
“HIIT the Inflammation”: Comparative Effects of Low-Volume Interval Training and Resistance Exercises on Inflammatory Indices in Obese Metabolic Syndrome Patients Undergoing Caloric Restriction

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Health Examinations
2.3.1. Measurements of Blood Pressure
2.3.2. Blood Collection
2.3.3. Anthropometric and Body Composition Measurements
2.3.4. MetS z-Score Determination
2.3.5. Cardiopulmonary Exercise Test (CPET)
2.3.6. Maximum Strength (Fmax) Testing
2.4. Nutritional Counseling
2.5. Exercise Training Programs
2.5.1. Very Low-Volume High-Intensity Interval Training
2.5.2. Resistance Training
2.5.3. Whole-Body Electromyostimulation
2.6. Statistical Analysis
3. Results
3.1. Study Flow
3.2. Nutritional Analysis
3.3. Anthropometric and Body Composition Data
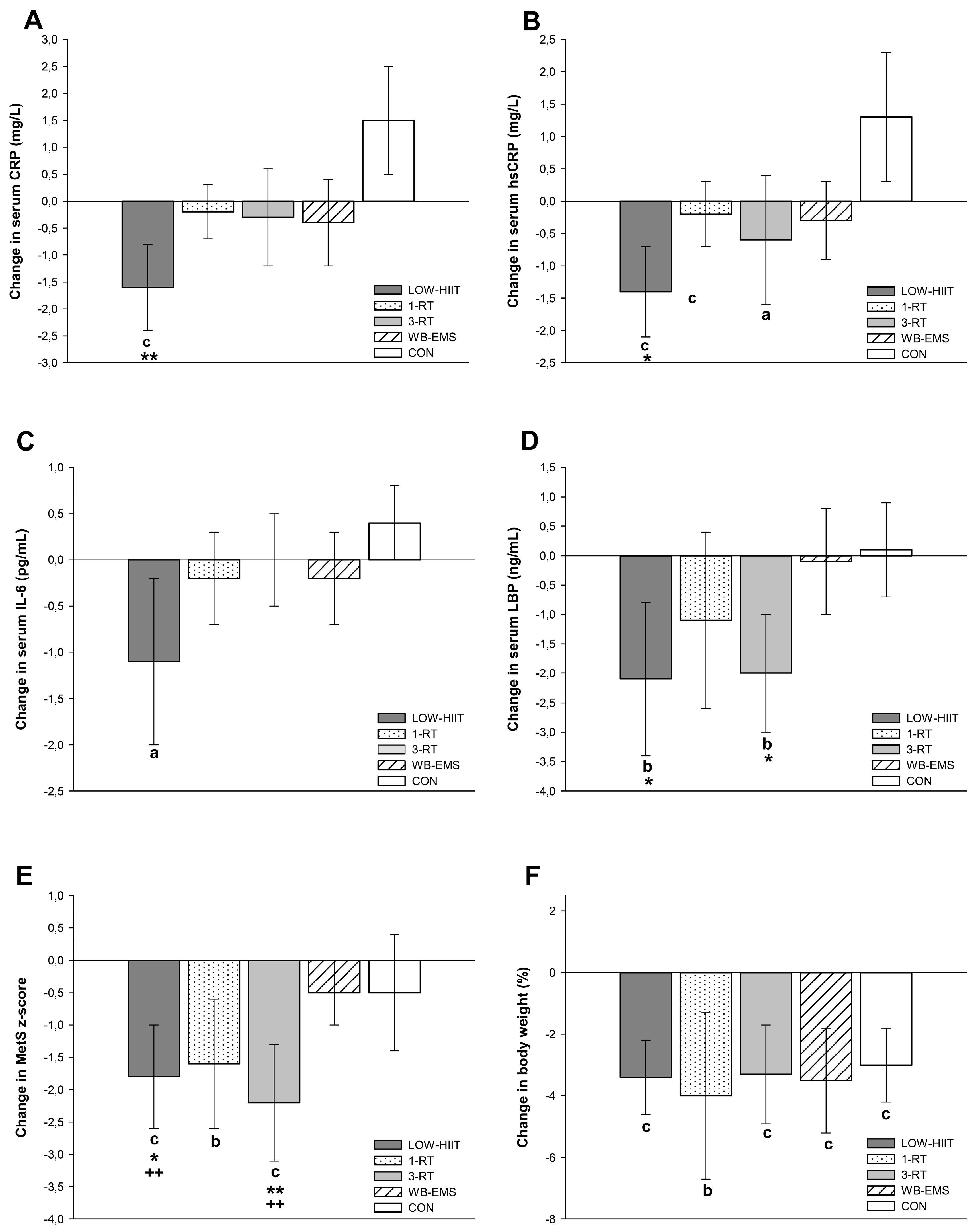
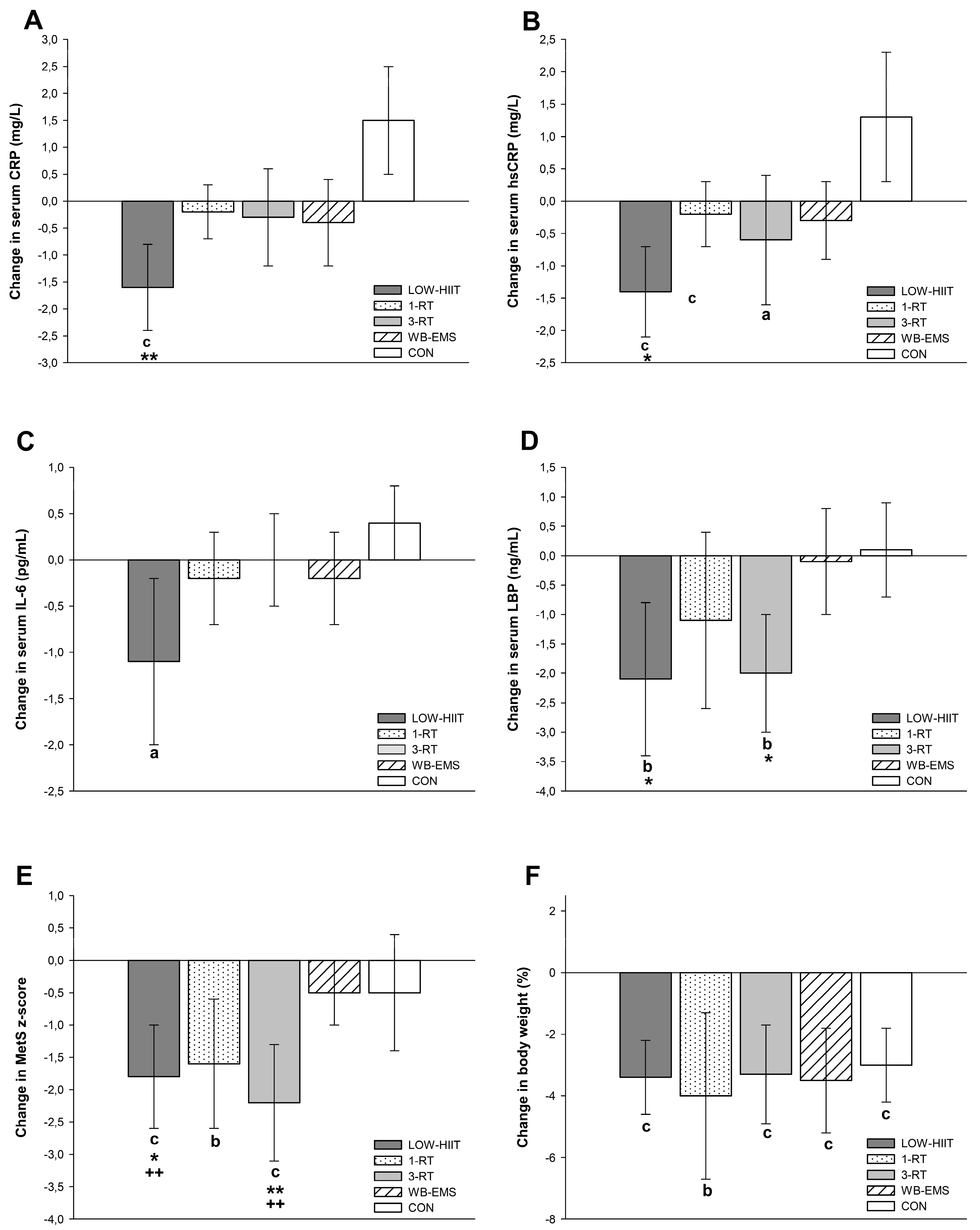
3.4. Inflammatory Markers
3.5. Cardiometabolic Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [PubMed]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.H.; Liu, W.; Ho, S.C. Metabolic syndrome and all-cause mortality: A meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 2010, 25, 375–384. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Estato, V.; Castro-Faria-Neto, H.C.; Tibirica, E. Obesity-related inflammation and endothelial dysfunction in COVID-19: Impact on disease severity. J. Inflamm. Res. 2021, 14, 2267–2276. [Google Scholar] [CrossRef] [PubMed]
- Mauvais-Jarvis, F. Aging, male sex, obesity, and metabolic inflammation create the perfect storm for COVID-19. Diabetes 2020, 69, 1857–1863. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.; Bressem, K.; Albrecht, J.; Thieß, H.M.; Vahldiek, J.; Hamm, B.; Makowski, M.R.; Niehues, A.; Niehues, S.M.; Adams, L.C. The role of visceral adiposity in the severity of COVID-19: Highlights from a unicenter cross-sectional pilot study in Germany. Metabolism 2020, 110, 154317. [Google Scholar] [CrossRef]
- Monteiro, R.; Azevedo, I. Chronic inflammation in obesity and the metabolic syndrome. Mediat. Inflamm. 2010, 2010, 289645. [Google Scholar] [CrossRef]
- Ramos-Nino, M.E. The role of chronic inflammation in obesity-associated cancers. ISRN Oncol. 2013, 2013, 697521. [Google Scholar] [CrossRef] [Green Version]
- Ellulu, M.S.; Patimah, I.; Khaza’ai, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar] [CrossRef]
- Makki, K.; Froguel, P.; Wolowczuk, I. Adipose tissue in obesity-related inflammation and insulin resistance: Cells, cytokines, and chemokines. ISRN Inflamm. 2013, 2013, 139239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zatterale, F.; Longo, M.; Naderi, J.; Raciti, G.A.; Desiderio, A.; Miele, C.; Beguinot, F. Chronic adipose tissue inflammation linking obesity to insulin resistance and type 2 diabetes. Front. Physiol. 2020, 10, 1607. [Google Scholar] [CrossRef] [PubMed]
- Caristia, S.; Vito, M.; Sarro, A.; Leone, A.; Pecere, A.; Zibetti, A.; Filigheddu, N.; Zeppegno, P.; Prodam, F.; Faggiano, F.; et al. Is caloric restriction associated with better healthy aging outcomes? A systematic review and meta-analysis of randomized controlled trials. Nutrients 2020, 12, 2290. [Google Scholar] [CrossRef] [PubMed]
- Stromsnes, K.; Correas, A.G.; Lehmann, J.; Gambini, J.; Olaso-Gonzalez, G. Anti-inflammatory properties of diet: Role in healthy aging. Biomedicines 2021, 9, 922. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K.; American College of Sports Medicine. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Rogers, R.J.; Davis, K.K.; Collins, K.A. Role of physical activity and exercise in treating patients with overweight and obesity. Clin. Chem. 2018, 64, 99–107. [Google Scholar] [CrossRef]
- Gabandé-Rodríguez, E.; Gómez de Las Heras, M.M.; Mittelbrunn, M. Control of inflammation by calorie restriction mimetics: On the crossroad of autophagy and mitochondria. Cells 2019, 9, 82. [Google Scholar] [CrossRef] [Green Version]
- Brown, W.M.; Davison, G.W.; McClean, C.M.; Murphy, M.H. A systematic review of the acute effects of exercise on immune and inflammatory indices in untrained adults. Sports Med. Open 2015, 1, 35. [Google Scholar] [CrossRef] [Green Version]
- Zheng, G.; Qiu, P.; Xia, R.; Lin, H.; Ye, B.; Tao, J.; Chen, L. Effect of aerobic exercise on inflammatory markers in healthy middle-aged and older adults: A systematic review and meta-analysis of randomized controlled trials. Front. Aging Neurosci. 2019, 11, 98. [Google Scholar] [CrossRef] [Green Version]
- Alizaei Yousefabadi, H.; Niyazi, A.; Alaee, S.; Fathi, M.; Mohammad Rahimi, G.R. Anti-inflammatory effects of exercise on metabolic syndrome patients: A systematic review and meta-analysis. Biol. Res. Nurs. 2021, 23, 280–292. [Google Scholar] [CrossRef]
- Calle, M.C.; Fernandez, M.L. Effects of resistance training on the inflammatory response. Nutr. Res. Pract. 2010, 4, 259–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Tudor-Locke, C.; Brashear, M.M.; Johnson, W.D.; Katzmarzyk, P.T. Accelerometer profiles of physical activity and inactivity in normal weight, overweight, and obese U.S. men and women. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Cavallini, M.F.; Callaghan, M.E.; Premo, C.B.; Scott, J.W.; Dyck, D.J. Lack of time is the consistent barrier to physical activity and exercise in 18 to 64 year-old males and females from both South Carolina and Southern Ontario. J. Phys. Act. Res. 2020, 5, 100–106. [Google Scholar] [CrossRef]
- Andersen, R.E.; Jakicic, J.M. Interpreting the physical activity guidelines for health and weight management. J. Phys. Act. Health 2009, 6, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; Little, J.P. Physiological basis of brief vigorous exercise to improve health. J. Physiol. 2020, 598, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Gillen, J.B.; Gibala, M.J. Is high-intensity interval training a time-efficient exercise strategy to improve health and fitness? Appl. Physiol. Nutr. Metab. 2014, 39, 409–412. [Google Scholar] [CrossRef]
- Vollaard, N.B.; Metcalfe, R.S. Research into health benefits of sprint interval training should focus on protocols with fewer and shorter sprints. Sports Med. 2017, 47, 2443–2451. [Google Scholar] [CrossRef] [Green Version]
- Iversen, V.M.; Norum, M.; Schoenfeld, B.J.; Fimland, M.S. No time to lift? Designing time-efficient training programs for strength and hypertrophy: A narrative review. Sports Med. 2021, 51, 2079–2095. [Google Scholar] [CrossRef]
- Kemmler, W.; Kleinöder, H.; Fröhlich, M. Editorial: Whole-body electromyostimulation: A training technology to improve health and performance in humans? Front. Physiol. 2020, 11, 523. [Google Scholar] [CrossRef]
- Gibala, M.J.; Gillen, J.B.; Percival, M.E. Physiological and health-related adaptations to low-volume interval training: Influences of nutrition and sex. Sports Med. 2014, 44 (Suppl. S2), 127–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sultana, R.N.; Sabag, A.; Keating, S.E.; Johnson, N.A. The effect of low-volume high-intensity interval training on body composition and cardiorespiratory fitness: A systematic review and meta-analysis. Sports Med. 2019, 49, 1687–1721. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Frenk, F.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Low-volume high-intensity interval training improves cardiometabolic health, work ability and well-being in severely obese individuals: A randomized-controlled trial sub-study. J. Transl. Med. 2020, 18, 419. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Frenk, F.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Effects of very low volume high intensity versus moderate intensity interval training in obese metabolic syndrome patients: A randomized controlled study. Sci. Rep. 2021, 11, 2836. [Google Scholar] [CrossRef]
- Ramos, J.S.; Dalleck, L.C.; Borrani, F.; Beetham, K.S.; Wallen, M.P.; Mallard, A.R.; Clark, B.; Gomersall, S.; Keating, S.E.; Fassett, R.G.; et al. Low-volume high-intensity interval training is sufficient to ameliorate the severity of metabolic syndrome. Metab. Syndr. Relat. Disord. 2017, 15, 319–328. [Google Scholar] [CrossRef]
- Myers, J.; Kokkinos, P.; Nyelin, E. Physical activity, cardiorespiratory fitness, and the metabolic syndrome. Nutrients 2019, 1, 1652. [Google Scholar] [CrossRef] [Green Version]
- Hsu, K.J.; Liao, C.D.; Tsai, M.W.; Chen, C.N. Effects of exercise and nutritional intervention on body composition, metabolic health, and physical performance in adults with sarcopenic obesity: A meta-analysis. Nutrients 2019, 11, 2163. [Google Scholar] [CrossRef] [Green Version]
- Reljic, D.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Iron beats electricity: Resistance training but not whole-body electromyostimulation improves cardiometabolic health in obese metabolic syndrome patients during caloric restriction-a randomized-controlled study. Nutrients 2021, 13, 1640. [Google Scholar] [CrossRef]
- Strasser, B.; Schobersberger, W. Evidence for resistance training as a treatment therapy in obesity. J. Obes. 2011, 2011, 482564. [Google Scholar] [CrossRef] [Green Version]
- Westcott, W.L. Resistance training is medicine: Effects of strength training on health. Curr. Sports Med. Rep. 2012, 11, 209–216. [Google Scholar] [CrossRef]
- Kemmler, W.; Weissenfels, A.; Willert, S.; Shojaa, M.; von Stengel, S.; Filipovic, A.; Kleinöder, H.; Berger, J.; Fröhlich, M. Efficacy and safety of low frequency whole-body electromyostimulation (WB-EMS) to improve health-related outcomes in non-athletic adults. A systematic review. Front. Physiol. 2018, 9, 573. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Konturek, P.C.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Effects of whole-body electromyostimulation exercise and caloric restriction on cardiometabolic risk profile and muscle strength in obese women with the metabolic syndrome: A pilot study. J. Physiol. Pharmacol. 2020, 71, 89–98. [Google Scholar]
- Gonzalo-Encabo, P.; Maldonado, G.; Valadés, D.; Ferragut, C.; Pérez-López, A. The role of exercise training on low-grade systemic inflammation in adults with overweight and obesity: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 13258. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Model Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 8th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; pp. 26–27. [Google Scholar]
- Tholl, U.; Lüders, S.; Bramlage, P.; Dechend, R.; Eckert, S.; Mengden, T.; Nürnberger, J.; Sanner, B.; Anlauf, M. The German Hypertension League (Deutsche Hochdruckliga) quality seal protocol for blood pressure-measuring devices: 15-year experience and results from 105 devices for home blood pressure control. Blood Press. Monit. 2016, 21, 197–205. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.J.R.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 138, e426–e483. [Google Scholar]
- Bosy-Westphal, A.; Jensen, B.; Braun, W.; Pourhassan, M.; Gallagher, D.; Müller, M.J. Quantification of whole-body and segmental skeletal muscle mass using phase-sensitive 8-electrode medical bioelectrical impedance devices. Eur. J. Clin. Nutr. 2017, 71, 1061–1067. [Google Scholar] [CrossRef]
- Earnest, C.P.; Artero, E.G.; Sui, X.; Lee, D.C.; Church, T.S.; Blair, S.N. Maximal estimated cardiorespiratory fitness, cardiometabolic risk factors, and metabolic syndrome in the aerobics center longitudinal study. Mayo Clin. Proc. 2013, 88, 259–270. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.L.; Slentz, C.A.; Houmard, J.A.; Samsa, G.P.; Duscha, B.D.; Aiken, L.B.; McCartney, J.S.; Tanner, C.J.; Kraus, W.E. Exercise training amount and intensity effects on metabolic syndrome (from studies of a targeted risk reduction intervention through defined exercise). Am. J. Cardiol. 2007, 100, 1759–1766. [Google Scholar] [CrossRef] [Green Version]
- Howley, E.T.; Bassett, D.R., Jr.; Welch, H.G. Criteria for maximal oxygen uptake: Review and commentary. Med. Sci. Sports Exerc. 1995, 27, 1292–1301. [Google Scholar] [CrossRef]
- Reynolds, J.M.; Gordon, T.J.; Robergs, R.A. Prediction of one repetition maximum strength from multiple repetition maximum testing and anthropometry. J. Strength Cond. Res. 2006, 20, 584–592. [Google Scholar] [PubMed] [Green Version]
- Dohoney, P.; Chromiak, J.A.; Lemire, D.; Abadie, B.R.; Kovacs, C. Prediction of one repetition maximum (1-RM) strength from a 4–6 RM and a 7–10 RM submaximal strength test in healthy young adult males. J. Exerc. Physiol. Online 2002, 5, 54–59. [Google Scholar]
- Brzycki, M. Strength testing: Predicting a one-rep max from repetitions to fatigue. J. Phys. Educ. Recreat. Danc. 1993, 64, 88–90. [Google Scholar] [CrossRef]
- Carels, R.A.; Young, K.M.; Coit, C.; Clayton, A.M.; Spencer, A.; Hobbs, M. Can following the caloric restriction recommendations from the Dietary Guidelines for Americans help individuals lose weight? Eat. Behav. 2006, 9, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Al-Nimr, R.I. Optimal protein intake during weight loss interventions in older adults with obesity. J. Nutr. Gerontol. Geriatr. 2019, 38, 50–68. [Google Scholar] [CrossRef]
- Reljic, D.; Wittmann, F.; Fischer, J.E. Effects of low-volume high-intensity interval training in a community setting: A pilot study. Eur. J. Appl. Physiol. 2018, 118, 1153–1167. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Taylor and Francis: Routledge, UK, 1988. [Google Scholar]
- Cardoso, I.L.; Paulos, A.T. C reactive protein and cardiovascular disease. Int. Arch. Cardiovasc. Dis. 2017, 1, 003. [Google Scholar]
- National Institute for Health and Care Excellence (NICE). Weight Management: Lifestyle Services for Overweight or Obese Adults. In Public Health Guideline PH53; National Institute for Health and Care Excellence: London, UK, 2014; Available online: https://www.nice.org.uk/guidance/ph53 (accessed on 3 March 2022).
- Bianchi, V.E. Weight loss is a critical factor to reduce inflammation. Clin. Nutr. ESPEN 2018, 28, 21–35. [Google Scholar] [CrossRef]
- Williamson, D.A.; Bray, G.A.; Ryan, D.H. Is 5% weight loss a satisfactory criterion to define clinically significant weight loss? Obesity 2015, 23, 2319–2320. [Google Scholar] [CrossRef] [Green Version]
- Davidson, L.E.; Hunt, S.C.; Adams, T.D. Fitness versus adiposity in cardiovascular disease risk. Eur. J. Clin. Nutr. 2019, 73, 225–230. [Google Scholar] [CrossRef]
- Ross, R.; Janiszewski, P.M. Is weight loss the optimal target for obesity-related cardiovascular disease risk reduction? Can. J. Cardiol. 2008, 24 (Suppl. D), 25D–31D. [Google Scholar] [CrossRef] [Green Version]
- Baskin, K.K.; Winders, B.R.; Olson, E.N. Muscle as a “mediator” of systemic metabolism. Cell. Metab. 2015, 21, 237–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reina, I.G.; Sanchez-Oliver, A.J.; Gonzalez-Matarin, P.J.; Butragueno, J.; Merchan, B.B.; Suarez-Carmona, W.; Isidro-Donate, F.; Tinahones, F.J.; Macias-Gonzalez, M. The role of muscle tissue and resistance training in cardiometabolic health. Int. J. Sports Sci. Med. 2019, 3, 1–12. [Google Scholar]
- Tuttle, C.S.L.; Thang, L.A.N.; Maier, A.B. Markers of inflammation and their association with muscle strength and mass: A systematic review and meta-analysis. Ageing Res. Rev. 2020, 64, 101185. [Google Scholar] [CrossRef]
- Pedersen, B.K. Anti-inflammatory effects of exercise: Role in diabetes and cardiovascular disease. Eur. J. Clin. Invest. 2017, 47, 600–611. [Google Scholar] [CrossRef] [Green Version]
- Cava, E.; Yeat, N.C.; Mittendorfer, B. Preserving healthy muscle during weight loss. Adv. Nutr. 2017, 8, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Sabag, A.; Little, J.P.; Johnson, N.A. Low-volume high-intensity interval training for cardiometabolic health. J. Physiol. 2022, 600, 1013–1026. [Google Scholar] [CrossRef]
- Phillips, W.T.; Ziuraitis, J.R. Energy cost of the ACSM single-set resistance training protocol. J. Strength Cond. Res. 2003, 17, 350–355. [Google Scholar] [CrossRef]
- Kemmler, W.; von Stengel, S.; Schwarz, J.; Mayhew, J.L. Effect of whole-body electromyostimulation on energy expenditure during exercise. J. Strength Cond. Res. 2012, 26, 240–245. [Google Scholar] [CrossRef] [Green Version]
- Boutcher, S.H. High-intensity intermittent exercise and fat loss. J. Obes. 2011, 2011, 868305. [Google Scholar] [CrossRef] [Green Version]
- Kolnes, K.J.; Petersen, M.H.; Lien-Iversen, T.; Højlund, K.; Jensen, J. Effect of exercise training on fat loss-energetic perspectives and the role of improved adipose tissue function and body fat distribution. Front. Physiol. 2021, 12, 737709. [Google Scholar] [CrossRef] [PubMed]
- Panissa, V.L.G.; Fukuda, D.H.; Staibano, V.; Marques, M.; Franchini, E. Magnitude and duration of excess of post-exercise oxygen consumption between high-intensity interval and moderate-intensity continuous exercise: A systematic review. Obes. Rev. 2021, 22, e13099. [Google Scholar] [CrossRef] [PubMed]
- Greer, B.K.; O’Brien, J.; Hornbuckle, L.M.; Panton, L.B. EPOC comparison between resistance training and high-intensity interval training in aerobically fit women. Int. J. Exerc. Sci. 2021, 14, 1027–1035. [Google Scholar]
- Callahan, M.J.; Parr, E.B.; Hawley, J.A.; Camera, D.M. Can high-intensity interval training promote skeletal muscle anabolism? Sports Med. 2021, 51, 405–421. [Google Scholar] [CrossRef]
- Kennedy, A.B.; Lavie, C.J.; Blair, S.N. Fitness or fatness: Which is more important? JAMA 2018, 319, 231–232. [Google Scholar] [CrossRef] [PubMed]
- Lee, J. Influences of cardiovascular fitness and body fatness on the risk of metabolic syndrome: A systematic review and meta-analysis. Am. J. Health Promot. 2020, 34, 796–805. [Google Scholar] [CrossRef] [PubMed]
- Martland, R.M.; Mondelli, V.; Gaughran, F.; Stubbs, B. Can high-intensity interval training improve physical and mental health outcomes? A meta-review of 33 systematic reviews across the lifespan. J. Sports Sci. 2020, 38, 430–469. [Google Scholar] [CrossRef]
- Mattioni Maturana, F.; Martus, P.; Zipfel, S.; Nieß, A.M. Effectiveness of HIIE versus MICT in improving cardiometabolic risk factors in health and disease: A meta-analysis. Med. Sci. Sports Exerc. 2021, 53, 559–573. [Google Scholar] [CrossRef]
- Khalafi, M.; Symonds, M.E. The impact of high-intensity interval training on inflammatory markers in metabolic disorders: A meta-analysis. Scand. J. Med. Sci. Sports 2020, 30, 2020–2036. [Google Scholar] [CrossRef]
- Leiva-Valderrama, J.M.; Montes-de-Oca-Garcia, A.; Opazo-Diaz, E.; Ponce-Gonzalez, J.G.; Molina-Torres, G.; Velázquez-Díaz, D.; Galán-Mercant, A. Effects of high-intensity interval training on inflammatory biomarkers in patients with type 2 diabetes. A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 12644. [Google Scholar] [CrossRef]
- Kelly, B.M.; Xenophontos, S.; King, J.A.; Nimmo, M.A. An evaluation of low volume high-intensity intermittent training (HIIT) for health risk reduction in overweight and obese men. BMC Obes. 2017, 4, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asle Mohammadi Zadeh, M.; Kargarfard, M.; Marandi, S.M.; Habibi, A. Diets along with interval training regimes improves inflammatory & anti-inflammatory condition in obesity with type 2 diabetes subjects. J. Diabetes Metab. Disord. 2018, 17, 253–267. [Google Scholar] [PubMed]
- Rose, G.L.; Skinner, T.L.; Mielke, G.I.; Schaumberg, M.A. The effect of exercise intensity on chronic inflammation: A systematic review and meta-analysis. J. Sci. Med. Sport 2021, 24, 345–351. [Google Scholar] [CrossRef]
- Langan, S.P.; Grosicki, G.J. Exercise is medicine…and the dose matters. Front. Physiol. 2021, 12, 660818. [Google Scholar] [CrossRef]
- Mirhafez, S.R.; Ebrahimi, M.; Saberi Karimian, M.; Avan, A.; Tayefi, M.; Heidari-Bakavoli, A.; Parizadeh, M.R.; Moohebati, M.; Azarpazhooh, M.R.; Esmaily, H.; et al. Serum high-sensitivity C-reactive protein as a biomarker in patients with metabolic syndrome: Evidence-based study with 7284 subjects. Eur. J. Clin. Nutr. 2016, 70, 1298–1304. [Google Scholar] [CrossRef]
- Srikanthan, K.; Feyh, A.; Visweshwar, H.; Shapiro, J.I.; Sodhi, K. Systematic review of metabolic syndrome biomarkers: A panel for early detection, management, and risk stratification in the West Virginian Population. Int. J. Med. Sci. 2016, 13, 25–38. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Quintela, A.; Alonso, M.; Campos, J.; Vizcaino, L.; Loidi, L.; Gude, F. Determinants of serum concentrations of lipopolysaccharide-binding protein (LBP) in the adult population: The role of obesity. PLoS ONE 2013, 8, e54600. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Lu, L.; Yao, P.; Ma, Y.; Wang, F.; Jin, Q.; Ye, X.; Li, H.; Hu, F.B.; Sun, L.; et al. Lipopolysaccharide binding protein, obesity status and incidence of metabolic syndrome: A prospective study among middle-aged and older Chinese. Diabetologia 2014, 57, 1834–1841. [Google Scholar] [CrossRef] [Green Version]
- Ruscica, M.; Ferri, N.; Macchi, C.; Corsini, A.; Sirtori, C.R. Lipid lowering drugs and inflammatory changes: An impact on cardiovascular outcomes? Ann. Med. 2018, 50, 461–484. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M. Canakinumab for residual inflammatory risk. Eur. Heart J. 2017, 38, 3545–3548. [Google Scholar] [CrossRef] [Green Version]
- Scheffer, D.D.L.; Latini, A. Exercise-induced immune system response: Anti-inflammatory status on peripheral and central organs. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165823. [Google Scholar] [CrossRef] [PubMed]
- Tsigalou, C.; Konstantinidis, T.; Paraschaki, A.; Stavropoulou, E.; Voidarou, C.; Bezirtzoglou, E. Mediterranean diet as a tool to combat inflammation and chronic diseases. An overview. Biomedicines 2020, 8, 201. [Google Scholar] [CrossRef]
- Boeno, F.P.; Ramis, T.R.; Munhoz, S.V.; Farinha, J.B.; Moritz, C.E.J.; Leal-Menezes, R.; Ribeiro, J.L.; Christou, D.D.; Reischak-Oliveira, A. Effect of aerobic and resistance exercise training on inflammation, endothelial function and ambulatory blood pressure in middle-aged hypertensive patients. J. Hypertens. 2020, 38, 2501–2509. [Google Scholar] [CrossRef] [PubMed]
- Wedell-Neergaard, A.S.; Krogh-Madsen, R.; Petersen, G.L.; Hansen, Å.M.; Pedersen, B.K.; Lund, R.; Bruunsgaard, H. Cardiorespiratory fitness and the metabolic syndrome: Roles of inflammation and abdominal obesity. PLoS ONE 2018, 13, e0194991. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, C.G., Jr.; Gomides, R.S.; Queiroz, A.C.; Pinto, L.G.; da Silveira Lobo, F.; Tinucci, T.; Mion, D., Jr.; de Moraes Forjaz, C.L. Acute and chronic effects of aerobic and resistance exercise on ambulatory blood pressure. Clinics 2010, 65, 317–325. [Google Scholar] [CrossRef] [Green Version]
- Law, M.R.; Morris, J.K.; Wald, N.J. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: Metaanalysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. Br. Med. J. 2009, 338, 1665. [Google Scholar] [CrossRef] [Green Version]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Bloodpressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Mengeste, A.M.; Rustan, A.C.; Lund, J. Skeletal muscle energy metabolism in obesity. Obesity 2021, 29, 1582–1595. [Google Scholar] [CrossRef]
- Mann, S.; Beedie, C.; Jimenez, A. Differential effects of aerobic exercise, resistance training and combined exercise modalities on cholesterol and the lipid profile: Review, synthesis and recommendations. Sports Med. 2014, 44, 211–221. [Google Scholar] [CrossRef] [Green Version]
- DeBoer, M.D.; Gurka, M.J.; Golden, S.H.; Musani, S.K.; Sims, M.; Vishnu, A.; Guo, Y.; Pearson, T.A. Independent associations between metabolic syndrome severity and future coronary heart disease by sex and race. J. Am. Coll. Cardiol. 2017, 69, 1204–1205. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Weißenfels, A.; Bebenek, M.; Fröhlich, M.; Kohl, M.; von Stengel, S. Effects of whole-body electromyostimulation versus high-intensity resistance exercise on body composition and strength: A randomized controlled study. Evid. Based Complement. Alternat. Med. 2016, 2016, 9236809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittmann, K.; Sieber, C.; von Stengel, S.; Kohl, M.; Freiberger, E.; Jakob, F.; Lell, M.; Engelke, K.; Kemmler, W. Impact of whole body electromyostimulation on cardiometabolic risk factors in older women with sarcopenic obesity: The randomized controlled FORMOsA-sarcopenic obesity study. Clin. Interv. Aging 2016, 11, 1697–1706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgs, C.; Skinner, M.; Hale, L. Outcomes of a community-based lifestyle programme for adults with diabetes or pre-diabetes. J. Prim. Health Care 2016, 8, 130–139. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variable | LOW-HIIT (n = 26) | 1-RT (n = 22) | 3-RT (n = 25) | WB-EMS (n = 26) | CON (n = 26) |
|---|---|---|---|---|---|
| Gender (f/m) | 10/16 | 16/6 | 15/10 | 18/8 | 18/8 |
| Age (years) | 50.6 ± 11.3 | 55.2 ± 12.1 | 52.7 ± 11.5 | 52.7 ± 12.5 | 49.0 ± 15.1 |
| BMI (kg/m2) | 37.8 ± 6.6 | 36.8 ± 7.4 | 40.1 ± 9.0 | 37.2 ± 4.0 | 38.0 ± 6.3 |
| CRP (mg/L) | 5.0 ± 3.4 | 6.1 ± 5.8 | 5.7 ± 6.3 | 4.1 ± 2.8 | 4.2 ± 3.3 |
| MetS z-score | 2.9 ± 3.9 | 3.4 ± 4.8 | 3.3 ± 4.3 | 2.6 ± 2.3 | 2.2 ± 3.1 |
| Variable | LOW-HIIT (n = 26) | 1-RT (n = 17) | 3-RT (n = 19) | WB-EMS (n = 20) | CON (n = 22) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Energy (kcal/day) | 2228 ± 896 | 1974 ± 801 | 2342 ± 907 | 1673 ± 520 a | 2344 ± 622 | 1769 ± 514 b | 2418 ± 695 | 1916 ± 415 b | 2237 ± 856 | 1798 ± 783 |
| Protein (g/day) | 92 ± 46 | 90 ± 31 | 102 ± 46 | 78 ± 28 a | 108 ± 41 | 80 ± 27 b | 96 ± 30 | 89 ± 31 | 94 ± 30 | 82 ± 33 |
| Protein (g/kg/day) | 0.8 ± 0.3 | 0.8 ± 0.3 | 0.9 ± 0.3 | 0.7 ± 0.3 | 1.0 ±0.4 | 0.8 ± 0.3 | 1.0 ± 0.5 | 0.8 ± 0.3 | 1.0 ± 0.3 | 0.9 ± 0.3 |
| Fat (g/day) | 89 ± 41 | 77 ± 36 | 97 ± 40 | 71 ± 28 | 96 ± 31 | 72 ± 26 b | 99 ± 40 | 80 ± 19 | 99 ± 57 | 70 ± 43 |
| Fat (g/kg/day) | 0.8 ± 0.3 | 0.7 ± 0.3 | 1.0 ± 0.4 | 0.8 ± 0.3 | 1.0 ± 0.4 | 0.8 ± 0.4 | 0.9 ± 0.4 | 0.8 ± 0.3 | 1.0 ± 0.5 | 0.7 ± 0.5 |
| CHO (g/day) | 216 ± 97 | 206 ± 92 | 237 ± 92 | 160 ± 51 b | 216 ± 58 | 170 ± 52 b | 249 ± 82 | 184 ± 61 a | 210 ± 76 | 180 ± 84 |
| CHO (g/kg/day) | 1.9 ± 0.7 | 1.8 ± 0.8 | 2.4 ± 0.7 | 1.8 ± 0.7 a | 2.4 ± 0.8 | 1.7 ± 0.7 b | 2.0 ± 0.7 | 1.6 ± 0.6 a | 2.1 ± 0.9 | 1.9 ± 1.0 |
| Fibres (g/day) | 23 ± 9 | 23 ± 11 | 24 ± 11 | 21 ± 8 | 23 ± 7 | 19 ± 7 | 22 ± 10 | 18 ± 7 | 24 ± 13 | 23 ± 10 |
| Variable | LOW-HIIT (n = 26) | 1-RT (n = 17) | 3-RT (n = 19) | WB-EMS (n = 20) | CON (n = 22) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Weight (kg) | 117.0 ± 26.1 | 113.0 ± 25.2 c | 102.9 ± 27.7 | 98.1 ± 26.0 b | 114.0 ± 30.1 | 110.3 ± 30.1 c | 106.1 ± 17.9 | 101.9 ± 14.6 c | 104.4 ± 20.5 | 101.5 ± 21.5 c |
| BMI (kg/m2) | 37.8 ± 6.6 | 36.5 ± 6.4 c | 36.5 ± 7.4 | 34.8 ± 7.1 b | 38.8 ± 8.1 | 37.5 ± 7.5 b | 37.3 ± 4.1 | 35.9 ± 3.2 c | 36.6 ± 5.2 | 35.5 ± 5.5 c |
| FM (kg) | 49.8 ± 14.8 | 46.3 ± 14.3 c,* | 47.7 ± 16.1 | 43.9 ± 14.8 b | 51.8 ± 16.6 | 48.0 ± 16.1 c,* | 46.0 ± 8.2 | 43.1 ± 6.1 b | 47.8 ± 11.5 | 45.7 ± 12.7 |
| FM (%) | 42.3 ± 7.6 | 40.7 ± 8.1 c,* | 45.8 ± 5.4 | 44.2 ± 5.7 b | 45.3 ± 6.6 | 43.3 ± 7.3 c,* | 43.6 ± 5.1 | 42.6 ± 5.0 b | 46.1 ± 7.0 | 44.9 ± 7.5 |
| SMM (kg) | 33.3 ± 9.0 | 32.8 ± 8.9 | 26.5 ± 7.8 | 25.8 ± 7.8 | 30.7 ± 10.4 | 30.6 ± 10.6 | 29.2 ± 7.0 | 28.3 ± 6.3 b | 27.5 ± 7.9 | 26.9 ± 7.9 c |
| TBW (L) | 50.0 ± 11.7 | 49.5 ± 11.7 | 41.6 ± 9.9 | 40.8 ± 9.9 | 46.7 ± 12.4 | 46.7 ± 12.8 c | 44.8 ± 9.1 | 43.9 ± 9.1 | 44.8 ± 10.8 | 43.9 ± 10.5 |
| Waist (cm) | 116 ± 19 | 110 ± 18 c,* | 111 ± 16 | 106 ± 14 c | 116 ± 18 | 111 ± 17 c,* | 114 ± 10 | 111 ± 9 b | 109 ± 11 | 107 ± 11 |
| Variable | LOW-HIIT (n = 26) | 1-RT (n = 17) | 3-RT (n = 19) | WB-EMS (n = 20) | CON (n = 22) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| CRP (mg/L) # | 5.0 ± 3.4 | 3.4 ± 2.7 b,* | 4.7 ± 4.8 | 4.5 ± 4.7 | 4.0 ± 3.3 | 3.7 ± 2.9 | 3.8 ± 2.4 | 3.4 ± 2.4 b | 3.9 ± 2.7 | 5.4 ± 8.0 |
| hsCRP (mg/L) # | 4.1 ± 3.1 | 2.7 ± 2.3 b,* | 4.0 ± 4.6 | 3.8 ± 4.6 | 3.3 ± 3.2 | 2.7 ± 2.5 a | 2.9 ± 2.0 | 2.6 ± 2.1 | 3.1 ± 2.4 | 4.4 ± 7.3 |
| IL-1β (pg/mL) | 6.3 ± 4.3 | 6.4 ± 3.8 | 9.7 ± 8.4 | 11.8 ± 9.8 | 9.8 ± 5.6 | 10.7 ± 6.5 | 10.0 ± 5.6 | 11.1 ± 8.3 | 6.7 ± 4.1 | 6.2 ± 3.8 |
| IL-6 (pg/mL) | 3.6 ± 3.0 | 2.5 ± 1.6 a | 2.8 ± 1.6 | 2.6 ± 1.7 | 2.6 ± 1.1 | 2.6 ± 1.6 | 2.5 ± 1.3 | 2.3 ± 1.2 | 3.1 ± 1.6 | 3.4 ± 3.0 |
| IFNγ (pg/mL) | 9.5 ± 6.8 | 8.8 ± 4.2 | 7.0 ± 4.1 | 6.4 ± 4.4 | 10.3 ± 9.4 | 9.1 ± 9.0 | 7.4 ± 2.9 | 7.2 ± 3.2 | 8.1 ± 4.5 | 7.5 ± 4.3 |
| Adiponectin [µ/mL) | 2.3 ± 1.3 | 2.2 ± 1.2 | 3.8 ± 2.7 | 3.9 ± 3.1 | 3.6 ± 3.0 | 3.2 ± 2.3 | 2.5 ± 1.5 | 2.4 ± 1.2 | 2.6 ± 1.3 | 2.6 ± 1.3 |
| LBP (ng/mL) # | 13.2 ± 2.5 | 11.1 ± 3.1 b,*,§ | 29.1 ± 7.6 | 28.0 ± 7.1 | 28.2 ± 3.6 | 26.3 ± 5.6 c | 23.6 ± 5.8 | 23.5 ± 5.8 | 16.9 ± 8.9 | 17.0 ± 9.4 |
| Variable | LOW-HIIT (n = 26) | 1-RT (n = 17) | 3-RT (n = 19) | WB-EMS (n = 20) | CON (n = 22) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Low risk (<1 mg/L) | 1 (3.8) | 6 (23.1) | 4 (23.5) | 6 (35.3) | 3 (15.8) | 4 (21.1) | 3 (15.0) | 3 (15.0) | 1 (4.5) | 3 (13.6) |
| Intermediate risk | 10 (38.5) | 13 (50.0) | 6 (25.3) | 3 (17.6) | 6 (31.6) | 7 (36.8) | 9 (45.0) | 10 (50.0) | 13 (59.1) | 8 (36.4) |
| (1–3 mg/L) | ||||||||||
| High risk | 15 (57.7) | 7 (26.9) | 7 (41.2) | 8 (47.1) | 7 (52.6) | 8 (42.1) | 8 (40.0) | 7 (35.0) | 8 (36.4) | 11 (50.0) |
| (>3 mg/L) | ||||||||||
| Variable | LOW-HIIT (n = 26) | 1-RT (n = 17) | 3-RT (n = 19) | WB-EMS (n = 20) | CON (n = 22) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| VO2max (mL/kg/min) # | 22.6 ± 5.5 | 25.6 ± 5.6 c,+ | 21.0 ± 5.4 | 22.2 ± 4.6 | 21.0 ± 5.1 | 22.0 ± 4.3 | 21.0 ± 5.7 | 21.7 ± 5.4 | 20.6 ± 7.4 | 20.2 ± 7.9 |
| MetS z-score # | 2.9 ± 3.8 | 1.1 ± 3.0 c,+ | 2.1 ± 3.8 | 0.5 ± 3.0 b | 2.8 ± 4.1 | 0.5 ± 3.9 c,+ | 2.3 ± 2.3 | 1.8 ± 2.3 | 2.0 ± 3.1 | 1.3 ± 3.0 |
| SBP (mmHg) # | 144 ± 17 | 133 ± 11 c | 148 ± 17 | 138 ± 12 | 142 ± 17 | 132 ± 16 b | 134 ± 14 | 137 ± 11 | 138 ± 13 | 137 ± 11 |
| DBP (mmHg) # | 94 ± 11 | 86 ± 8 c | 92 ± 16 | 87 ± 10 | 87 ± 9 | 83 ± 9 b | 86 ± 9 | 88 ± 10 | 89 ± 9 | 87 ± 7 |
| MAB (mmHg) # | 111 ± 11 | 102 ± 7 c | 111 ± 14 | 104 ± 9 a | 106 ± 11 | 99 ± 11 b | 102 ± 9 | 104 ± 9 | 105 ± 9 | 104 ± 7 |
| Glucose (mg/dL) | 101 ± 18 | 100 ± 12 | 96 ± 16 | 96 ± 12 | 105 ± 13 | 99 ± 14 a | 104 ± 12 | 102 ± 14 | 98 ± 15 | 95 ± 16 |
| Triglycerides (mg/dL) | 132 ± 56 | 128 ± 44 | 126 ± 43 | 119 ± 28 | 146 ± 89 | 124 ± 56 a | 133 ± 59 | 118 ± 36 | 148 ± 73 | 130 ± 64 |
| Cholesterol (mg/dL) | 214 ± 33 | 213 ± 35 | 228 ± 29 | 218 ± 33 | 227 ± 55 | 216 ± 45 b | 217 ± 35 | 210 ± 31 | 235 ± 42 | 222 ± 33 a |
| HDL (mg/dL) | 49 ± 10 | 48 ± 11 | 59 ± 19 | 59 ± 18 | 59 ± 17 | 58 ± 15 | 53 ± 14 | 52 ± 13 | 56 ± 12 | 54 ± 12 |
| LDL (mg/dL) | 144 ± 27 | 143 ± 27 | 148 ± 23 | 138 ± 22 a | 144 ± 39 | 137 ± 34 | 143 ± 28 | 137 ± 24 | 154 ± 33 | 147 ± 26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reljic, D.; Dieterich, W.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. “HIIT the Inflammation”: Comparative Effects of Low-Volume Interval Training and Resistance Exercises on Inflammatory Indices in Obese Metabolic Syndrome Patients Undergoing Caloric Restriction. Nutrients 2022, 14, 1996. https://doi.org/10.3390/nu14101996
Reljic D, Dieterich W, Herrmann HJ, Neurath MF, Zopf Y. “HIIT the Inflammation”: Comparative Effects of Low-Volume Interval Training and Resistance Exercises on Inflammatory Indices in Obese Metabolic Syndrome Patients Undergoing Caloric Restriction. Nutrients. 2022; 14(10):1996. https://doi.org/10.3390/nu14101996
Chicago/Turabian StyleReljic, Dejan, Walburga Dieterich, Hans J. Herrmann, Markus F. Neurath, and Yurdagül Zopf. 2022. "“HIIT the Inflammation”: Comparative Effects of Low-Volume Interval Training and Resistance Exercises on Inflammatory Indices in Obese Metabolic Syndrome Patients Undergoing Caloric Restriction" Nutrients 14, no. 10: 1996. https://doi.org/10.3390/nu14101996
APA StyleReljic, D., Dieterich, W., Herrmann, H. J., Neurath, M. F., & Zopf, Y. (2022). “HIIT the Inflammation”: Comparative Effects of Low-Volume Interval Training and Resistance Exercises on Inflammatory Indices in Obese Metabolic Syndrome Patients Undergoing Caloric Restriction. Nutrients, 14(10), 1996. https://doi.org/10.3390/nu14101996