
Nutritional Status and Serum Levels of Micronutrients in an Elderly Group Who Participate in the Program for Complementary Food in Older People (PACAM) from the Metropolitan Region, Santiago de Chile

 , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
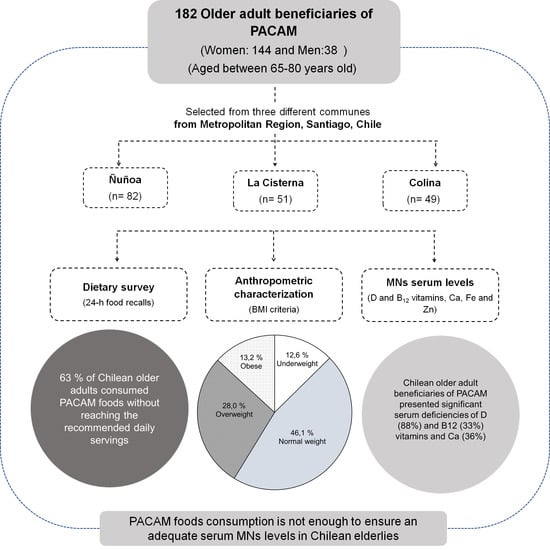
2.1. Setting and Sampling
2.2. Nutritional Status of the Elderly
2.3. Dietary and Nutrients Intake of the Elderly
2.4. Serum Micronutrients Status of the Elderly
2.5. Statistical Methods
2.6. Ethical Considerations
3. Results
3.1. Sample Characteristics and Nutritional Status
3.2. Micronutrient Intake
3.3. Serum Levels and Deficit of Micronutrients
4. Discussion
4.1. Nutritional Status
4.2. Micronutrient Intake
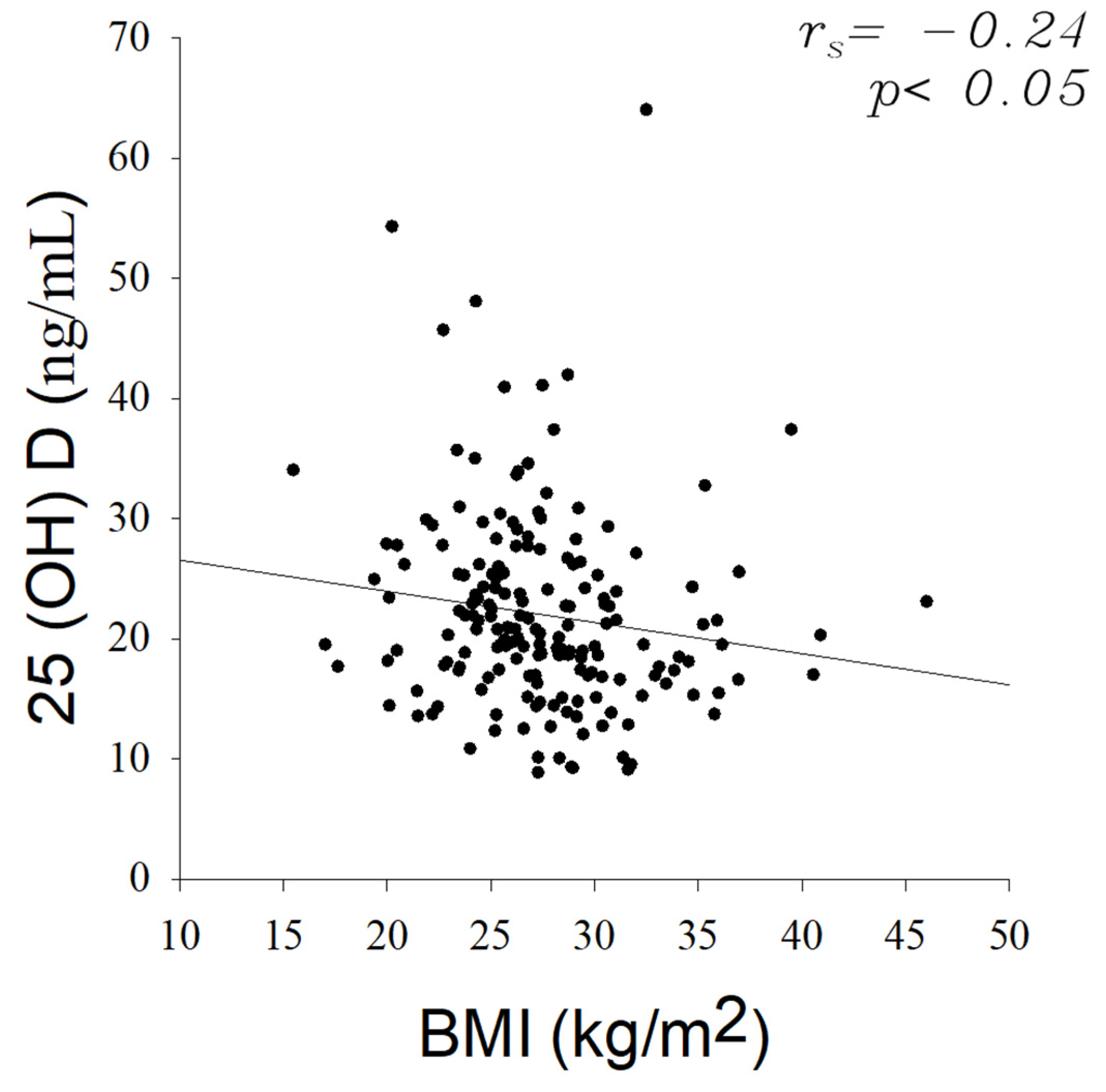
4.3. Serum Levels and Deficit of Micronutrients
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Global Strategy and Action Plan on Ageing and Health. 2017. Available online: https://www.who.int/ageing/WHO-GSAP-2017.pdf?ua=1 (accessed on 29 November 2021).
- Da Silva, W.A.A.; Barbosa, K.T.F.; De Oliveira, F.M.R.L.; De Brito, F.M.; Ramos, S.S.N.D.L.; Fernandes, A.M.; Fontana, N.; De Lacerda, H.J.M.; De Soares, L.C.; Nunes, T.B. Personal and behavioral determinants of active aging. Int. Arch. Med. 2016, 9, 1–10. [Google Scholar] [CrossRef]
- Hernández-Olivas, E.; Muñoz-Pina, S.; Sánchez-García, J.; Andrés, A.; Heredia, A. Understanding the role of food matrix on the digestibility of dairy products under elderly gastrointestinal conditions. Food Res. Int. 2020, 137, 109454. [Google Scholar] [CrossRef]
- INE. Estimaciones y Proyecciones de La Población de Chile 2002-2035 Totales Regionales, Población Urbana y Rural. Síntesis de Resultados. 2019. Available online: https://www.ine.cl/docs/default-source/proyecciones-de-poblacion/publicaciones-y-anuarios/base-2017/ine_estimaciones-y-proyecciones-2002-2035_base-2017_reg_%C3%A1rea_s%C3%ADntesis.pdf?sfvrsn=aaeb88e7_5 (accessed on 29 November 2021).
- United Nations, Department of Economic and Social Affairs, P.D. World Population Prospects: The 2015 Revision, Key Findings and Advance Tables. Working Paper No ESA/P/WP.241. 2015. Available online: https://population.un.org/wpp/publications/files/key_findings_wpp_2015.pdf (accessed on 29 November 2021).
- Sanchez, H.; Albala, C.; Lera, L.; Dangour, A.D.; Uauy, R. Effectiveness of the National Program of Complementary Feeding for Older Adults in Chile on Vitamin B12 Status in Older Adults; Secondary Outcome Analysis from the CENEX Study (ISRCTN48153354). Nutr. J. 2013, 12, 124. [Google Scholar] [CrossRef]
- Ministerio de Salud. Programa de Alimentación Complementaria Del Adulto Mayor; Ministerio de Salud: Santiago, Chile, 2001; pp. 1–67.
- Dangour, A.D.; Moreno, X.; Albala, C.; Rivera-Marquez, A.; Lera, L.; Villalobos, A.; Morris, S.S.; Uauy, R. Chile’s National Nutritional Supplementation Program for Older People: Lessons Learned. Food Nutr. Bull. 2005, 26, 190–197. [Google Scholar] [CrossRef]
- Masi, C.; Atalah, E. Análisis de La Aceptabilidad, Consumo y Aporte Nutricional Del Programa Alimentario Del Adulto Mayor. Rev. Méd. Chil. 2008, 136, 415–422. [Google Scholar] [CrossRef][Green Version]
- Russell, R.M. Factors in Aging That Effect the Bioavailability of Nutrients. J. Nutr. 2001, 131, 1359–1361. [Google Scholar] [CrossRef]
- Ministerio de Salud (MINSAL). Guía Clínica Examen de Medicina Preventiva; Ministerio de Salud: Santiago, Chile, 2008.
- Naska, A.; Lagiou, A.; Lagiou, P. Dietary Assessment Methods in Epidemiological Research: Current State of the Art and Future Prospects. F1000Research 2017, 6, 926. [Google Scholar] [CrossRef] [PubMed]
- Cerda, R.; Barrero, C.; Arena, M.; Bascuñán, K.; Jiménez, C. Atlas Fotográfico de Alimentos y Preparaciones Típicas Chilenas. Encuesta Nacional de Consumo Alimentario 2010; Ministerio de Salud: Santiago, Chile, 2010; p. 143.
- Milla, P.G.; Johns, P.C.; Agüero, S.D. Asociación Del Consumo de Desayuno y La Calidad de Vida En Adultos Mayores Autonomos Chilenos. Nutr. Hosp. 2014, 30, 845–850. [Google Scholar] [CrossRef]
- FAO/WHO Expert Consultation. Human Vitamin and Mineral Requirements, 2nd ed.; World Health Organization: Geneva, Switzerland, 2005; p. 341. [Google Scholar]
- Durán, S.; Alejandra Ulloa, A.; Sussanne Reyes, G. Comparación Del Consumo de Vitaminas y Minerales En Adultos Mayores Chilenos Según Estado Nutricional. Rev. Med. Chil. 2014, 142, 1594–1602. [Google Scholar] [CrossRef] [PubMed][Green Version]
- World Health Organization. Guidelines on Food Fortification with Micronutrients; World Health Organization, Food and Agricultural Organization of the United Nations: Geneva, Switzerland, 2006.
- Akbulut, G.; Ersoy, G. Assessment of nutrition and life quality scores of individuals aged 65 and over from different socio-economic levels in Turkey. Arch. Gerontol. Geriatr. 2008, 47, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Seidell, J.C.; Visscher, T.L.S. Body Weight and Weight Change and Their Health Implications for the Elderly. Eur. J. Clin. Nutr. 2000, 54, S33–S39. [Google Scholar] [CrossRef]
- Green, S.M.; Watson, R. Nutritional Screening and Assessment Tools for Use by Nurses: Literature Review. J. Adv. Nurs. 2005, 50, 69–83. [Google Scholar] [CrossRef]
- Donini, L.M.; De Felice, M.R. and Cannella, C. Nutritional Status Determinants and Cognition in the Elderly. Arch. Gerontol. Geriatr. 2007, 44, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health (Chile). Encuesta Nacional de Salud 2016–2017 Primeros Resultados; Ministerio de Salud: Santiago, Chile, 2017.
- Agüero, S.D.; Leiva, A.V. Caracterización Antropométrica, Calidad y Estilos de Vida Del Anciano Chileno Octogenario. Nutr. Hosp. 2015, 31, 2554–2560. [Google Scholar] [CrossRef]
- Albala, C.; Sánchez, H.; Lera, L.; Angel, B.; Cea, X. Socioeconomic Inequalities in Active Life Expectancy and Disability Related to Obesity among Older People. Rev. Med. Chil. 2011, 139, 1276–1285. [Google Scholar] [CrossRef] [PubMed]
- Salazar, N.; Arboleya, S.; Fernández-Navarro, T.; de los Reyes-Gavilán, C.G.; Gonzalez, S.; Gueimonde, M. Age-Associated Changes in Gut Microbiota and Dietary Components Related with the Immune System in Adulthood and Old Age: A Cross-Sectional Study. Nutrients 2019, 11, 1765. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Kamath, V. The Influences of Age on Olfaction: A Review. Front. Psychol. 2014, 5, 20. [Google Scholar] [CrossRef]
- González, C.N.; Peñad’Ardaillon, F.; Durán Agüero, S. Caracterización de La Ingesta de Alimentos y Nutrientes En Adultos Mayores Chilenos. Rev. Chil. Nutr. 2016, 43, 346–352. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; Sisto, A.; Marzetti, E. Anorexia of Aging: Risk Factors, Consequences, and Potential Treatments. Nutrients 2016, 8, 69. [Google Scholar] [CrossRef] [PubMed]
- Olivares, M.; Lera, L.; Albala, C.; Pizarro, F.; Araya, M. Prevalencia de Las Deficiencias de Zinc y Cobre En Adultos Mayores de La Región Metropolitana de Santiago. Rev. Med. Chil. 2011, 139, 283–289. [Google Scholar] [CrossRef]
- Charlton, K.E.; Bourne, L.T.; Steyn, K.; Laubscher, J.A. Poor Nutritional Status in Older Black South Africans. Asia Pac. J. Clin. Nutr. 2001, 10, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhao, L.; Man, Q.; Wang, J.; Zhao, W.; Zhang, J. Dietary Micronutrients Intake Status among Chinese Elderly People Living at Home: Data from CNNHS 2010–2012. Nutrients 2019, 11, 1787. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.L.; Maisey, S.; Southon, S.; Wright, A.J.A.; Finglas, P.M.; Fulcher, R.A. Relationships between Micronutrient Intake and Biochemical Indicators of Nutrient Adequacy in a ‘Free-Living’ Elderly UK Population. Br. J. Nutr. 1997, 77, 225–242. [Google Scholar] [CrossRef]
- Asamane, E.A.; Greig, C.A.; Thompson, J.L. The Association between Nutrient Intake, Nutritional Status and Physical Function of Community-Dwelling Ethnically Diverse Older Adults. BMC Nutr. 2020, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Yannakoulia, M.; Mamalaki, E.; Anastasiou, C.A.; Mourtzi, N.; Lambrinoudaki, I.; Scarmeas, N. Eating Habits and Behaviors of Older People: Where Are We Now and Where Should We Go? Maturitas 2018, 114, 14–21. [Google Scholar] [CrossRef]
- Troncoso, C.; Petermann-Rocha, F.; Brown, R.; Leiva, A.M.; Martinez, M.A.; Diaz-Martinez, X.; Garrido-Mendez, A.; Poblete-Valderrama, F.; Iturra-Gonzalez, J.A.; Villagran, M.; et al. Patterns of Healthy Lifestyle Behaviours in Older Adults: Findings from the Chilean National Health Survey 2009–2010. Exp. Gerontol. 2018, 113, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Echeverría, G.; Dussaillant, C.; McGee, E.E.; Mena, C.; Nitsche, M.P.; Urquiaga, I.; Bitran, M.; Pedrals, N.; Rigotti, A. Promoting and Implementing the Mediterranean Diet in the Southern Hemisphere: The Chilean Experience. Eur. J. Clin. Nutr. 2019, 72, 38–46. [Google Scholar] [CrossRef]
- Programa de Alimentación Complementaria del Adulto Mayor. BASES PACAM; Ministerio de Salud: Santiago, Chile, 2021.
- Hossein-Nezhad, A.; Holick, M.F. Vitamin D for Health: A Global Perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef]
- Meehan, M.; Penckofer, S. The Role of Vitamin D in the Aging Adult. J. Aging Gerontol. 2014, 2, 60–71. [Google Scholar] [CrossRef]
- Allen, L.H. How Common Is Vitamin B-12 Deficiency? Am. J. Clin. Nutr. 2009, 89, 693–696. [Google Scholar] [CrossRef]
- Lachner, C.; Steinle, N.I.; Regenold, W.T. The Neuropsychiatry of Vitamin B 12 Deficiency in Elderly Patients. J. Neuropsychiatry Clin. Neurosci. 2012, 24, 5–15. [Google Scholar] [CrossRef]
- Carrasco, M.; Domínguez De, A.; Martínez, G.; Ihle, S.; Rojas, V.; Foradori, A.; Marín, P.P. Vitamin D Levels in Older Healthy Chilean Adults and Their Association with Functional Performance. Niveles de Vitamina D En Adultos Mayores Saludables Chilenos y Su Relación Con Desempeño Funcional. Rev. Med. Chil. 2014, 142, 1385–1391. [Google Scholar] [CrossRef]
- Eussen, S.J.P.M.; De Groot, L.C.P.G.M.; Clarke, R.; Schneede, J.; Ueland, P.M.; Hoefnagels, W.H.L.; Van Staveren, W.A. Oral Cyanocobalamin Supplementation in Older People with Vitamin B 12 Deficiency: A Dose-Finding Trial. Arch. Intern. Med. 2005, 165, 1167–1172. [Google Scholar] [CrossRef] [PubMed]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased Bioavailability of Vitamin D in Obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef] [PubMed]
- Soskić, S.; Stokić, E.; Isenović, E.R. The Relationship between Vitamin D and Obesity. Curr. Med. Res. Opin. 2014, 30, 1197–1199. [Google Scholar] [CrossRef]
- Carrelli, A.; Bucovsky, M.; Horst, R.; Cremers, S.; Zhang, C.; Bessler, M.; Schrope, B.; Evanko, J.; Blanco, J.; Silverberg, S.; et al. Vitamin D Storage in Adipose Tissue of Obese and Normal Weight Women. Physiol. Behav. 2017, 32, 237–242. [Google Scholar] [CrossRef]
- Orces, C.H. The Association between Obesity and Vitamin D Status among Older Adults in Ecuador: Analysis of the SABE Survey. Nutr. Hosp. 2018, 35, 1066–1071. [Google Scholar] [CrossRef]
- Gonçalves, T.J.M.; Gonçalves, S.E.A.B.; Guarnieri, A.; Risegato, R.C.; Guimarães, M.P.; de Freitas, D.C.; Razuk-Filho, A.; Benedito Junior, P.B.; Parrillo, E.F. Prevalence of Obesity and Hypovitaminosis D in Elderly with Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Nutr. ESPEN 2020, 40, 110–114. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Duong, T.; Cauley, J.A.; Heaney, R.P.; Wolf, R.L.; Harris, E.; Cummings, S.R. Low Fractional Calcium Absorption Increases the Risk for Hip Fracture in Women with Low Calcium Intake. Ann. Intern. Med. 2000, 132, 345–353. [Google Scholar] [CrossRef]
- Veldurthy, V.; Wei, R.; Oz, L.; Dhawan, P.; Jeon, Y.H.; Christakos, S. Vitamin D, Calcium Homeostasis and Aging. Bone Res. 2016, 4, 16041. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P. Vitamin D and Calcium Interactions: Functional Outcomes. Am. J. Clin. Nutr. 2008, 88, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Tejwani, V.; Qian, Q. Calcium Regulation and Bone Mineral Metabolism in Elderly Patients with Chronic Kidney Disease. Nutrients 2013, 5, 1913–1936. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, F. Vitamin B12 Sources and Bioavailability. Exp. Biol. Med. 2007, 232, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- Dias, F.; Costa, S.O.; de Freitas, J.P.; Pinto, A.D.C.R.; Vigario, P.; Mainenti, M.R.M. Functional Capacity of Oldest Old Living in a Long-stay Institution in Rio De Janeiro, Brazil. J. Phys. Ther. Sci. 2014, 26, 1097–1105. [Google Scholar] [CrossRef][Green Version]
- Weaver, C.M.; Proulx, W.R.; Heaney, R. Choices for achieving adequate dietary calcium with a vegetarian diet. Am. J. Clin. Nutr. 1999, 70, 543s–548s. [Google Scholar] [CrossRef] [PubMed]
- Guéguen, L.; Pointillart, A. The Bioavailability of Dietary Calcium. J. Am. Coll. Nutr. 2000, 19, 119S–136S. [Google Scholar] [CrossRef]
- Antoine, T.; Icard-Vernière, C.; Scorrano, G.; Salhi, A.; Halimi, C.; Georgé, S.; Carrière, F.; Mouquet-Rivier, C.; Reboul, E. Evaluation of Vitamin D Bioaccessibility and Mineral Solubility from Test Meals Containing Meat and/or Cereals and/or Pulses Using in Vitro Digestion. Food Chem. 2021, 347, 128621. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Evaluated Parameters | Elderly Group | ||||
|---|---|---|---|---|---|
| n = 182 | |||||
| 25th Percentile | Median | 75th Percentile | 95th Percentile | ||
| BMI (kg/m2) | 24.85 | 27.22 | 29.61 | 35.92 | |
| Micronutrient intake | Recommended Daily Dose [15,16] | ||||
| Vitamin A (µg/day) | 700 (women) and 900 (men) | 246.06 | 381.67 | 596.45 | 1104.46 |
| Vitamin B12 (µg/day) | 2.40 | 1.29 | 1.95 | 2.89 | 4.81 |
| Vitamin D3 (µg/day) | 15 | 0.94 | 3.62 | 6.60 | 11.19 |
| Calcium (mg/day) | 1200 | 359.67 | 548.94 | 762.66 | 1348.73 |
| Zinc (mg/day) | 8 (women) and 11 (men) | 4.33 | 5.93 | 7.91 | 10.84 |
| Plasma micronutrient level | Normal values [17] | ||||
| Vitamin A (µg/dL) | 20–100 | 47.00 | 53.00 | 67.00 | 85.30 |
| Vitamin B12 (pg/mL) | 279–996 | 255.50 | 301.00 | 383.00 | 627.20 |
| [25(OH)D] (ng/mL) | 30–100 | 16.88 | 20.23 | 25.37 | 37.34 |
| Calcium (mg/dL) | 8.5–10.5 | 8.31 | 8.74 | 9.23 | 10.35 |
| Zinc (µg/dL) | 75–120 | 89.39 | 99.96 | 113.40 | 158.69 |
| Evaluated Parameters | Gender Group | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | |||||||||
| n = 38 | n = 144 | |||||||||
| 25th Percentile | Median | 75th Percentile | 95th Percentile | 25th Percentile | Median | 75th Percentile | 95th Percentile | |||
| BMI (kg/m2) | 24.03 | 26.85 | 28.99 | 35.08 | 24.94 | 27.27 | 30.13 | 35.94 | 0.26 | |
| Micronutrient intake | Recommended Daily Dose [15,16] | 25th percentile | Median | 75th percentile | 95th percentile | 25th percentile | Median | 75th percentile | 95th percentile | p-value |
| Vitamin A (µg/day) | 700 (women) and 900 (men) | 183.00 | 367.69 | 509.06 | 893.05 | 251.11 | 381.67 | 613.92 | 1229.34 | 0.52 |
| Vitamin B12 (µg/day) | 2.40 | 1.49 | 1.96 | 2.89 | 3.90 | 1.20 | 1.92 | 2.90 | 5.13 | 0.62 |
| Vitamin D3 (µg/day) | 15 | 0.78 | 3.48 | 6.79 | 9.66 | 0.91 | 3.47 | 6.33 | 11.43 | 0.52 |
| Calcium (mg/day) | 1200 | 322.08 | 477.15 | 723.32 | 1207.11 | 369.46 | 542.29 | 741.80 | 1443.72 | 1.00 |
| Zinc (mg/day) | 8 (women) and 11 (men) | 5.03 | 7.19 | 9.49 | 10.97 | 4.08 | 5.76 | 7.34 | 11.08 | 0.02 * |
| Serum micronutrient level | Normal values [17] | 25th percentile | Median | 75th percentile | 95th percentile | 25th percentile | Median | 75th percentile | 95th percentile | p-value |
| VitaminA (µg/dL) | 20–100 | 46.00 | 58.00 | 71.00 | 102.80 | 47.00 | 52.00 | 66.00 | 84.10 | 0.11 |
| Vitamin B12 (pg/mL) | 279–996 | 243.00 | 290.00 | 350.00 | 906.80 | 257.50 | 304.50 | 390.25 | 623.70 | 0.21 |
| [25(OH)D] (ng/mL) | 30–100 | 17.60 | 20.72 | 25.32 | 34.64 | 16.87 | 19.93 | 25.43 | 40.89 | 0.45 |
| Calcium (mg/dL) | 8.5–10.5 | 8.23 | 8.53 | 9.11 | 14.25 | 8.34 | 8.79 | 9.24 | 10.34 | 0.22 |
| Zinc (µg/dL) | 75–120 | 88.51 | 100.29 | 116.07 | 168.05 | 89.58 | 99.95 | 113.21 | 167.66 | 0.85 |
| Evaluate Parameters | Age Group | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 60–75 Years | >75 Years | |||||||||
| n = 99 | n = 83 | |||||||||
| 25th Percentile | Median | 75th Percentile | 95th Percentile | 25th Percentile | Median | 75th Percentile | 95th Percentile | |||
| BMI (kg/m2) | 25.27 | 27.33 | 30.52 | 36.1651 | 24.32 | 26.81 | 28.76 | 35.4204 | 0.05 | |
| Micronutrient intake | Recommended Daily Dose [15,16] | 25th percentile | Median | 75th percentile | 95th percentile | 25th percentile | Median | 75th percentile | 95th percentile | p-value |
| Vitamin A (µg/day) | 700 (women) and 900 (men) | 210.71 | 354.56 | 494.97 | 972.18 | 260.89 | 450.01 | 673.31 | 1676.77 | 0.01 * |
| Vitamin B12 (µg/day) | 2.40 | 1.13 | 1.88 | 2.69 | 5.19 | 1.45 | 2.06 | 3.04 | 4.85 | 0.16 |
| Vitamin D3 (µg/day) | 15 | 0.64 | 3.12 | 6.01 | 9.95 | 1.39 | 3.89 | 7.32 | 13.08 | 0.05 |
| Calcium (mg/day) | 1200 | 303.70 | 497.18 | 699.84 | 1052.58 | 411.32 | 588.36 | 857.31 | 1570.49 | 0.04 * |
| Zinc (mg/day) | 8 (women) and 11 (men) | 3.88 | 5.52 | 7.23 | 9.30 | 4.91 | 6.25 | 8.85 | 11.54 | 0.02 * |
| Serum micronutrient level | Normal values [17] | 25th percentile | Median | 75th percentile | 95th percentile | 25th percentile | Median | 75th percentile | 95th percentile | p-value |
| Vitamin A (µg/dL) | 20–100 | 46.25 | 53.50 | 68.00 | 90.60 | 47.00 | 52.00 | 65.50 | 80.40 | 0.47 |
| Vitamin B12 (pg/mL) | 279–996 | 252.00 | 300.50 | 376.50 | 641.60 | 270.50 | 304.00 | 393.00 | 649.80 | 0.47 |
| [25(OH)D] (ng/mL) | 30–100 | 16.77 | 19.54 | 24.24 | 41.17 | 17.34 | 20.72 | 27.14 | 35.00 | 0.69 |
| Calcium (mg/dL) | 8.5–10.5 | 8.31 | 8.73 | 9.26 | 10.25 | 8.32 | 8.74 | 9.19 | 10.66 | 0.83 |
| Zinc (µg/dL) | 75–120 | 90.47 | 101.84 | 119.48 | 169.16 | 88.13 | 97.76 | 109.14 | 150.59 | 0.01 * |
| Evaluated Parameters | Food PACAM Consumption Group | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Consumes | Does not Consume | |||||||||
| n = 115 | n = 67 | |||||||||
| 25th Percentile | Median | 75th Percentile | 95th Percentile | 25th Percentile | Median | 75th Percentile | 95th Percentile | |||
| BMI (kg/m2) | 25.04 | 27.22 | 29.72 | 35.94 | 24.35 | 27.06 | 29.62 | 35.54 | 0.38 | |
| Micronutrient intake | Recommended Daily Dose [15,16] | 25th percentile | Median | 75th percentile | 95th percentile | 25th percentile | Median | 75th percentile | 95th percentile | p-value |
| Vitamin A (µg/day) | 700 (women) and 900 (men) | 241.90 | 381.32 | 612.20 | 1388.47 | 250.86 | 373.69 | 497.35 | 926.21 | 0.27 |
| Vitamin B12 (µg/day) | 2.40 | 1.30 | 1.99 | 2.84 | 4.60 | 1.17 | 1.90 | 3.06 | 5.40 | 0.71 |
| Vitamin D3 (µg/day) | 15 | 1.31 | 3.93 | 6.69 | 12.38 | 0.63 | 2.68 | 5.15 | 10.21 | 0.03 * |
| Calcium (mg/day) | 1200 | 392.40 | 555.72 | 762.73 | 1458.51 | 308.89 | 475.66 | 700.17 | 1015.18 | 0.07 |
| Zinc (mg/day) | 8 (women) and 11 (men) | 4.92 | 6.28 | 8.52 | 11.14 | 3.89 | 5.13 | 6.58 | 9.95 | 0.00 * |
| Serum micronutrient level | Normal values [17] | 25th percentile | Median | 75th percentile | 95th percentile | 25th percentile | Median | 75th percentile | 95th percentile | p-value |
| Vitamin A (µg/dL) | 20–100 | 47.00 | 55.00 | 67.00 | 86.40 | 46.00 | 51.50 | 67.25 | 85.65 | 0.23 |
| Vitamin B12 (pg/mL) | 279–996 | 263.00 | 301.00 | 375.00 | 587.20 | 242.75 | 306.50 | 387.00 | 758.70 | 0.77 |
| [25(OH)D] (ng/mL) | 30–100 | 16.89 | 20.39 | 24.24 | 37.34 | 16.85 | 19.45 | 26.13 | 39.04 | 0.61 |
| Calcium (mg/dL) | 8.5–10.5 | 8.31 | 8.69 | 9.11 | 10.15 | 8.32 | 8.79 | 9.34 | 11.70 | 0.41 |
| Zinc (µg/dL) | 75–120 | 87.96 | 98.85 | 109.84 | 142.89 | 93.27 | 103.47 | 119.63 | 238.52 | 0.01 * |
| GROUPS | [25(OH)D] (<30 ng/mL) | Vitamin B12 (<279 ng/mL) | Calcium (<8.5 mg/dL) | Zinc (<75 µg/L) | |
|---|---|---|---|---|---|
| Nutritional status | Underweight | 12.42% (n = 20) | 14.75% (n = 9) | 12.12% (n = 8) | 36.36% (n = 4) |
| Normal | 44.72% (n = 72) | 42.62% (n = 26) | 37.88% (n = 25) | 27.27% (n = 3) | |
| Overweight | 29.81% (n = 48) | 27.87% (n = 17) | 33.33% (n = 22) | 27.27% (n = 3) | |
| Obese | 13.04% (n = 21) | 14.75% (n = 9) | 16.67% (n = 11) | 9.09% (n = 1) | |
| Gender | Male | 21.12% (n = 34) | 24.59% (n = 15) | 27.27% (n = 18) | 27.27% (n = 3) |
| Female | 78.88% (n = 127) | 75.41% (n = 46) | 72.73% (n = 48) | 72.73% (n = 8) | |
| Age group | 60–75 | 53.42% (n = 86) | 60.66% (n = 37) | 50% (n = 33) | 54.55% (n = 6) |
| >75 | 46.58% (n = 75) | 39.34% (n = 24) | 50% (n = 33) | 45.45% (n = 5) | |
| PACAM consumption | Consumes | 63.35% (n = 102) | 59.02% (n = 36) | 69.70% (n = 46) | 63.64% (n = 7) |
| Does not consume | 36.65% (n = 59) | 40.98% (n = 25) | 30.30% (n = 20) | 36.36% (n = 4) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arazo-Rusindo, M.C.; Zúñiga, R.N.; Cortés-Segovia, P.; Benavides-Valenzuela, S.; Pérez-Bravo, F.; Castillo-Valenzuela, O.; Mariotti-Celis, M.S. Nutritional Status and Serum Levels of Micronutrients in an Elderly Group Who Participate in the Program for Complementary Food in Older People (PACAM) from the Metropolitan Region, Santiago de Chile. Nutrients 2022, 14, 3. https://doi.org/10.3390/nu14010003
Arazo-Rusindo MC, Zúñiga RN, Cortés-Segovia P, Benavides-Valenzuela S, Pérez-Bravo F, Castillo-Valenzuela O, Mariotti-Celis MS. Nutritional Status and Serum Levels of Micronutrients in an Elderly Group Who Participate in the Program for Complementary Food in Older People (PACAM) from the Metropolitan Region, Santiago de Chile. Nutrients. 2022; 14(1):3. https://doi.org/10.3390/nu14010003
Chicago/Turabian StyleArazo-Rusindo, Migdalia Caridad, Rommy N. Zúñiga, Pablo Cortés-Segovia, Sergio Benavides-Valenzuela, Francisco Pérez-Bravo, Oscar Castillo-Valenzuela, and María Salomé Mariotti-Celis. 2022. "Nutritional Status and Serum Levels of Micronutrients in an Elderly Group Who Participate in the Program for Complementary Food in Older People (PACAM) from the Metropolitan Region, Santiago de Chile" Nutrients 14, no. 1: 3. https://doi.org/10.3390/nu14010003
APA StyleArazo-Rusindo, M. C., Zúñiga, R. N., Cortés-Segovia, P., Benavides-Valenzuela, S., Pérez-Bravo, F., Castillo-Valenzuela, O., & Mariotti-Celis, M. S. (2022). Nutritional Status and Serum Levels of Micronutrients in an Elderly Group Who Participate in the Program for Complementary Food in Older People (PACAM) from the Metropolitan Region, Santiago de Chile. Nutrients, 14(1), 3. https://doi.org/10.3390/nu14010003