
The Effects of “Diet–Smoking–Gender” Three-Way Interactions on Cognitive Impairment among Chinese Older Adults



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Participants
2.2. Measurements
2.2.1. Cognitive Impairment
2.2.2. Dietary Diversity
2.2.3. Smoking Behavior
2.2.4. Covariates
2.3. Statistical Analysis
3. Results
- (1)
- Among all samples, high DDS was negatively associated with cognitive impairment (OR = 0.94; 95%CI = 0.90, 0.98), and males had better cognitive function (OR = 0.81; 95%CI = 0.77, 0.86) compared with females.
- (2)
- Among all samples, there was a significant “high DDS–smoking” interaction effect (OR = 1.11; 95%CI = 1.00, 1.24) on cognitive impairment. Regarding never-smoking participants, OR1 of cognitive impairment for high DDS versus low DDS was 0.92. Regarding participants who smoked in the past, OR2 of cognitive impairment for high DDS versus low DDS was 0.92 × 1.11 = 1.02 > 1.0 > OR1. Compared with never-smoking participants with low DDS, OR3 of cognitive impairment for participants who smoked in the past with high DDS was 0.92 × 0.92 × 1.11 = 0.94 > OR1. OR1, OR2, and OR3 indicate that “smoking in the past” may decrease the protective effect of high DDS on cognitive function.
- (3)
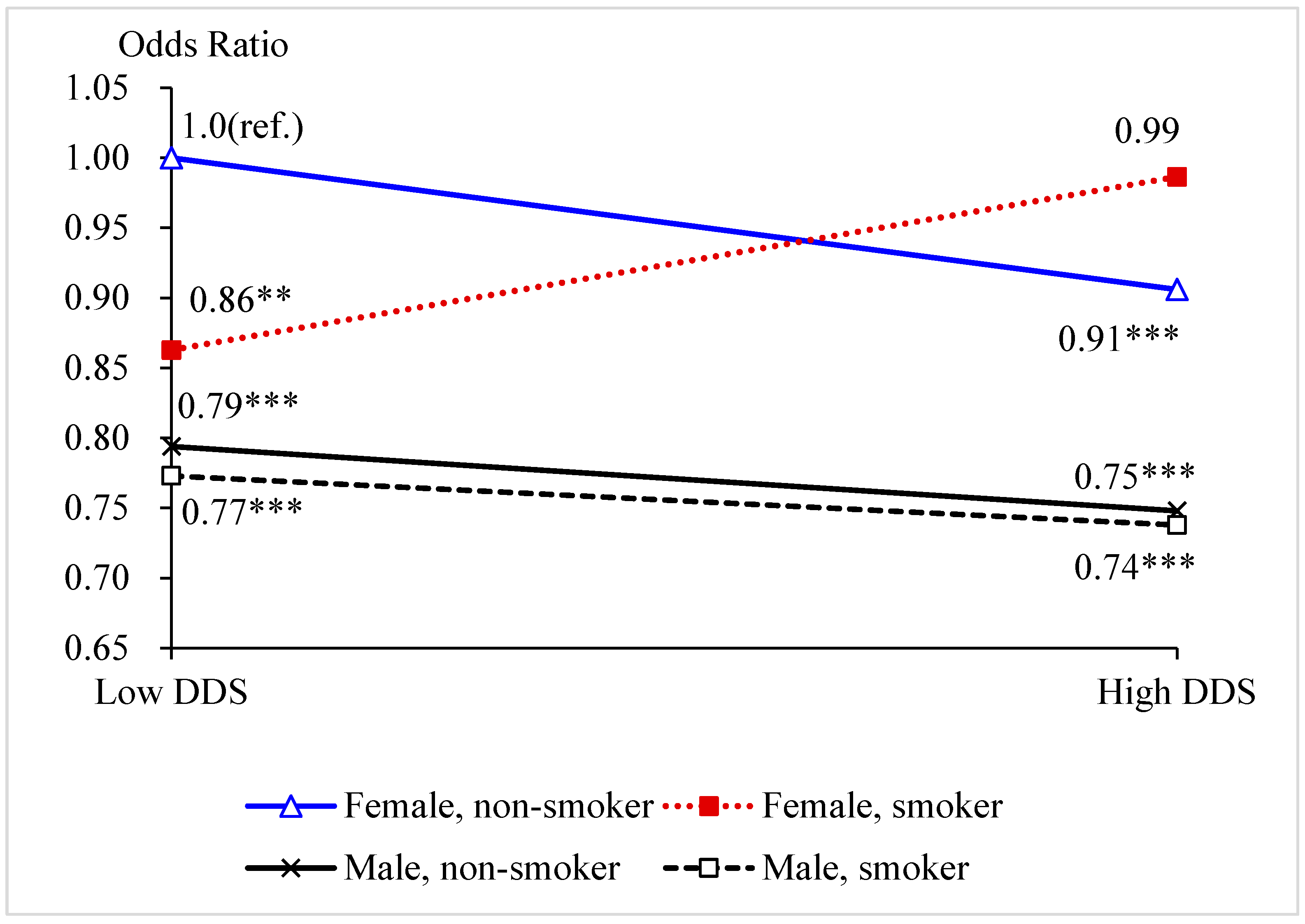
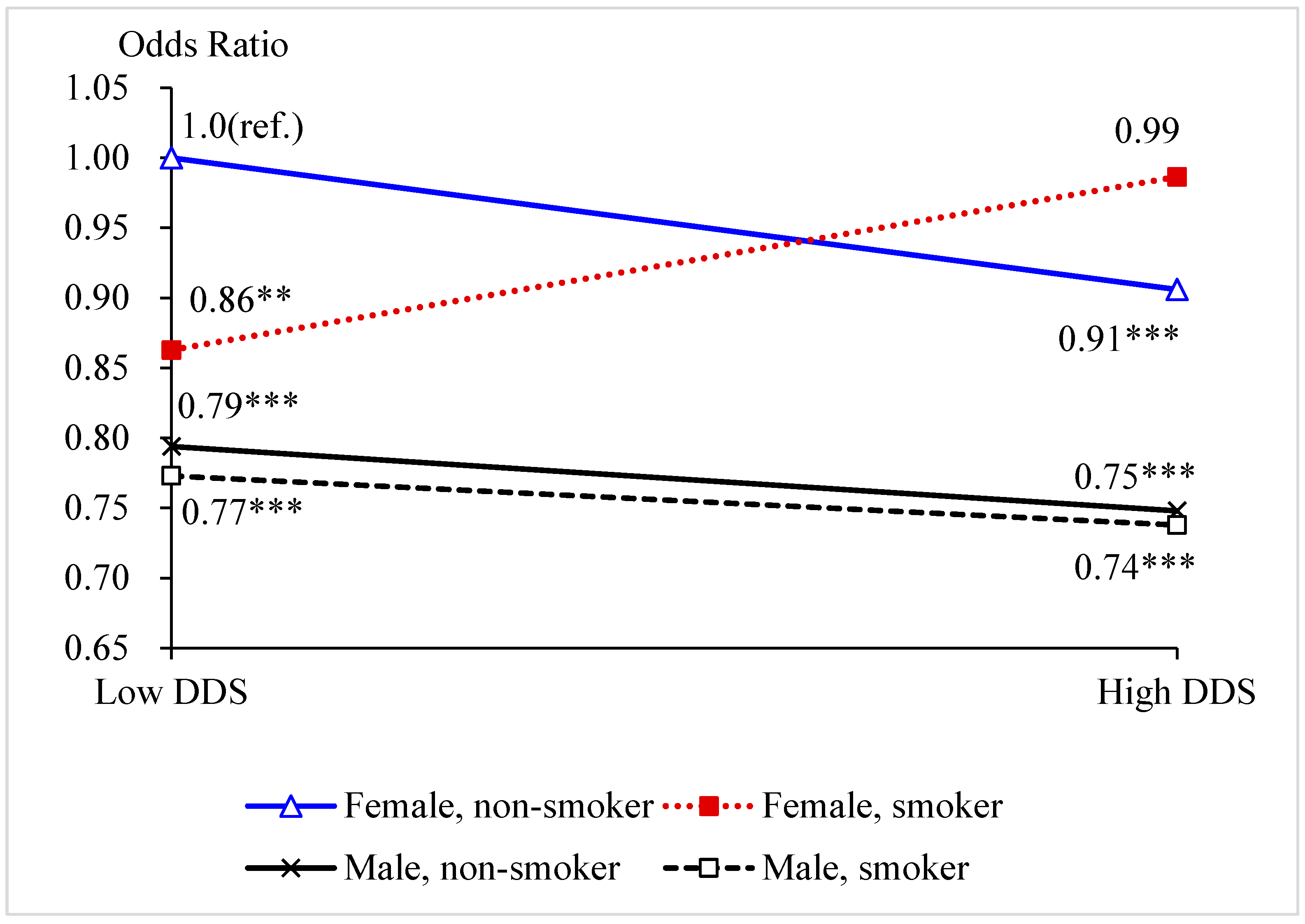
- Among all samples, there was a significant “high DDS–smoking–gender” three-way interaction effect (OR = 0.80; 95%CI = 0.65, 1.00) on cognitive impairment.
- (4)
- Among males, “high DDS–smoking” two-way interaction effects on cognitive function were not significant, which indicates that high DDS was always a protective factor with respect to cognitive function among males, regardless of their smoking behavior in the past.
- (5)
- Among females, there was a significant “high DDS–smoking” interaction effect (OR = 1.26; 95%CI = 1.07, 1.49) on cognitive impairment. Regarding never-smoking females, OR4 of cognitive impairment for high DDS versus low DDS was 0.92. Regarding females who smoked in the past, OR5 of cognitive impairment for high DDS versus low DDS was 0.92 × 1.26 = 1.16 > 1.0 > OR4. Compared with never-smoking females with low DDS, OR6 of cognitive impairment for females who smoked in the past with high DDS was 0.92 × 0.87 × 1.26 = 1.01 > 1.0 > OR4. OR4, OR5, and OR6 indicate that “smoking in the past” may offset the protective effect of high DDS on cognitive function among females.
- (1)
- Among all samples, we found that a high dietary frequency of “meat” (OR = 0.95; 95%CI = 0.90, 0.99), “fish or seafood” (OR = 0.95; 95%CI = 0.91, 1.00), “beans” (OR = 0.96; 95%CI = 0.91, 1.00), “tea” (OR = 0.92; 95%CI = 0.87, 0.96), and “garlic” (OR = 0.96; 95%CI = 0.92, 1.00) were associated with a lower risk of cognitive impairment.
- (2)
- Among all samples, there was a significant “high dietary frequency–smoking–gender” three-way interaction effect on cognitive impairment with “meat” or “fish or seafood” as the diet dichotomous variable.
- (3)
- Among males, the “high dietary frequency–smoking” interaction effect on cognitive impairment with “meat” as the diet dichotomous variable was not significant, which indicates that high dietary frequency of “meat” was always a protective factor with respect to cognitive function among males, regardless of their smoking behavior in the past. Regarding “fish or seafood”, there was a significant “high dietary frequency–smoking” interaction effect (OR = 0.89; 95%CI = 0.77, 1.02) on cognitive impairment. For never-smoking males, the OR of cognitive impairment for high dietary frequency versus low dietary frequency was 0.99. For males who smoked in the past, the OR of cognitive impairment for high dietary frequency versus low dietary frequency was 0.99 × 0.89 = 0.88. Compared with never-smoking males with low dietary frequency, the OR of cognitive impairment for males who smoked in the past with high dietary frequency was 0.99 × 1.02 × 0.89 = 0.90. These results indicate that high dietary frequency of “fish or seafood” was a protective factor with respect to cognitive function among both never-smoking males and males who smoked in the past.
- (4)
- Among females, regarding “meat”, there was a significant “high dietary frequency–smoking” interaction effect (OR = 1.17; 95%CI = 0.99, 1.38) on cognitive impairment. For never-smoking females, the OR of cognitive impairment for high dietary frequency versus low dietary frequency was 0.93. For females who smoked in the past, the OR of cognitive impairment for high dietary frequency versus low dietary frequency was 0.93 × 1.17 = 1.09 > 0.93. Compared with never-smoking females with low dietary frequency, the OR of cognitive impairment for females who smoked in the past with high dietary frequency was 0.93 × 0.90 × 1.17 > 0.93. These estimates indicate that “smoking in the past” may offset the protective effect of high dietary frequency of “meat” on cognitive function among females. Similarly, the results also indicate that “smoking in the past” may offset the protective effect of high dietary frequency of “fish or seafood” on cognitive function among females.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kivipelto, M.; Mangialasche, F.; Snyder, H.M.; Allegri, R.; Andrieu, S.; Arai, H.; Baker, L.; Belleville, S.; Brodaty, H.; Brucki, S.M.; et al. World-Wide FINGERS Network: A global approach to risk reduction and prevention of dementia. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2020, 16, 1078–1094. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Zhou, R.; Li, F.; Chen, L.; Wu, K.; Huang, J.; Liu, H.; Huang, Z.; Xu, L.; Yuan, Z.; et al. Association between dietary diversity and cognitive impairment among the oldest-old: Findings from a nationwide cohort study. Clin. Nutr. 2021, 40, 1452–1462. [Google Scholar] [CrossRef] [PubMed]
- Momtaz, Y.A.; Ibrahim, R.; Hamid, T.A.; Chai, S.T. Smoking and cognitive impairment among older persons in Malaysia. Am. J. Alzheimer’s Dis. Other Dement. 2015, 30, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Park, B.; Park, J.; Jun, J.K.; Choi, K.S.; Suh, M. Gender differences in the association of smoking and drinking with the development of cognitive impairment. PLoS ONE 2013, 8, e75095. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.C.; Chang, Y.H.; Lee, M.S.; Wahlqvist, M.L. Dietary quality may enhance survival related to cognitive impairment in Taiwanese elderly. Food Nutr. Res. 2011, 55, 7387. [Google Scholar] [CrossRef] [PubMed]
- Knoops, K.T.; de Groot, L.C.; Kromhout, D.; Perrin, A.E.; Moreiras-Varela, O.; Menotti, A.; van Staveren, W.A. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA 2004, 292, 1433–1439. [Google Scholar] [CrossRef]
- Chuang, S.Y.; Lo, Y.L.; Wu, S.Y.; Wang, P.N.; Pan, W.H. Dietary Patterns and Foods Associated With Cognitive Function in Taiwanese Older Adults: The Cross-sectional and Longitudinal Studies. J. Am. Med. Dir. Assoc. 2019, 20, 544–550.e4. [Google Scholar] [CrossRef]
- Scarmeas, N.; Anastasiou, C.A.; Yannakoulia, M. Nutrition and prevention of cognitive impairment. Lancet Neurol. 2018, 17, 1006–1015. [Google Scholar] [CrossRef]
- Deschasaux, M.; Huybrechts, I.; Julia, C.; Hercberg, S.; Egnell, M.; Srour, B.; Kesse-Guyot, E.; Latino-Martel, P.; Biessy, C.; Casagrande, C.; et al. Association between nutritional profiles of foods underlying Nutri-Score front-of-pack labels and mortality: EPIC cohort study in 10 European countries. BMJ 2020, 370, m3173. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Smiciklas-Wright, H.; Guthrie, H.A.; Krebs-Smith, J. The effects of variety in food choices on dietary quality. J. Am. Diet. Assoc. 1987, 87, 897–903. [Google Scholar]
- de Oliveira Otto, M.C.; Anderson, C.A.M.; Dearborn, J.L.; Ferranti, E.P.; Mozaffarian, D.; Rao, G.; Wylie-Rosett, J.; Lichtenstein, A.H. Dietary Diversity: Implications for Obesity Prevention in Adult Populations: A Science Advisory From the American Heart Association. Circulation 2018, 138, e160–e168. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Kraus, V.B.; Gao, X.; Yin, Z.; Zhou, J.; Mao, C.; Duan, J.; Zeng, Y.; Brasher, M.S.; Shi, W.; et al. Higher dietary diversity scores and protein-rich food consumption were associated with lower risk of all-cause mortality in the oldest old. Clin. Nutr. 2020, 39, 2246–2254. [Google Scholar] [CrossRef] [PubMed]
- Milte, C.M.; Ball, K.; Crawford, D.; McNaughton, S.A. Diet quality and cognitive function in mid-aged and older men and women. BMC Geriatr. 2019, 19, 361. [Google Scholar] [CrossRef] [Green Version]
- Gu, Q.; Sable, C.M.; Brooks-Wilson, A.; Murphy, R.A. Dietary patterns in the healthy oldest old in the healthy aging study and the Canadian longitudinal study of aging: A cohort study. BMC Geriatr. 2020, 20, 106. [Google Scholar] [CrossRef] [Green Version]
- Jee, S.H.; Suh, I.; Kim, I.S.; Appel, L.J. Smoking and atherosclerotic cardiovascular disease in men with low levels of serum cholesterol: The Korea Medical Insurance Corporation Study. JAMA 1999, 282, 2149–2155. [Google Scholar] [CrossRef] [Green Version]
- Gorelick, P.B.; Sacco, R.L.; Smith, D.B.; Alberts, M.; Mustone-Alexander, L.; Rader, D.; Ross, J.L.; Raps, E.; Ozer, M.N.; Brass, L.M.; et al. Prevention of a first stroke: A review of guidelines and a multidisciplinary consensus statement from the National Stroke Association. JAMA 1999, 281, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Cervilla, J.A.; Prince, M.; Mann, A. Smoking, drinking, and incident cognitive impairment: A cohort community based study included in the Gospel Oak project. J. Neurol. Neurosurg. Psychiatry 2000, 68, 622–626. [Google Scholar] [CrossRef] [Green Version]
- Anstey, K.J.; von Sanden, C.; Salim, A.; O’Kearney, R. Smoking as a risk factor for dementia and cognitive decline: A meta-analysis of prospective studies. Am. J. Epidemiol. 2007, 166, 367–378. [Google Scholar] [CrossRef]
- Ford, A.B.; Mefrouche, Z.; Friedland, R.P.; Debanne, S.M. Smoking and cognitive impairment: A population-based study. J. Am. Geriatr. Soc. 1996, 44, 905–909. [Google Scholar] [CrossRef]
- Doll, R.; Peto, R.; Boreham, J.; Sutherland, I. Smoking and dementia in male British doctors: Prospective study. BMJ 2000, 320, 1097–1102. [Google Scholar] [CrossRef] [Green Version]
- Fratiglioni, L.; Wang, H.X. Smoking and Parkinson’s and Alzheimer’s disease: Review of the epidemiological studies. Behav. Brain Res. 2000, 113, 117–120. [Google Scholar] [CrossRef]
- Nordberg, A. Biological markers and the cholinergic hypothesis in Alzheimer’s disease. Acta Neurol. Scandinavica. Suppl. 1992, 139, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Reitz, C.; Luchsinger, J.; Tang, M.X.; Mayeux, R. Effect of smoking and time on cognitive function in the elderly without dementia. Neurology 2005, 65, 870–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terry, A.V.; Callahan, P.M. Nicotinic Acetylcholine Receptor Ligands, Cognitive Function, and Preclinical Approaches to Drug Discovery. Nicotine Tob. Res. Off. J. Soc. Res. Nicotine Tob. 2019, 21, 383–394. [Google Scholar] [CrossRef]
- Halliwell, B. Cigarette Smoking and Health: A Radical View. J. R. Soc. Health 1993, 113, 91–96. [Google Scholar] [CrossRef]
- Margetts, B.M.; Jackson, A.A. Interactions between people’s diet and their smoking habits: The dietary and nutritional survey of British adults. BMJ 1993, 307, 1381–1384. [Google Scholar] [CrossRef] [Green Version]
- Oksuzyan, A.; Shkolnikova, M.; Vaupel, J.W.; Christensen, K.; Shkolnikov, V.M. Sex differences in health and mortality in Moscow and Denmark. Eur. J. Epidemiol. 2014, 29, 243–252. [Google Scholar] [CrossRef] [Green Version]
- Crimmins, E.M.; Kim, J.K.; Solé-Auró, A. Gender differences in health: Results from SHARE, ELSA and HRS. Eur. J. Public Health 2011, 21, 81–91. [Google Scholar] [CrossRef] [Green Version]
- Jia, L.; Quan, M.; Fu, Y.; Zhao, T.; Li, Y.; Wei, C.; Tang, Y.; Qin, Q.; Wang, F.; Qiao, Y.; et al. Dementia in China: Epidemiology, clinical management, and research advances. Lancet Neurol. 2020, 19, 81–92. [Google Scholar] [CrossRef]
- Au, B.; Dale-McGrath, S.; Tierney, M.C. Sex differences in the prevalence and incidence of mild cognitive impairment: A meta-analysis. Ageing Res. Rev. 2017, 35, 176–199. [Google Scholar] [CrossRef]
- Wang, J.; Xiao, L.D.; Wang, K.; Luo, Y.; Li, X. Gender Differences in Cognitive Impairment among Rural Elderly in China. Int. J. Environ. Res. Public Health 2020, 17, 3724. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Feng, Q.; Hesketh, T.; Christensen, K.; Vaupel, J.W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: A cohort study. Lancet 2017, 389, 1619–1629. [Google Scholar] [CrossRef]
- Zeng, Y. Towards Deeper Research and Better Policy for Healthy Aging—Using the Unique Data of Chinese Longitudinal Healthy Longevity Survey. China Econ. J. 2012, 5, 131–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Y.; Peng, C.-Y.J. Principled missing data methods for researchers. Springerplus 2013, 2, 222. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Li, H.; Jia, J.; Yang, Z. Mini-Mental State Examination in Elderly Chinese: A Population-Based Normative Study. J. Alzheimer’s Dis. JAD 2016, 53, 487–496. [Google Scholar] [CrossRef]
- Qiu, L.; Sautter, J.; Gu, D. Associations between frequency of tea consumption and health and mortality: Evidence from old Chinese. Br. J. Nutr. 2012, 108, 1686–1697. [Google Scholar] [CrossRef] [Green Version]
- Yin, Z.; Brasher, M.S.; Kraus, V.B.; Lv, Y.; Shi, X.; Zeng, Y. Dietary Diversity Was Positively Associated with Psychological Resilience among Elders: A Population-Based Study. Nutrients 2019, 11, 650. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Wu, Y.; Han, T.; Liu, E. Changes in Cognitive Function and Risk Factors for Cognitive Impairment of the Elderly in China: 2005–2014. Int. J. Environ. Res. Public Health 2019, 16, 2847. [Google Scholar] [CrossRef] [Green Version]
- Kuang, W.; Gao, M.; Tian, L.; Wan, Y.; Qiu, P. Trends in the prevalence of cognitive impairment in Chinese older adults: Based on the Chinese Longitudinal Healthy Longevity Survey cohorts from 1998 to 2014. Int. Health 2020, 12, 378–387. [Google Scholar] [CrossRef] [Green Version]
- Parrott, M.D.; Shatenstein, B.; Ferland, G.; Payette, H.; Morais, J.A.; Belleville, S.; Kergoat, M.J.; Gaudreau, P.; Greenwood, C.E. Relationship between diet quality and cognition depends on socioeconomic position in healthy older adults. J. Nutr. 2013, 143, 1767–1773. [Google Scholar] [CrossRef] [PubMed]
- Samieri, C.; Jutand, M.A.; Féart, C.; Capuron, L.; Letenneur, L.; Barberger-Gateau, P. Dietary patterns derived by hybrid clustering method in older people: Association with cognition, mood, and self-rated health. J. Am. Diet. Assoc. 2008, 108, 1461–1471. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, S.; Wang, W.; Zhang, D. Association between Dietary Protein Intake and Cognitive Function in Adults Aged 60 Years and Older. J. Nutr. Health Aging 2020, 24, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Nurk, E.; Drevon, C.A.; Refsum, H.; Solvoll, K.; Vollset, S.E.; Nygård, O.; Nygaard, H.A.; Engedal, K.; Tell, G.S.; Smith, A.D. Cognitive performance among the elderly and dietary fish intake: The Hordaland Health Study. Am. J. Clin. Nutr. 2007, 86, 1470–1478. [Google Scholar] [CrossRef]
- Ghasemi Fard, S.; Wang, F.; Sinclair, A.J.; Elliott, G.; Turchini, G.M. How does high DHA fish oil affect health? A systematic review of evidence. Crit. Rev. Food Sci. Nutr. 2019, 59, 1684–1727. [Google Scholar] [CrossRef] [Green Version]
- Mancini, E.; Beglinger, C.; Drewe, J.; Zanchi, D.; Lang, U.E.; Borgwardt, S. Green tea effects on cognition, mood and human brain function: A systematic review. Phytomedicine Int. J. Phytother. Phytopharm. 2017, 34, 26–37. [Google Scholar] [CrossRef] [Green Version]
- Lawson, L.D.; Hunsaker, S.M. Allicin Bioavailability and Bioequivalence from Garlic Supplements and Garlic Foods. Nutrients 2018, 10, 812. [Google Scholar] [CrossRef] [Green Version]
- Li, X.H.; Li, C.Y.; Lu, J.M.; Tian, R.B.; Wei, J. Allicin ameliorates cognitive deficits ageing-induced learning and memory deficits through enhancing of Nrf2 antioxidant signaling pathways. Neurosci. Lett. 2012, 514, 46–50. [Google Scholar] [CrossRef]
- Higgins, J.P.; Flicker, L. Lecithin for dementia and cognitive impairment. Cochrane Database Syst. Rev. 2003, 3, Cd001015. [Google Scholar] [CrossRef]
- Almeida, N.L.; Rodrigues, S.J.; Gonçalves, L.M.; Silverstein, S.M.; Sousa, I.C.; Gomes, G.H.; Butler, P.D.; Fernandes, T.P.; Santos, N.A. Opposite effects of smoking and nicotine intake on cognition. Psychiatry Res. 2020, 293, 113357. [Google Scholar] [CrossRef]
- Katsiardanis, K.; Diamantaras, A.A.; Dessypris, N.; Michelakos, T.; Anastasiou, A.; Katsiardani, K.P.; Kanavidis, P.; Papadopoulos, F.C.; Stefanadis, C.; Panagiotakos, D.B.; et al. Cognitive impairment and dietary habits among elders: The Velestino Study. J. Med. Food 2013, 16, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Hossin, M.Z. The male disadvantage in life expectancy: Can we close the gender gap? Int. Health 2021, 13, 482–484. [Google Scholar] [CrossRef] [PubMed]
- Sabia, S.; Elbaz, A.; Dugravot, A.; Head, J.; Shipley, M.; Hagger-Johnson, G.; Kivimaki, M.; Singh-Manoux, A. Impact of smoking on cognitive decline in early old age: The Whitehall II cohort study. Arch. Gen. Psychiatry 2012, 69, 627–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.C.; Lu, T.H.; Liao, W.C.; Yuan, S.C.; Kuo, P.C.; Chuang, H.L.; Lee, M.C.; Yen, C.H. Cigarette smoking and cognitive impairment: A 10-year cohort study in Taiwan. Arch. Gerontol. Geriatr. 2010, 51, 143–148. [Google Scholar] [CrossRef]
- Mons, U.; Schöttker, B.; Müller, H.; Kliegel, M.; Brenner, H. History of lifetime smoking, smoking cessation and cognitive function in the elderly population. Eur. J. Epidemiol. 2013, 28, 823–831. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | 2002 | 2005 | 2008–2009 | 2011–2012 | 2014 | 2017–2018 |
|---|---|---|---|---|---|---|
| n = 15,953 | n = 15,555 | n = 16,849 | n = 9716 | n = 7116 | n = 13,165 | |
| Cognitive Impairment (%) | ||||||
| Yes | 4133 (25.9) | 2869 (20.0) | 3559 (23.2) | 1974 (21.4) | 1312 (19.5) | 2680 (21.3) |
| No | 11,804 (74.1) | 11,484 (80.0) | 11,762 (76.8) | 7254 (78.6) | 5423 (80.5) | 9897 (78.7) |
| DDS | ||||||
| DDS (0–7), mean (SD) | 4.39 (1.99) | 4.47 (1.96) | 2.42 (1.97) | 2.49 (1.97) | 2.58 (2.00) | 2.84 (1.98) |
| High DDS (%) | 11,083 (69.5) | 11,034 (70.9) | 5097 (30.3) | 3086 (31.8) | 2375 (33.4) | 5259 (39.9) |
| Low DDS (%) | 4870 (30.5) | 4521 (29.1) | 11,752 (69.7) | 6630 (68.2) | 4741 (66.6) | 7906 (60.1) |
| Ever smoker (%) | ||||||
| Yes | 5373 (33.7) | 5231 (33.6) | 5271 (31.3) | 3048 (31.4) | 2091 (29.4) | 3719 (28.2) |
| No | 10,580 (66.3) | 10,324 (66.4) | 11,578 (68.7) | 6668 (68.6) | 5025 (70.6) | 9446 (71.8) |
| Gender (%) | ||||||
| Male | 6807 (42.7) | 6665 (42.8) | 7187 (42.7) | 4378 (45.1) | 3283 (46.1) | 5632 (42.8) |
| Female | 9146 (57.3) | 8890 (57.2) | 9662 (57.3) | 5338 (54.9) | 3833 (53.9) | 7533 (57.2) |
| Covariates | ||||||
| Age, mean (SD) | 86.28 (11.7) | 86.13 (11.7) | 86.93 (11.8) | 85.75 (11.4) | 85.31 (10.7) | 85.46 (11.9) |
| Region (%) | ||||||
| East province | 7663 (48.0) | 7040 (45.3) | 7796 (46.3) | 4645 (47.8) | 3452 (48.5) | 6754 (51.3) |
| Middle/west | 8290 (52.0) | 8515 (54.7) | 9053 (53.7) | 5071 (52.2) | 3664 (51.5) | 6411 (48.7) |
| Residence (%) | ||||||
| Urban area | 7339 (46.0) | 6929 (44.5) | 6628 (39.3) | 4601 (47.4) | 3193 (44.9) | 7568 (57.5) |
| Rural area | 8614 (54.0) | 8626 (55.5) | 10,221 (60.7) | 5115 (52.6) | 3923 (55.1) | 5597 (42.5) |
| Married/partnered (%) | ||||||
| Yes | 5017 (31.4) | 5070 (32.6) | 5481 (32.5) | 3690 (38.0) | 2778 (39.0) | 5363 (40.7) |
| No | 10,936 (68.6) | 10,485 (67.4) | 11,368 (67.5) | 6026 (62.0) | 4338 (61.0) | 7802 (59.3) |
| Years of schooling, mean (SD) | 2.02 (3.50) | 2.11 (3.53) | 2.04 (3.42) | 2.29 (3.51) | 2.38 (3.47) | 3.16 (4.23) |
| # of family members, mean (SD) | 2.95 (1.87) | 2.82 (1.73) | 2.68 (1.68) | 2.61 (1.75) | 2.37 (1.61) | 2.37 (1.61) |
| Log of income per capita, mean (SD) | 7.59 (1.23) | 7.86 (1.45) | 8.32 (1.31) | 8.64 (1.61) | 8.95 (1.48) | 9.22 (1.82) |
| Poor self-rated health (%) | ||||||
| Yes | 2466 (15.5) | 2351 (15.1) | 2407 (14.3) | 1556 (16.0) | 1001 (14.1) | 1732 (13.2) |
| No | 13,487 (84.5) | 13,204 (84.9) | 14,442 (85.7) | 8160 (84.0) | 6115 (85.9) | 11,433 (86.8) |
| Regular exercise (%) | ||||||
| Yes | 5919 (37.1) | 5434 (34.9) | 5042 (29.9) | 2521 (25.9) | 1910 (26.8) | 4189 (31.8) |
| No | 10,034 (62.9) | 10,121 (65.1) | 11,807 (70.1) | 7195 (74.1) | 5206 (73.2) | 8976 (68.2) |
| Items | Male | Female | ||
|---|---|---|---|---|
| Non-Smoker | Smoker | Non-Smoker | Smoker | |
| n = 13,617 | n = 19,175 | n = 36,709 | n = 4650 | |
| Cognitive impairment | ||||
| Yes (%) | 2465 (18.1) | 2685 (14.0) | 10,107 (27.5) | 1270 (27.3) |
| No (%) | 11,152 (81.9) | 16,490 (86.0) | 26,602 (72.5) | 3380 (72.7) |
| Dietary diversity score (DDS) | ||||
| DDS (0–7), mean (SD) | 3.50 (2.17) | 3.74 (2.14) | 3.10 (2.16) | 3.37 (2.17) |
| High DDS (%) | 7079 (52.0) | 10,759 (56.1) | 16,279 (44.3) | 2301 (49.5) |
| Low DDS (%) | 6538 (48.0) | 8416 (43.9) | 20,430 (55.7) | 2349 (50.5) |
| (1) All Samples | (2) All Samples | (3) All Samples | (4) Males Only | (5) Females Only | |
|---|---|---|---|---|---|
| OR [95%CI] | OR [95%CI] | OR [95%CI] | OR [95%CI] | OR [95%CI] | |
| High DDS (low DDS *) | 0.94 [0.90, 0.98] *** | 0.92 [0.87, 0.98] *** | 0.91 [0.85, 0.96] *** | 0.91 [0.82, 1.02] * | 0.92 [0.87, 0.98] ** |
| Ever smoking (no *) | 0.97 [0.92, 1.03] | 0.92 [0.83, 1.01] * | 0.86 [0.77, 0.97] ** | 0.96 [0.87, 1.06] | 0.87 [0.77, 0.97] ** |
| Male (female *) | 0.81 [0.77, 0.86] *** | 0.82 [0.76, 0.88] *** | 0.79 [0.73, 0.86] *** | -- | -- |
| Interaction items | |||||
| High DDS × smoking | 1.11 [1.00, 1.24] * | 1.26 [1.07, 1.49] *** | 1.01 [0.88, 1.16] | 1.26 [1.07, 1.49] *** | |
| High DDS × male | 0.98 [0.88, 1.08] | 1.04 [0.92, 1.17] | -- | -- | |
| Smoking× male | 1.02 [0.91, 1.14] | 1.13 [0.97, 1.31] | -- | -- | |
| High DDS × smoking × male | 0.80 [0.65, 1.00] ** | -- | -- | ||
| Covariates | |||||
| Age | 1.12 [1.12, 1.12] *** | 1.12 [1.12, 1.12] *** | 1.12 [1.12, 1.12] *** | 1.11 [1.11, 1.12] *** | 1.12 [1.12, 1.13] *** |
| East China (middle/west *) | 0.95 [0.91, 1.00] ** | 0.95 [0.91, 1.00] ** | 0.95 [0.91, 1.00] ** | 0.98 [0.91, 1.05] | 0.94 [0.89, 0.99] ** |
| Urban residence (rural *) | 0.98 [0.93, 1.02] | 0.98 [0.93, 1.02] | 0.98 [0.93, 1.02] | 1.01 [0.94, 1.09] | 0.97 [0.91, 1.02] |
| Married (others *) | 0.78 [0.73, 0.83] *** | 0.78 [0.73, 0.83] *** | 0.78 [0.73, 0.83] *** | 0.79 [0.73, 0.86] *** | 0.73 [0.66, 0.81] *** |
| Years of schooling | 1.02 [1.01, 1.03] *** | 1.02 [1.01, 1.03] *** | 1.02 [1.01, 1.03] *** | 1.02 [1.01, 1.03] *** | 1.01 [1.00, 1.03] ** |
| Number of family members | 1.03 [1.01, 1.04] *** | 1.03 [1.01, 1.04] *** | 1.03 [1.01, 1.04] *** | 1.02 [1.00, 1.04] ** | 1.03 [1.01, 1.04] *** |
| Log of income per capita | 0.91 [0.90, 0.93] *** | 0.91 [0.90, 0.93] *** | 0.91 [0.90, 0.93] *** | 0.91 [0.89, 0.93] *** | 0.92 [0.90, 0.93] *** |
| Poor self-rated health (good #) | 1.97 [1.87, 2.08] *** | 1.97 [1.87, 2.08] *** | 1.97 [1.87, 2.08] *** | 2.22 [2.03, 2.43] *** | 1.84 [1.72, 1.97] *** |
| Regular exercise (no #) | 0.76 [0.73, 0.80] *** | 0.76 [0.73, 0.80] *** | 0.76 [0.73, 0.80] *** | 0.75 [0.70, 0.81] *** | 0.77 [0.73, 0.83] *** |
| Waves (2002 #) | |||||
| 2005 | 0.80 [0.75, 0.85] *** | 0.80 [0.75, 0.85] *** | 0.80 [0.75, 0.85] *** | 0.76 [0.68, 0.84] *** | 0.83 [0.77, 0.89] *** |
| 2008 | 0.91 [0.86, 0.98] *** | 0.91 [0.86, 0.97] *** | 0.91 [0.86, 0.97] *** | 0.83 [0.75, 0.93] *** | 0.96 [0.89, 1.04] |
| 2011 | 0.96 [0.89, 1.03] | 0.96 [0.89, 1.03] | 0.96 [0.89, 1.03] | 0.82 [0.72, 0.93] *** | 1.05 [0.95, 1.15] |
| 2014 | 0.96 [0.88, 1.05] | 0.96 [0.88, 1.05] | 0.96 [0.88, 1.05] | 0.91 [0.79, 1.04] | 1.00 [0.89, 1.11] |
| 2018 | 1.00 [0.93, 1.08] | 1.00 [0.93, 1.07] | 1.00 [0.93, 1.07] | 0.96 [0.85, 1.08] | 1.03 [0.94, 1.12] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.; Zhang, X.; Feng, Q.; Zeng, Y. The Effects of “Diet–Smoking–Gender” Three-Way Interactions on Cognitive Impairment among Chinese Older Adults. Nutrients 2022, 14, 2144. https://doi.org/10.3390/nu14102144
Chen H, Zhang X, Feng Q, Zeng Y. The Effects of “Diet–Smoking–Gender” Three-Way Interactions on Cognitive Impairment among Chinese Older Adults. Nutrients. 2022; 14(10):2144. https://doi.org/10.3390/nu14102144
Chicago/Turabian StyleChen, Huashuai, Xuxi Zhang, Qiushi Feng, and Yi Zeng. 2022. "The Effects of “Diet–Smoking–Gender” Three-Way Interactions on Cognitive Impairment among Chinese Older Adults" Nutrients 14, no. 10: 2144. https://doi.org/10.3390/nu14102144
APA StyleChen, H., Zhang, X., Feng, Q., & Zeng, Y. (2022). The Effects of “Diet–Smoking–Gender” Three-Way Interactions on Cognitive Impairment among Chinese Older Adults. Nutrients, 14(10), 2144. https://doi.org/10.3390/nu14102144