Bomar, M.C.; Harms, K.J.; Rebik, J.D.; Mast, S.M.; Akagi, N.; Dooley, G.P.; et al. Pharmacokinetic Investigation of Commercially Available Edible Marijuana Products in Humans: Potential Influence of Body Composition and Influence on Glucose Control. Pharmaceuticals 2021, 14, 817. [Google Scholar] [CrossRef]
- Newman, A.A.; Grimm, N.C.; Wilburn, J.R.; Schoenberg, H.M.; Trikha, S.R.J.; Luckasen, G.J.; Biela, L.M.; Melby, C.L.; Bell, C. Influence of Sodium Glucose Co-Transporter 2 Inhibition On The Physiological Adaptation to Endurance Exercise Training. J. Clin. Endocrinol. Metab. 2019, 104, 1953–1966. [Google Scholar] [CrossRef]
- Lonac, M.C.; Richards, J.C.; Schweder, M.M.; Johnson, T.K.; Bell, C. Influence of Short-Term Consumption of the Caffeine-free, Epigallocatechin-3-gallate Supplement, Teavigo, on Resting Metabolism and The Thermic Effect of Feeding. Obesity 2011, 19, 298–304. [Google Scholar] [CrossRef]
- Newsom, S.A.; Paxton, R.J.; Rynn, G.M.; Bell, C. Influence of ascorbic acid on the thermic effect of feeding in overweight and obese adult humans. Obesity 2008, 16, 1749–1754. [Google Scholar] [CrossRef]
- Weir, J. New methods for calculating metabolic rate with special reference to protein metabolism. J. Physiol. Lond. 1949, 109, 1–9. [Google Scholar] [CrossRef]
- Dash, R.P.; Srinivas, N.R.; Babu, R.J. Use of sorbitol as pharmaceutical excipient in the present day formulations-issues and challenges for drug absorption and bioavailability. Drug Dev. Ind. Pharm. 2019, 45, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Izgelov, D.; Shmoeli, E.; Domb, A.J.; Hoffman, A. The effect of medium chain and long chain triglycerides incorporated in self-nano emulsifying drug delivery systems on oral absorption of cannabinoids in rats. Int. J. Pharm. 2020, 580, 119201. [Google Scholar] [CrossRef]
- Luo, H.; Li, Z.; Yao, M.; McClements, D.J.; Xiao, H. Impact of excipient emulsions made from different types of oils on the bioavailability and metabolism of curcumin in gastrointestinal tract. Food Chem. 2022, 370, 130980. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, K.; Ishihara, K.; Ishida, M.; Watanabe, A.; Fujiwara, M.; Komatsu, Y.; Shirai, M.; Kato, Y.; Takanezawa, A.; Furuyashiki, T.; et al. Rapid rehydration and moderate plasma glucose elevation by fluid containing enzymatically synthesized glycogen. J. Nutr. Sci. Vitaminol. 2011, 57, 170–176. [Google Scholar] [CrossRef]
- Stob, N.R.; Bell, C.; van Baak, M.A.; Seals, D.R. Thermic effect of food and beta-adrenergic thermogenic responsiveness in habitually exercising and sedentary healthy adult humans. J. Appl. Physiol. 2007, 103, 616–622. [Google Scholar] [CrossRef][Green Version]
- Izgelov, D.; Davidson, E.; Barasch, D.; Regev, A.; Domb, A.J.; Hoffman, A. Pharmacokinetic investigation of synthetic cannabidiol oral formulations in healthy volunteers. Eur. J. Pharm. Biopharm. 2020, 154, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Knaub, K.; Sartorius, T.; Dharsono, T.; Wacker, R.; Wilhelm, M.; Schon, C. A Novel Self-Emulsifying Drug Delivery System (SEDDS) Based on VESIsorb((R)) Formulation Technology Improving the Oral Bioavailability of Cannabidiol in Healthy Subjects. Molecules 2019, 24, 2967. [Google Scholar] [CrossRef]
- Astray, G.; Mejuto, J.C.; Xiao, J.; Simal-Gandara, J. Benefits, toxicity and current market of cannabidiol in edibles. Crit. Rev. Food Sci. Nutr. 2022, 1–13. [Google Scholar] [CrossRef]
- Miller, O.S.; Elder, E.J., Jr.; Jones, K.J.; Gidal, B.E. Analysis of cannabidiol (CBD) and THC in nonprescription consumer products: Implications for patients and practitioners. Epilepsy Behav. 2022, 127, 108514. [Google Scholar] [CrossRef]
- Cujic-Nikolic, N.; Stanisavljevic, N.; Savikin, K.; Kalusevic, A.; Nedovic, V.; Samardzic, J.; Jankovic, T. Chokeberry polyphenols preservation using spray drying: Effect of encapsulation using maltodextrin and skimmed milk on their recovery following in vitro digestion. J. Microencapsul. 2019, 36, 693–703. [Google Scholar] [CrossRef]
- Rehrer, N.J.; Wagenmakers, A.J.; Beckers, E.J.; Halliday, D.; Leiper, J.B.; Brouns, F.; Maughan, R.J.; Westerterp, K.; Saris, W.H. Gastric emptying, absorption, and carbohydrate oxidation during prolonged exercise. J. Appl. Physiol. 1992, 72, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Ravussin, E.; Lillioja, S.; Knowler, W.C.; Christin, L.; Freymond, D.; Abbott, W.G.; Boyce, V.; Howard, B.V.; Bogardus, C. Reduced rate of energy expenditure as a risk factor for body-weight gain. N. Engl. J. Med. 1988, 318, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Van Zant, R.S. Influence of diet and exercise on energy expenditure—A review. Int. J. Sport Nutr. 1992, 2, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Granata, G.P.; Brandon, L.J. The thermic effect of food and obesity: Discrepant results and methodological variations. Nutr. Rev. 2002, 60, 223–233. [Google Scholar] [CrossRef]
- Jones, P.P.; Van Pelt, R.E.; Johnson, D.G.; Seals, D.R. Role of sympathetic neural activation in age- and habitual exercise-related differences in the thermic effect of food. J. Clin. Endocrinol. Metab. 2004, 89, 5138–5144. [Google Scholar] [CrossRef]
- Schwartz, R.S.; Jaeger, L.F.; Veith, R.C. The thermic effect of feeding in older men: The importance of the sympathetic nervous system. Metabolism 1990, 39, 733–737. [Google Scholar] [CrossRef]
- Bell, C.; Stob, N.R.; Seals, D.R. Thermogenic Responsiveness to {beta}-Adrenergic Stimulation is Augmented in Exercising versus Sedentary Adults: Role of Oxidative Stress. J. Physiol. 2006, 570, 629–653. [Google Scholar] [CrossRef]
- Chouchani, E.T.; Kajimura, S. Metabolic adaptation and maladaptation in adipose tissue. Nat. Metab. 2019, 1, 189–200. [Google Scholar] [CrossRef]
- Shin, S.; Ajuwon, K.M. Lipopolysaccharide Alters Thermogenic and Inflammatory Genes in White Adipose Tissue in Mice Fed Diets with Distinct 18-Carbon Fatty-Acid Composition. Lipids 2018, 53, 885–896. [Google Scholar] [CrossRef]
- Atalay, S.; Jarocka-Karpowicz, I.; Skrzydlewska, E. Antioxidative and Anti-Inflammatory Properties of Cannabidiol. Antioxidants 2019, 9, 21. [Google Scholar] [CrossRef]
- Zorzenon, M.R.T.; Santiago, A.N.; Mori, M.A.; Piovan, S.; Jansen, C.A.; Perina Padilha, M.E.; Ciotta, S.R.; Cezar de Freitas Mathias, P.; Guimaraes, F.S.; Weffort de Oliveira, R.M.; et al. Cannabidiol improves metabolic dysfunction in middle-aged diabetic rats submitted to a chronic cerebral hypoperfusion. Chem. Biol. Interact. 2019, 312, 108819. [Google Scholar] [CrossRef] [PubMed]
- Bielawiec, P.; Harasim-Symbor, E.; Konstantynowicz-Nowicka, K.; Sztolsztener, K.; Chabowski, A. Chronic Cannabidiol Administration Attenuates Skeletal Muscle De Novo Ceramide Synthesis Pathway and Related Metabolic Effects in a Rat Model of High-Fat Diet-Induced Obesity. Biomolecules 2020, 10, 1241. [Google Scholar] [CrossRef] [PubMed]
- Jadoon, K.A.; Ratcliffe, S.H.; Barrett, D.A.; Thomas, E.L.; Stott, C.; Bell, J.D.; O’Sullivan, S.E.; Tan, G.D. Efficacy and Safety of Cannabidiol and Tetrahydrocannabivarin on Glycemic and Lipid Parameters in Patients With Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled, Parallel Group Pilot Study. Diabetes Care 2016, 39, 1777–1786. [Google Scholar] [CrossRef]
- Gabbay, E.; Avraham, Y.; Ilan, Y.; Israeli, E.; Berry, E.M. Endocannabinoids and liver disease—Review. Liver Int. 2005, 25, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Devinsky, O.; Cross, J.H.; Laux, L.; Marsh, E.; Miller, I.; Nabbout, R.; Scheffer, I.E.; Thiele, E.A.; Wright, S.; Cannabidiol in Dravet Syndrome Study, G. Trial of Cannabidiol for Drug-Resistant Seizures in the Dravet Syndrome. N. Engl. J. Med. 2017, 376, 2011–2020. [Google Scholar] [CrossRef] [PubMed]
- Devinsky, O.; Patel, A.D.; Cross, J.H.; Villanueva, V.; Wirrell, E.C.; Privitera, M.; Greenwood, S.M.; Roberts, C.; Checketts, D.; VanLandingham, K.E.; et al. Effect of Cannabidiol on Drop Seizures in the Lennox-Gastaut Syndrome. N. Engl. J. Med. 2018, 378, 1888–1897. [Google Scholar] [CrossRef] [PubMed]
- Thiele, E.A.; Marsh, E.D.; French, J.A.; Mazurkiewicz-Beldzinska, M.; Benbadis, S.R.; Joshi, C.; Lyons, P.D.; Taylor, A.; Roberts, C.; Sommerville, K.; et al. Cannabidiol in patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE4): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2018, 391, 1085–1096. [Google Scholar] [CrossRef]
- Miller, I.; Scheffer, I.E.; Gunning, B.; Sanchez-Carpintero, R.; Gil-Nagel, A.; Perry, M.S.; Saneto, R.P.; Checketts, D.; Dunayevich, E.; Knappertz, V.; et al. Dose-Ranging Effect of Adjunctive Oral Cannabidiol vs Placebo on Convulsive Seizure Frequency in Dravet Syndrome: A Randomized Clinical Trial. JAMA Neurol. 2020, 77, 613–621. [Google Scholar] [CrossRef]
- Kaufmann, R.; Aqua, K.; Lombardo, J.; Lee, M. Observed Impact of Long-term Consumption of Oral Cannabidiol on Liver Function in Healthy Adults. Cannabis Cannabinoid Res. 2021. [Google Scholar] [CrossRef]
- Mohr, A.E.; Ramos, C.; Tavarez, K.; Arciero, P.J. Lower Postprandial Thermogenic Response to an Unprocessed Whole Food Meal Compared to an Iso-Energetic/Macronutrient Meal Replacement in Young Women: A Single-Blind Randomized Cross-Over Trial. Nutrients 2020, 12, 2469. [Google Scholar] [CrossRef]
- Li, J.; Carvajal, R.; Bruner, L.; Kaminski, N.E. The current understanding of the benefits, safety, and regulation of cannabidiol in consumer products. Food Chem. Toxicol. 2021, 157, 112600. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | Description |
|---|---|
| 725 | Water soluble. Contains sorbitol. |
| 088 | Not water soluble. Contains medium chain triglyceride coconut oil. |
| 126 | Water soluble. Contains gum arabic and maltodextrin |
| 213 | Water soluble. Contains gum arabic and sorbitol |
| 625 | Not water soluble. Pure CBD as crystalline powder (>99% purity) |
| Variable | Mean ± SD | Range |
|---|---|---|
| Age (years) | 26 ± 8 | 20–51 |
| Height (cm) | 176 ± 6 | 166–185 |
| Body Mass (kg) | 93.2 ± 12.8 | 72.8–120.9 |
| Body Mass Index (kg/m2) | 29.7 ± 2.8 | 25.8–35.2 |
| Fat Mass (kg) | 26.9 ± 65 | 15.4–37.4 |
| % Body Fat | 28.6 ± 4.7 | 20.7–38.0 |
| Lean Mass (kg) | 63.7 ± 8.3 | 52.2–80.4 |
| Parameter | 088 | 126 | 213 | 625 | 725 | |
|---|---|---|---|---|---|---|
| Tmax (min) | Mean SD Median Range n | 116.3 b,c,e 76.0 90.0 45–240 12 | 35.4 *,b 13.5 30.0 20–60 14 | 51.8 d,e 24.2 52.5 20–120 14 | 129.5 *,a,d 89.6 60 45–240 11 | 38.2 a,c 24.9 30.0 20–120 14 |
| Cmax (ng/mL) | Mean SD Median Range n | 0.5 a,c 0.2 0.5 0.2–1.0 12 | 3.1 *,a,e 2.1 2.8 0.8–7.1 14 | 2.2 b,c 2.0 1.5 0.5–7.8 14 | 0.4 *,b,d 0.6 0.2 0.13–2.33 11 | 1.8 d,e 1.5 1.2 0.7–6.2 14 |
| AUC0–4 (min × ng/mL) | Mean SD Median Range n | 62.8 a,c,e 29.7 59.0 14.4–108.6 12 | 272.3 *,a,f 176.0 238.1 82.5–602.5 14 | 208.6 b,c 151.1 153.0 67.6–582.9 14 | 46.0 *,b,d 59.4 28.9 4.2–210.7 11 | 177.3 d,e,f 104.8 146.4 87.1–433.3 14 |
| AUC0–inf (min × ng/mL) | Mean SD Median Range n | - - - - - | 385.2 226.6 319.6 93.8–676.0 6 | 367.6 217.1 285.6 163.7–704.1 5 | - - - - - | 301.6 221.9 301.6 144.7–458.5 2 |
| t½ (min) | Mean SD Median Range n | 280.7 141.5 245.7 151.5–523.4 5 | 171.0 129.2 113.2 55.4–464.9 14 | 140.5 96.6 106.4 80.0–415.9 11 | 442.7 451.0 200.7 164.2–963.1 3 | 133.1 26.7 128.7 94.6–181.8 13 |
| ke (1/h) | Mean SD Median n | 0.003 0.001 0 5 | 0.006 0.003 0.010 14 | 0.006 0.002 0.01 11 | 0.003 0.002 0.000 3 | 0.005 0.001 0.010 13 |
| Vd (mL) | Mean SD Median n | - - - - | 11836405 7642484 11901025 6 | 13130100 6339554 14091985 5 | - - - - | 22687960 16435999 22687960 2 |
| Parameter | 088 | 126 | 213 | 625 | 725 | |
|---|---|---|---|---|---|---|
| Tmax (min) | Mean SD Median Range n | 120.0 c,d,e 69.3 120.0 60–240 7 | 45.0 *,c 13.2 45.0 30–60 14 | 66.4 b,e 30.4 60.0 30–120 14 | 144.0 *,a,b 91.0 120.0 60–240 5 | 50.4 a,d 30.9 45.0 30–120 14 |
| Cmax (ng/mL) | Mean SD Median Range n | 0.2 *,c,d 0.1 0.2 0.1–0.3 7 | 0.6 *,a,b 0.3 0.5 0.3–1.5 14 | 0.5 c 0.4 0.3 0.2–1.8 14 | 0.2 a,e 0.1 0.2 0.1–0.4 5 | 0.4 b,d,e 0.2 0.4 0.1–0.9 14 |
| AUC0–4 (min × ng/mL) | Mean SD Median Range n | 18.0 *,c,e 9.4 16.6 3.4–31.3 7 | 65.1 *,a,b 49.0 52.1 9.3–209.7 14 | 51.3 c,d 40.6 40.3 6.7–157.1 14 | 18.4 a,d,f 11.9 16.0 6.2–37.7 5 | 45.3 b,e,f 27.0 44.2 5.7–90.3 14 |
| AUC0–inf (min × ng/mL) | Mean SD Median Range n | - - - - - | 240.3 - 240.3 240.3 1 | 126.6 68.7 126.6 78.0–175.2 2 | - - - - - | - - - - - |
| t½ (min) | Mean SD Median Range n | - - - - - | 175.1 141.4 118.7 68.8–543.3 11 | 195.0 130.7 143.2 62.6–380.22 7 | - - - - - | 186.7 88.3 161.4 81.0–390.0 10 |
| Ke (1/h) | Mean SD Median n | - - - - | 0.006 0.003 0.010 11 | 0.005 0.004 0.000 7 | - - - - | 0.004 0.002 0.000 10 |
| Vd (mL) | Mean SD Median n | - - - - | 12396095 - 12396095 1 | 31161801 22199818 31161801 2 | - - - - | - - - - |
| Parameter | 088 | 126 | 213 | 625 | 725 | |
|---|---|---|---|---|---|---|
| Tmax (min) | Mean SD Median Range n | 110.4 c,d,e,f 58.1 120 45–240 14 | 60.0 b,f 42.0 52.5 30–180 14 | 58.9 a,e 19.9 60 30–120 14 | 156.9 *,a,b,c 67.3 120.0 60–240 13 | 55.7 *,d 20.7 52.5 30–120 14 |
| Cmax (ng/mL) | Mean SD Median Range n | 0.62 a,e,g 0.38 0.54 0.2–1.3 14 | 4.89 *,a,b,c 3.78 3.91 1.8–16.0 14 | 3.14 c,d,e 1.82 2.48 0.8–6.4 14 | 0.71 *,d,f 1.45 0.26 0.1–5.5 13 | 2.73 b,f,g 1.64 2.27 1.0–6.3 14 |
| AUC0–4 (min × ng/mL) | Mean SD Median Range n | 88.8 a,e,g 53.1 84.4 22.0–172.2 14 | 523.6 *,a,b,c 350.1 392.6 184.3–1389.7 14 | 380.1 c,d,e 208.7 295.7 100.9–782.7 14 | 81.0 *,d,f 132.5 43.0 8.0–506.3 13 | 343.9 b,f,g 174.3 292.0 139.2–706.0 14 |
| AUC0–inf (min × ng/mL) | Mean SD Median Range n | - - - - | 598.2 391.7 487.8 216.9–1244.1 5 | 584.1 208.7 586.4 314.3–893.0 5 | - - - - | 531.1 207.1 455.1 372.8–765.5 3 |
| t½ (min) | Mean SD Median Range n | 368.9 407.9 200.4 98.9–975.9 4 | 108.1 38.6 94.8 62.5–177.6 12 | 132.4 75.9 117.7 70.1–360.3 13 | 163.6 57.6 163.6 122.8–204.3 2 | 109.6 25.0 104.4 78.2–166.8 13 |
| Ke (1/h) | Mean SD Median n | 0.004 0.003 0.000 4 | 0.007 0.002 0.010 12 | 0.006 0.002 0.010 13 | 0.005 0.002 0.000 2 | 0.007 0.001 0.010 13 |
| Vd (mL) | Mean SD Median n | - - - - | 7361772 4728622 6678818 5 | 6506682 2353415 6593583 5 | - - - - | 8096154 3862326 7746967 3 |
| Parameter | 088 | 126 | 213 | 625 | 725 | |
|---|---|---|---|---|---|---|
| Tmax (min) | Mean SD Median Range n | 175.7 c,d,e,f 49.7 180.0 120–240 14 | 93.2 *,d 40.0 90.0 45–180 14 | 111.4 b,f 32.1 120.0 60–180 14 | 210.0 *,a,b,c 45.6 240.0 120–240 14 | 111.4 a,e 32.1 120.0 60–180 14 |
| Cmax (ng/mL) | Mean SD Median Range n | 15.6 a,f 9.1 14.4 3.6–33.4 14 | 86.7 *,a,b,c 58.2 72.3 21.1–249.7 14 | 59.3 c,d 29.8 51.4 11.7–118.7 14 | 12.2 *,d,e 11.8 7.4 1.2–42.9 14 | 53.8 b,e,f 22.9 51.6 13.4–108.4 14 |
| AUC0–4 (min × ng/mL) | Mean SD Median Range n | 2284.9 a,e,g 1361.2 2276.1 547–5275 14 | 14907.4 *,a,b,c 10354.6 12327.3 3778–43275 14 | 10233.4 c,d,e 5421.8 8900.2 2127–23257 14 | 1743.7 *,d,f 1907.4 974.0 183–7126 14 | 9457.3 b,f,g 4263.4 7923.3 2432–20208 14 |
| AUC0–inf (min × ng/mL) | Mean SD Median Range n | - - - - - | - - - - - | - - - - - | - - - - - | - - - - - |
| t½ (min) | Mean SD Median Range n | - - - - - | 408.6 292.0 296.4 154.9–981.1 7 | 385.8 150.1 431.4 218.2–507.9 3 | - - - - - | 282.5 26.6 267.8 266.4–313.2 3 |
| Ke (1/h) | Mean SD Median n | - - - - | 0.002 0.001 0.000 7 | 0.002 0.001 0.000 3 | - - - - | 0.002 0.000 0.000 3 |
| Vd (mL) | Mean SD Median n | - - - - | - - - - | - - - - | - - - - | - - - - |
| Formula | Time min | Ca mg/dL | BUN mg/dL | CRE mg/dL | ALP U/L | ALT U/L | AST U/L | TBIL mg/dL | ALB g/dL | TP g/dL |
|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | 0 | 9.4 | 15.1 | 1.1 | 62.1 | 26.1 | 28.0 | 0.8 | 3.6 | 6.5 |
| ±0.6 | ±2.7 | ±0.2 | ±8.6 | ±10.1 | ±12.3 | ±0.3 | ±0.3 | ±0.5 | ||
| 60 | 9.4 | 14.6 | 1.1 | 62.9 | 26.9 | 30.7 | 0.8 | 3.6 | 6.6 | |
| ±0.5 | ±2.9 | ±0.2 | ±9.8 | ±10.8 | ±10.4 | ±0.3 | ±0.2 | ±0.5 | ||
| 240 | 9.3 | 13.9 | 1.1 | 58.8 | 26.0 | 29.4 | 0.8 | 3.4 | 6.3 | |
| ±0.5 | ±2.5 | ±0.3 | ±8.5 | ±11.2 | ±10.1 | ±0.3 | ±0.3 | ±0.4 | ||
| 625 | 0 | 9.3 | 15.0 | 1.1 | 61.9 | 30.5 | 30.6 | 0.9 | 3.8 | 6.7 |
| ±0.5 | ±3.6 | ±0.2 | ±9.4 | ±11.2 | ±7.3 | ±0.2 | ±0.3 | ±0.6 | ||
| 60 | 9.5 | 14.8 | 1.1 | 61.6 | 30.4 | 31.4 | 0.9 | 3.8 | 6.8 | |
| ±0.4 | ±3.9 | ±0.3 | ±9.3 | ±11.0 | ±7.4 | ±0.2 | ±0.2 | ±0.4 | ||
| 240 | 9.1 | 13.8 | 1.1 | 62.3 | 30.7 | 31.9 | 1.0 | 4.0 | 7.0 | |
| ±2.2 | ±3.7 | ±0.2 | ±9.2 | ±11.5 | ±7.5 | ±0.3 | ±0.2 | ±0.7 | ||
| 088 | 0 | 8.9 | 14.6 | 1.1 | 62.5 | 28.0 | 30.5 | 1.0 | 3.9 | 6.8 |
| ±2.2 | ±2.8 | ±0.2 | ±7.9 | ±10.9 | ±4.1 | ±0.3 | ±0.3 | ±0.3 | ||
| 60 | 9.6 | 14.4 | 1.2 | 60.5 | 27.9 | 30.6 | 0.9 | 3.8 | 6.7 | |
| ±0.4 | ±2.8 | ±0.2 | ±7.2 | ±10.0 | ±4.6 | ±0.2 | ±0.3 | ±0.4 | ||
| 240 | 9.7 | 13.4 | 1.2 | 60.2 | 28.6 | 31.1 | 1.0 | 3.9 | 6.9 | |
| ±0.5 | ±2.5 | ±0.2 | ±8.0 | ±10.6 | ±6.8 | ±0.2 | ±0.3 | ±0.6 | ||
| 213 | 0 | 9.3 | 15.4 | 1.2 | 60.3 | 29.0 | 33.5 | 1.0 | 3.8 | 6.7 |
| ±0.5 | ±3.9 | ±0.2 | ±6.8 | ±10.6 | ±7.0 | ±0.4 | ±0.3 | ±0.5 | ||
| 60 | 9.4 | 15.5 | 1.1 | 61.0 | 29.1 | 30.9 | 1.0 | 3.8 | 6.7 | |
| ±0.4 | ±4.1 | ±0.4 | ±8.7 | ±9.8 | ±5.1 | ±0.4 | ±0.2 | ±0.3 | ||
| 240 | 9.5 | 14.3 | 1.1 | 62.1 | 28.7 | 30.4 | 1.1 | 3.9 | 6.8 | |
| ±0.3 | ±3.5 | ±0.3 | ±9.5 | ±10.5 | ±5.9 | ±0.4 | ±0.2 | ±0.3 | ||
| 126 | 0 | 9.4 | 15.4 | 1.1 | 63.6 | 27.5 | 30.2 | 1.0 | 3.9 | 6.8 |
| ±0.3 | ±4.5 | ±0.2 | ±10.8 | ±8.4 | ±3.4 | ±0.6 | ±0.2 | ±0.2 | ||
| 60 | 9.5 | 15.1 | 1.2 | 61.9 | 29.3 | 29.4 | 1.0 | 3.8 | 6.7 | |
| ±0.5 | ±4.6 | ±0.3 | ±11.0 | ±8.1 | ±8.7 | ±0.6 | ±0.3 | ±0.4 | ||
| 240 | 9.5 | 14.0 | 1.1 | 61.4 | 28.2 | 30.3 | 1.1 | 3.9 | 6.8 | |
| ±0.4 | ±4.2 | ±0.3 | ±9.6 | ±7.9 | ±4.1 | ±0.6 | ±0.3 | ±0.3 | ||
| 725 | 0 | 9.4 | 15.9 | 1.1 | 60.4 | 27.7 | 29.2 | 0.9 | 3.8 | 6.8 |
| ±0.4 | ±3.3 | ±0.3 | ±12.0 | ±9.1 | ±5.0 | ±0.4 | ±0.3 | ±0.4 | ||
| 60 | 9.6 | 15.3 | 1.1 | 60.9 | 27.3 | 28.9 | 0.9 | 3.8 | 6.7 | |
| ±0.2 | ±3.3 | ±0.1 | ±11.4 | ±8.7 | ±4.3 | ±0.4 | ±0.2 | ±0.3 | ||
| 240 | 8.9 | 14.1 | 1.0 | 61.0 | 27.6 | 29.6 | 1.0 | 3.9 | 6.9 | |
| ±2.3 | ±3.1 | ±0.2 | ±12.6 | ±9.8 | ±4.4 | ±0.4 | ±0.2 | ±0.4 | ||
| p-Value | CBD | 0.964 | 0.765 | 0.836 | 0.863 | 0.462 | 0.810 | 0.022 | <0.001 | 0.010 |
| Time | 0.370 | <0.001 | 0.483 | 0.480 | 0.425 | 0.979 | <0.001 | 0.052 | 0.291 | |
| Inter. | 0.417 | 0.368 | 0.163 | 0.358 | 0.614 | 0.230 | <0.001 | 0.002 | 0.058 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abbotts, K.S.S.; Ewell, T.R.; Butterklee, H.M.; Bomar, M.C.; Akagi, N.; Dooley, G.P.; Bell, C. Cannabidiol and Cannabidiol Metabolites: Pharmacokinetics, Interaction with Food, and Influence on Liver Function. Nutrients 2022, 14, 2152. https://doi.org/10.3390/nu14102152
Abbotts KSS, Ewell TR, Butterklee HM, Bomar MC, Akagi N, Dooley GP, Bell C. Cannabidiol and Cannabidiol Metabolites: Pharmacokinetics, Interaction with Food, and Influence on Liver Function. Nutrients. 2022; 14(10):2152. https://doi.org/10.3390/nu14102152
Chicago/Turabian StyleAbbotts, Kieran Shay Struebin, Taylor Russell Ewell, Hannah Michelle Butterklee, Matthew Charles Bomar, Natalie Akagi, Gregory P. Dooley, and Christopher Bell. 2022. "Cannabidiol and Cannabidiol Metabolites: Pharmacokinetics, Interaction with Food, and Influence on Liver Function" Nutrients 14, no. 10: 2152. https://doi.org/10.3390/nu14102152
APA StyleAbbotts, K. S. S., Ewell, T. R., Butterklee, H. M., Bomar, M. C., Akagi, N., Dooley, G. P., & Bell, C. (2022). Cannabidiol and Cannabidiol Metabolites: Pharmacokinetics, Interaction with Food, and Influence on Liver Function. Nutrients, 14(10), 2152. https://doi.org/10.3390/nu14102152