
Longitudinal Association of Dietary Energy Density with Abdominal Obesity among Chinese Adults from CHNS 1993–2018


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Data
2.3. Definition of DED and Abdominal Obesity
2.4. Assessment of Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics by the Quartile of DED
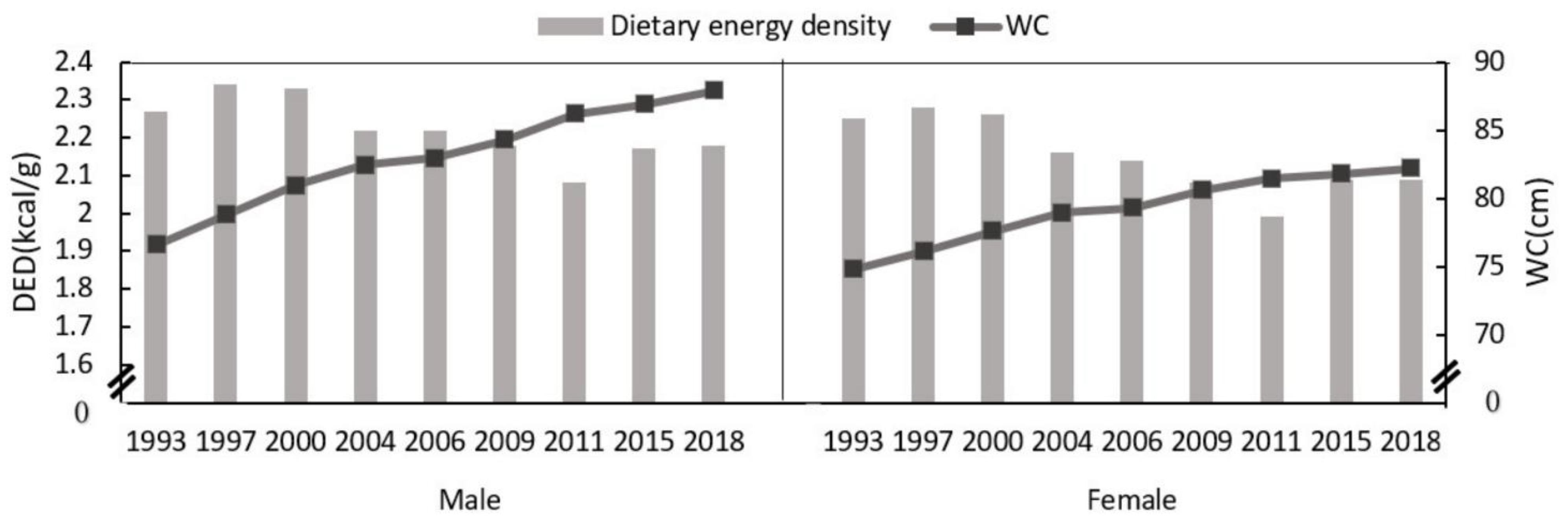
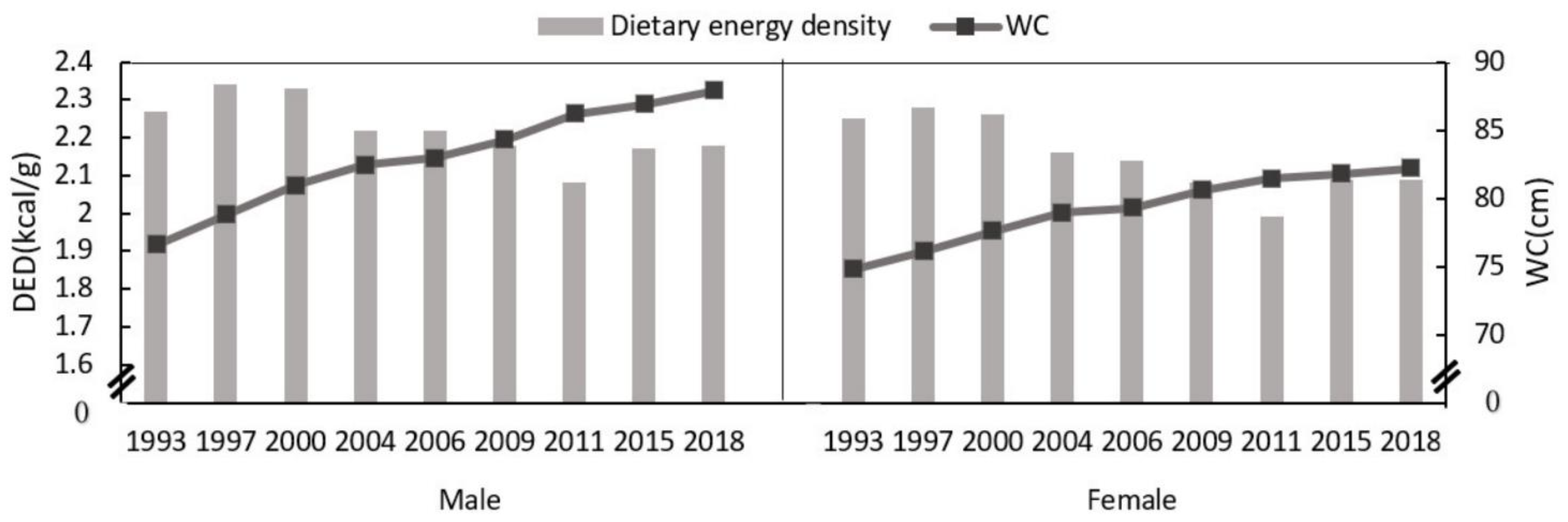
3.2. Changes in DED and Waist Circumference in Males and Females from 1993 to 2018
3.3. Association between DED and Waist Circumference in Subjects Aged 18–64 from 1993 to 2018
3.4. Association between DED and Abdominal Obesity in Subjects Aged 18–64 from 1993 to 2018
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wan, H.; Wang, Y.; Xiang, Q.; Fang, S.; Chen, Y.; Chen, C.; Zhang, W.; Zhang, H.; Xia, F.; Wang, N.; et al. Associations between abdominal obesity indices and diabetic complications: Chinese visceral adiposity index and neck circumference. Cardiovasc. Diabetol. 2020, 19, 118. [Google Scholar] [CrossRef] [PubMed]
- Niu, J.; Seo, D.C. Central obesity and hypertension in Chinese adults: A 12-year longitudinal examination. Prev. Med. 2014, 62, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Maynard, L.M.; Li, C. Trends in mean waist circumference and abdominal obesity among US adults, 1999–2012. JAMA 2014, 312, 1151–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Peng, Q.; Yang, Y.; Zheng, S.; Wang, Y.; Lu, W. The prevalence and increasing trends of overweight, general obesity, and abdominal obesity among Chinese adults: A repeated cross-sectional study. BMC Public Health 2019, 19, 1293. [Google Scholar] [CrossRef] [Green Version]
- Stookey, J.D. Energy density, energy intake and weight status in a large free-living sample of Chinese adults: Exploring the underlying roles of fat, protein, carbohydrate, fiber and water intakes. Eur. J. Clin. Nutr. 2001, 55, 349–359. [Google Scholar] [CrossRef] [Green Version]
- Bes-Rastrollo, M.; Dam, R.M.v.; Martinez-Gonzalez, M.A.; Li, T.Y.; Sampson, L.L.; Hu, F.B. Prospective study of dietary energy density and weight gain in women. Am. J. Clin. Nutr. 2008, 88, 769–777. [Google Scholar] [CrossRef]
- Drewnowski, A.; Almiron-Roig, E.; Marmonier, C.; Lluch, A. Dietary Energy Density and Body Weight: Is There a Relationship? Nutr. Rev. 2004, 62, 403–413. [Google Scholar] [CrossRef]
- Howarth, N.C.; Murphy, S.P.; Wilkens, L.R.; Hankin, J.H.; Kolonel, L.N. Dietary energy density is associated with overweight status among 5 ethnic groups in the multiethnic cohort study. J. Nutr. 2006, 136, 2243–2248. [Google Scholar] [CrossRef] [Green Version]
- Zhu, S.; Wang, Z.; Heshka, S.; Heo, M.; Faith, M.S.; Heymsfield, S.B. Waist circumference and obesity-associated risk factors among whites in the third National Health and Nutrition Examination Survey: Clinical action thresholds. Am. J. Clin. Nutr. 2002, 76, 743–749. [Google Scholar] [CrossRef]
- Goh, V.H.H.; Hart, W.G. Excess fat in the abdomen but not general obesity is associated with poorer metabolic and cardiovascular health in premenopausal and postmenopausal Asian women. Maturitas 2018, 107, 33–38. [Google Scholar] [CrossRef]
- Schroder, H.; Mendez, M.A.; Gomez, S.F.; Fito, M.; Ribas, L.; Aranceta, J.; Serra-Majem, L. Energy density, diet quality, and central body fat in a nationwide survey of young Spaniards. Nutrition 2013, 29, 1350–1355. [Google Scholar] [CrossRef] [PubMed]
- Bazshahi, E.; Pourreza, S.; Imani, H.; Azadbakht, L.; Ebaditabar, M.; Davarzani, S.; Babaei, N.; Naghshi, S.; Djafarian, K.; Shab-Bidar, S. The Association of Dietary Energy Density and Body Composition Components in a Sample of Iranian Adults. Front. Nutr. 2021, 8, 751148. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Xue, H.; Chen, Y.; Zhang, X.; Quan, L.; Gong, Y.; Cheng, G. Dietary energy density is positively associated with body composition of adults in Southwest China. Public Health Nutr. 2018, 21, 1827–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Zhai, F.Y.; Du, S.F.; Popkin, B.M. The China Health and Nutrition Survey, 1989–2011. Obes. Rev. 2014, 15 (Suppl. S1), 2–7. [Google Scholar] [CrossRef] [Green Version]
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort Profile: The China Health and Nutrition Survey--monitoring and understanding socio-economic and health change in China, 1989–2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [Green Version]
- Jiang, H.; Zhang, J.; Du, W.; Su, C.; Zhang, B.; Wang, H. Energy intake and energy contributions of macronutrients and major food sources among Chinese adults: CHNS 2015 and CNTCS 2015. Eur. J. Clin. Nutr. 2021, 75, 314–324. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, B.; Zhai, F.; Wang, H.; Zhang, J.; Du, W.; Su, C.; Zhang, J.; Jiang, H.; Popkin, B.M. Fatty and lean red meat consumption in China: Differential association with Chinese abdominal obesity. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 869–876. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Wang, G.; Pan, X. China Food Composition; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Rolls, B.J. Plenary Lecture 1: Dietary strategies for the prevention and treatment of obesity. Proc. Nutr. Soc. 2010, 69, 70–79. [Google Scholar] [CrossRef] [Green Version]
- Coorperative Meta-analysis Group of China Obesity Task Force. Predictive values of body mass index and waist cirumferene to risk factors of related diseases in Chinese adult population. Zhong Hua Liu Xing Bing Xue Za Zhi 2002, 23, 10–15. [Google Scholar]
- Su, C.; Song, X.; Hu, H.; Du, W.; Wang, H.; Zhang, B. Longitudinal Association between Urbanicity and Total Dietary Fat Intake in Adults in Urbanizing China from 1991 to 2015: Findings from the CHNS. Nutrients 2020, 12, 1597. [Google Scholar] [CrossRef]
- Kant, A.K.; Graubard, B.I. Secular trends in patterns of self-reported food consumption of adult Americans: NHANES 1971–1975 to NHANES 1999–2002. Am. J. Clin. Nutr. 2006, 84, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Barton, K.L.; Wrieden, W.L.; Sherriff, A.; Armstrong, J.; Anderson, A.S. Energy density of the Scottish diet estimated from food purchase data: Relationship with socio-economic position and dietary targets. Br. J. Nutr. 2014, 112, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Reid, R.E.B. The prehistoric roots of Chinese cuisines: Mapping staple food systems of China, 6000 BC-220 AD. PLoS ONE 2020, 15, e0240930. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Jiang, H.; Huang, F.; Zhang, B.; Zhang, J.; Wang, H. Cereals and tubers intake in Chinese adults aged 18–59 from 15 provinces in 2015. Ying Yang Xue Bao 2018, 40, 115–121. [Google Scholar]
- Lahong, J.; Dongmei, Y.; Hongyun, F.; Qiya, G.; Xiaoli, X.; Shujuan, L.; Liyun, Z. Trends and food sources composition of energy, protein and fat in Chinese residents, 1992–2012. Wei Sheng Yan Jiu 2018, 47, 689–694+704. [Google Scholar]
- Du, H.; van der A, D.L.; Ginder, V.; Jebb, S.A.; Forouhi, N.G.; Wareham, N.J.; Halkjaer, J.; Tjønneland, A.; Overvad, K.; Jakobsen, M.U.; et al. Dietary Energy Density in Relation to Subsequent Changes of Weight and Waist Circumference in European Men and Women. PLoS ONE 2009, 4, e5339. [Google Scholar] [CrossRef] [Green Version]
- Mendoza, J.A.; Drewnowski, A.; Christakis, D.A. Dietary energy density is associated with obesity and the metabolic syndrome in U.S. adults. Diabetes Care 2007, 30, 974–979. [Google Scholar] [CrossRef] [Green Version]
- Rouhani, M.H.; Haghighatdoost, F.; Surkan, P.J.; Azadbakht, L. Associations between dietary energy density and obesity: A systematic review and meta-analysis of observational studies. Nutrition 2016, 32, 1037–1047. [Google Scholar] [CrossRef]
- Murakami, K.; Livingstone, M.B.E.; Okubo, H.; Sasaki, S. Energy density of the diets of Japanese adults in relation to food and nutrient intake and general and abdominal obesity: A cross-sectional analysis from the 2012 National Health and Nutrition Survey, Japan. Br. J. Nutr. 2017, 117, 161–169. [Google Scholar] [CrossRef] [Green Version]
- Santosa, S.; Jensen, M.D. The Sexual Dimorphism of Lipid Kinetics in Humans. Front. Endocrinol. 2015, 6, 103. [Google Scholar] [CrossRef] [Green Version]
- Baker, A.H.; Wardle, J. Sex differences in fruit and vegetable intake in older adults. Appetite 2003, 40, 269–275. [Google Scholar] [CrossRef]
- Emanuel, A.S.; McCully, S.N.; Gallagher, K.M.; Updegraff, J.A. Theory of Planned Behavior explains gender difference in fruit and vegetable consumption. Appetite 2012, 59, 693–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingstone, K.M.; Sexton-Dhamu, M.J.; Pendergast, F.J.; Worsley, A.; Brayner, B.; McNaughton, S.A. Energy-dense dietary patterns high in free sugars and saturated fat and associations with obesity in young adults. Eur. J. Nutr. 2021, 61, 1595–1607. [Google Scholar] [CrossRef]
- Buckland, N.J.; Camidge, D.; Croden, F.; Lavin, J.H.; Stubbs, R.J.; Hetherington, M.M.; Blundell, J.E.; Finlayson, G. A Low Energy-Dense Diet in the Context of a Weight-Management Program Affects Appetite Control in Overweight and Obese Women. J. Nutr. 2018, 148, 798–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewnowski, A.; Specter, S.E. Poverty and obesity: The role of energy density and energy costs. Am. J. Clin. Nutr. 2004, 79, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Vernarelli, J.A.; DiSarro, R. Debunking the High Cost of Healthy Diets: Consumer Behavior Predicts Dietary Energy Density in a Nationally Representative Sample of US Adults. Am. J. Health Promot. 2021, 35, 543–550. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Males | p | Females | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Q1 1 | Q2 | Q3 | Q4 | Q1 | Q2 | Q3 | Q4 | |||
| N | 731 | 775 | 730 | 752 | 851 | 879 | 857 | 865 | ||
| DED (kcal/g) 2 | 1.7 ± 0.0 | 2.1 ± 0.0 | 2.4 ± 0.0 | 2.8 ± 0.0 | <0.001 | 1.7 ± 0.0 | 2.1 ± 0.0 | 2.4 ± 0.0 | 2.8 ± 0.0 | <0.001 |
| Age (years) | 39.9 ± 0.5 | 40.1 ± 0.5 | 39.2 ± 0.5 | 39.5 ± 0.5 | 0.544 | 39.1 ± 0.4 | 39.5 ± 0.4 | 39.1 ± 0.4 | 39.0 ± 0.4 | 0.814 |
| Urban and rural (%) | ||||||||||
| Urban | 21.5 | 30.7 | 33.7 | 36.8 | <0.001 | 23.7 | 31.0 | 34.2 | 34.8 | <0.001 |
| Rural | 78.5 | 69.3 | 66.3 | 63.2 | 76.3 | 69.0 | 65.8 | 65.2 | ||
| Region (%) | ||||||||||
| North | 30.8 | 29.8 | 34.7 | 45.1 | <0.001 | 29.7 | 32.3 | 37.7 | 46.8 | <0.001 |
| South | 69.2 | 70.2 | 65.3 | 54.9 | 70.3 | 67.7 | 62.3 | 53.2 | ||
| Education level (%) | ||||||||||
| Primary school and below | 47.2 | 41.9 | 41.5 | 37.9 | 0.010 | 60.8 | 56.9 | 57.6 | 61.0 | 0.100 |
| Middle school | 33.7 | 34.2 | 36.6 | 40.0 | 26.4 | 26.2 | 25.8 | 25.9 | ||
| High school and above | 19.1 | 23.9 | 21.9 | 22.1 | 12.8 | 16.9 | 16.6 | 13.1 | ||
| Income level (%) | ||||||||||
| Low | 36.4 | 28.1 | 30.4 | 37.1 | 0.001 | 33.0 | 29.7 | 32.9 | 39.1 | 0.005 |
| Medium | 32.7 | 34.5 | 36.4 | 32.2 | 32.3 | 34.2 | 34.0 | 30.3 | ||
| High | 30.9 | 37.4 | 33.2 | 30.7 | 34.7 | 36.1 | 33.1 | 30.6 | ||
| Urbanicity index | 44.4 ± 0.6 | 50.1 ± 0.6 | 50.7 ± 0.6 | 47.5 ± 0.6 | <0.001 | 46.3 ± 0.6 | 49.2 ± 0.6 | 50.1 ± 0.6 | 46.8 ± 0.6 | <0.001 |
| Physical activity (MET hours/week) | 381.9 ± 8.6 | 323.6 ± 7.6 | 324.4 ± 7.9 | 336.4 ± 8.2 | <0.001 | 433.0 ± 9.1 | 392.6 ± 8.8 | 380.4 ± 8.9 | 392.5 ± 8.6 | <0.001 |
| Current smoker (%) | 66.3 | 66.7 | 67.1 | 69.8 | 0.474 | 3.8 | 5.1 | 4.5 | 3.4 | 0.339 |
| Alcohol consumption (%) | 64.6 | 63.0 | 64.0 | 63.0 | 0.904 | 13.8 | 11.7 | 11.2 | 10.8 | 0.214 |
| WC (cm) | 75.9 ± 0.3 | 76.1 ± 0.3 | 76.8 ± 0.3 | 77.5 ± 0.3 | 0.001 | 74.2 ± 0.3 | 74.1 ± 0.3 | 75.1 ± 0.3 | 76.0 ± 0.3 | <0.001 |
| Abdominal obesity (%) | 16.4 | 15.6 | 16.4 | 21.1 | 0.018 | 23.2 | 24.9 | 28.5 | 34.0 | <0.001 |
| Dietary intake | ||||||||||
| Total energy(kcal/day) | 2237.0 ± 2 7.8 | 2637.2 ± 20.7 | 2839.6 ± 24.3 | 2988.0 ± 23.3 | <0.001 | 2066.9 ± 20.7 | 2310.6 ± 17.4 | 2445.6 ± 20.3 | 2649.4 ± 20.8 | <0.001 |
| The proportion of energy protein | 13.6 ± 0.1 | 13.3 ± 0.1 | 12.9 ± 0.1 | 12.2 ± 0.1 | <0.001 | 13.6 ± 0.1 | 13.2 ± 0.1 | 12.7 ± 0.1 | 12.2 ± 0.1 | <0.001 |
| The proportion of energy fat | 23.0 ± 0.5 | 23.3 ± 0.4 | 25.5 ± 0.4 | 26.2 ± 0.4 | <0.001 | 21.6 ± 0.4 | 22.8 ± 0.3 | 24.1 ± 0.4 | 25.7 ± 0.4 | <0.001 |
| The proportion of energy carbohydrate | 63.4 ± 0.5 | 63.4 ± 0.4 | 61.5 ± 0.4 | 61.6 ± 0.4 | <0.001 | 64.8 ± 0.4 | 64.0 ± 0.4 | 63.2 ± 0.4 | 62.1 ± 0.4 | <0.001 |
| DED | p-Trend 3 | ||||
|---|---|---|---|---|---|
| Q1 2 | Q2 | Q3 | Q4 | ||
| Male | |||||
| Model 1 4 | 0 | 0.18 (−0.03, 0.39) | 0.07 (−0.14, 0.29) | −0.05 (−0.27, 0.17) | 0.561 |
| Model 2 | 0 | 0.21 (−0.01, 0.42) | 0.11 (−0.11, 0.32) | −0.01 (−0.22, 0.21) | 0.825 |
| Model 3 | 0 | 0.21 (−0.01, 0.42) | 0.10 (−0.11, 0.32) | −0.01 (−0.22, 0.22) | 0.842 |
| Model 4 | 0 | 0.23 (0.02, 0.45) * | 0.14 (−0.08, 0.36) | 0.01 (−0.22, 0.25) | 0.984 |
| Female | |||||
| Model 1 | 0 | −0.02 (−0.22, 0.19) | 0.09 (−0.11, 0.30) | 0.29 (0.07, 0.50) ** | 0.004 |
| Model 2 | 0 | 0.01 (−0.19, 0.21) | 0.13 (−0.08, 0.33) | 0.33 (0.12, 0.54) ** | 0.001 |
| Model 3 | 0 | −0.01 (−0.20, 0.20) | 0.09 (−0.11, 0.29) | 0.27 (0.06, 0.48) * | 0.006 |
| Model 4 | 0 | −0.01 (−0.21, 0.20) | 0.08 (−0.13, 0.29) | 0.24 (0.01, 0.46) * | 0.024 |
| DED | p-Trend 3 | ||||
|---|---|---|---|---|---|
| Q1 2 | Q2 | Q3 | Q4 | ||
| Male | |||||
| Model 1 4 | 1.00 | 1.03 (0.93, 1.14) | 1.02 (0.92, 1.13) | 1.00 (0.90, 1.11) | 0.986 |
| Model 2 | 1.00 | 1.04 (0.94, 1.16) | 1.04 (0.94, 1.15) | 1.02 (0.92, 1.14) | 0.677 |
| Model 3 | 1.00 | 1.05 (0.95, 1.16) | 1.05 (0.94, 1.16) | 1.02 (0.93, 1.14) | 0.593 |
| Model 4 | 1.00 | 1.06 (0.96, 1.18) | 1.07 (0.96, 1.19) | 1.05 (0.93, 1.17) | 0.397 |
| Female | |||||
| Model 1 | 1.00 | 1.01 (0.92, 1.11) | 1.05 (0.96, 1.16) | 1.15 (1.04, 1.26) ** | 0.003 |
| Model 2 | 1.00 | 1.04 (0.95, 1.14) | 1.07 (0.98, 1.18) | 1.18 (1.07, 1.29) ** | 0.003 |
| Model 3 | 1.00 | 1.03 (0.94, 1.13) | 1.06 (0.97, 1.16) | 1.15 (1.05, 1.27) ** | 0.002 |
| Model 4 | 1.00 | 1.04 (0.94, 1.14) | 1.07 (0.97, 1.18) | 1.16 (1.05, 1.29) ** | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, H.; Zuo, L.; Song, X.; Su, C.; Wang, H.; Zhang, B.; Ding, G. Longitudinal Association of Dietary Energy Density with Abdominal Obesity among Chinese Adults from CHNS 1993–2018. Nutrients 2022, 14, 2151. https://doi.org/10.3390/nu14102151
Hu H, Zuo L, Song X, Su C, Wang H, Zhang B, Ding G. Longitudinal Association of Dietary Energy Density with Abdominal Obesity among Chinese Adults from CHNS 1993–2018. Nutrients. 2022; 14(10):2151. https://doi.org/10.3390/nu14102151
Chicago/Turabian StyleHu, Haojie, Lijun Zuo, Xiaoyun Song, Chang Su, Huijun Wang, Bing Zhang, and Gangqiang Ding. 2022. "Longitudinal Association of Dietary Energy Density with Abdominal Obesity among Chinese Adults from CHNS 1993–2018" Nutrients 14, no. 10: 2151. https://doi.org/10.3390/nu14102151
APA StyleHu, H., Zuo, L., Song, X., Su, C., Wang, H., Zhang, B., & Ding, G. (2022). Longitudinal Association of Dietary Energy Density with Abdominal Obesity among Chinese Adults from CHNS 1993–2018. Nutrients, 14(10), 2151. https://doi.org/10.3390/nu14102151