
Vitamin D Deficiency Is Significantly Associated with Retinopathy in Type 2 Diabetes Mellitus: A Case-Control Study

 ,
,
Abstract
1. Introduction
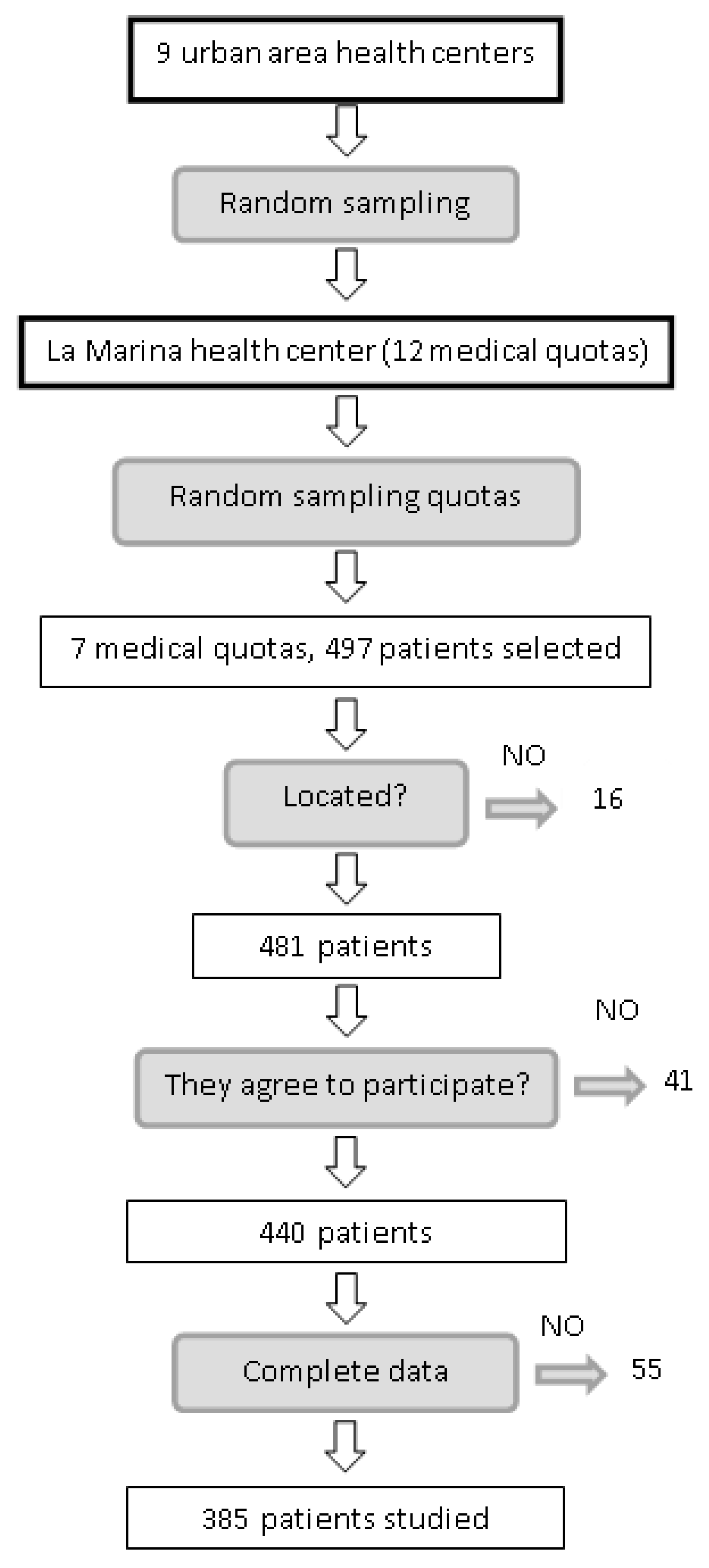
2. Methods
3. Results
3.1. Characteristics of the Study Sample
3.2. Variables Associated with DR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Financial Support
References
- Bourne, R.R.; Stevens, G.A.; White, R.A.; Smith, J.L.; Flaxman, S.R.; Price, H.; Jonas, J.B.; Keeffe, J.; Leasher, J.; Naidoo, K.; et al. Causes of visión loss worldwide. Syst. Anal. 2013, 1, e339–e349. [Google Scholar]
- Liew, G.; Michaelides, M.; Bunce, C. A comparison of the causes of blindness certifications in England and Wales in working age adults (16–64 years), 1999–2000 with 2009–2010. BMJ Open 2014, 4, e004015. [Google Scholar] [CrossRef] [PubMed]
- Quartilho, A.; Simkiss, P.; Zekite, A.; Xing, W.; Wormald, R.; Bunce, C. Leading causes of certifiable visual loss in England and Wales during the year ending 31 March 2013. Eye 2016, 30, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Wacker, M.; Holick, M.F. Vitamin D—Effects on skeletal and extraskeletal health and the need for supplementation. Nutrients 2013, 5, 111–148. [Google Scholar] [CrossRef] [PubMed]
- Haussler, M.R.; Livingston, S.; Sabir, Z.L.; Haussler, C.A.; Jurutka, P.W. Vitamin D Receptor Mediates a Myriad of Biological Actions Dependent on Its 1,25-Dihydroxyvitamin D Ligand: Distinct Regulatory Themes Revealed by Induction of Klotho and Fibroblast Growth Factor-23. JBMR Plus 2020, 5, e10432. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Scragg, R.; Sluyter, J.D. Is There Proof of Extraskeletal Benefits From Vitamin D Supplementation From Recent Mega Trials of Vitamin D? JBMR Plus 2021, 5, e10459. [Google Scholar] [CrossRef] [PubMed]
- Schöttker, B.; Ball, D.; Gellert, C.; Brenner, H. Serum 25-hydroxyvitamin D levels and overall mortality. A systematic review and meta-analysis of prospective cohort studies. Ageing Res. Rev. 2013, 12, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Keum, N.; Lee, D.H.; Greenwood, D.C.; Manson, J.E.; Giovannucci, E. Vitamin D supplementation and total cancer incidence and mortality: A meta-analysis of randomized controlled trials. Ann. Oncol. 2019, 30, 733–743. [Google Scholar] [CrossRef] [PubMed]
- Jolliffe, D.A.; Camargo, C.A., Jr.; Sluyter, J.D.; Aglipay, M.; Aloia, J.F.; Ganmaa, D.; Bergman, P.; Bischoff-Ferrari, H.A.; Borzutzky, A.; Damsgaard, C.T.; et al. Vitamin D supplementation to prevent acute respiratory infections: A systematic review and meta-analysis of aggregate data from randomised controlled trials. Lancet Diabetes Endocrinol. 2021, 9, 276–292. [Google Scholar] [CrossRef]
- Zhang, J.; Upala, S.; Sanguankeo, A. Relationship between vitamin D deficiency and diabetic retinopathy: A meta-analysis. Can. J. Ophthalmol. 2017, 52, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Luo, B.A.; Gao, F.; Qin, L.L. The Association between Vitamin D Deficiency and Diabetic Retinopathy in Type 2 Diabetes: A Meta-Analysis of Observational Studies. Nutrients 2017, 9, 307. [Google Scholar] [CrossRef] [PubMed]
- Alam, U.; Amjad, Y.; Chan, A.W.; Asghar, O.; Petropoulos, I.N.; Malik, R.A. Vitamin D Deficiency Is Not Associated with Diabetic Retinopathy or Maculopathy. J. Diabetes Res. 2016, 2016, 6156217. [Google Scholar] [CrossRef]
- Alcubierre, N.; Valls, J.; Rubinat, E.; Cao, G.; Esquerda, A.; Traveset, A.; Granado-Casas, M.; Jurjo, C.; Mauricio, D. Vitamin D Deficiency Is Associated with the Presence and Severity of Diabetic Retinopathy in Type 2 Diabetes Mellitus. J. Diabetes Res. 2015, 2015, 374178. [Google Scholar] [CrossRef]
- Herrmann, M.; Sullivan, D.R.; Veillard, A.-S.; McCorquodale, T.; Straub, I.R.; Scott, R.; Laakso, M.; Topliss, D.; Jenkins, A.; Blankenberg, S.; et al. Serum 25-hydroxyvitamin D: A predictor of macrovascular and microvascular complications in patients with type 2 diabetes. Diabetes Care 2015, 38, 521–528. [Google Scholar] [CrossRef]
- Zoppini, G.; Galletti, A.; Targher, G.; Brangani, C.; Pichiri, I.; Trombetta, M.; Negri, C.; De Santi, F.; Stoico, V.; Cacciatori, V.; et al. Lower levels of 25-hydroxyvitamin D3 are associated with a higher prevalence of microvascular complications in patients with type 2 diabetes. BMJ Open Diabetes Res. Care 2015, 3, e000058. [Google Scholar] [CrossRef] [PubMed]
- Engelen, L.; Schalkwijk, C.G.; Eussen, S.J.P.M.; Scheijen, J.L.J.M.; Soedamah-Muthu, S.S.; Chaturvedi, N.; Fuller, J.H.; Stehouwer, C.D.A. Low 25-hydroxyvitamin D2 and 25-hydroxyvitamin D3 levels are independently associated with macroalbuminuria, but not with retinopathy and macrovascular disease in type 1 diabetes: The EURODIAB prospective complications study. Cardiovasc. Diabetol. 2015, 14, 67. [Google Scholar] [CrossRef] [PubMed]
- Jee, D.; Han, K.D.; Kim, E.C. Inverse Association between High Blood 25-Hydroxyvitamin D Levels and Diabetic Retinopathy in a Representative Korean Population. PLoS ONE. 2014, 9, e115199. [Google Scholar] [CrossRef]
- Castillo Otí, J.M. Prevalencia y Factores de Riesgo Asociados a la Retinopatía Diabética en Cantabria. Ph.D. Thesis, Universidad de Cantabria, Santander, Spain, 2016. [Google Scholar]
- Yau, J.W.Y.; Rogers, S.L.; Kawasaki, R.; Lamoureux, E.L.; Kowalski, J.W.; Bek, T.; Chen, S.-J.; Dekker, J.M.; Fletcher, A.; Grauslund, J.; et al. Meta-Analysis for Eye Disease (META-EYE) Study Group. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012, 35, 556–564. [Google Scholar] [CrossRef]
- Navarro Valverde, C.; Quesada Gómez, J.M. Vitamin D Deficiency in Spain. Reality or Myth? Rev. Osteoporos. Metab. Min. 2014, 6, 5–10. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1889-836X2014000500002&Ing=es (accessed on 26 November 2021). [CrossRef]
- Aldington, S.J.; Kohner, E.M.; Meuer, S.; Klein, R.; Sjolie, A.K. Methodology for retinal photography and assessment of diabetic retinopathy: The EURODIAB IDDM complications study. Diabetología 1995, 38, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, C.P.; Ferris, F.L.; Klein, R.E.; Lee, P.P.; Agardh, C.D.; Davis, M.; Dills, D.; Kampik, A.; Pararajasegaram, R.; Verdaguer, J.T. Proposed International Clinical Diabetic Retinopathy and Diabetic Macular Edema Disease Severity Scales. Ophthalmology 2003, 110, 1677–1682. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of medical care in diabetes–2015. Diabetes Care 2015, 38, 49–57. [Google Scholar] [CrossRef]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; Lefevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. Evidence based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef]
- KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 5–14.
- Hosmer, D.W.; Lemeshow, S. Applied logistic regression. In Model-Building Strategies and Methods for Logistic Regression, 3rd ed.; Whiley: Hoboken, NJ, USA, 2013; Chapter 4; pp. 89–151. [Google Scholar]
- Hilbe, J.M. Logistic regression models. In Analysis of Model Fit; Chapman & Hall/CRC Press: Boca Raton, FL, USA, 2009; Chapter 7; pp. 243–296. [Google Scholar]
- Vittinghoff, E.; McCulloch, C.E. Relaxing the rule of ten events per variable in logistic and Cos regression. Am. J. Epidemiol. 2007, 165, 710–718. [Google Scholar] [CrossRef]
- He, R.; Shen, J.; Liu, F.; Zeng, H.; Li, L.; Yu, H.; Lu, H.; Wu, Q.; Jia, W. Vitamin D deficiency increases the risk of retinopathy in Chinese patients with type 2 diabetes. Diabet. Med. 2014, 31, 1657–1664. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Kotake, M.; Ono, Y.; Kato, T.; Oda, N.; Hayakawa, N.; Hashimoto, S.; Itoh, M. Hypovitaminosis D in type 2 diabetes mellitus: Association with microvascular complications and type of treatment. Endocr. J. 2006, 53, 503–510. [Google Scholar] [CrossRef]
- Kaur, H.; Donaghue, K.C.; Chan, A.K.; Benitez-Aguirre, P.; Hing, S.; Lloyd, M.; Cusumano, J.; Pryke, A.; Craig, M.E. Vitamin D deficiency is associated with retinopathy in children and adolescents with type 1 diabetes. Diabetes Care 2011, 34, 1400–1402. [Google Scholar] [CrossRef] [PubMed]
- Patrick, P.A.; Visintainer, P.F.; Shi, Q.; Weiss, I.A.; Brand, D.A. Vitamin D and retinopathy in adults with diabetes mellitus. Arch. Ophthalmol. 2012, 130, 756–760. [Google Scholar] [CrossRef]
- Ahmadieh, H.; Azar, S.T.; Lakkis, N.; Arabi, A. Hypovitaminosis D in Patients with Type 2 Diabetes Mellitus: A Relation to Disease Control and Complications. ISRN Endocrinol. 2013, 2013, 641098. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, S.; Singh, R.P.; Dwivedi, N.C.; Singh, K.; Gupta, A.; Mathur, M. Vitamin D levels and microvascular complications in type 2 diabetes. Indian J. Endocrinol. Metab. 2014, 18, 537–541. [Google Scholar] [CrossRef]
- Shimo, N.; Yasuda, T.; Kaneto, H.; Katakami, N.; Kuroda, A.; Sakamoto, F.; Takahara, M.; Irie, Y.; Horikawa, K.; Miyashita, K.; et al. Vitamin D deficiency is significantly associated with retinopathy in young Japanese type 1 diabetic patients. Diabetes Res. Clin. Pract. 2014, 106, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Usluogullari, C.A.; Balkan, F.; Caner, S.; Ucler, R.; Kaya, C.; Ersoy, R.; Cakir, B. The relationship between microvascular complications and vitamin D deficiency in type 2 diabetes mellitus. BMC Endocr. Disord. 2015, 15, 33. [Google Scholar] [CrossRef] [PubMed]
- Millen, A.E.; Sahli, M.W.; Nie, J.; LaMonte, M.J.; Lutsey, P.L.; Klein, B.E.K.; Mares, J.A.; Meyers, K.J.; Andrews, C.A.; Klein, R. Adequate vitamin D status is associated with the reduced odds of prevalent diabetic retinopathy in African Americans and Caucasians. Cardiovasc. Diabetol. 2016, 15, 128. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.H.; Kim, K.J.; Kim, B.Y.; Kim, C.H.; Kang, S.K.; Mok, J.O. Relationship between vitamin D status and vascular complications in patients with type 2 diabetes mellitus. Nutr. Res. 2016, 36, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Poncelas, A.; Miravet-Jiménez, S.; Casellas, A.; La Puente, J.F.B.-D.; Franch-Nadal, J.; López-Simarro, F.; Mata-Cases, M.; Mundet-Tudurí, X. Prevalence of diabetic retinopathy in individuals with type 2 diabetes who had recorded diabetic retinopathy from retinal photographs in Catalonia (Spain). Br. J. Ophthalmol. 2015, 99, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Romero-Aroca, P.; de la Riva-Fernández, S.; Valls-Mateu, A.; Sagarra-Alamo, R.; Moreno-Ribas, A.; Soler, N. Changes observed in diabetic retinopathy: Eight-year follow-up of a Spanish population. Br. J. Ophthalmol. 2016, 100, 1366–1371. [Google Scholar] [CrossRef] [PubMed]
- Romero-Aroca, P.; Fernández-Alart, J.; Baget-Bernaldiz, M.; Méndez-Marín, I.; Salvat-Serra, M. Diabetic Retinopathy Epidemiology in Type II Diabetic Patients. Effec of the Changes in the Diagnostic Criteria and the Stricter Control of the Diabetes between 1993 and 2005 on the Incidence of Diabetic Retinopathy. Arch. Soc. Esp. Oftalmol. 2007, 82, 209–218. [Google Scholar]
- Santos-Bueso, E.; Fernández-Pérez, C.; Macarro, A.; Fernández-Vigo, J. Prevalence of diabetic retinopathy in the city of Badajoz 2002 (Extremadura project to prevent blindness). Arch. Soc. Esp. Oftalmol. 2007, 82, 153–158. [Google Scholar] [PubMed]
- Thomas, R.L.; Dunstan, F.D.; Luzio, S.D.; Chowdhury, S.R.; North, R.V.; Hale, S.L.; Gibbins, R.L.; Owens, D.R. Prevalence of diabetic retinopathy within a national diabetic retinopathy screening service. Br. J. Ophthalmol. 2015, 99, 648. [Google Scholar] [CrossRef]
- Wong, T.Y.; Klein, R.; Islam, F.M.A.; Cotch, M.F.; Folsom, A.R.; Klein, B.E.; Sharrett, A.R.; Shea, S. Diabetic retinopathy in a multi-ethnic cohort in the United States. Am. J. Ophthalmol. 2006, 141, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Tapp, R.J.; Shaw, J.E.; Harper, C.A.; de Courten, M.P.; Balkau, B.; McCarty, D.J.; Taylor, H.R.; Welborn, T.A.; Zimmet, P.Z. The prevalence of and factors associated with diabetic retinopathy in the Australian population. Diabetes Care 2003, 26, 1731–1737. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, D.M.; Scott, J.A.; Vora, J.P.; Harding, S.P. Prevalence of diabetic eye disease in an inner city population: The Liverpool Diabetic Eye Study. Eye 1999, 13, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Mast, R.; Jansen, A.P.D.; Walraven, I.; Rauh, S.P.; Heijden, A.A.W.A.V.D.; Heine, R.J.; Elders, P.J.M.; Dekker, J.M.; Nijpels, G.; Hugtenburg, J.G. Time to insulin initiation and longterm effects of initiating insulin in people with type 2 diabetes mellitus: The Hoorn Diabetes Care.System Cohort Study. Eur. J. Endocrinol. 2016, 174, 563–571. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Total | No DR | DR | |
|---|---|---|---|---|
| No. (%) or mean (SD) | No. (%) or mean (SD) | No. (%) or mean (SD) | p-Value | |
| Age | 69.89 (9.86) | 69.54 (9.95) | 73.43 (8.08) | 0.040 |
| Sex | 0.592 | |||
| Men | 213 (55.30) | 195 (54.90) | 18 (60) | |
| Women | 172 (44.70) | 160 (45.10) | 12 (40) | |
| Years since diagnosis | 10.99 (7.06) | 10.69 (6.89) | 14.57 (8.11) | 0.016 |
| Body mass index | 29.90 (4.77) | 29.98 (4.85) | 28.94 (3.76) | 0.164 |
| HbA1c a | 6.71 (6.17, 7.40) | 6.68 (6.13, 7.33) | 7.29 (6.68, 8.08) | 0.001 |
| 25(OH)D a | 20 (13.3, 28) | 20.80 (14, 28) | 15.50 (10.8, 23.3) | 0.013 |
| <10 ng/mL | 28 (7.30) | 22 (6.20) | 6(20) | |
| 10–31.99 | 289 (75.10) | 267 (75.20) | 22 (73.30) | |
| ≥32 ng/mL | 68 (17.70) | 66 (18.60) | 2 (6.70) | |
| 1,25(OH)2D pg/mL a | 33 (20–53) | 35 (21, 54) | 24.50 (13, 38.25) | 0.021 |
| Patients on insulin | 70 (18.20) | 53 (14.90) | 17 (56.70) | <0.001 |
| HBP | 306 (79.50) | 276(77.70) | 30 (100) | 0.004 |
| Dyslipidemia | 255 (66.20) | 239 (67.30) | 16 (53.30) | 0.120 |
| Smoking | 58 (16.34) | 54 (15.20) | 4 (13.30) | 0.838 |
| Cardiovascular events | 134 (34.80) | 118 (33.20) | 16 (53.30) | 0.027 |
| Kidney failure | 91 (23.60) | 78 (22) | 13 (43.30) | 0.008 |
| Diabetic retinopathy | 30 (7.80) |
| OR | 95% CI | p-Value | |
|---|---|---|---|
| Female sex | 0.813 | 0.380, 1.737 | 0.592 |
| Age (years) | 1.044 | 1.002, 1.089 | 0.041 |
| Age at diagnosis | 1.000 | 0.964, 1.036 | 0.987 |
| Years since diagnosis | 1.062 | 1.018, 1.107 | 0.005 |
| Body mass index | 0.952 | 0.877, 1.034 | 0.237 |
| Normal weight (reference value) | 0.230 | ||
| Obesity G-1 | 1.330 | 0.426, 4.152 | 0.624 |
| Obesity G-2 | 0.639 | 0.188, 2.169 | 0.473 |
| Glycemic control | |||
| HbA1c(<7) (reference) | 0.005 | ||
| HbA1c (7–7.9) | 2.911 | 1.216, 6.968 | 0.016 |
| HbA1c (8–10) | 5.148 | 1.827, 14.511 | 0.002 |
| HbA1c (>10) | 11.400 | 0.952, 136.482 | 0.055 |
| Treatment of diabetes | |||
| Diet (reference value) | <0.001 | ||
| OAD | 2.324 | 0.295, 18.286 | 0.423 |
| Insulin | 21.778 | 2.542, 186.566 | 0.005 |
| OAD + insulin | 12.600 | 1.526, 104.035 | 0.019 |
| HBP (yes) | 4.984 | 1.175, 21.130 | 0.029 |
| Cardiovascular events (yes) | 2.295 | 1.084, 4.862 | 0.030 |
| No events (reference value) | 0.073 | ||
| 1 event | 1.929 | 0.804, 4.628 | 0.141 |
| 2 events | 3.276 | 1.173, 9.150 | 0.024 |
| 3 events | -- | -- | -- |
| 4 events | 16.929 | 1.005, 285.073 | 0.050 |
| Dyslipidemia | |||
| Good control (reference value) | 0.802 | ||
| Poor control 1 factor | 0.633 | 0.245, 1.635 | 0.345 |
| Poor control 2 factor | 0.688 | 0.248, 1.909 | 0.473 |
| Poor control 3 factor | 0.619 | 0.185, 2.068 | 0.436 |
| Kidney disease | |||
| Normal (reference value) | 0.109 | ||
| Grade 2 (mild) | 1.849 | 0.589, 5.807 | 0.293 |
| Grade 3a | 2.696 | 0.840, 8.655 | 0.096 |
| Grade 3b | 4.044 | 1.218, 13.429 | 0.022 |
| Grade 4 | 8.088 | 0.698, 93.722 | 0.094 |
| Grade 5 | -- | -- | -- |
| Smoking | 0.892 | 0.299, 2.665 | 0.838 |
| 25(OH)D | 0.947 | 0.906, 0.991 | 0.018 |
| 25(OH)D Categorized | |||
| >16 ng/mL (reference value) | 0.001 | ||
| ≤16 ng/mL | 2.427 | 1.142, 5.160 | 0.021 |
| 1,25(OH)2D | |||
| >29 pg/mL (reference value) | 0.001 | ||
| ≤29 pg/mL | 3.313 | 1.338, 8.205 | 0.010 |
| Variable | p-Value | OR | 95% CI |
|---|---|---|---|
| 25(OH)D > 16 ng/mL and 1,25(OH)2D > 29 pg/mL | 0.011 | ||
| 25(OH)D > 16 a and 1,25(OH)2D ≤ 29 b | 0.882 | 1.14 | 0.21, 6.04 |
| 25(OH)D ≤ 16 a and 1,25(OH)2D > 29 b | 0.341 | 1.85 | 0.52, 6.61 |
| 25(OH)D ≤ 16 a and 1,25(OH)2D ≤ 29 | 0.003 | 5.21 | 1.76, 15.42 |
| Constant | <0.001 | 0.04 |
| p-Value | OR | 95% CI | AUC (%) | |
|---|---|---|---|---|
| Model 1 | 76.3 | |||
| Treatment of diabetes (reference: Diet) | 0.000 | |||
| Oral antidiabetic drugs (OAD) | 0.436 | 2.28 | 0.29, 18.11 | |
| Insulin | 0.004 | 24.93 | 2.80, 221.65 | |
| OAD + insulin | 0.028 | 10.95 | 1.30, 92.32 | |
| HBP (reference: Normal BP) | 0.167 | |||
| Stage 1 | 0.073 | 2.28 | 0.93, 5.62 | |
| Stage 2 | 0.229 | 2.62 | 0.55, 12.58 | |
| Levels of 25(OH)D (≤16 ng/mL) | 0.027 | 2.47 | 1.11, 5.52 | |
| Model 2 | 78.2 | |||
| Treatment of diabetes (reference: Diet) | 0001 | |||
| Oral antidiabetic drugs (OAD) | 0.660 | 1.60 | 0.20, 13.02 | |
| Insulin | 0.035 | 11.65 | 1.18, 114.64 | |
| OAD + insulin | 0.055 | 8.23 | 0.96, 70.78 | |
| HBP (reference: Normal BP) | 0.150 | |||
| Stage 1 | 0.068 | 2.57 | 0.93, 7.10 | |
| Stage 2 | 0.172 | 3.22 | 0.60, 17.26 | |
| Levels of 1,25(OH)2D (<29 pg/mL) | 0.038 | 2.73 | 1.06, 7.07 | |
| Model 3 | 79.3 | |||
| Treatment of diabetes (reference: Diet) | 0.001 | |||
| Oral antidiabetic drugs (OAD) | 0.523 | 1.99 | 0.24, 16.54 | |
| Insulin | 0.022 | 15.15 | 1.49, 154.15 | |
| OAD + Insulin | 0.041 | 9.67 | 1.10, 85.10 | |
| HBP (reference: Normal BP) | 0.145 | |||
| Stage 1 | 0.064 | 2.66 | 0.94, 7.48 | |
| Stage 2 | 0.181 | 3.26 | 0.58, 18.47 | |
| 25(OH)D > 16 ng/mL and 1,25(OH)2D > 29 pg/mL | 0.046 | |||
| 25(OH)D > 16 a and 1,25(OH)2D ≤ 29 b | 0.507 | 1.57 | 0.41, 5.99 | |
| 25(OH)D ≤ 16 a and 1,25(OH)2D > 29 b | 0.706 | 1.39 | 0.25, 7.77 | |
| 25(OH)D ≤ 16 a and 1,25(OH)2D ≤ 29 b | 0.010 | 4.48 | 1.43, 13.99 |
| p-Value | OR | 95% CI | |
|---|---|---|---|
| Diet or OAD (reference) | <0.001 | ||
| Insulin analogues | <0.001 | 5.65 | 2.26, 14.12 |
| Human insulin | <0.001 | 12.39 | 4.46, 34.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castillo-Otí, J.M.; Galván-Manso, A.I.; Callejas-Herrero, M.R.; Vara-González, L.A.; Salas-Herrera, F.; Muñoz-Cacho, P. Vitamin D Deficiency Is Significantly Associated with Retinopathy in Type 2 Diabetes Mellitus: A Case-Control Study. Nutrients 2022, 14, 84. https://doi.org/10.3390/nu14010084
Castillo-Otí JM, Galván-Manso AI, Callejas-Herrero MR, Vara-González LA, Salas-Herrera F, Muñoz-Cacho P. Vitamin D Deficiency Is Significantly Associated with Retinopathy in Type 2 Diabetes Mellitus: A Case-Control Study. Nutrients. 2022; 14(1):84. https://doi.org/10.3390/nu14010084
Chicago/Turabian StyleCastillo-Otí, José M., Ana I. Galván-Manso, María R. Callejas-Herrero, Luís A. Vara-González, Fernando Salas-Herrera, and Pedro Muñoz-Cacho. 2022. "Vitamin D Deficiency Is Significantly Associated with Retinopathy in Type 2 Diabetes Mellitus: A Case-Control Study" Nutrients 14, no. 1: 84. https://doi.org/10.3390/nu14010084
APA StyleCastillo-Otí, J. M., Galván-Manso, A. I., Callejas-Herrero, M. R., Vara-González, L. A., Salas-Herrera, F., & Muñoz-Cacho, P. (2022). Vitamin D Deficiency Is Significantly Associated with Retinopathy in Type 2 Diabetes Mellitus: A Case-Control Study. Nutrients, 14(1), 84. https://doi.org/10.3390/nu14010084